
Abstract
Objective
Conventional computed tomography (CT) imaging is the standard imaging technique for temporal bone diseases, whereas cone-beam CT (CBCT) imaging is a very fast imaging tool with a significant less radiation dose compared with conventional CT. We hypothesize that a system for intraoperative cone-beam CT provides comparable image quality to diagnostic CT for identifying temporal bone anatomical landmarks in cadaveric specimens.
Study Design
Cross-sectional study.
Setting
University tertiary care facility.
Subjects and Methods
Twenty cadaveric temporal bones were affixed into a head phantom and scanned with both a prototype cone-beam CT C-arm and multislice helical CT. Imaging performance was evaluated by 3 otologic surgeons and 1 head and neck radiologist. Participants were presented images in a randomized order and completed landmark identification questionnaires covering 21 structures.
Results
CBCT and multislice CT have comparable performance in identifying temporal structures. Three otologic surgeons indicated that CBCT provided statistically equivalent performance for 19 of 21 landmarks, with CBCT superior to CT for the chorda tympani and inferior for the crura of the stapes. Subgroup analysis showed that CBCT performed superiorly for temporal bone structures compared with CT. The radiologist rated CBCT and CT as statistically equivalent for 18 of 21 landmarks, with CT superior to CBCT for the crura of stapes, chorda tympani, and sigmoid sinus.
Conclusion
CBCT provides comparable image quality to conventional CT for temporal bone anatomical sites in cadaveric specimens. Clinical applications of low-dose CBCT imaging in surgical planning, intraoperative guidance, and postoperative assessment are promising but require further investigation.
Keywords
The goal of temporal bone surgery in patients with acute or chronic ear disease is to achieve a dry ear with preservation or improvement of hearing. Besides a thorough understanding of the anatomy and dissection techniques, accurate imaging is required not only for diagnostic purposes but also to aid in surgical planning and postoperative follow-up.
In current practice, otologic surgeons and radiologists specialized in head and neck imaging use helical multislice computed tomography (CT) scans for diagnosis, preoperative planning, and follow-up visits. Recent studies have shown that cone-beam CT (CBCT) is a reliable technique for imaging of small distinct areas with significantly less radiation dose per investigation as compared with conventional CT.1-3 A literature review of the use of CBCT in head and neck applications shows a number of studies determining the efficacy in dental and maxillofacial diagnostics.4,5 Application of this technology in head and neck imaging and temporal bone imaging is developing.6-8 Our research group has developed an integrated image-guided system, the individual components of which includes a high-performance mobile C-arm–based CBCT, deformable image registration, and 3D visualization software allowing near real-time image acquisition with surgical instrument guidance and tracking.9-11
To date, helical CT remains the gold standard for temporal bone imaging due to the superior image quality of bony structures. Over the past several years, our group has demonstrated the feasibility of CBCT imaging in the evaluation of the middle and inner ear. We have found that CBCT provides sufficient spatial accuracy for intraoperative usage during temporal bone surgery.12,13 The aim of this study is to investigate the imaging performance of CBCT with a cadaveric temporal bones model in comparison with conventional multislice helical CT. This preclinical study serves as an essential step in investigating the clinical feasibility of using CBCT for preoperative planning, intraoperative surgical guidance, and postoperative follow-up for patients with acute and chronic ear disease. This study involves a customized questionnaire that evaluates image quality in temporal bone landmark identification tasks for 21 anatomical structures in the (1) external ear canal, (2) middle ear, (3) inner ear, and (4) temporal bone. Three experienced otologic surgeons and 1 head and neck radiologist reviewed both CBCT and conventional CT images of the temporal bone. The questionnaires were provided at the end of each image review session to evaluate the visibility of specific landmarks. The collected questionnaires were then statistically analyzed by our institution’s biostatistician.
Materials and Methods
Temporal Bone Specimens and Imaging Phantom
Twenty cadaveric temporal bones were acquired from the Division of Anatomy, University of Toronto, in compliance with the Anatomy Act of Ontario and Institutional Research Ethics Board protocols. To provide clinically realistic imaging characteristics (eg, dose, scatter), each sectioned temporal bone (right or left) was placed within a custom head phantom, as shown in Figure 1 . The phantom consists of sections of an anthropomorphic head imaging phantom (RANDO, The Phantom Laboratory, Salem, NY) and a central acrylic section with 2 compartments, and it is similar to the effect of a “normal head” on radiation dose, image resolution, and scatter. Each compartment can hold either an acrylic block or a sectioned cadaveric temporal bone. During imaging, a single temporal bone is placed within either the left or right compartment, and the remaining compartment houses an acrylic block. Each specimen was imaged within the phantom by both CBCT and multislice CT, as described below.
