
Abstract
Objective. To evaluate the usefulness of video pneumatic otoscopy (VPO) for the diagnosis of conductive hearing loss (CHL) with normal tympanic membranes (TM).
Study Design. Prospective study.
Setting. Tertiary care hospital.
Subjects and Methods. Thirty-seven ears with CHL and 9 control ears with normal TMs were included. The VPO was performed preoperatively in all patients. The authors captured TM images in 3 stages of the VPO (static, positive, and negative pressure stage) in all subjects and measured the amount of relative position differences of the umbo. Pure-tone audiometry and temporal bone computed tomography (TBCT) were performed preoperatively. The possible causes of hearing loss were evaluated during exploratory tympanotomy in the patients with CHL.
Results. Fifteen patients had stapedial fixation, 10 had fixation of the malleus or incus (MIF), and 12 had ossicular discontinuity. The positional differences between the negative and positive pressure stage of the MIF group were significantly smaller between the CHL and control groups (P = .001). The air-bone gap showed no significant difference among the CHL groups. The sensitivity, specificity, and diagnostic accuracy of the VPO for the diagnosis of MIF, with a cutoff value of 1.5% or less in terms of the movement of umbo, were 80.0%, 92.6%, and 89.2%, respectively. These findings were comparable to those of the TBCT, which were 90.0%, 85.2%, and 86.5%, respectively.
Conclusion. The VPO is a simple, noninvasive, and accurate tool for the differential diagnosis of CHL with a normal TM.
Pneumatic otoscopy (PO) is a well-known method used to assess for the presence of a middle ear effusion (MEE) and hypomobility of the tympanic membrane (TM). The recent clinical practice guidelines for otitis media with effusion (OME) recommend that clinicians use PO as the primary diagnostic method for MEE. 1 Movement of the TM can be documented with video pneumatic otoscopy (VPO) using an otoendoscope and video apparatus. In the previous study, we found parameters of the VPO such as minimal pressure, maximal pressure, and movement of the umbo useful for the visual diagnosis of an MEE. 2 Among these parameters, since the pressure of the external auditory canal (EAC) is not usually measured in the clinical setting, the movement of the umbo may be the most practical and reliable parameter reflecting the middle ear status in the clinical setting.
Conductive hearing loss (CHL) with a normal TM is a common problem encountered in the otology clinic. The etiology for this condition includes congenital or acquired ossicular discontinuity, ossicular fixation, and otosclerosis. As the otoendoscopic findings usually reveal a normal TM, a preoperative diagnosis is often unlikely before exploration, and high-resolution temporal bone computed tomography (TBCT) may be helpful for the diagnosis. Because the fixation or discontinuity of the ossicular chain may affect the movement of the TM during the PO, the evaluation of TM movement using the VPO may provide reliable information on the middle ear status of this patient group.
The purpose of this study was to evaluate the usefulness of the VPO by quantitative analysis of the TM for the assessment of the middle ear status in patients with CHL and a normal TM. The diagnostic accuracy of the VPO was evaluated and compared with that of the TBCT.
Materials and Methods
Patient Selection
The Institutional Review Board of Samsung Medical Center granted approval for this study. A total of 37 patients with unilateral CHL and a normal TM (14 men and 23 women) 13 to 67 years of age (mean 38.35 years) participated in this prospective study. Nine patients without ear abnormalities were also included in the study as controls.
All patients underwent pure-tone audiogram (PTA) testing on the day of the first visit. A history was obtained on previous episodes of chronic otitis media (COM), other otological conditions, and treatment, including surgery and ventilation tube insertion. Patients with a history of previous ear surgery were excluded from the study. Likewise, ears with a perforated TM, atrophy, or significant tympanosclerosis, which may affect the movement of the TM, were also excluded. A normal control group included 9 healthy ears without hearing loss in 9 adults (4 men and 5 women) 15 to 36 years of age (mean, 25.56 years). All enrolled patients underwent VPO and high-resolution TBCT. Subsequently, exploratory tympanotomy with proper reconstruction of the ossicular chain was performed in all CHL patients. The status of the ossicular chain was carefully examined and recorded during the operation.
