
Abstract
Objectives. To determine the prevalence of positional plagiocephaly and brachycephaly in teenagers born after the “Back to Sleep” campaign but before orthotic helmet treatment became widely available and to provide long-term outcomes data on those children with plagiocephaly who were not treated with remolding therapy.
Study Design. Cross-sectional analysis.
Setting. Local high schools in the Minneapolis–St Paul Metro area.
Subjects and Methods. Subjects were selected if they attended participating high schools and were born after the Back to Sleep campaign began. Skull measurements, including transcranial diameter, length, and width, were taken. Overall facial appearance was inspected for any apparent abnormal characteristics. Cranial vault asymmetry and cephalic index were calculated for each participant. Plagiocephaly was diagnosed if cranial vault asymmetry was >1 cm. Brachycephaly was diagnosed if the cephalic index was >0.90.
Results. There were 1045 participants, ranging from 12 to 17 years old, with an average age of 15.7 years. The prevalence of plagiocephaly was 1.1%. The prevalence of brachycephaly was 1.0%. The overall prevalence of a deformational cranial abnormality was 2.0%. Of those who met diagnostic criteria of plagiocephaly or brachycephaly, 38.1% were noted to have abnormal facial characteristics.
Conclusions. The prevalence of plagiocephaly and brachycephaly in teenagers is significantly lower than the 20% to 48% prevalence found in infants in previous studies, suggesting most children will outgrow the condition without intervention. Additional studies are needed to determine which patients might benefit from treatment and which will likely have resolution without intervention, since treating all infants who meet criteria results in significant overtreatment.
The terms positional plagiocephaly and deformational plagiocephaly are used to describe an abnormally shaped skull caused by mechanical forces. Simply put, the terms describe an infant or toddler who develops a flat area of the skull at the back of the head (occiput) due to being positioned flat on his or her back during sleep. Brachycephaly is the term used to describe flattening along the entire posterior aspect of the skull, resulting in an increased width-to-length ratio of the skull.1,2 Plagiocephaly and brachycephaly develop because of the moldable nature of the infant’s skull due to the fontanelles and patent cranial sutures. Figures 1 and 2 show examples of infants who meet criteria for brachycephaly and plagiocephaly.

An infant with brachycephaly, showing the flattening of the occipital portion of the skull.

An infant with plagiocephaly that shows the asymmetry of the frontal bone and occiput.
In 1992, the American Academy of Pediatrics published a report linking sudden infant death syndrome (SIDS) to babies sleeping in the prone position, and they began the “Back to Sleep” campaign, which recommended that infants be placed in the supine position when sleeping. 3 Prior to 1992, most infants were placed prone when sleeping. Since the Back to Sleep campaign, there has been concern that an increasing number of infants are developing positional plagiocephaly and brachycephaly. 4 A review of the literature indicates anywhere from 20% to nearly 50% of 6-month-old infants may have positional plagiocephaly.4-6 While there has been an increase in plagiocephaly and brachycephaly, the rate of SIDS has decreased by 50% since the Back to Sleep campaign started, 7 from 1.4 of 1000 live births in the late 1980s to a current rate of 0.54 of 1000 live births. 3 In 2003, the American Academy of Pediatrics published a report suggesting ways to prevent plagiocephaly, which included encouraging “tummy time” while the infant is awake and limiting time spent in car seats. 8 However, even with the recommendations to prevent plagiocephaly, the incidence remains high, and parents frequently voice concern to their primary care provider. Consequently, the use of a specially designed molding helmet, or cranial orthotic device, to correct plagiocephaly has become more widespread. Reports from orthotic helmet manufacturers have indicated an increase in requests for helmet fittings by 15% each year. 9 Cranial orthoses are regulated by the US Food and Drug Administration (FDA) and are considered a Class II neurology device. They were approved by the FDA in 1998. 10