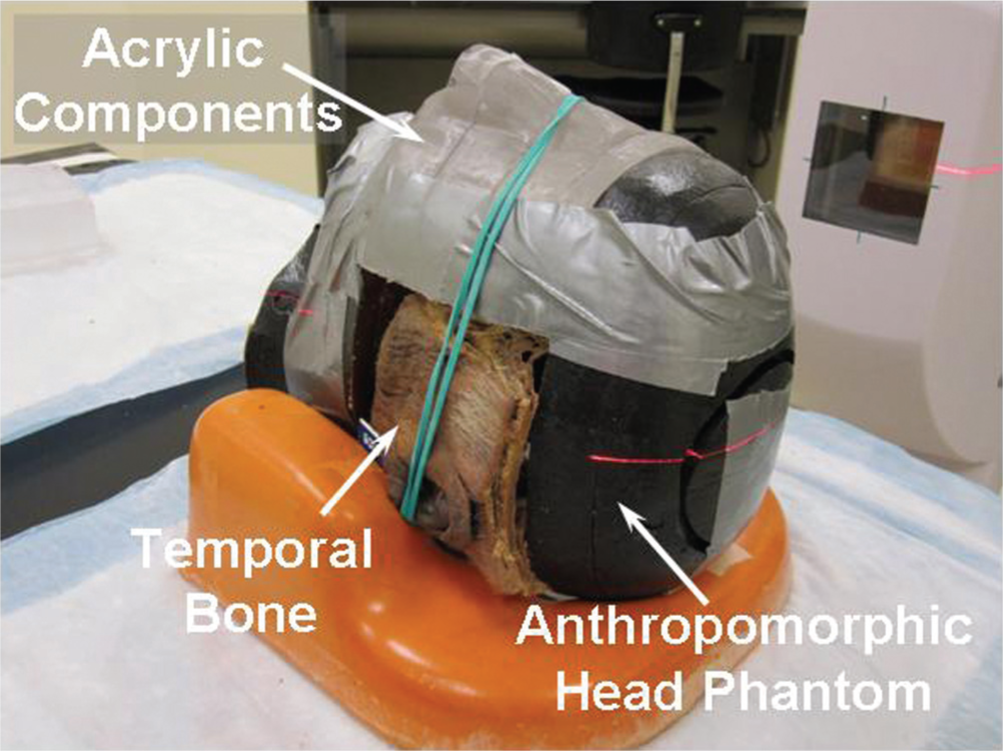
The head phantom was designed to fit a cadaveric temporal bone, and the shelf of the temporal bone corresponds to the surface anatomy of the head.
CBCT Imaging
As shown in Figure 2 , a prototype mobile C-arm for intraoperative CBCT was developed in collaboration with Siemens Healthcare (Erlangen, Germany). Key modifications include a flat-panel detector (Paxscan 4030CB, Varian, Palo Alto, CA), motorized orbit, method for geometric calibration, and software control system. Volumetric images with a field of view of ~20 × 20 × 15 cm3 are reconstructed within ~15 seconds of scan completion (~1 minute acquisition). For this study, an isotropic voxel size of 0.4 mm3 was used to generate image volumes of (512 × 512 × 384) voxels. The radiation dose per scan is ~10 mGy (~0.35 mSv) to a dosimetry head phantom at 100 kVp and 170 mAs, relatively low in comparison to a typical 2- to 5-mSv diagnostic head CT. 10 In the context of temporal bone imaging, the image quality of CBCT at this radiation dose has been validated during cadaveric experiments involving temporal bone dissection, 12 ossicular reconstruction, 14 and cochlear implantation 15 and patient imaging studies in the operating room. 7
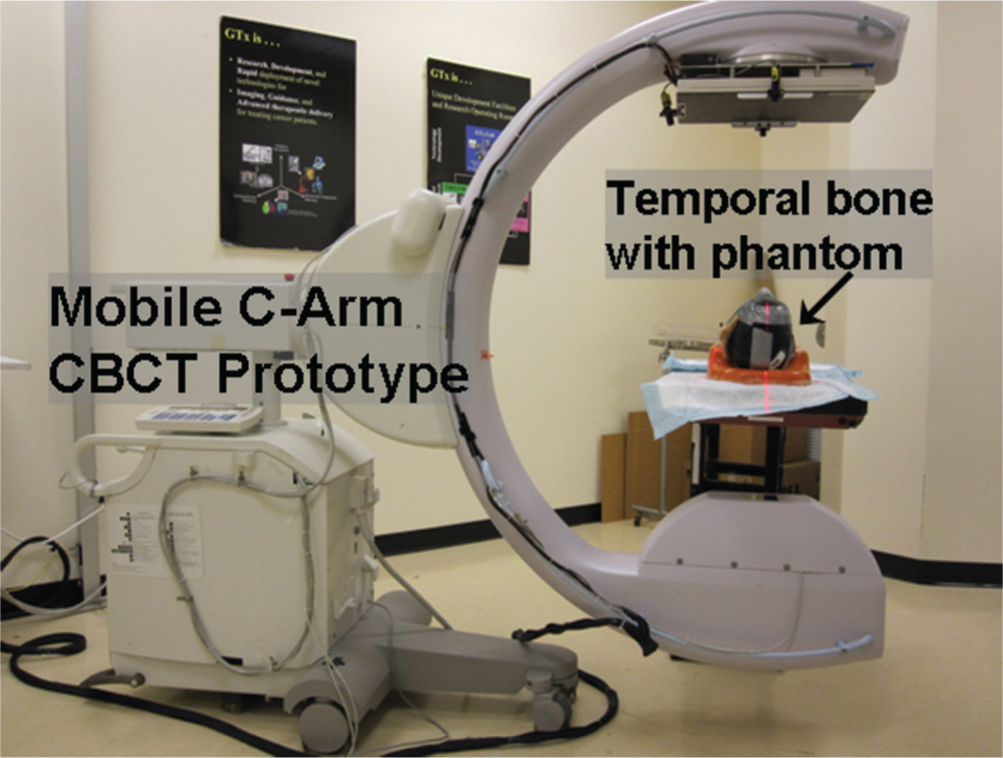
Mobile C-arm for cone-beam computed tomography imaging used for temporal bone imaging.