Video Pneumatic Otoscopy
Equipment
The dynamic movements of the TM were recorded and digitized using a CCD camera (OTV-SP1; Olympus, Tokyo, Japan) and video monitor system (LMD-2140MD; Olympus) with S-VHS input to a visual board (MIRO DC 30; Pinnacle system, Mountain View, California) in a PC-based computer.
Procedures for Recording of TM Movement
All measurements were performed by a single otologist. At first, a gentle but firm pressure was applied to cause maximal excursion of the TM. If the TM did not move with the initial positive pressure, more pressure was applied progressively to cause movement. Then, the same amount of pressure was applied 3 to 4 times in each ear. The movement of the TM and the malleus, associated with the deflation and inflation of the rubber bulb, was recorded in the form of a digital moving picture (MPEG). During the recording, the tip of the endoscope stayed fixed in the EAC, and the angle of the endoscope facing the TM was kept constant (
Quantitative Analysis of the TM Movement
Still images of the TM in the static stage, the positive pressure (pos) stage, and the negative pressure (neg) stage were saved in a JPEG file from the MPEG file ( Figure 1 ). Quantitative analysis of the TM was performed by 3 otolaryngologists. The printed images of the TM with reference lines at each stage were provided without any information about the patients; all measurements were done separately. The average value of 3 measurements was used for the quantitative analysis of TM movement.
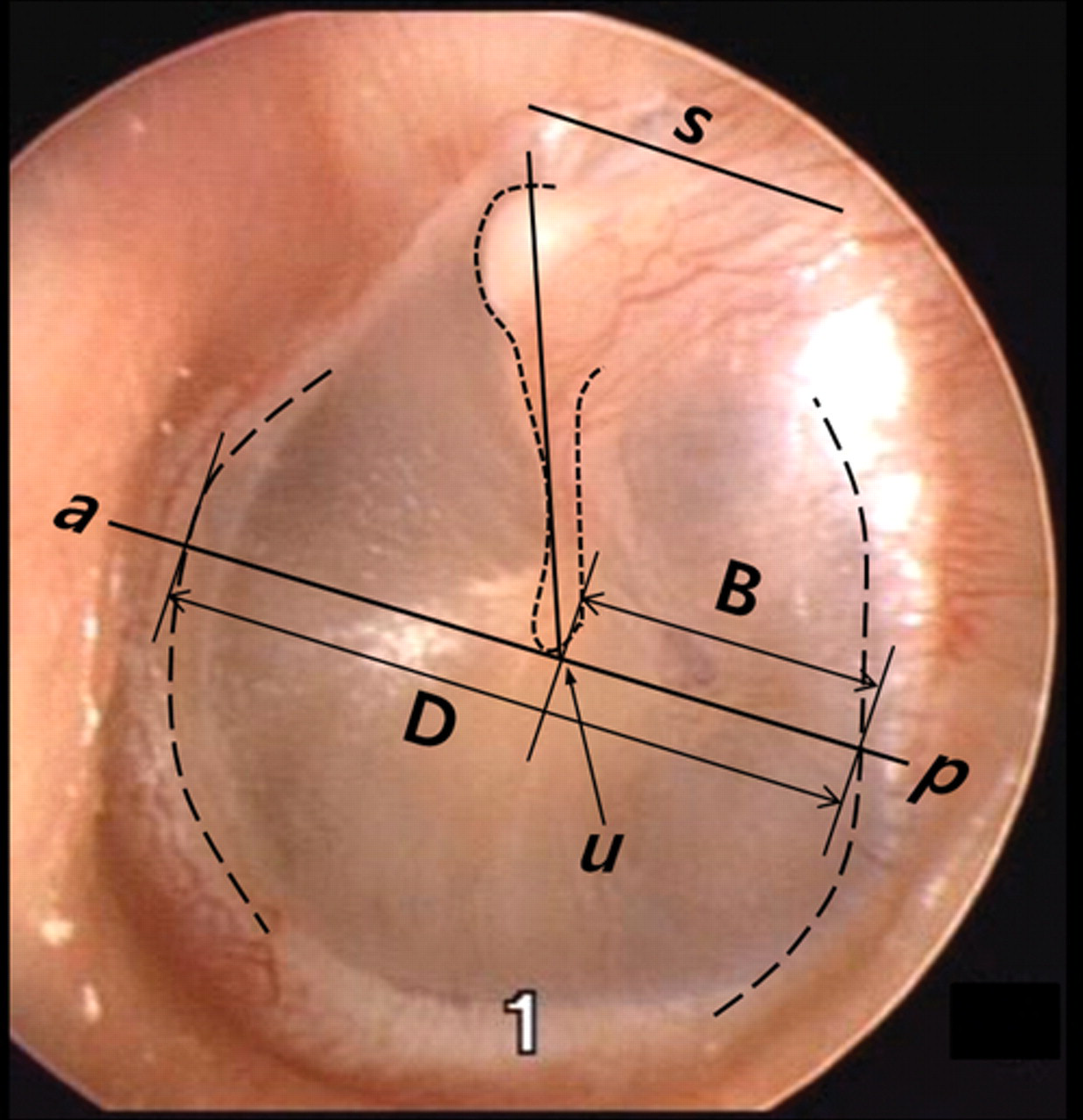