Numerous studies in the past few years have advocated different tools for diagnosing positional plagiocephaly, ranging from computed tomography scans and digital surfacing technology to the standard anthropomorphic measurements using a tape measure and calipers.9,11 No studies prove that imaging tools improve the diagnosis when compared with standard anthropomorphic measurements. 9 The best documented anthropomorphic measurements to diagnose plagiocephaly are the oblique transcranial diameter from each side, which measures from frontozygomatic to the contralateral occipital distance. The cranial vault asymmetry is the absolute difference between the 2 oblique transcranial diameter measurements. Most craniofacial surgeons recommend treatment of plagiocephaly if the cranial vault asymmetry is greater than 1 cm.1,12 The cranial index, which is the maximum width divided by the maximum length, is used to diagnose brachycephaly.9,13 The diagnosis of brachycephaly is given if the cranial index is greater than 0.85 to 0.90. 1
The exact number of orthoses prescribed each year is unknown, but one hospital in Minnesota published a report in 2004 stating they prescribed 300 helmets/y. 10 Extrapolating from that data set, it is likely that in Minnesota, a minimum of 500 helmets are currently prescribed per year. With that extrapolated frequency in Minnesota, it is likely more than 25,000 helmets are prescribed nationally each year. The total cost nationwide would approach $75 million, if each of the 25,000 helmets costs $3000.14,15
Most studies have followed infants diagnosed with plagiocephaly only up to age 2 years. No study has evaluated the incidence in older children to determine whether positional plagiocephaly and brachycephaly persist into adolescence or whether children’s skulls naturally grow into normal shape with age.4,9,11The primary objective of this study was to determine the prevalence of positional plagiocephaly and/or brachycephaly in teenagers born after the Back to Sleep campaign but before helmeting became available with the 1998 FDA approval of orthotic helmets to better understand long-term outcomes for infants diagnosed today. This question is much more pressing since the Back to Sleep campaign has resulted in a significant increase in skull asymmetries in infants.
Materials and Methods
This study was approved by the Institutional Review Board at Children’s Hospitals and Clinics of Minnesota. This cross-sectional study was conducted to determine the prevalence of plagiocephaly and brachycephaly in teenagers born after the Back to Sleep campaign but before helmeting became widely available. Local high schools and junior high schools were contacted to get local participation. Students were able to participate in the study if they were born after 1992 but before 1998, which is when FDA approval for cranial orthotics was granted. All participants were required to have a signed parental permission slip, and any student could decline participation.
Age, sex, and race were recorded from each participant, but no other personal information was recorded. The face was visually inspected for any gross abnormalities or asymmetries. The head circumference was measured using a disposable tape measure. The head width, length, and bilateral oblique transcranial diameters were obtained using anthropometric calipers. All measurements were obtained by the lead researcher in a consistent fashion. Prior to the start of this study, the lead researcher was validated in obtaining these measurements by the craniofacial surgeon of the Craniofacial/Plagiocephaly Clinic at Children’s Hospitals and Clinics of Minnesota.
The diagnosis of plagiocephaly was based on the calculation of cranial vault asymmetry, which is the absolute difference between the bilateral oblique transcranial diameters ( Figure 3 ). Cranial vault asymmetry greater than 1 cm was used as our criterion for the diagnosis of plagiocephaly. The diagnosis of brachycephaly was based on the calculation of cephalic index, which is width divided by length. Brachycephaly was diagnosed if the cephalic index was greater than 0.90. Incidence of plagiocephaly and brachycephaly by sex was compared using χ2, or Fisher exact test if cell entries did not meet the requirement of χ2, with a 2-sided P value <.05 for significance. Ninety-five percent confidence intervals on the prevalence of plagiocephaly and brachycephaly in this study population are based on the variance of a binomial distribution. SPSS version 17.0 (SPSS Inc, Chicago, Illinois) was used for statistical analysis.