Multislice CT Imaging
Conventional CT images were acquired with an Aquilion 64 (Toshiba, Tokyo, Japan) using institutional temporal bone-scanning protocols ( Figure 3 ). The imaging technique of 120 kV, 260 mA, 0.5 seconds, and 220-mm display field of view was applied. The acquired images had a resolution of 512 × 512 pixels with a pixel size of 0.5 mm2 and a slice thickness of 0.5 mm. To maximize the visibility of tissue-specific structures and anatomy, 3 different filter convolutions (FCs) were applied: bone high resolution (FC81) for smoothing and edge enhancement, bone sharp (FC31) for edge enhancement only, and head soft tissue (FC03) for enhanced tissue contrast.
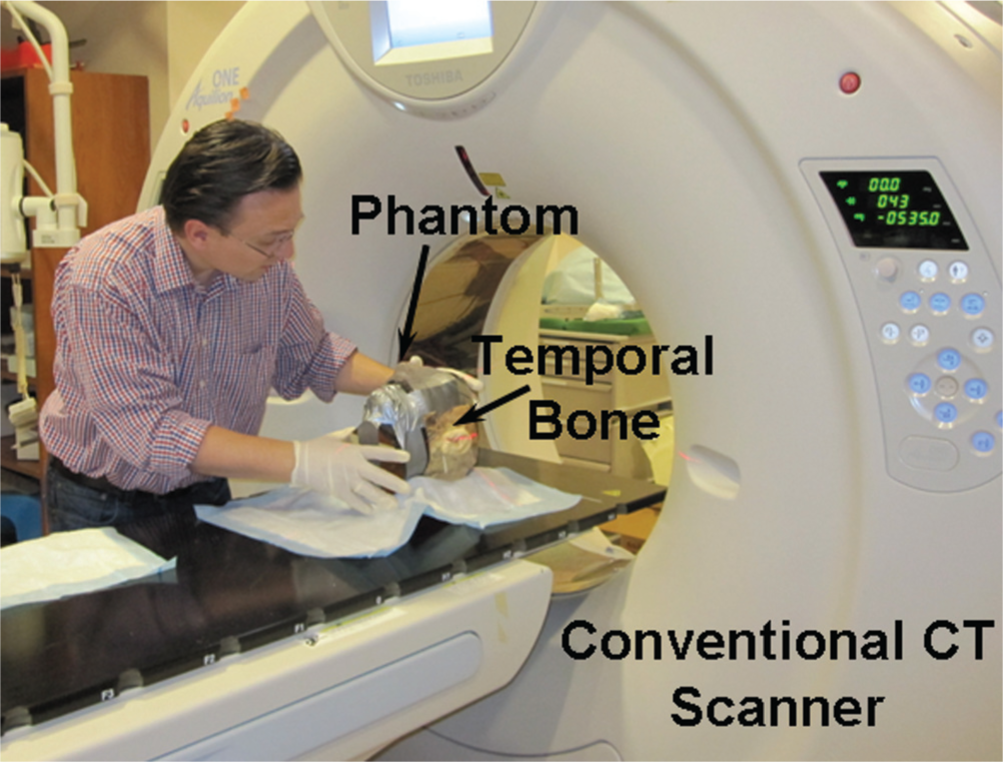
Illustration shows cadaveric temporal bone affixed into a head phantom being imaged by conventional multislice helical computed tomography.
Image Quality Evaluation
Three otologists and 1 head and neck radiologist independently completed the study questionnaire to provide a qualitative assessment of conventional CT and CBCT image quality. The order of the specimens and imaging modality was randomized. During the image evaluation session, all reviewers were free to adjust the window/level, as well as pan/zoom, according to their personal preference in clinical practice. After reviewing each image, a questionnaire was completed to evaluate the visibility of 21 anatomical landmarks and structures within 4 regions: (1) external ear canal (Q1), (2) middle ear (Q2-11), (3) inner ear (Q12-16), and (4) temporal bone (Q17-21). A binary scale (0 = inadequate, 1 = adequate) was employed for the otologist observer study that harmonized a surgical perspective in determining the detectability of landmarks in preoperative planning. A 5-point Likert-type scale (1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, 5 = very satisfied) was used for the image evaluation by the head and neck radiologist. This 5-point scale was further grouped into 2 levels such that (1-2) was mapped to 0 and (3-5) was mapped to 1.
