
Abstract
Clinical practice guidelines (CPGs) have become increasingly important in recent years due to an increasing emphasis on evidence-based practice, as well as serious discussions in academic, medical, and legal circles about their possible role in measuring physician performance, setting provider reimbursement strategy, and establishing protection from litigation in the future. At the same time, CPGs are costly to develop. Thus, as CPGs gain influence in medical practice, it will become essential that CPGs are developed using trustworthy standards and that the authors of CPGs are not being unduly influenced by financial pressures from external stakeholders. Since 2004, the 9 CPGs sponsored by the American Academy of Otolaryngology—Head and Neck Surgery Foundation have been developed with full disclosure and appropriate management of potential financial conflicts of interest. This commentary discusses the potential for conflict of interest in otolaryngology CPGs and how the otolaryngology guideline development process can serve as a model for other professional medical organizations.
Keywords
For-Profit Industry Presence in Clinical Practice Guidelines
One aspect of a trustworthy clinical practice guideline (CPG) is that it is characterized by an extensive systematic review by content experts, methodologists and researchers, patients and their advocates, and other stakeholders, which is then endorsed by one or more professional organizations. Thus, despite what one’s opinion of the use of CPGs in medicine might be, it is difficult to argue that the CPG lacks influence in the contemporary health care paradigm. Even though consistent CPG adherence has yet to be used as a metric for physician performance on a national scale, an incentive for reimbursement, or even as a defense against litigation, such possibilities may theoretically become reality in the future.
Given the singular influence CPGs are gaining over medical practice, we should be mindful of which stakeholders other than patients stand to benefit the most from CPG implementation. For guidance, consider the 2011 Institute of Medicine (IOM) report Clinical Practice Guidelines We Can Trust. The language of the first 2 items in the checklist—establishing transparency and management of conflict of interest—quite clearly demonstrate that the IOM is greatly concerned about the influence of for-profit industry interests on the development of CPGs. 1
During the 2013 fiscal year, the American Academy of Otolaryngology—Head and Neck Surgery Foundation (AAO-HNSF) spent $450,000 on its CPG and consensus statement program. This translates to about $100,000 to $120,000 per guideline, including approximately $30,000 for 2 in-person meetings and 3 teleconferences, $75,000 for staffing (including a staff liaison and external search strategist), and $10,000 to $20,000 for purchasing articles, printing, and indirect costs. The costs of AAO-HNSF guideline development, which are covered by the organization’s operational budget, are significantly less than the $200,000 to $800,000 per guideline estimate provided by the IOM over 2 decades ago. 2 For professional organizations without the money to sponsor guideline development, industry support is one way of overcoming this barrier, but obtaining funding from commercial entities carries its own risks and tradeoffs. From an industry perspective, investment in CPG development may be much like investment in any other tangible product, involving close supervision of research design, data collection and analysis, and publication of results. In select cases, it may be in the form of an unrestricted educational or research grant, where the investor has no control over how the funding is used and/or no knowledge of the final CPG content until after publication. While corporate involvement should not necessarily be interpreted as the sign of a poor-quality product, no study has been undertaken evaluating the methodological quality of CPGs based on industry support or the impact of industry conflict of interest (COI) on guideline recommendations. 3 There is also no literature on the prevalence of guideline funding models across specialties. 4
Given that for-profit industries have been shown to influence everything from prescription patterns and hospital formulary development to favorable scientific publication patterns, 5 COI reporting trends in CPG development are an important consideration. The interactions between guideline authors and for-profit commercial entities are highly complex, and although nonfinancial pressures such as intellectual bias resulting from the desire for career advancement or professional accolades do exist, most research to date has studied financial COI, which is somewhat easier to characterize.
Observations from Otolaryngology Guidelines
I examined the 9 CPGs formally sponsored by the AAO-HNSF in order to determine the state of CPG development and COI reporting in our specialty. The guideline funding source, number of authors declaring for-profit industry relationships, and number of companies disclosed are listed in Table 1 . I disregarded the American Society of Anesthesiologists operating room fire management practice advisory and the 3 AAO-HNSF clinical consensus statements since they were produced using a different methodological process.