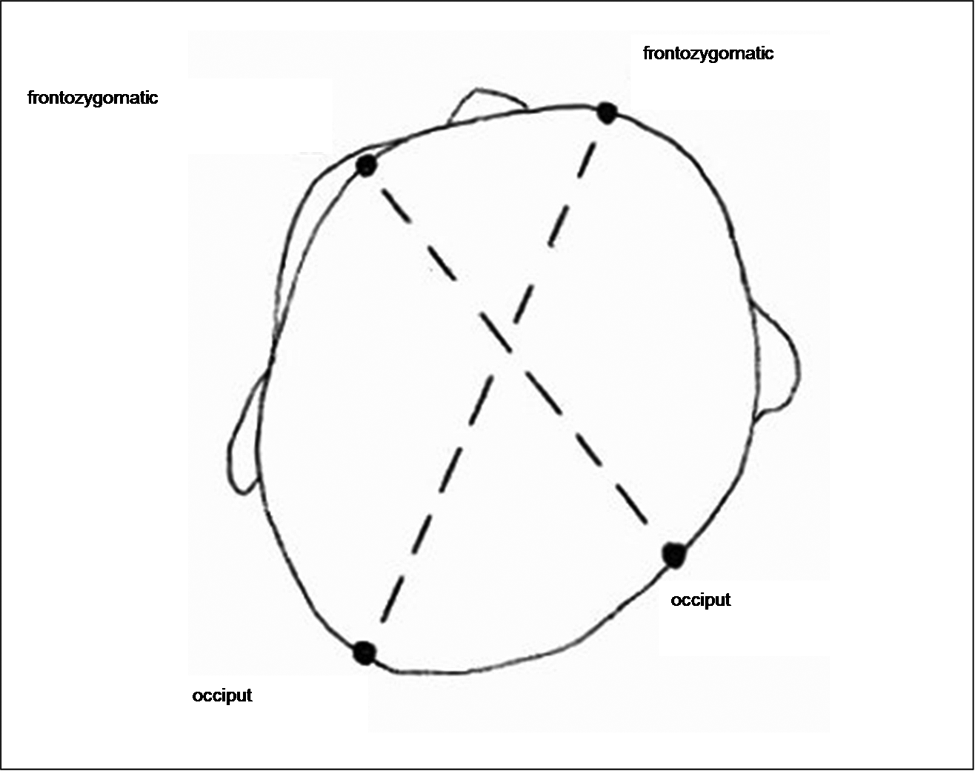
Transcranial diameter is the distance from the left frontozygomatic point to the oblique right occiput and from the right frontozygomatic point to the left occiput, as shown by the dotted lines above. 13
Estimates for the number needed to treat (NNT) were calculated using assumed prevalence rates for plagiocephaly and/or brachycephaly in infants from 20% to 40%. The no treatment retention rate was calculated as the prevalence rate in the total teenage study population divided by the decimal equivalent of the assumed prevalence rates of 20% to 40%. We also assumed that infants treated with a helmet would not have retention as adolescents. A second NNT estimate for abnormal facial characteristics due to retention of plagiocephaly and/or brachycephaly was calculated. Prevalence for nontreatment cases was calculated as (percentage retention) × (the percentage with abnormal facial characteristics among participants with plagiocephaly and/or brachycephaly). Prevalence for treated cases was equal to the prevalence for participants who did not have either plagiocephaly and/or brachycephaly. An NNT of 1 would mean that everyone improves with treatment and no one improves without treatment, whereas a higher NNT means a less effective treatment.
Results
A total of 1045 students agreed to participate in this study. Two students declined to participate; approximately 30 students forgot signed consent forms and could not participate. Participant ages ranged from 12 to 17 years, with a mean of 15.7 years (SD, 1.3). Girls made up 63.4% (663/1045) of the participants and outnumbered boys in this study since one of the participating schools was an all-girl school. Most of the participants were white (88.8%). The average oblique transcranial diameters (right frontal to left occiput, left frontal to right occiput) were the same at 17.4 cm.
The prevalence of plagiocephaly based on the >1-cm cranial vault asymmetry criteria was 0.9% (6/663) in girls and 1.6% (6/382) in boys (P = .37), with an overall prevalence of 1.1% (95% confidence interval [CI], 0.5%-1.8%). All cases of plagiocephaly occurred in whites.
The prevalence of brachycephaly was 0.8% (5/663) in girls and 1.3% (5/382) in boys (P = .51), with the overall prevalence of 1.0% (95% CI, 0.5%-1.6%). The prevalence in non-whites of 3.4% (4/117) is statistically greater when compared with the white prevalence of 0.6% (6/928; P = .018). The results are summarized in Table 1 .