Statistical Analysis
The cross-table technique was employed to summarize the performance agreement between CT and CBCT. The Kappa agreement test was then further applied to assess the level of agreement, with additional analysis to detect if there is a significant surgeon’s effect on the agreement test. To test whether CT and CBCT have significantly different answers adjusted on the surgeon’s effect, a generalized estimating equation (GEE) model was also applied. Subgroup analysis was conducted on the questionnaire responses from the 4 anatomical regions (external ear canal, middle ear, inner ear, and temporal bone) using 2 approaches (categorical variables and continuous variables approach). The grouping scheme of categorical variables grouped the response of the question “0” if one of the responses in the group is “0”; otherwise, the response of the group is “1.” Continuous variable used an additive approach in which the responses of the group are represented by summing the count of “1.” Repeated measurement analysis was applied to the subgroup analysis with a continuous variables approach. The assessment of significant differences between CT and CBCT in the radiologist observer study was evaluated using paired t tests and paired Wilcoxon tests. The binomial proportion test was also applied to evaluate significant differences. Statistical Analysis Software (SAS) 9.3 (SAS Institute Inc, Cary, NC) was used to perform all calculations. A P value of less than .05 was deemed to be statistically significant.
Results
Twenty cadaveric temporal bones were scanned inside the custom head phantom using both a prototype CBCT C-arm and a multislice helical CT scanner. Figure 4 shows images of a temporal bone acquired by conventional CT ( Figure 4a , b , c ) and the corresponding images from CBCT ( Figure 4d , e , f ). In total, 40 temporal bone volumetric images were acquired. Three otology specialists and 1 head and neck radiologist participated in the image performance review and landmark identification evaluation. In the otology group, 13 bones in common across 3 surgeons were reviewed. Seven bone images, including both CT and CBCT, were not reviewed because either the data being reviewed were unavailable during the review session or the field of view (FOV) was not appropriate. Seventy-eight questionnaires were completed by 3 otologists for CT and CBCT images. The radiologist reviewed all CT and CBCT images of 20 bones. However, a CT scan of 1 bone had an inappropriate FOV for analysis. Thirty-eight questionnaires were completed by the radiologist.
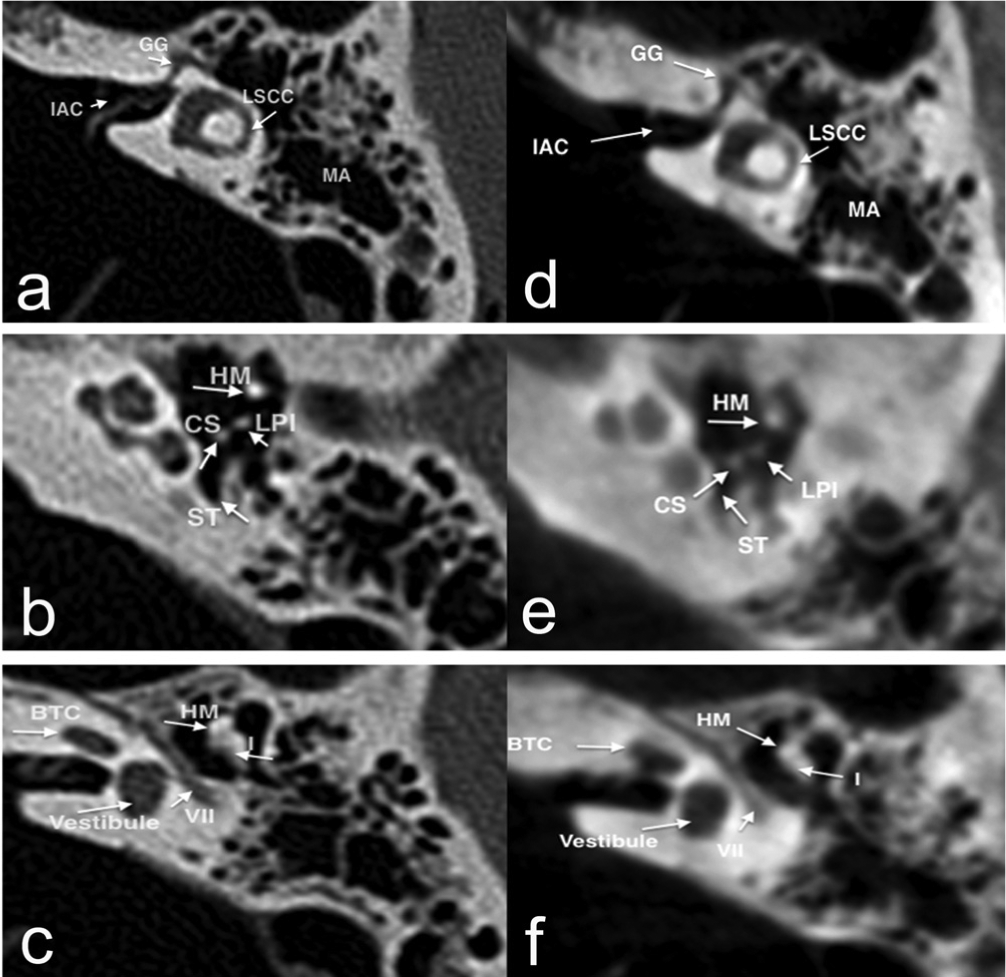
Slice images of a temporal bone acquired by a conventional computed tomography scan (a, b, c) and the corresponding slices by cone-beam computed tomography (d, e, f). BTC, basal turn of cochlea; CS, capitulum of stapes; GG, geniculate ganglion; HM, handle of malleus; I, incus; IAC, internal auditory canal; LPI, long process of incus; LSCC, lateral semicircular canal; MA, mastoid antrum; ST, sinus tympani; VII, facial nerve.