Funding and conflicts of interest reported by authors of clinical practice guidelines developed by the American Academy of Otolaryngology—Head and Neck Surgery Foundation.
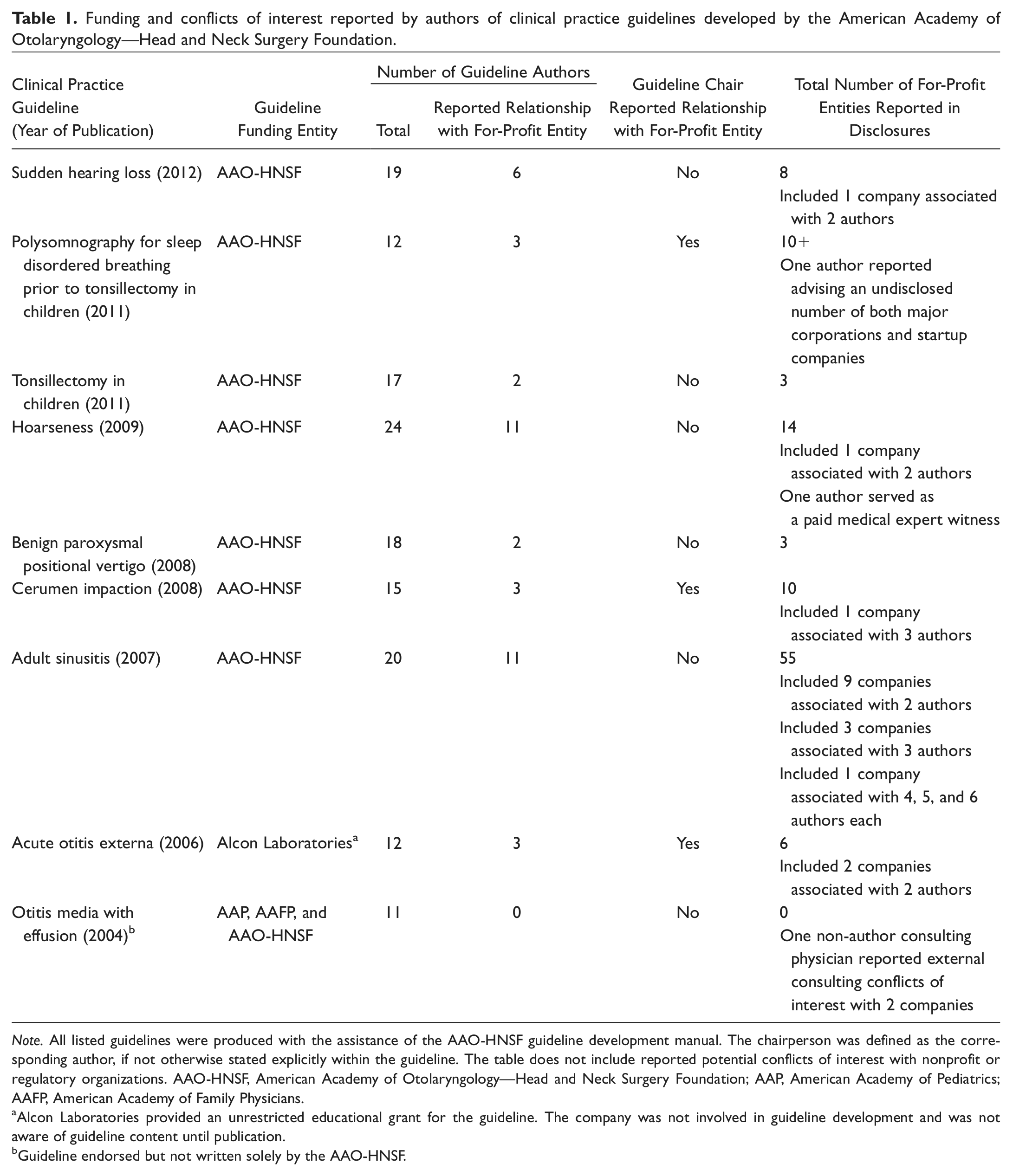
Note. All listed guidelines were produced with the assistance of the AAO-HNSF guideline development manual. The chairperson was defined as the corresponding author, if not otherwise stated explicitly within the guideline. The table does not include reported potential conflicts of interest with nonprofit or regulatory organizations. AAO-HNSF, American Academy of Otolaryngology—Head and Neck Surgery Foundation; AAP, American Academy of Pediatrics; AAFP, American Academy of Family Physicians.