Still image during VPO of a normal tympanic membrane (TM): an outline of the handle of the malleus was drawn for each image. An s line connects the anterior and posterior tympanic spine. Parallel to the s line, the ap line was drawn to meet the u line at the pos point. The length between a and p was defined as the horizontal diameter of the TM (D). The u was defined as a point where the tip of the malleus handle crosses the ap line. The distance between the u and p point was defined as B. VPO, video pneumatic otoscopy; static, static pressure stage.
Measurement of the position of the umbo ( Figure 1 )
First, using the drawing function of software (Microsoft Office PowerPoint 2007), a horizontal line (line s) passing through the anterior and posterior tympanic spine was drawn. Second, the outlines of the anterior and posterior bony annulus, at the pos stage, were used as a reference. The 3 lines were grouped as a template and copied to the other images at the static and neg stages. Then, the images were printed out, and the fourth line (ap) horizontal to the line s passing through the umbo tip (point u) was manually drawn on the printed image at each stage. The anterior (a) and posterior points (p) were marked at where the outlines of the anterior and posterior bony annulus and the ap lines crossed. The distance between the a and b points was defined as the horizontal diameter of the TM (D). The length (B) between point p and point u was measured at each stage ( Figure 1 ). Considering the variable distance from the TM and possible subtle movement of the otoendoscope, the B/D percentage was defined as the position of the umbo. 2
Difference in position of the umbo at each stage
To define the movement of the umbo, the B/D percentage at each stage was obtained first. Next, the degrees of movement of the umbo from the neg to pos stage (B/D neg − B/D pos , %), from the neg to static stage (B/D neg − B/D static , %), and from the static to pos stage (B/D static − B/D pos , %) were calculated ( Table 1 ).
