
Abstract
Objective
To review information on magnetic resonance imaging (MRI) issues for commonly used otologic implants.
Data Sources
Manufacturing companies, National Library of Medicine’s online database, and an additional online database (www.MRIsafety.com).
Review Methods
A literature review of the National Library of Medicine’s online database with focus on MRI issues for otologic implants was performed. The MRI information on implants provided by manufacturers was reviewed.
Results
Baha and Ponto Pro osseointegrated implants’ abutment and fixture and the implanted magnet of the Sophono Alpha 1 and 2 abutment-free systems are approved for 3-Tesla magnetic resonance (MR) systems. The external processors of these devices are MR Unsafe. Of the implants tested, middle ear ossicular prostheses, including stapes prostheses, except for the 1987 McGee prosthesis, are MR Conditional for 1.5-Tesla (and many are approved for 3-Tesla) MR systems. Cochlear implants with removable magnets are approved for patients undergoing MRI at 1.5 Tesla after magnet removal. The MED-EL PULSAR, SONATA, CONCERT, and CONCERT PIN cochlear implants can be used in patients undergoing MRI at 1.5 Tesla with application of a protective bandage. The MED-EL COMBI 40+ can be used in 0.2-Tesla MR systems. Implants made from nonmagnetic and nonconducting materials are MR Safe.
Conclusion
Knowledge of MRI guidelines for commonly used otologic implants is important. Guidelines on MRI issues approved by the US Food and Drug Administration are not always the same compared with other parts of the world.
Implications for Practice
This monograph provides a current reference for physicians on MRI issues for commonly used otologic implants.
Keywords
Magnetic resonance imaging (MRI) is an important diagnostic imaging technique restricted in patients with certain implants, which include passive and active (or electronic) devices. 1 The powerful static magnetic fields used for MRI have the potential to attract ferromagnetic components. In addition, the static magnetic field may demagnetize or damage electronic components and lead to hardware malfunction for cochlear implants and similar electronic devices. 1 Radiofrequency (RF) energy can heat particular implants under certain MRI conditions and potentially lead to patient injuries. 2 Finally, artifacts related to the presence of metallic implants can affect the diagnostic use of MRI, especially when implants, such as certain cochlear implants, contain magnets.
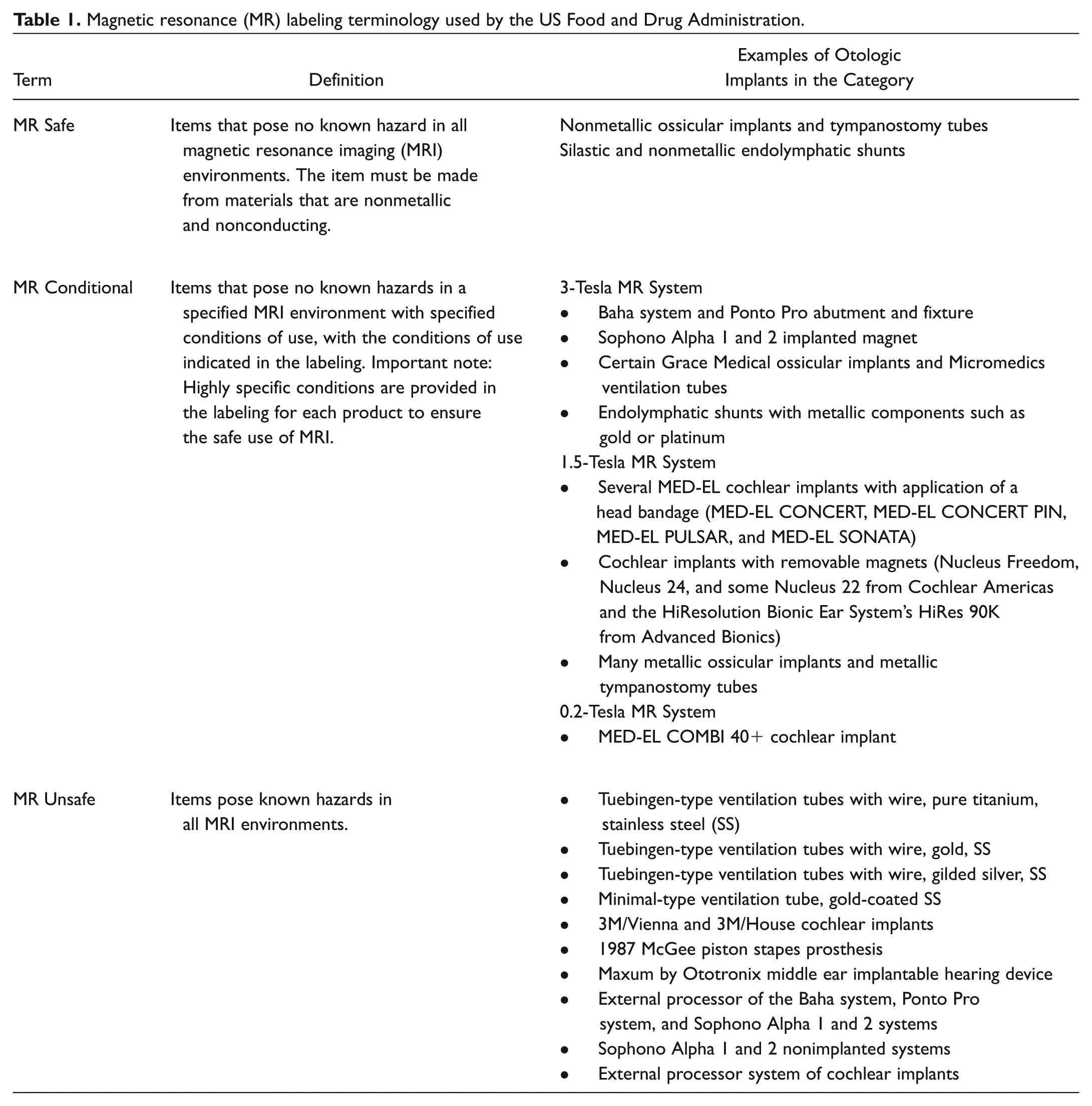