Alcon Laboratories provided an unrestricted educational grant for the guideline. The company was not involved in guideline development and was not aware of guideline content until publication.
Guideline endorsed but not written solely by the AAO-HNSF.
As mandated by the AAO-HNSF guideline development manual, all participating authors are required to disclose COI, including “none” if there were no relevant relationships. There was an average of 16.4 authors per guideline, with approximately 4.6 (27.7%) authors per guideline reporting at least 1 for-profit industry-related COI. Thus, the remaining 72.3% of authors specifically had no COI to report. The range of industry-related disclosures was almost universally financial, including direct employment, directorship, or consultancy; membership in a speakers’ bureau or advisory board; research grants; and stock ownership. Unfortunately, obtaining an accurate estimate of the number of reported industry affiliations per author was not possible due to occasional nonspecific disclosure statements (eg, “scientific/medical adviser to major corporations [ie, WebMD, BASF, NFL, MLB], and several startup companies”).
Alcon Laboratories, which specializes in ophthalmic and otic products, was declared as an industry relationship at least once in 6 of the 9 (66.7%) guidelines, highest among all reported firms. Of these 6 guidelines, 1 specifically mentions products sold by Alcon (ciprofloxacin-dexamethasone and ciprofloxacin-hydrocortisone for acute otitis externa), 2 cover other medical conditions of potential interest (otitis media with effusion and cerumen impaction), and the remaining 3 appear to be outside of the scope of Alcon’s interests. The adult sinusitis CPG from 2007 reported the highest number of authors with potential COI (11 of 20, 55%). Three of the 11 authors reported current or previous industry employment, while a sizable 55 companies were represented overall, including 8 of the top 10 largest global pharmaceutical firms by 2012 market capitalization (Pfizer, Merck & Co, Novartis, GlaxoSmithKline, Abbott Laboratories, Sanofi-Aventis, Bristol-Myers Squibb, and AstraZeneca). Fifteen firms had relationships with multiple authors disclosed, led by Merck with 6 authors.
Future Directions
I highlighted the adult sinusitis CPG not as an indictment, but simply to measure progress in guideline development and demonstrate that COI cannot be adequately managed until it is fully disclosed. In the most recent version of the AAO-HNSF guideline development manual, instructions are provided for not only appropriate COI disclosure (eg, “[authors’] role is to declare, not interpret”) but also COI management. This process occurs even before authors begin formally identifying evidence. 6 However, reporting of author COI is currently the exception rather than the rule in medical guidelines. A systematic review of CPGs by Norris et al found that as little as 3.7% of guidelines disclosed authorship COI. 3 This may be the result of inconsistently defined and applied systematic rules on COI reporting in guidelines, which across professional, governmental, and health care provider organizations frequently do not meet even a single criterion for COI disclosure as defined in Clinical Practice Guidelines We Can Trust. 7
Just over one-quarter of the authors of the 9 AAO-HNSF–endorsed guidelines had any for-profit industry disclosures. In contrast, 18 of the 20 (90%) authors of 3 major guidelines sponsored by the American Psychiatric Association had undisclosed financial associations with companies whose products were either being considered or included in the guidelines being authored. 8 One-third of the otolaryngology guidelines were chaired by an individual with declared for-profit industry COI, compared to 81% of the chairs of cardiovascular guideline panels. 9 Finally, just 1 of the otolaryngology CPGs (acute otitis externa) received direct industry funding, and this was provided in the form of an unrestricted educational grant without any other involvement in development or industry awareness of content until guideline publication.