Surgeon Response Evaluation
Questions 6 (crura of stapes), 7 (round window niche), 9 (tympanic membrane), 16 (size of vestibular aqueduct), and 19 (chorda tympani) illustrate significant disagreement among the 3 surgeons. Therefore, further Kappa test analysis showed an overall Kappa coefficient for question 6 (crura of stapes), 7 (round window niche), 9 (tympanic membrane), 16 (size of vestibular duct), and 19 (chorda tympani in mastoid bone) of −0.25, −0.13, 0.03, 0.35, and −0.12, respectively. Question 6 has the most significant disagreement. To equalize the effect of each independent surgeon, GEE models were used to adjust agreement and disagreement results. Interestingly, this model shows that CBCT has superior performance (score = 1.12) on question 19 (chorda tympani; Pr > IZI =0.02) and inferior performance (score = −0.97) on question 6 (crura of stapes) with marginal significance (Pr > IZI = 0.06) in comparison with the multislice helical CT.
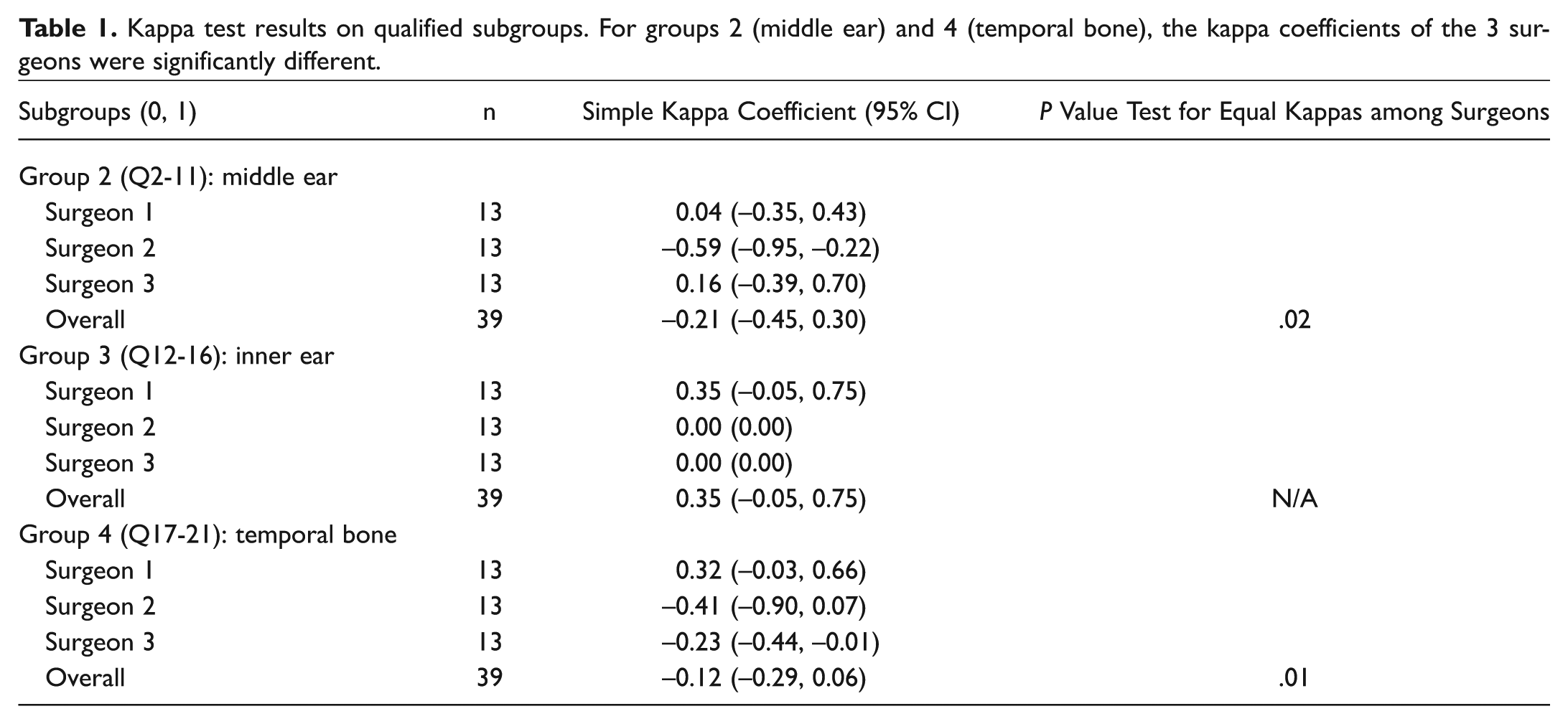
For subgroup analysis, the landmarks were grouped into 4 groups that represented the structures of (1) external ear: patent external auditory canal (Q1); (2) middle ear: head of malleus (Q2), handle of malleus (Q3), short (Q4) and long (Q5) process of incus, crura of stapes (Q6), round window niche (Q7), tegmen (Q8), tympanic membrane (Q9), scutum (Q10), and apacity in middle ear, status of sinus tympani and facial nerve recess (Q11); (3) inner ear: location