In 2005, the American Society for Testing and Materials (ASTM) International developed terminology used for labeling implants and devices. 3 MRI Safe and MRI Compatible are considered outdated and are no longer acceptable for labeling by manufacturers or approved by the US Food and Drug Administration (FDA) since they are confusing terms that are often used incorrectly and interchangeably.4,5 With incorrect use of MRI labeling terminology, there may be an unacceptable risk to patient safety.4,5 The current labeling is as follows: MR Safe refers to objects that are nonmetallic and nonconductive and pose no known hazards in all MRI environments.3-5 MR Conditional refers to items that have demonstrated to pose no known hazards in a specified MRI environment with specific conditions of use indicated.3-5 MR Unsafe are items that pose hazards in all MRI environments.3-5 The current standard of care in MRI settings is to determine the type of implant that might be in a patient during the screening procedure and to identify the implant as “MR Safe,”“MR Conditional,” or “MR Unsafe.” 6 If there is no information available, then the implant or device is considered MR Unsafe. As such, the radiologist needs to decide whether to scan the patient based on the risk vs benefit for the patient (see Table 1 ).
Magnetic resonance (MR) labeling terminology used by the US Food and Drug Administration.
Importantly, the standard of care for managing a patient with an otologic implant in need of an MRI is to accurately identify the type of implant and to diligently review the most up-to-date MRI information available for the device. 1 MRI-related labeling of otologic implants comes from the peer-reviewed literature or results of ex vivo testing of the device and is indicated in the device labeling or instructions for use. 1 Protecting patients from MRI-related adverse outcomes is an important responsibility of the medical team.
The practicing physician and patient in the United States should question the safety of MRI examinations in the setting of an implanted otologic device. Therefore, the purpose of this article is to provide a source that reviews the current information and presents information for MRI issues (ie, magnetic field interactions, heating, and artifacts) for otologic devices most commonly implanted. The goal is to provide this information in a simple layout based on available literature to date. Notably, the information provided in this review is subject to change based on additional testing of implants and with the advancement and changes in MRI technology.