Several questions remain unanswered. Is a guideline with over half of the authors reporting potential conflicts with 55 for-profit industrial firms more likely to be influenced than a guideline with, say, 10% authorship with industry COI, and in what aspects? Do certain types of relationships leave researchers more prone to bias during CPG development compared to others, for example stock ownership versus unrestricted research grant support? It is easy to simply count the number of relationships a CPG writer has with industry, far harder and more controversial to establish a threshold number and admixture of industry relationships correlating with consequential impact upon CPG development. As Bekelman et al 10 have shown, there are many instances of financial COI with commercial interests affecting investigator behavior and research conclusions, but few practical solutions for mitigating impact. Surveys determining what types of industry relationships are considered more “high risk” for bias compared to others might be an appropriate initial step toward clarifying the situation further.
Even if guideline writers were able to divorce CPG development from direct industry funding, is it possible to adequately control its influence when it appears through indirect means like advisory board membership? One of several proposals that have been considered is the exclusion of any and all industry-affiliated physicians from CPG development, which might omit some content experts with otherwise stellar qualifications for evaluating evidence and leading guideline development. 11 In order to lessen this risk, Rothman et al offer the unique solution of circulating guideline drafts widely to individuals with and without industry backing for comment but leaving the final version to be approved solely by non–industry-supported professionals. 11
The AAO-HNSF guideline development manual clearly describes how to properly disclose and manage potential COI. However, other select organizations such as the American Academy of Dermatology (AAD) 12 and the American College of Chest Physicians (AACP) 13 improve on this by including discrete flowcharts in their own manuals on the process for reporting and managing COI, an inclusion that the AAO-HNSF should consider for the next iteration of the guideline development manual. For organizations without the means to produce an internal CPG development manual, both the IOM report Clinical Practice Guidelines We Can Trust 1 and the Guidelines International Network 14 are excellent starting resources.
Ultimately, while developing a systematic process for guideline development may be a logical initial step for all professional organizations, there are few available choices for acquiring funding to produce guidelines. Ever since political machinations nearly eliminated the Agency for Health Care Policy and Research (now known as the Agency for Healthcare Research and Quality) in 1995, the US federal government has avoided directly funding CPGs and instead now serves as a repository of guidelines through the National Guideline Clearinghouse. 15 The AAO-HNSF primarily uses internal funding to support guideline development, with the single exception of an unrestricted grant to support the 2006 acute otitis externa guideline. However, this financial model is not necessarily viable for other professional societies with fewer resources. Many for-profit entities such as pharmaceutical companies, medical device manufacturers, and insurers have substantial resources to support guideline development, but unacceptable financial motivations may well be introduced into the guideline process. In fact, certain organizations such as the Cochrane Collaboration have a written policy that prohibits for-profit industry support for their research.
Conclusions
Efforts to reduce industry COI during the process of CPG development are commendable, and the otolaryngology community may be poised to become a model for how guidelines can be manufactured with both complete disclosure and appropriate management of COI. As stakeholders in medical care, for-profit industrial firms do deserve representation. However, only through full disclosure can all parties be made fully aware of the complex relationships between individuals and for-profit industry and that the financial motivations of commercial businesses sometimes may place their long-term goals at odds with clinicians, patients, and other groups. Furthermore, management of industry COI can only be accomplished through complete disclosure of all relevant relationships. It is clear that more work is necessary to not only report and manage COI in CPG development thoroughly, but also to determine the quantitative and qualitative impact of for-profit influences on the quality and outcomes of guideline production.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.