
Abstract
Objective
(1) Understand the epidemiology of obstructive sleep apnea (OSA) ambulatory office visits in the United States. (2) Quantify the prevalence of comorbid illnesses that are likely to occur in the setting of OSA.
Methods
From the 2008-2009 National Ambulatory Medical Care Surveys and National Hospital Ambulatory Medical Care Surveys, adult cases with a diagnosis of OSA were extracted. The epidemiology of OSA was determined. The prevalences of comorbid priority illnesses (obesity, asthma, cerebrovascular disease, depression, hypertension, and ischemic heart disease) were also determined.
Study Design
Cross-sectional analysis of a national survey database.
Setting
Ambulatory care settings in the United States.
Results
There were an estimated 4.1 ± 1.2 million annual visits with a diagnosis of OSA (60% ± 3.2% men; mean age, 56.4 ± 0.9 years). There were 419,000 ± 28,000 visits annually to otolaryngologists for OSA. Comorbid illnesses were obesity (23.8% ± 5.2%), asthma (14.3% ± 3.0%), cerebrovascular disease (2.5% ± 1.5%), depression (23.2% ± 2.6%), hypertension 53.8% ± 3.9%), and ischemic heart disease (10.3% ± 3.0%). Adjusting for age, sex, ethnicity, obesity, and race, statistically significant increased odds for the presence of obesity (3.6, P < .001), asthma (2.7, P < .001), depression (2.5, P < .001), and hypertension (2.0, P < .001) with OSA were noted. Increased odds for cerebrovascular disease and ischemic heart disease were not identified (P = .725 and P = .083, respectively).
Conclusion
Obstructive sleep apnea is a relatively common diagnosis in ambulatory and otolaryngologic care. It is associated with a significantly increased prevalence of several key priority health care conditions in the United States. Otolaryngologists and health care providers should be aware of these associations, understanding the potentially broad impact of OSA on general health.
Obstructive sleep apnea (OSA) is thought to affect approximately 3% to 7% of men and 2% to 5% of women in adulthood. 1 Aside from the well-known symptomatology of OSA, including daytime somnolence, decreased work productivity, and risk of motor vehicle accidents, OSA has also been associated with a higher prevalence of chronic, comorbid medical conditions. These are manifold and include hypertension, obesity, heart disease, cerebrovascular disease, and others. 2 With the current and anticipated obesity epidemic in the United States, OSA as a population diagnosis is strongly expected to increase in prevalence. 3
Otolaryngologists are often a key component of the OSA management team. Therefore, it is essential that otolaryngologists be aware of the associated medical comorbidities with OSA, as they affect treatment opportunities, treatment choices, and outcomes of therapy. However, the epidemiology of outpatient visits is relatively poorly understood, especially as it pertains to visits to otolaryngology–head and neck surgery. Otolaryngologists who diagnose and treat OSA must be familiar with its epidemiology and background medical conditions. Therefore, we sought to determine contemporary epidemiology of OSA with respect to office visits and to identify significant, comorbid conditions.
Methods
The study population was formed by the combined 2008 and 2009 National Ambulatory Medical Care Survey (NAMCS) and National Hospital Ambulatory Care Survey (NHAMCS). These annual surveys are conducted by the National Center for Healthcare Statistics, a branch of the Centers for Disease Control and Prevention. The data obtained are based on a national sample of visits to nonfederally employed office-based physicians who are primarily engaged in direct patient care (NAMCS) and on a national sample of visits to the outpatient departments of noninstitutional general and short-stay hospitals (NHMACS). These data sets are considered gold-standard data sets with respect to health care statistics in the United States. This study was reviewed by the Partners Human Studies Committee and deemed exempt from review.
From the combined 2008 and 2009 NAMCS and NHAMCS files, all coded outpatient visits for obstructive sleep apnea (International Classification of Diseases, Ninth Revision [ICD-9] code 327.23) were identified from the 3 allowed diagnosis fields, and then the cases were restricted to adult cases with age ≥18.0 years. Standard demographic information was tabulated, including patient age, sex, race, and ethnicity. Contained within each patient record are values for priority conditions that are explicitly queried at each office visit formally, rather than relying on diagnosis codes. Values for these priority conditions (obesity, asthma, cerebrovascular disease, depression, hypertension, and ischemic heart disease) were also extracted for each record. Data were imported into SPSS version 17.0 (SPSS, Inc, an IBM Company, Chicago, Illinois).