Methods
A literature review of the National Library of Medicine’s online database was performed with a focus on MRI safety of routinely used implanted hearing devices. The search was restricted to the more commonly used otologic implants, including stapes and metallic middle ear prostheses, cochlear implants, osseointegrated cochlear stimulators, middle ear hearing aid implants, and endolymphatic shunts. Keywords used were as follows: MRI safety, otologic implants, cochlear implants, osseointegrated cochlear simulators, Baha, Sophono, Ponto Pro, stapes prosthesis, middle ear prosthesis, middle ear implantable hearing device, Vibrant Soundbridge, and endolymphatic shunts. Non-English studies were excluded. In addition, manufacturing companies were contacted via phone or email for devices with little or no literature available on MRI issues. Manufacturing company websites were searched for MRI safety guidelines based on the FDA recommendations. Content from the website www.MRIsafety.com, which is an international resource of MRI safety and patient management information, was also used for this review.
Results
Stapes Prostheses
A stapes prosthesis is used in a patient with otosclerosis. In otosclerosis, there is conductive hearing loss due to disruption of normal conduction of sound through the ossicular chain secondary to a fixed stapes. Operative correction of this condition involves implanting a middle ear stapes prosthesis to restore ossicular chain mobility and conduction of sound from the tympanic membrane to the inner ear (oval window).
Of all the otologic implants, the stapes prostheses’ relation to the electromagnetic fields used for MRI has been the most studied.6-19 Tested stapes prosthetic devices are reported as MR Conditional in 1.5-Tesla MR systems with the exception of 1 device. 8 The 1987 McGee stainless steel prostheses were recalled after it became evident that they were incorrectly manufactured using “magnetic grade” 400 stainless steel. Tests performed to evaluate magnetic field interactions at 1.5 Tesla by Applebaum and Valvassori 9 raised the initial suspicion toward these implants. A total of 28 lots of the McGee piston (Richards Company, Memphis, Tennessee) made with grade 400 stainless steel were recalled. 8 Shellock and Sawyer-Glover 20 have documented the 1987 recalled lots. 21 If patients with a 1987 McGee stainless steel prosthesis need an MRI, they may require a revision stapedectomy to revise their prostheses to a device that is acceptable for MRI. 8 Many implants, including certain devices from Grace Medical (Memphis, Tennessee), have 3.0-Tesla MR Conditional approval at this time. 21
Although stapes prostheses are known as MR Conditional, Syms and Peterman 11 noted significant in vitro rotational activity of the Medtronic (Minneapolis, Minnesota) Xomed stainless steel piston and wire prostheses and cupped piston prostheses when tested at 1.5 Tesla. They attributed their findings to possible manufacturer variability. 11 Syms and Peterman 11 concluded that the clinical significance of their findings is unclear. To date, there are no reports of MRI-related issues associated with the implants studied by Syms and Peterman. 11 Magnetic resonance imaging continues to be recommended by the manufacturing company of these devices.
Metallic Middle Ear Ossicular Chain Reconstruction Implants
Middle ear ossicular chain reconstruction prosthetic devices, like the stapes prosthesis, are also used to restore conduction of sound from the tympanic membrane to the inner ear. If the stapes is mobile, a partial ossicular chain reconstruction prosthesis (PORP) is used. This implant connects to the stapes and partially replaces the ossicular chain. If the stapes is fixed or anatomically absent, a total ossicular chain prosthesis (TORP) is used, which replaces the entire ossicular chain function from the tympanic membrane to the oval window.
Not all middle ear ossicular reconstruction devices are made from metallic materials. Many of the studies investigating MRI issues for stapes prostheses also studied various TORPs and PORPs.6,9,10,18,19 Of the metallic partial or total ossicular chain reconstruction devices, the majority are made out of titanium. The tested partial and total ossicular chain prostheses are MR Conditional for 1.5-Tesla MR systems. Many devices are also MR Conditional for 3-Tesla MR systems. 21 Studies in higher magnetic fields show promising results for stapes prostheses, TORPs, and PORPs in fields as strong as 9.4 Tesla (only 1 such MR system operating at this field strength exists).18,19 The authors could not identify MR Unsafe TORPs or PORPs in this review.