Incidence of Plagiocephaly and Brachycephaly
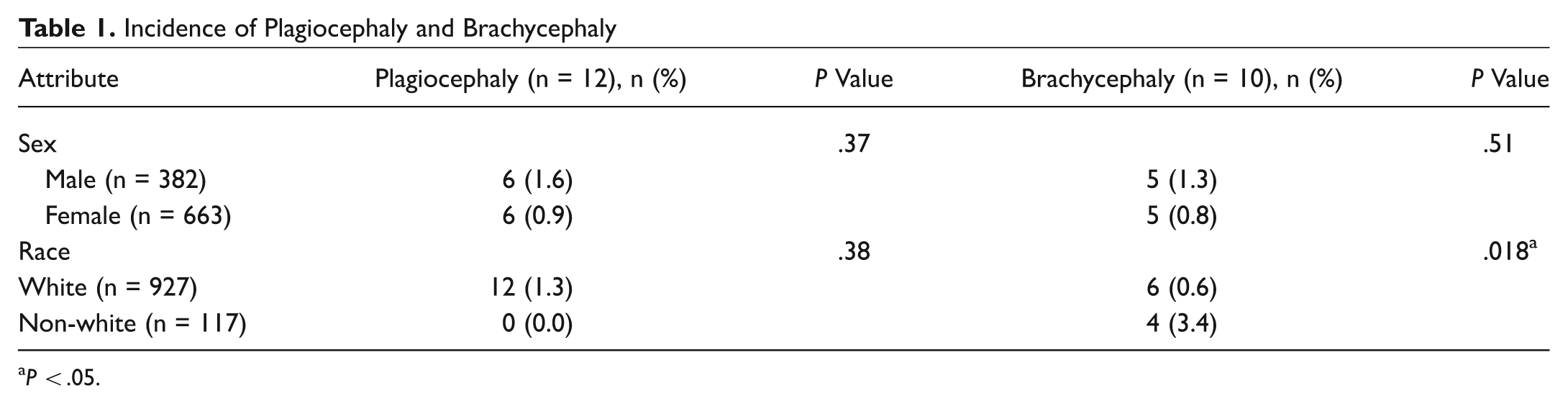
P < .05.
The overall prevalence of having a deformational cranial abnormality (either brachycephaly or plagiocephaly) was 2.0% (21/1045), with only 1 person meeting criteria for both diagnoses.
Abnormal facial characteristics were noted at the time of measurements and included narrow-set eyes, wide-set eyes, frontal prominence, flat nose, and low-set ears. These characteristics were based strictly on observation, and no facial analysis measurements were taken to make formal diagnoses. Of all the participants, 2.1% (22/1042) were noted to have an abnormal facial characteristic. Of the 21 participants with plagiocephaly and/or brachycephaly, 8 (38.1%) had abnormal facial characteristics compared with 14 of 1024 (1.4%) of those without this diagnosis (P < .001).
The number of infants needed to treat (NNT) for deformational cranial abnormalities is 10.0 if the prevalence in 6-month-old infants is estimated at 20% and the prevalence in teenagers is 2.0%, as shown in Table 2 . In simple terms, this calculation assumed that the prevalence decreased from 20% in infants to 2% in teenagers just by outgrowing the condition and that all infants treated with a helmet would have resolution of plagiocephaly. The NNT of 10 means that 10 infants diagnosed with plagiocephaly and/or brachycephaly would need to be treated with a helmet to prevent 1 teenager from having a persistent cranial abnormality.
Number Needed to Treat Based on Incidence Rates from 20% to 40%
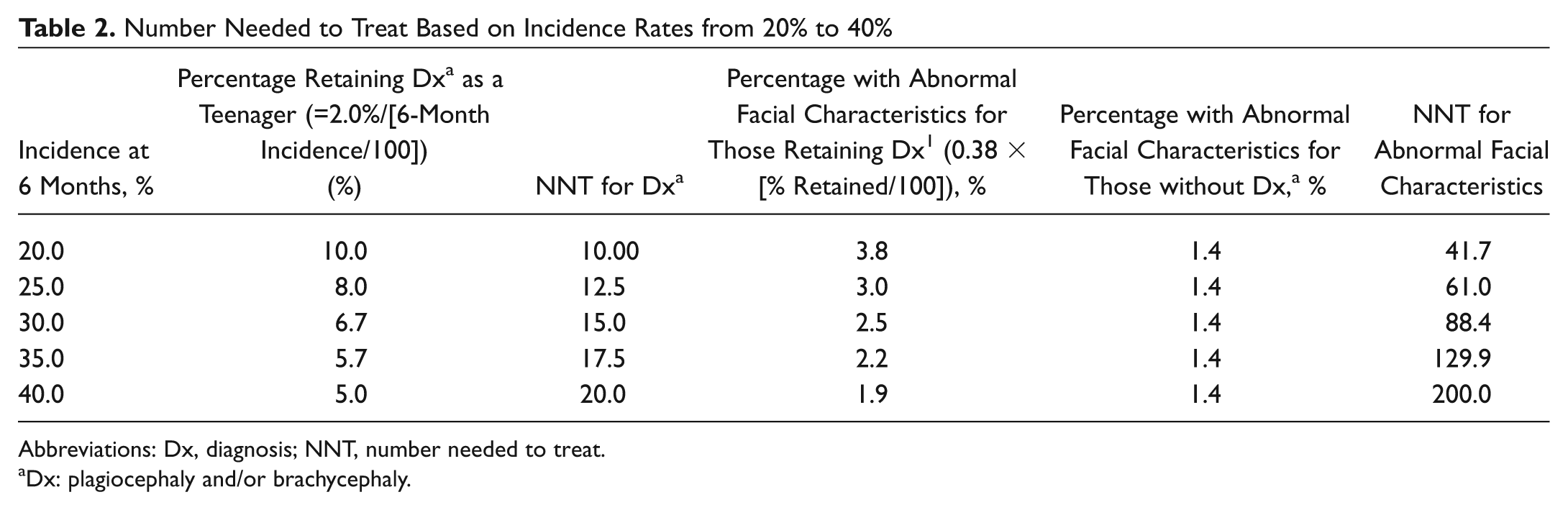
Abbreviations: Dx, diagnosis; NNT, number needed to treat.