The presence of each of the priority conditions listed above was determined according to the presence or absence of a sleep apnea diagnosis. Next, a multivariate logistic regression model was constructed for each of the priority condition diagnoses above against the presence or absence of sleep apnea, controlling for age, sex, race, and ethnicity. Furthermore, for asthma, cerebrovascular disease, depression, hypertension, and ischemic heart disease, obesity was included as a covariate. Statistical significance was set at P = .05. Population statistics were deemed reliable if the relative standard error of the estimate was less than 30%.
Results
Among 897.9 ± 41.3 million adult office visits (annualized), 4.1 ± 1.2 million visits carried with them a coded diagnosis of obstructive sleep apnea. Table 1 presents the demographic characteristics of the overall population of patients’ office visits. Table 2 presents the demographics characteristics of patients with office visits with an accompanying diagnosis of OSA. There were an estimated 419,000 ± 28,000 annualized visits to otolaryngologists and surgical specialties. Therefore, otolaryngologists accounted for approximately 10% of OSA-related visits annually.
Demographic Characteristics of the Overall Visit Population
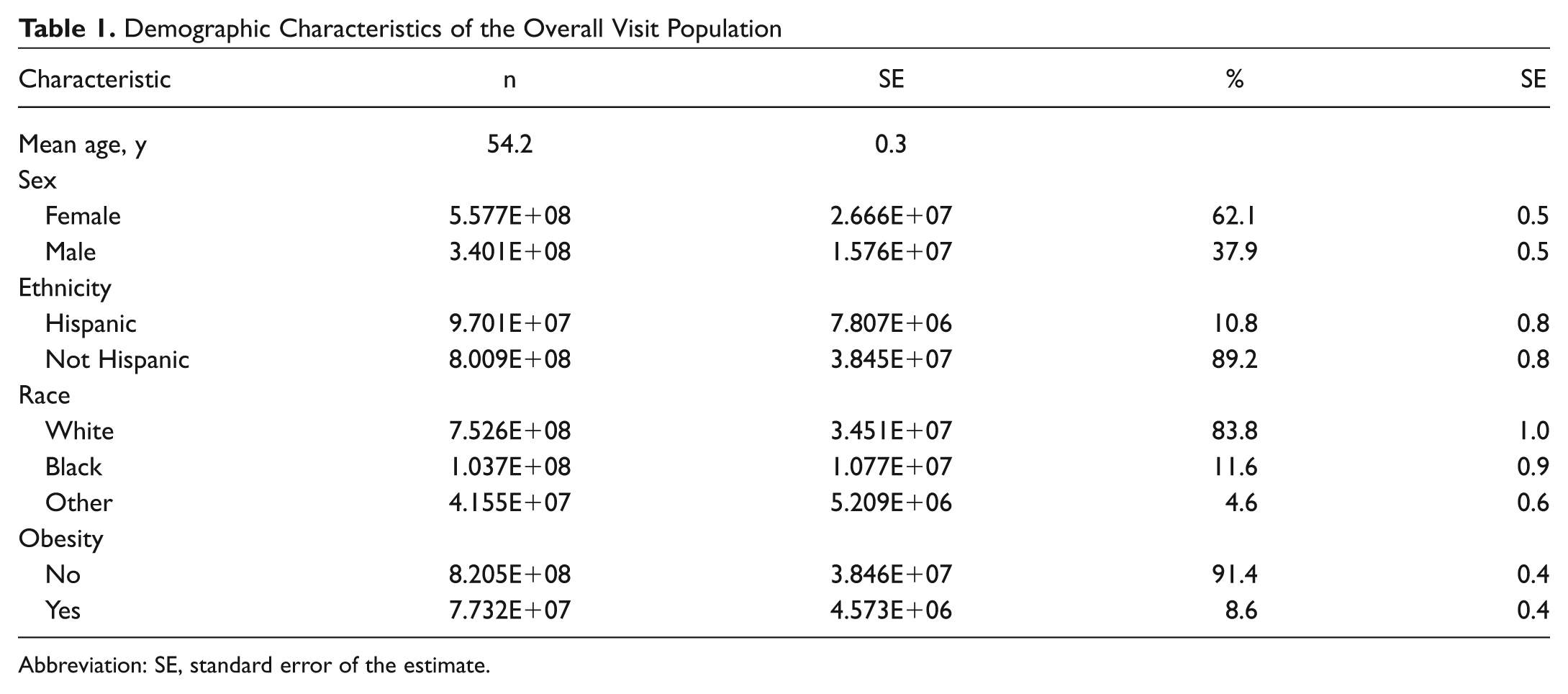
Abbreviation: SE, standard error of the estimate.