Osseointegrated Cochlear Stimulator
Osseointegrated cochlear stimulators are indicated for patients with conductive or mixed hearing loss or single-sided deafness. This technology transfers sound through the skull directly to the inner ear, bypassing the middle ear. The Baha system fixture, Ponto Pro system, and Sophono system are the commonly used devices in the United States that use this technology.
The Baha system consists of an implanted fixture and abutment. The abutment is a screw that protrudes through the skin and accommodates the external processor. The fixture and abutment are made out of titanium, which is a paramagnetic metal. They are approved for use (ie, MR Conditional) in 3.0-Tesla MR systems. 22 The external processor is ferromagnetic and must be removed before scanning. In fact, 1 study suggested evidence that the use of the Baha system fixture and abutment may be safe for patients in fields as strong as 9.4 Tesla. 23 Only 1 investigation identified in the English literature focused on testing the MRI safety of the Baha abutment and fixture. 23
The Ponto system by Oticon Medical (Askim, Sweden) is a fully digital and programmable bone-anchored power processor. The fixture and abutment for this device is MR Conditional in 3-Tesla MR systems, but like the Baha system, the external processor needs to be removed from the patient prior to MRI. 24
The Sophono bone conduction hearing systems (Sophono Inc, Boulder, Colorado) use a magnetic coupling system. These devices may be more appealing to some patients since they do not involve an abutment screw behind the ear like the Baha and Ponto systems. The Alpha 1 and Alpha 2 nonimplanted systems use a bone conduction headband or soft band or a metal headband and do not involve an implanted magnet. All components to the nonimplanted Alpha systems are considered MR Unsafe. 25 The Alpha 1 and Alpha 2 abutment-free systems involve a bone-anchored hearing device and magnet. The implanted magnets of the abutment-free Alpha systems have been classified as MR Conditional in 3-Tesla MR systems since April 2013 with FDA approval. 25 To minimize demagnetization of the implanted magnet, the patient’s head should be positioned along the long axis of the scanner and the patient’s head should not move during the scanning process. 25 To avoid overheating of the internal magnet, patients should not undergo more than 15 minutes of continuous scanning per pulse sequence. 25 The external sound processors of the Alpha abutment-free systems are MR Unsafe and should be removed prior to entering the MRI suite area. 25
Middle Ear Implantable Hearing Devices
Middle ear implantable hearing devices are indicated for patients with moderate to severe hearing loss who do not benefit from or medically tolerate hearing aids. This technology amplifies sound by converting mechanical sound energy electrically or electromagnetically into a vibratory signal. The Vibrant Soundbridge (MED-EL, Durham, North Carolina), Esteem by Envoy (Envoy Medical, Saint Paul, Minnesota), and Ototronix Maxum (Ototronix, Houston, Texas) are 3 middle ear implantable hearing devices.
The Vibrant Soundbridge (VSB) consists of an external receiver and middle ear implant. The implantable part of the VSB includes 2 samarium-cobalt magnets. 2 The floating mass transducer (FMT) is a part of the implant that is usually secured onto the long process of the incus and less commonly onto the stapes, oval window, or round window.2,26,27
The instructions provided by the manufacturer of the VSB device state that MRI should not be performed in patients implanted with this device (ie, MR Unsafe). The recent reports of symptoms experienced by patients while undergoing MRI raise concerns as described below.