Demographic and Audiological Data and the Amount of Umbo Movement of Each Group of Patients
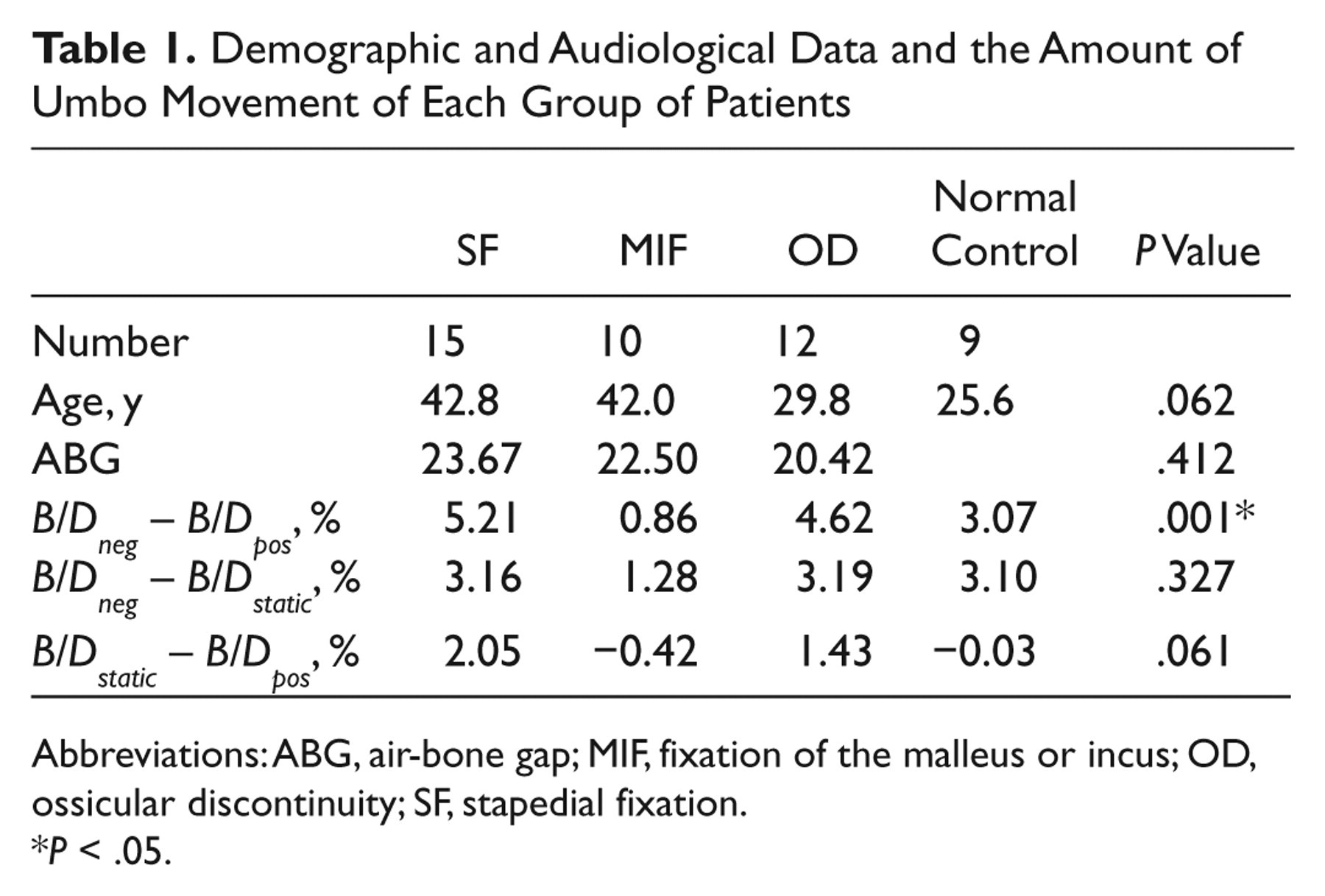
Abbreviations: ABG, air-bone gap; MIF, fixation of the malleus or incus; OD, ossicular discontinuity; SF, stapedial fixation.
P < .05.
Operative Findings of the Exploratory Tympanotomy
During the exploratory tympanotomy, the middle ear status, including the continuity and mobility of the ossicular chain, was evaluated, and the possible etiologies of CHL were assessed according to the middle ear status, including fixation of the stapes footplate with an intact ossicular chain, a fixed ossicular chain lateral to the incudostapedial joint, and an unconnected ossicular chain, defined as stapedial fixation (SF), fixation of the malleus or incus (MIF), and ossicular discontinuity (OD), respectively.
Temporal Bone Computerized Tomography
A high-resolution TBCT was obtained with a 0.625-mm slice thickness, 120 kV, 250 mAs, and continuous nonoverlapping sections. TBCTs were reviewed by 2 radiologists, and the most likely etiology of conductive hearing loss was made after discussion about SF, MIF, and OD. The results were used to compare the diagnostic accuracy of TBCT with that of the VPO. An example of the TBCT findings of MIF is shown in Figure 2 .