Demographic Characteristics of the Visit Population with Obstructive Sleep Apnea
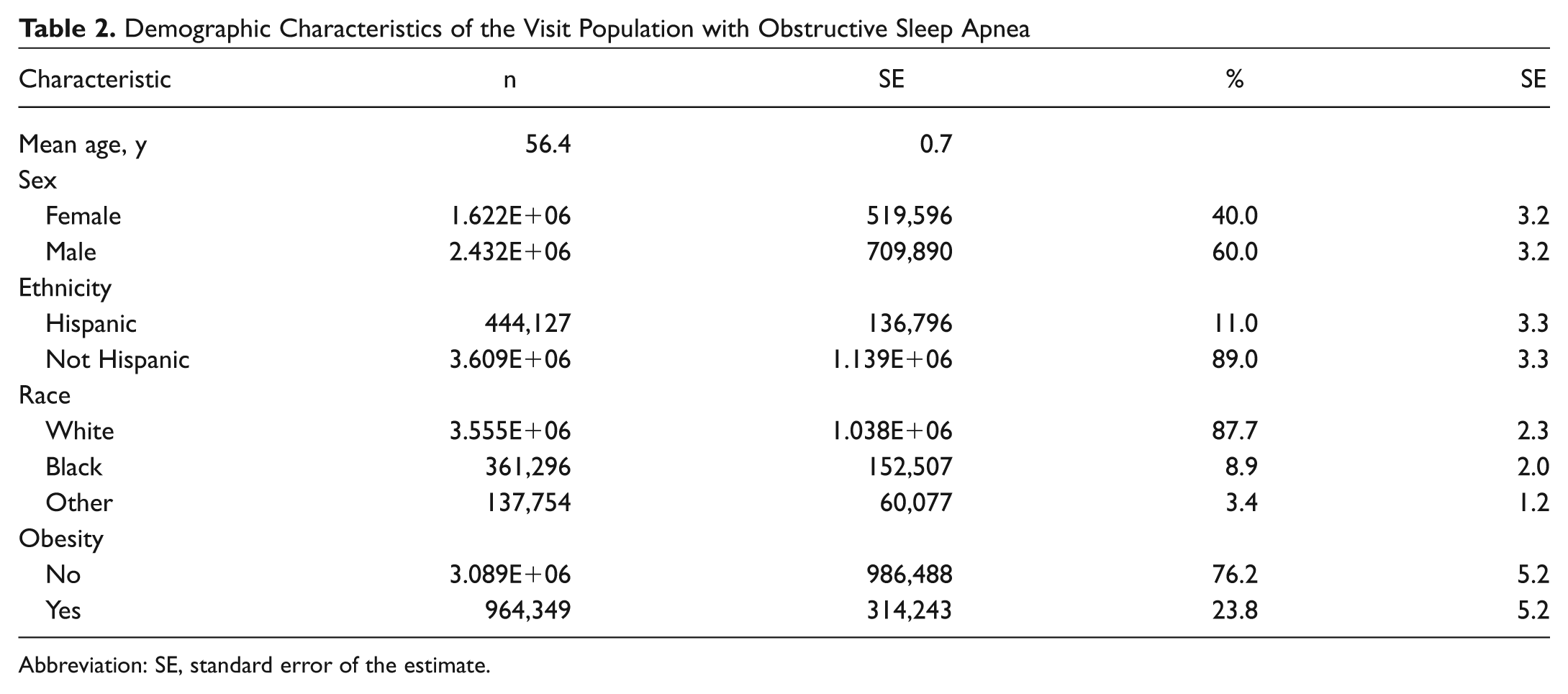
Abbreviation: SE, standard error of the estimate.