Studies have shown in vitro positional changes of the FMT 28 but no changes to the ossicular chain integrity with MRI exposure. 29 The implications of the findings are unknown in practical situations. There are reports of “loud bang noise” and loud, continuous noise perception, pain, pressure at the receiver bed, and subcutaneous movement of the implant receiver in patients with VSB devices who have had an MRI. There are also reports of the need for repositioning the FMT portion of the VSB in patients who have undergone MRI. 26
Unlike the VSB, a literature review on the Esteem by Envoy and Ototronix Maxum did not reveal studies performed to investigate MRI issues. The Esteem by Envoy Medical and Maxum by Ototronix are currently not approved for patients referred for MRI procedures. In fact, Ototronix Maxum is classified as MR Unsafe. 21 Like the VSB, the Maxum by Ototronix converts and amplifies sound electromagnetically to a vibratory signal. The Maxum implant consists of a surgically implanted neodymium-iron-boron magnet encased in a titanium canister, which is attached to the ossicular chain. The Esteem by Envoy converts and amplifies sound electrically into a vibratory signal through a piezoelectric transducer device implanted in the middle ear. Piezoelectric transducers are made up of piezoelectric crystals that have the advantage of being inert in a magnetic field and therefore are not significantly affected by MRI. Studies are currently being conducted for MRI safety of Esteem implants with the device turned off during MRI. Unlike in the United States, certain Esteem by Envoy models have MR Conditional approval at 3 Tesla in Europe if the device is turned off. 30
Tympanostomy Tubes
The use of metallic tympanostomy tubes is currently not a common practice. The nonmetallic tympanostomy tubes are MR Safe. Of the metallic implants, the Kurz Medical Tuebingen-type ventilation tubes with wire-pure titanium-stainless steel (Kurz Medical, Tucker, Georgia), the Tuebingen-type ventilation tubes with wire-gold-stainless steel, the Tuebingen-type ventilation tubes with wire-gilded silver-stainless steel, and the minimal-type ventilation tube with gold-coated stainless steel are MR Unsafe. 21 The authors could not identify other tympanostomy tubes labeled as MR Unsafe. Metallic tympanostomy tubes that have been tested are MR Conditional with more and more tubes approved for patients undergoing examinations in 3-Tesla MR systems.
Cochlear Implants
Cochlear implantation is mainly indicated in severe-to-profound hearing loss that cannot be adequately aided using standard hearing aids. This technology involves directly implanting electrodes into the cochlea through the round window or a cochleostomy immediately adjacent to the round window.
Cochlear implants typically consist of a pair of magnets that can create serious problems with MRI. 31 The external processor system of all cochlear implant devices is MR Unsafe. Two older models of cochlear implants, the 3M/Vienna and 3M/House cochlear implants, are listed as MR Unsafe on the MRIsafety.com website. 21 The literature reports MRI in patients with several different types of implants with no reported adverse effects. 32 Obtaining FDA approvals for cochlear implants in the United States is a work in progress with adjustments made by manufacturing companies and additional safety testing.
Cochlear implants with removable magnets were produced by manufacturers, including the newer Cochlear Americas Implants (Nucleus Freedom, Nucleus 24, and some Nucleus 22 implants; Cochlear Americas, Centennial, Colorado) and the HiResolution Bionic Ear System’s HiRes 90K (Advanced Bionics, Valencia, California). Cochlear Americas Nucleus 5 devices, the CI512 and CI513 (which as of the writing of this review are not available due to an FDA recall), also have removable magnets. With these devices, the internal magnet can be surgically removed from the patients under local anesthesia for 1.5-Tesla MR systems. 33 The magnet can be removed, the open wound covered with a sterile dry dressing, MRI obtained, and a new magnet replaced under sterile conditions in a 4-hour period.33,34 If the patient needs more than 1 MRI, the removed magnet can be replaced with a titanium plug and a new magnet can be placed when the patient has obtained all necessary MRIs.33,34
The MED-EL COMBI 40+ and PULSAR (MED-EL) devices’ internal magnet is protected by a robust ceramic case. The MED-EL CONCERT, CONCERT PIN, and SONATA cochlear implants’ internal magnetics are in a titanium and silicon case. In 2013, the FDA approved MED-EL CONCERT, MED-EL CONCERT PIN, MED-EL PULSAR, and MED-EL SONATA for use in 1.5-Tesla MR systems with the use of a tightly fit head bandage. 35 Scanning conditions and instructions for these devices can be found on the company website. 35 The aforementioned approval is the first time the FDA has approved the use of cochlear implants under conditional circumstances in 1.5-Tesla MR systems. The MED-EL COMBI 40+ is still only recommended for patients undergoing MRI at 0.2 Tesla. 35 Notably, there are few facilities in the United States using MR systems operating at this static magnetic field strength.