An axial TBCT image of a patient with MIF: This image shows abnormal calcified bridges between the epitympanic wall and the malleus and incus (black and white arrows). TBCT, temporal bone computed tomography; MIF, fixation of the malleus or incus.
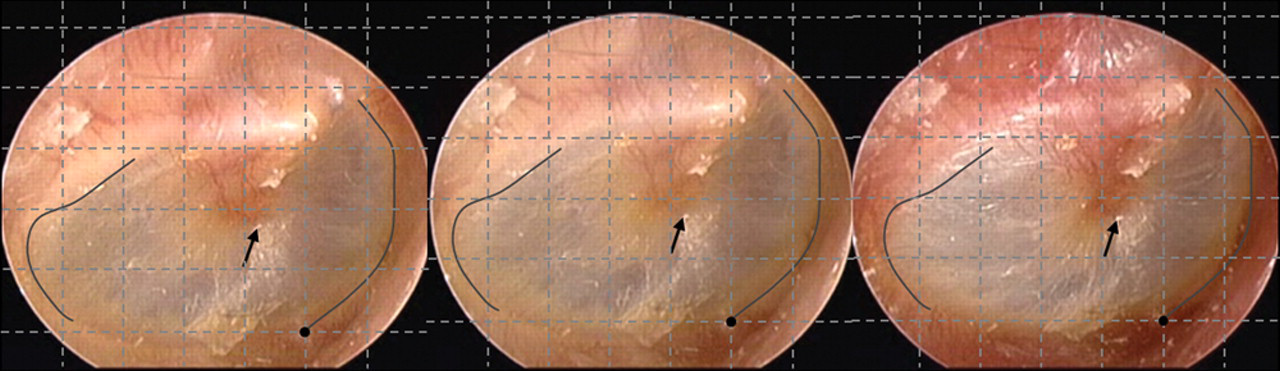
Serial images of the TM with fixation of the malleus or incus at each pressure stage (static, pos, neg) are shown. The TM looks normal, but the umbo (arrows) barely moves during VPO. Grid lines are overlaid on each image with reference to the contour lines of anterior and posterior annuluses and a fixed point. TM, tympanic membrane; VPO, video pneumatic otoscopy; static, static pressure stage; pos, positive pressure stage; neg, negative pressure stage.
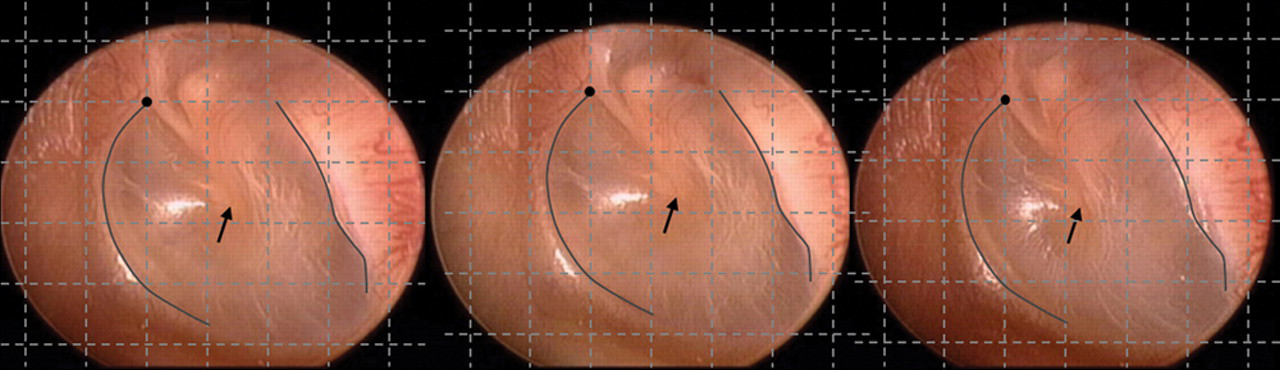
Serial images of the TM with stapedial fixation at each pressure stage (static, pos, neg). The tympanic membrane looks normal, and the umbo (arrows) shows a subtle movement during the VPO. Grid lines are overlaid on each image with reference to the contour lines of anterior and posterior annuluses and a fixed point. VPO, video pneumatic otoscopy; static, static pressure stage; pos, positive pressure stage; neg, negative pressure stage.