of the internal auditory meatus (Q12), internal auditory canal (IAC) (Q13), semicircular canals (Q14), appearance of cochlea, vestibule, modiolous (Q15), and size of vestibular aqueduct (Q16); and (4) temporal bone: location of the jugular bulb (Q17), course of facial nerve (Q18), chorda tympani in mastoid bone (Q19), sigmoid sinus (Q20), and mastoid air cell aeration (Q21). Middle ear and temporal bone groups demonstrated significance in the disagreement of CT and CBCT from the surgeons’ responses. The number of disagreements in the middle ear and temporal bone was 22 (group 2) and 20 (group 4), respectively. Table 1 shows the kappa coefficients of the 3 surgeons, with group 2 and group 4 expressing significant differences. Results from the GEE model of subgroup analysis shows that CBCT has superior performance in investigating temporal structures; however, it may due to the 1-sided response from question 19 (chorda tympani).
Kappa test results on qualified subgroups. For groups 2 (middle ear) and 4 (temporal bone), the kappa coefficients of the 3 surgeons were significantly different.
Radiology Response Evaluation
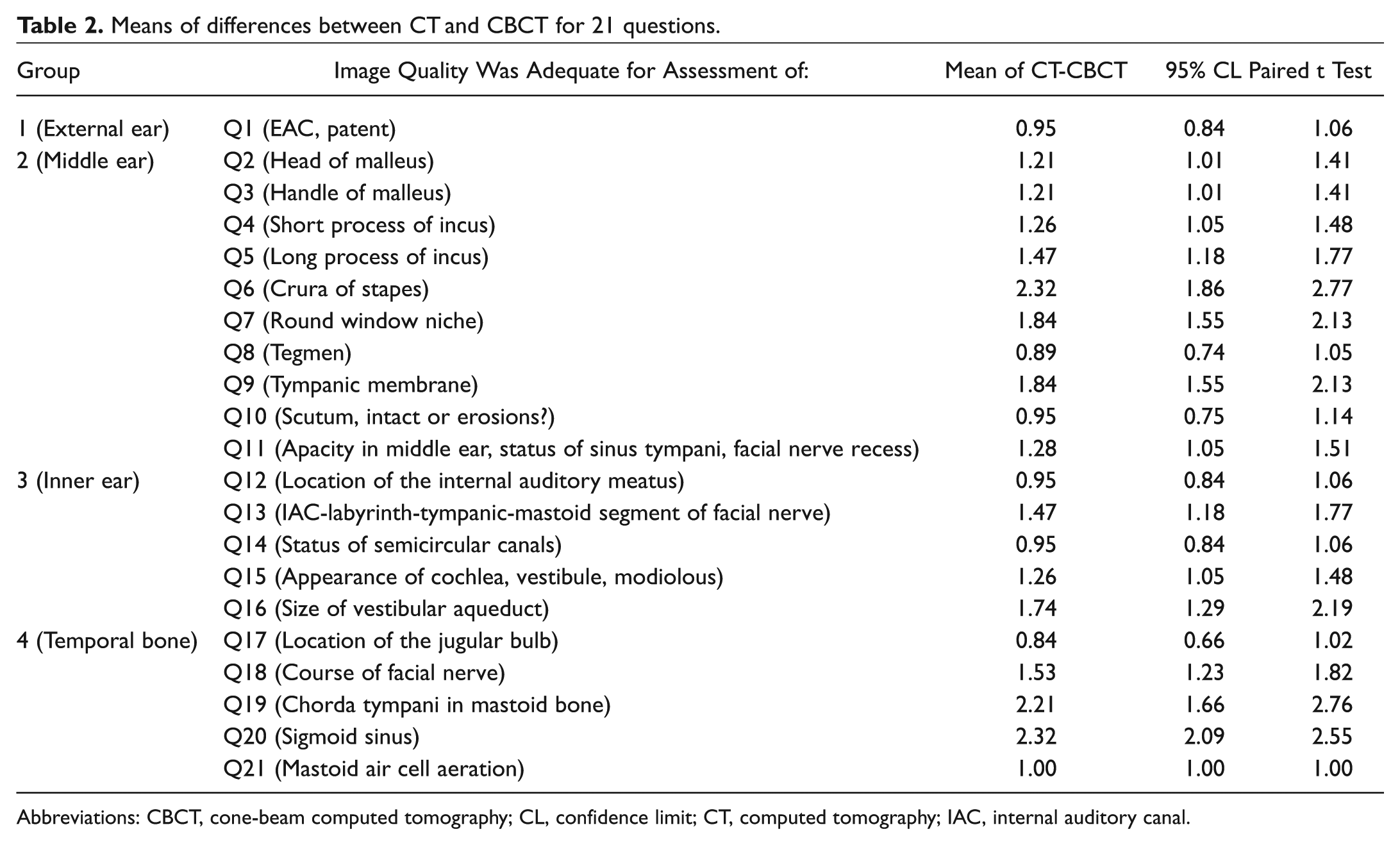
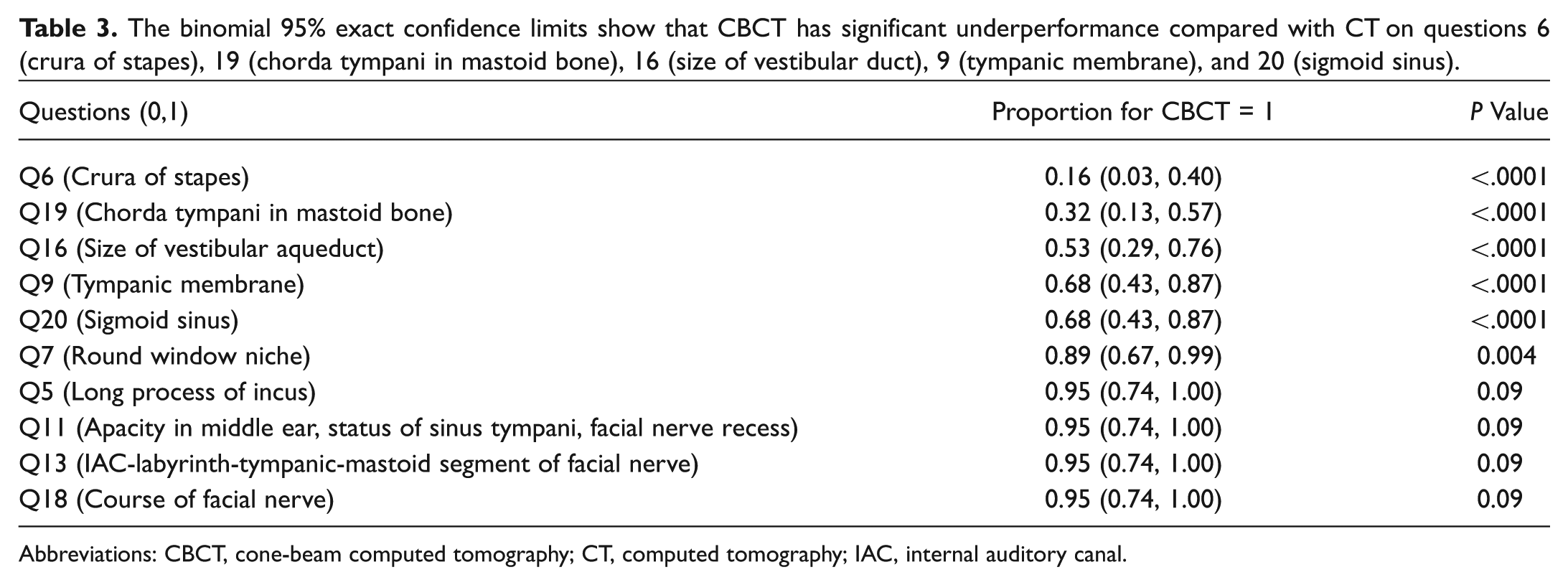
One head and neck radiologist participated in the study and reviewed 20 bones of CT and CBCT images; however, 1 set of images was acquired with inadequate FOV. This pair of CT and CBCT images was discarded from statistical analysis. In total, 38 