Studies show that applying compression dressings over cochlear implants in cadaver temporal bones may help to prevent magnet movement and demagnetization at 1.5 Tesla. 36 A study of 16 patients with cochlear implant devices representing all 3 major manufacturing companies who underwent MRI after binding the implant with mold material and gauze revealed no device problems. 37 In Europe, a broader range of cochlear implants is approved for patients undergoing MRI at 3 Tesla with the use of head bandages. With current trends around the world and more literature demonstrating safety, a broader category of cochlear implants may obtain FDA approval in the future, even in 3-Tesla MR systems, although it must be noted that the acceptance criteria for proper MRI testing performed on implants are different in the United States vs other countries.
Despite approval of use of a broader category of cochlear implants in other parts of the world, there continue to be reports of internal magnet migration secondary to MRI examinations with and without use of head bandages.38-40 In 1 reported case of magnet migration, the magnet was repositioned manually without the need for surgical intervention. 39
Endolymphatic Shunts
Endolymphatic shunt placement is a surgical option for the management of Meniere’s disease. This procedure is now mostly replaced by endolymphatic sac decompression. Surgeons mostly self-craft silastic sheets into shunts 41 ; however, there is a 1965 report of self-crafted shunts made from Teflon. 42 Patients with shunts made from silastic and Teflon can undergo imaging in 3-Tesla MR systems. The Medtronic Austin endolymphatic shunt (Medtronic, Minneapolis, Minnesota) and Pulec endolymphatic shunt are labeled MR Conditional at 3 Tesla.43,44 The Hood Laboratory (Pembroke, Massachusetts) Arenberg inner ear valve shunt, Huang inner ear shunt, Gibson inner ear shunt, and Hood endolymphatic shunt tube were reported as “MR compatible” by the company.45,46 This form of reporting does not meet the current standards, and we cannot comfortably conclude that the implants are MR Conditional at 3 Tesla. The authors could not identify MR Unsafe endolymphathic shunts (see Table 2 ).