Acquisition of the Air-Bone Gap
Pure-tone audiometry was performed in all patients with CHL before surgery. The average hearing level difference between air and bone conduction from 0.5, 1, 2, and 3 kHz was defined as the air-bone gap (ABG).
Statistical Analysis
Statistical analysis was performed using PASW statistics software (version 17; SPSS, an IBM Company, Chicago, Illinois) with the significance level set at P < .05. For comparison of the VPO parameters among each group, a 1-way analysis of variance (ANOVA) with multiple comparisons and a paired t test were used. The Spearman correlation coefficient was used to evaluate the correlation between ABG and VPO parameters.
Results
Demographic Data
The number of patients in each CHL group was 15 with SF, 10 with MIF, and 12 with OD. Their mean ages were 42.8, 42.0, and 29.8 years, respectively ( Table 1 ). The mean age of the OD group was younger than the other groups (P = .062), supporting the congenital nature of the disorder.
Quantitative Measurements of the Parameters in Each Ear With CHL and Normal Ears
The amount of positional difference of the umbo between the negative and positive pressure stage (B/D neg − B/D pos ) of the MIF group was significantly smaller compared to the other CHL groups and the normal group (P = .001). Although the amount of positional difference between the neg and static stage (B/D neg − B/D static ) and static and pos stage (B/D static − B/D pos ) was small in the MIF group, there were no significant differences among 3 CHL groups and the normal group ( Table 1 ).
Comparison of Accuracy With the TBCT