questionnaires using a 5-point Likert-type scale were collected at the end of the review sessions. Using a paired t test and a paired Wilcoxon test, the P values of both tests were less than .0001 for each question, which suggests conventional CT imaging has superior performance to CBCT imaging in temporal bone landmark identification. Table 2 illustrates the mean score of differences between CT and CBCT in which crura of stapes (Q6), chorda tympani in mastoid bone (Q19), and sigmoid sinus (Q20) show high scores of difference, where the values are 2.32, 2.21, and 2.32, respectively, implying CT is outperforming CBCT for these specific structures. Converting the 5-point Likert-type scale into a binary scale by grouping the score of 3,4,5 to 1 and 1,2 to 0, Table 3 illustrates that CT has superior performance for crura of stapes (Q6), tympanic membrane (Q9), size of the vestibular duct (Q16), chorda tympani in mastoid bone (Q19), and sigmoid sinus (Q20) compared with CBCT with exact P values less than .0001.
Means of differences between CT and CBCT for 21 questions.
Abbreviations: CBCT, cone-beam computed tomography; CL, confidence limit; CT, computed tomography; IAC, internal auditory canal.
The binomial 95% exact confidence limits show that CBCT has significant underperformance compared with CT on questions 6 (crura of stapes), 19 (chorda tympani in mastoid bone), 16 (size of vestibular duct), 9 (tympanic membrane), and 20 (sigmoid sinus).