Table 3 presents the results for the medical conditions associated with OSA. Obesity was significantly associated with an OSA diagnosis (P < .001). Among the screened for priority medical conditions, asthma, depression, and hypertension were each significantly associated with an OSA diagnosis (all P < .001), while adjusting for obesity, age, sex, race, and ethnicity. The odds for asthma, depression, and hypertension each more than doubled in the presence of an OSA diagnosis.
Comorbid Disease Prevalence among US Adults with and without Obstructive Sleep Apnea (OSA)
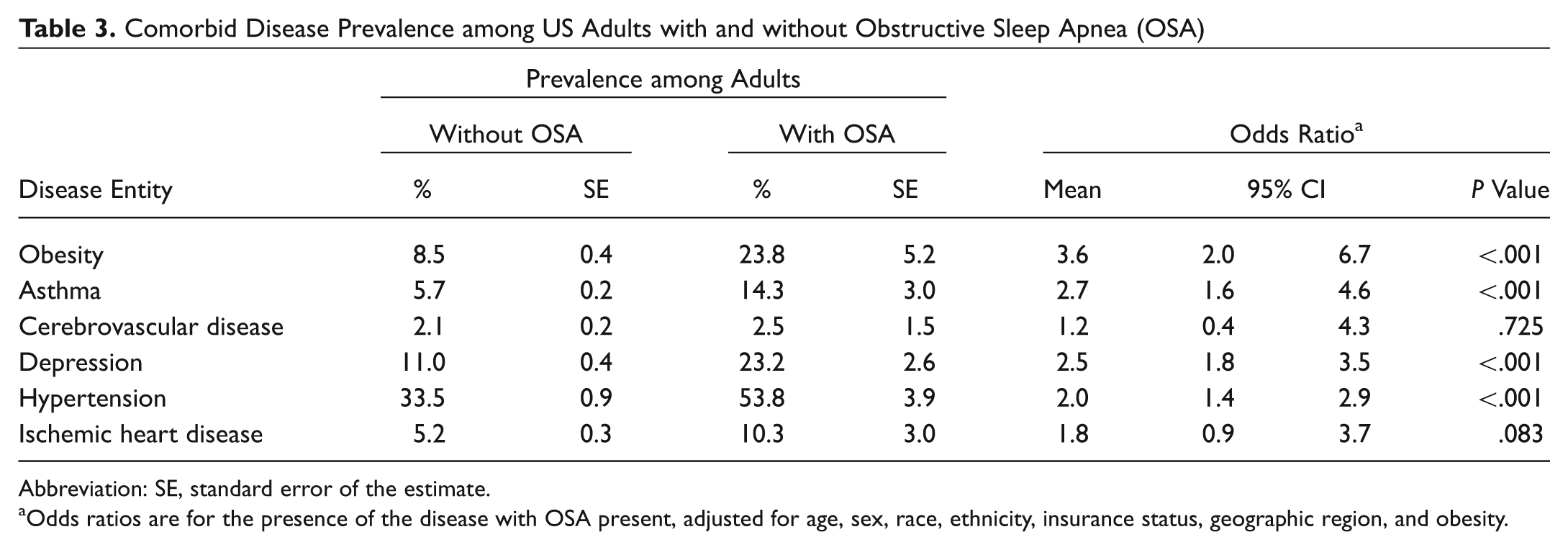
Abbreviation: SE, standard error of the estimate.
Odds ratios are for the presence of the disease with OSA present, adjusted for age, sex, race, ethnicity, insurance status, geographic region, and obesity.