Dx: plagiocephaly and/or brachycephaly.
When facial characteristics are taken into account, if the assumption is made that abnormal facial characteristics are a result of persistent plagiocephaly, the NNT for plagiocephaly to prevent development of abnormal facial characteristics is nearly 42, meaning that 42 infants with plagiocephaly and/or brachycephaly would need to be treated with a helmet to prevent 1 infant from having persistent cranial abnormalities that results in facial asymmetry as a teenager.
Discussion
The results of this study show an overall prevalence of plagiocephaly and brachycephaly of 2.0%, which is significantly lower than the prevalence in infants quoted in recent literature (20% to 50%).4-6 However, 2.0% is greater than the prevalence of plagiocephaly prior to the 1992 Back to Sleep campaign, which was 1 out of 300 (0.3%).6,12,16,17 The statistic of 1 out of 300 was based on studies on congenital torticollis, which is associated with positional plagiocephaly. 17 The criteria used in this study for diagnosing plagiocephaly was cranial vault asymmetry greater than 1 cm, which is used by most plagiocephaly clinics when determining which infants should get treatment.1,12 However, other sources have stricter criteria and consider normal cranial vault asymmetry less than or equal to 4 mm. Furthermore, some recommend the criteria for diagnosing brachycephaly to be cranial index <0.85, rather than the more commonly used 0.90, which is used in this study.1,18 Using these criteria, the prevalence in this study would have been closer to 8% rather than 2.0%. There is no literature or guidelines that advocate treating plagiocephaly for an asymmetry less than 1 cm. Most of the literature on plagiocephaly encompasses the diagnosis of brachycephaly, so for this discussion, they have been referred to as deformational cranial abnormality or just plagiocephaly. Although there were more girls than boys, the number of boys was well over 300, and the results were still statistically significant if only male participants were included.
There is an ongoing debate among craniofacial providers as to how best to treat deformational skull abnormalities. The conservative management strategy focuses on physical therapy and using frequent head position changes to keep the infant off of the flat spot. This includes increasing “tummy time,” avoiding spending too long sitting in a car seat, and physical therapy for infants with torticollis or who favor one side. The less-conservative treatment strategy focuses on liberal use of cranial orthotic devices. Cranial orthotic devices involve a specialized helmet that is readjusted every couple of weeks. The infants wear the helmet for 23 hours per day, for 3 to 9 months. 6 According to parental surveys, compliance with helmeting therapy has been found to be 85% to 90%. 16 Success rates of helmeting are generally favorable, with complete resolution of plagiocephaly in 60% to 90% of patients, to some studies just quoting that 100% of parents noted improvement in the appearance of their infant’s skull.13,16,19 The complication rate associated with helmeting therapy is low but includes contact dermatitis and pressure ulcers. 6
The arguments for helmeting therapy include the concern that if untreated, deformational plagiocephaly could persist into adulthood, resulting in noticeable head shape abnormalities. This could lead to teasing and poor self-esteem. 20 Studies have shown that at age 2 years, infants diagnosed with plagiocephaly who were not treated or treated only with conservative management still met the criteria for diagnosis. 19 This means that when the condition is diagnosed at age 4 to 6 months, it typically does not resolve spontaneously by age 2 years. However, until this present study, no one had evaluated whether deformational cranial abnormalities persisted into adolescence.