Since the movement of the umbo in the MIF group was shown to be useful for the differential diagnosis, the diagnostic accuracy was compared with that of the TBCT. The TBCT was reviewed, and the radiologic diagnosis for each case was categorized into 3 groups. There were 16 patients in the SF group, 12 in the MIF group, and 9 in the OD group. To diagnose the MIF with a cutoff value of 1.5% or less, in terms of the movement of the umbo, the sensitivity, specificity and diagnostic accuracy of the VPO were 80.0%, 92.6%, and 89.2%, respectively. When the cutoff value was increased to 2% or less, the sensitivity, specificity, and diagnostic accuracy of the VPO were 80.0%, 88.9%, and 86.5%, respectively. The sensitivity, specificity, and diagnostic accuracy of the TBCT were 90.0%, 85.2%, and 86.5%, respectively ( Table 2 ).
Sensitivity, Specificity, and Diagnostic Accuracy of the VPO for the Diagnosis of MIF Compared to the TBCT
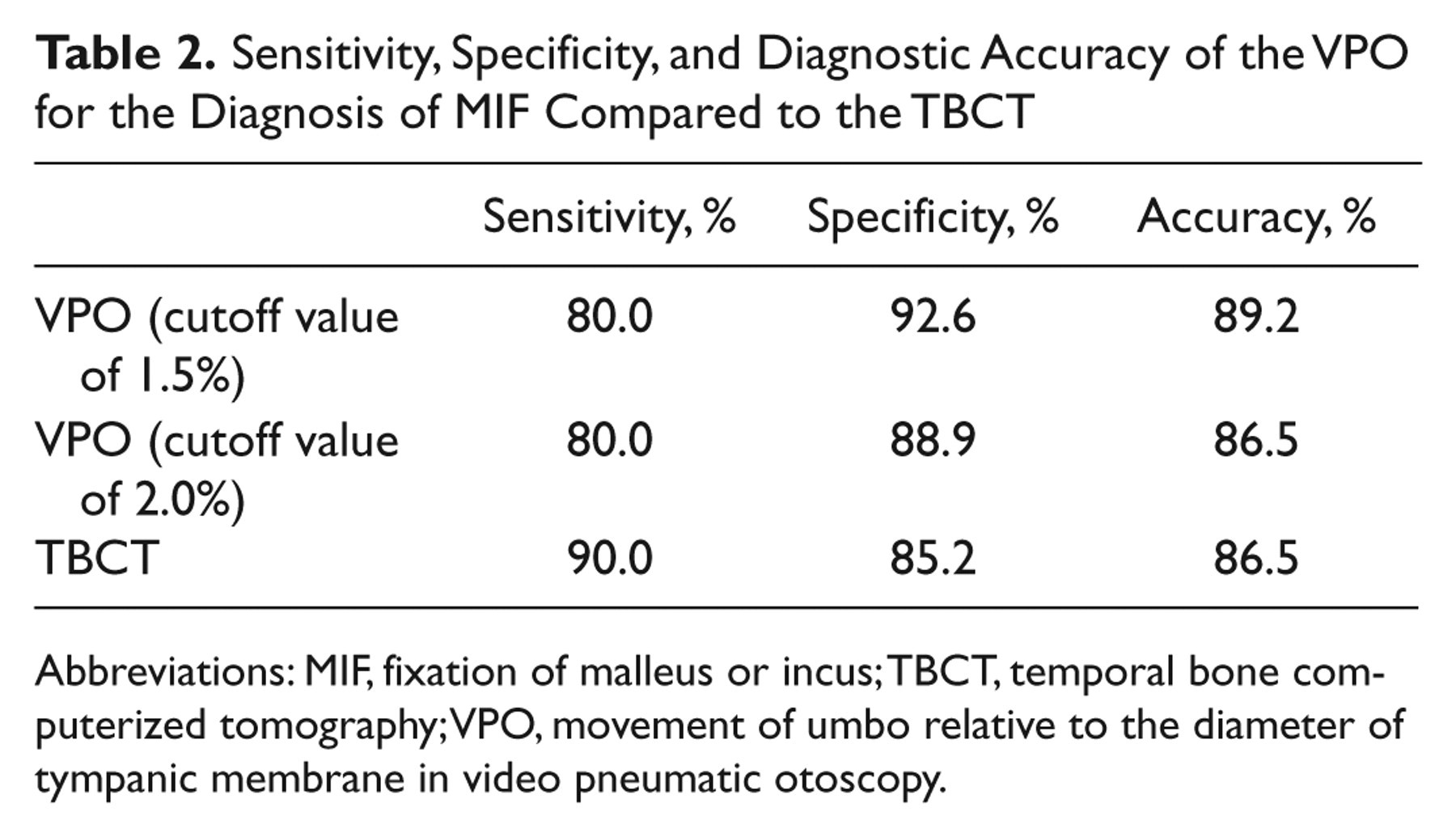
Abbreviations: MIF, fixation of malleus or incus; TBCT, temporal bone computerized tomography; VPO, movement of umbo relative to the diameter of tympanic membrane in video pneumatic otoscopy.
Correlation With the Air-Bone Gap
The average ABGs of the SF, MIF, and OD groups were 23.67, 22.50, and 20.42, respectively ( Table 1 ). The ABG did not have a significant difference among the CHL groups or any correlation with the umbo movement ( Table 1 ).
Discussion
Patients with CHL and a normal TM usually undergo surgical exploration of the middle ear to determine the final diagnosis and improve hearing, even though comprehensive examinations, including audiometry, tympanometry, and computed tomography (CT) scanning, are initially performed. Kakehata et al 3 suggested that transtympanic endoscopy through a perforation made by a laser-assisted myringotomy might be a safe and effective office-based procedure for the diagnosis of CHL and an alternative procedure that could be used to replace the exploratory tympanotomy. However, this method is invasive and limited in its ability to correct hearing loss.