Abbreviations: CBCT, cone-beam computed tomography; CT, computed tomography; IAC, internal auditory canal.
Discussion
In otological imaging, multislice helical CT is a tool commonly used for diagnostic and disease management and pre- or postoperative surgical investigation because of its accurate detection of bony structure such as auditory ossicular chain and mastoid bone.16-18 However, advancements in CBCT imaging over the past decade have demonstrated that this imaging technique can provide sufficient image quality and spatial resolution of the bony components of the temporal bone, frontal, and lateral skull base.6,19 A recent study from Monteiro et al 14 also showed the utility of CBCT for intraoperative use in determining the position of ossicular reconstruction prostheses of the middle ear. Other studies reported the successful implementation of CBCT in image-guided surgery20,21 and treatment planning. 22 In oral and maxilla investigations, Liang et al 2 reported that some of the commercially available head and neck CBCT scanners have better imaging performance compared with conventional multislice CT. Since our system has a mobile C-arm, real-time “on the table” imaging capabilities are provided for intraoperative imaging.
Considering the reported advantages of CBCT noted in the literature, we wanted to investigate the potential clinical utility of CBCT in otologic surgery, especially as it pertains to image performance and bony landmark identification. In our study, 3 otology surgeons and 1 head and neck radiologist participated in an observational study to evaluate both CT and CBCT image quality of key cadaveric temporal bone landmarks, which were selected based on their clinical and surgical relevance in common chronic ear diseases including chronic otitis media, cholesteatoma, and otosclerosis and their treatment. Evaluation of the questionnaires from the surgeons revealed in general little difference in image quality between CBCT and CT. CBCT was significantly better in displaying the chorda tympani, which is crucial for intraoperative surgical guidance. In clear contrast to the surgeons, the radiologist generally preferred the conventional CT studies over the CBCT images.
A limitation of CBCT image quality was determining the crura of the stapes and chorda tympani. No doubt it is very important to gain as much information about the temporal bone anatomy as possible from imaging studies, but it is important to keep in mind that the crura of the stapes and chorda tympani are structures that have to be assessed initially clinically and, subsequently, intraoperatively. According to the intraoperative status, further surgical management has to be adopted by the surgeon during the surgery.
Despite its careful execution and design, this study has notable limitations. In particular, our data are derived from cadaveric studies, and further studies will be needed to support the preliminary data. Another point is that we have included only 1 radiologist with a special focus on head and neck radiology.
We strongly acknowledge that multislice helical CT scanning is the standard imaging technique for investigation and diagnosis of ear disease. However, there are associated disadvantages of using conventional CT compared with CBCT, one of which is the higher radiation dose to the patient.1,9,10 Repeated radiation exposure can cause biological tissue damage, especially radiation-sensitive tissues such as the optic nerve, chiasm, and brain stem. When repeated CT examinations are needed for disease management, the cumulative radiation exposure becomes a key issue to patients with chronic ear disease. However, CBCT could provide an alternative for CT examinations with minimal dose to achieve satisfactory image quality. Based on our previous investigations, CBCT requires only 10% of CT dosage to provide sufficient image quality. 10 A similar finding was also reported by Scarfe et al. 23 The comparatively low radiation dose of CBCT was also mentioned in other studies.24-27
Another significant advantage of our prototype CBCT is its mobility. In particular, the mobile-arm CBCT allows for accessible “on the table” or intraoperative imaging that is nearly real time. In contrast, intraoperative imaging on a standard CT scanner requires patient movement and thus is highly challenging for the whole operating room team. The lower purchase and maintenance cost of CBCT as well as the advantages related to its smaller size and its mobility would be of benefit in independent practice or small clinics. The migration of CBCT imaging into clinical practice will of course require additional clinical studies to validate the results presented in this study. CBCT technology is still being actively researched in the academic arena, with the current areas of interest being low-dose iterative reconstruction,28-30 scatter correction,31-34 lag correction,35-38 and metal artifact reduction.39-41
Conclusion
In summary, we suggest that multislice helical CT for the initial diagnostic workup should be the first choice of imaging, whereas CBCT should be assigned for evaluation of the proximate pre- or intraoperative status or for follow-up patients. Nevertheless, since an ultimate conclusion regarding the best imaging tool for the management of temporal bone diseases cannot be made based on cadaver temporal bone imaging alone, the specifications of protocols adequate for clinical otologic CBCT require further study.
Author Contributions
Disclosures
Footnotes
Acknowledgements
This work is supported by the TECHNA-Guided Therapeutics (GTx) Program at the University Health Network, including The Kevin and Sandra Sullivan Chair in Surgical Oncology, The Hatch Engineering Fellowship Fund, The RACH Fund, and the Princess Margaret Hospital Foundation. Thank you to Ms D. Rego, Ms M. Romanova, Mr J. Faria, and Ms L. Satterthwaite from the Surgical Skills Centre (Mt. Sinai Hospital, Toronto, Ontario, Canada) for their assistance with cadaver studies. Initial development of the C-arm prototype was performed in collaboration with Siemens Healthcare (Siemens XP, Erlangen, Germany).
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.