Arguments against helmeting therapy and focusing on conservative management include the fact that multiple studies have shown significant improvement in cranial abnormalities with repositioning and physical therapy. 6 Because of increased awareness, more infants are being referred to plagiocephaly clinics at younger ages, when improvement from conservative management is more likely. The cost of an orthotic helmet is estimated to be $1500 to $3000.14,15According to 2009 data from the Centers for Disease Control and Prevention, estimated births in the United States were just more than 1.13 million. 21 Based on previous data that 20% to 50% of infants meet criteria for plagiocephaly, 826,000 infants would be diagnosed each year using the lowest estimate of 20%. If all of those infants were helmeted, that would be a cost of more than $1 billion. However, as noted in the introduction, the estimated number of helmets prescribed as of 2004 was closer to 25,000 helmets/y. 10
The results of our data show that a small percentage, 2.0%, of the population has persistent deformational cranial abnormalities in adolescence. The NNT of 10 when simply taking into account plagiocephaly and brachycephaly shows that a significant number of infants must be treated with helmeting to prevent 1 adolescent from having persistent cranial abnormalities. One way to counsel parents on whether or not to treat with an orthotic device would be that their infant has a 10% chance of having persistent cranial abnormality if no orthotic device is prescribed.
Another significant finding of our study was the correlation between persistent deformational cranial abnormalities and abnormal facial characteristics. Cranial abnormalities described asymmetry of the skull itself, while abnormal facial characteristics were general observations made about the participant’s facial symmetry. Previous studies have shown that persistent plagiocephaly results in the development of abnormal facial characteristics. 6 The NNT of 42 when facial characteristics are taken into account indicates that a large number of infants must be treated with helmets to prevent 1 infant from having facial asymmetry in their adolescent years. It is important to note that most parents present to the plagiocephaly clinic with concerns that their infant will have persistent head abnormalities and are not focused on facial asymmetry. If parents are concerned about facial asymmetry, our data support counseling parents that their infant has an approximately 2% chance of having facial asymmetry develop and persist into adolescence if they do not treat the plagiocephaly. The high NNT indicates that if all infants who meet criteria for diagnosis of plagiocephaly are treated, there will be a significant number of infants who are treated unnecessarily.
There are some limitations to this study. This study showed that in the vast majority of cases, plagiocephaly and brachycephaly will have resolved by adolescence without helmeting therapy, but it did not determine the age at which this resolution takes place. It would be helpful to know the rate at which the abnormality resolves. The craniofacial provider would be better able to counsel parents if we knew when the head shape normalizes. Further research is warranted to help answer these types of questions. Another limitation is that no social history or past medical history was obtained from the participants, so it is unknown whether participants have risk factors for the development of plagiocephaly, such as the first born or premature birth, or whether the participant slept on his or her back, even though all were born after the Back to Sleep campaign began. While the method of obtaining anthropomorphic measurements has been validated in the past for diagnosing cranial abnormalities, there are arguments that other methods would give more accurate results. However, realistically, imaging scans could not be done on such a large scale. The abnormal facial characteristics were based on observation, without facial analysis measurements in order to make a formal diagnosis. While the purpose was to detect facial asymmetry that would be noticeable to the general public, there is no way to validate whether others would notice the same facial asymmetry as the lead researcher. A final limitation is that this study had to rely on the schools that were willing to participate in the study, which can affect the demographics of the study.
Conclusion
This is the first study to look at the incidence of plagiocephaly and brachycephaly in an older population born after the Back to Sleep campaign but before cranial orthotic devices were approved by the FDA. This study found that the incidence of plagiocephaly and brachycephaly that persists into adolescence is 2.0%. This is significantly lower than the 20% to 50% incidence seen in infants. The results of this study demonstrate that if all infants diagnosed with a deformational cranial abnormality are treated with helmeting, significant overtreating would be occurring since the problem does not persist into adolescence in a large majority of the cases. Further studies are warranted to determine the rate of spontaneous resolution, which infants diagnosed with plagiocephaly and brachycephaly should be treated aggressively, and which infants will likely achieve resolution with conservative therapy alone.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2011 AAO-HNSF Annual Meeting & OTO EXPO; September 11 to 14, 2011; San Francisco, California.