There have been several reports on diagnostic methods for the middle ear pathology of patients with CHL. Shahnaz and Polka 4 evaluated alternative tympanometric parameters for distinguishing normal ears from ears with otosclerosis; they found that multifrequency tympanometry (MFT) was better than the standard low-frequency tympanometry in differentiating otosclerotic and normal ears. In addition, they compared the usefulness of the energy reflectance (ER), MFT, and conventional tympanometry for distinguishing otosclerosis from normal ears. ER patterns compared to normal ears correctly identified 82% of the otosclerotic ears with a low false-positive rate (17.2%). 5
Funasaka et al 6 developed sweep frequency tympanometry and used it to differentiate middle ear pathologies. In their study of human temporal bones, 83% of the ears with ossicular discontinuity and malleus/incus fixation and 55% of the ears with stapedial fixation were correctly identified using this equipment. 7
The VPO is a standard method used for the diagnosis of MEE. In all patients with CHL, VPO is routinely used in our clinic to check the mobility and rule out MEEs. The VPO is safe and easy to perform in the office, and little cost and time are required for its use. As some patients with CHL show different mobility of the TM, this prospective study was designed to review and document VPO findings to determine the useful diagnostic parameters. Analysis of this simple procedure showed significant hypomobility of the TM in the ears with MIF. Contrary to our expectation, the TMs with stapedial fixation failed to show a difference from those with ossicular discontinuity or normal TMs with regard to movement of the umbo. According to our experience, a slight movement of the umbo, which is only 1.5% to 2% of the diameter of the TM, was enough to detect.
Several investigators have reported on the frequency of MIF among primary stapedectomy cases, which has ranged from only 0.4% to 1.6%. 8-10 Although the pathogenesis is not completely understood, MIF presents in the form of unilateral or, more rarely, bilateral progressive conductive hearing loss with an intact TM. Idiopathic or primary malleus fixation occurs most commonly in the later decades of life and is frequently associated with presbyacusis. 11 This condition occurs equally in men and women and often in patients with no apparent history of ear abnormalities. 12 In an analysis of a series of 340 exploratory tympanotomies for CHL, the most common operative diagnosis was otosclerosis (n = 164, 48.2%), followed by ossicular discontinuity (n = 103, 30.3%). Fixation of the malleus and/or incus was only 2.3% (n = 8) in this series. 13
TBCT is known as a reliable, sensitive, and specific method used for the diagnosis of CHL with a normal TM. 14 In this study, the sensitivity, specificity, and diagnostic accuracy of TBCT were 90.0%, 85.2%, and 86.5%, respectively. The diagnostic accuracy of the VPO with a cutoff value of 2% was the same as the TBCT (86.5%). The diagnostic accuracy of the VPO was even higher (89.2%) than that of the TBCT when the cutoff value was set at 1.5%. Although the sensitivity was higher with the TBCT, the specificity was superior with the VPO. These findings indicate that the VPO can detect the absence of fixation of the malleus or incus more accurately. These results suggest that the VPO can be used as an alternative and supplementary diagnostic tool for patients with CHL and a normal TM. It may be especially valuable when radiation is contraindicated or not recommended, such as in the case of pregnant women. Although the result of VPO does not preclude the purpose of exploration, which provides exact diagnosis and definitive treatment, the clues of middle ear pathology obtained from VPO can help clinicians in patient counseling and preoperative planning.
The limitations of this study include the following. First, this study includes a small number of subjects, which makes the generalization of the results difficult. Second, as it is difficult to manually apply a same pressure at every procedure of VPO, a subtle inconsistency of pressure may have hampered the accurate analysis of umbo movement. Therefore, further modification of the system, which can provide a constant pressure using a manometer, would be necessary for clinical use of the VPO technique. Third, the VPO parameters were manually measured from the captured TM images. Although we used a computer in some steps of the analysis, most of the work was processed manually; this may have increased the likelihood of processing error. More advanced digital equipment with appropriate software may be necessary for the actualization of the methods discussed here.
Despite these limitations, the results of this study suggest useful parameters for the quantitative analysis of VPO findings for the diagnosis of patients with CHL and a normal TM. Further studies with a larger study group and more standardized, computerized methods of analysis are needed for clinical application of the results of this study.
Conclusion
The movement of the umbo between the negative and positive pressure stages in patients with MIF was significantly smaller than in the other CHL groups and the group of normal ears. The diagnostic accuracy of the VPO for the diagnosis of MIF was comparable to the TBCT. These results suggest that the VPO is a useful office-based, noninvasive diagnostic tool for the diagnosis of patients with CHL and a normal TM.
Author Contributions
Disclosures
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.