Discussion
This study represents a novel epidemiologic study at the national level regarding the ambulatory visit diagnoses of OSA, visits to otolaryngologists, and comorbid medical conditions associated with the diagnosis of OSA. Increasingly, physicians and patients are becoming aware of the symptoms, diagnosis, and health implications of OSA. In fact, with the aging and increasing obesity of the US population, it has been surmised that there will be an epidemic of OSA in the upcoming years. 3
Several key points elucidated by the data merit mention. First, otolaryngologists are seeing only a small fraction of OSA diagnoses, approximating only 10%. Although it is expected and true that OSA is more commonly diagnosed by primary care physicians, pulmonologists, and neurologists, otolaryngologists are often involved in the spectrum of care, especially when it comes to surgical consideration. In fact, otolaryngologists are uniquely poised to not only diagnose OSA but also discuss and offer various treatments, both surgical and nonsurgical, for OSA. Given the relatively low otolaryngology penetration into the epidemiology of OSA diagnoses, further investigation as to potential barriers to access to care may be warranted.
Not surprisingly, we found a number of significant associations between notable medical comorbidities and the presence of OSA as a diagnosis. First, these data confirm at a national level that obesity in adults is strongly associated with an OSA diagnosis. This also further reinforces the impact that increasing trends toward obesity in the United States is likely to have on the prevalence of OSA in the near future. Given the seriousness of an OSA diagnosis and the associated costs of both surgical and nonsurgical treatment of OSA, considerable emphasis on obesity control in the US health care system is likely warranted. For example, recent data have indicated that for those patients significantly obese, bariatric surgery may significantly reduce the apnea-hypopnea index in OSA. 4 However, such surgery is not consistently curative of OSA, and therefore obesity prevention is much more desirable. 4
In this population-based analysis, we found significant increased odds ratios for the presence of asthma, depression, and hypertension with an OSA diagnosis. Asthma and OSA are both airway disorders, and investigators have long posited a significant relationship between these 2 airway diseases. For example, many triggers for asthma are also thought to be significant triggers for worsening of OSA. 5 Other smaller, case-control studies have demonstrated an association between OSA and asthma, including a higher rate of asthma exacerbations in patients with OSA.6,7 Similarly, other case-control studies have demonstrated significant relationships between hypertension and OSA. In fact, untreated OSA is felt to be a significant cause of refractory hypertension.8,9 The addition of continuous positive airway pressure (CPAP) therapy will in turn often lead to better hypertensive control. 10
Finally, we noted a significant association between depression and OSA, with approximately one-fourth of those patient visits with an OSA diagnosis also having depression ( Table 1 ). The rate of depression in the setting of OSA varies widely in the literature from 7% to 63% depending on method of depression assessment. 11 Our data confirm published cohort data in Swedish patients that indicate a prevalence of depression based on Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnostic criteria of 23%.11,12 The current data represent the first nationally based population estimate of the incidence of depression among patients with OSA in the United States.
Several limitations of the current analysis merit mention. First of all, the selection of OSA patients/visits was dependent on ICD-9 coding. In such studies, it is always possible that there existed patients with OSA who were not coded and also patients erroneously coded within the database. Furthermore, we chose an extremely strict single diagnosis code for OSA and therefore may have missed some cases coded with other more general sleep-disordered breathing codes. However, previous studies have verified a relatively high level of diagnostic accuracy in the coding schema of the NAMCS. 13 Second, our method analysis highlights an association between OSA and the study comorbid diagnoses. However, this should not be taken to imply actual causation. Regardless, otolaryngologists should be aware of these associations, as they may influence surgical risk (eg, asthma, hypertension), influence quality of life/compliance with therapy (eg, depression), and help provide a more rounded therapeutic plan for their patients with OSA. Finally, one should not take the current office visit figures to represent the epidemiology of the diagnosis of OSA in the general population; rather, this is an analysis of the epidemiology of office visits, and therefore the denominator is different than the general population. As such, approximately 0.5% of ambulatory office visits carried a diagnosis of OSA and should not be misinterpreted as a 0.5% prevalence of OSA among persons. Similarly, the obesity figures derived their numbers based on office visits and not the general population.
Conclusion
Currently, approximately 10% of OSA ambulatory health care visits are associated with otolaryngologic care. The diagnosis of OSA is associated with a higher prevalence of priority conditions in adults in the United States, including obesity, hypertension, asthma, and depression. Further study will be required to better understand these relationships and to monitor the prevalence of these conditions in the face of an aging and increasingly obese US population.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article will be presented at the 2012 AAO-HNSF Annual Meeting and OTO EXPO; September 9-12, 2012; Washington, DC.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.