Summary of MRI labeling for otologic implants.
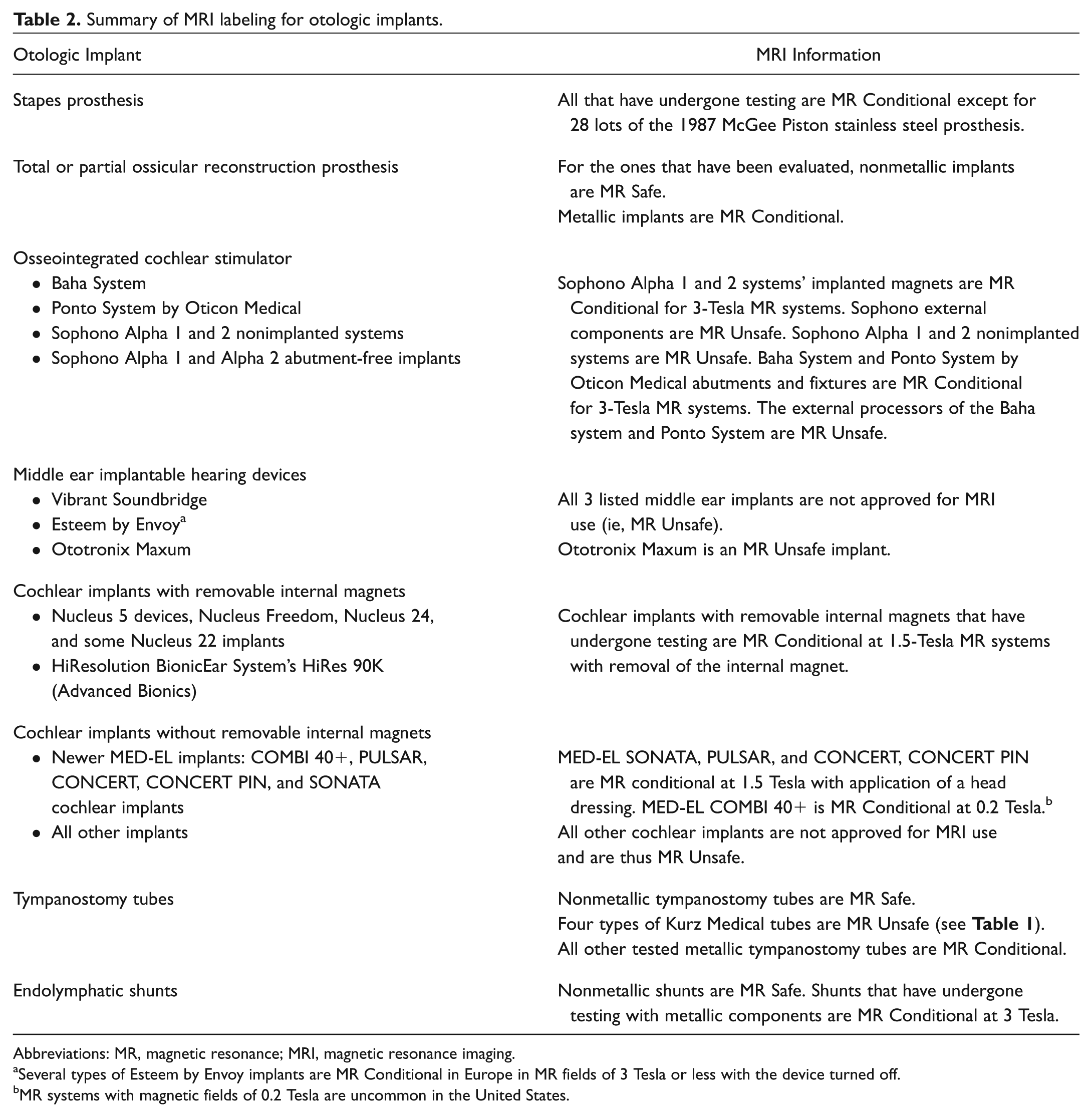
Abbreviations: MR, magnetic resonance; MRI, magnetic resonance imaging.
Several types of Esteem by Envoy implants are MR Conditional in Europe in MR fields of 3 Tesla or less with the device turned off.
MR systems with magnetic fields of 0.2 Tesla are uncommon in the United States.
Discussion
Currently, 3 Tesla is the strongest field used in the clinical setting for MRI. Implants with strong magnetic properties are associated with risks with MRI. The medical community is more familiar with MRI issues of the common implants such as heart valves, hemostatic clips, and orthopedic implants. However, we suspect that most physicians are unfamiliar with otologic implants and their MRI labeling status.
The ideal implant would be both inherently and functionally safe with no artifact properties. 18 Notably, if metal is involved in the implant, it must be labeled MR Conditional. There is a trend toward manufacturing nonferromagnetic materials for certain implants, if possible. As such, there would be no MRI issues. With regard to magnetic field interactions, the presumably safe metals include titanium, aluminum, beryllium, copper, magnesium, nickel, gold, and silver. However, even the so-called safe metals are conductors and, as such, may heat during MRI under certain conditions and cause burns. Furthermore, metallic implants will have associated artifacts depending primarily on the magnetic susceptibility of the material and the pulse sequences that are used for the MRI examination.
With the progression of MRI testing and review by the FDA, we anticipate a change in the near future in the United States to include MR Conditional labeling of some cochlear implants and the Esteem middle ear implantable hearing device. In Europe, there is a range of cochlear implants approved for 3-Tesla MR systems. The same holds true for the Esteem by Envoy.
It is imperative that the operating surgeon carefully and accurately report the type of implant used in the operative report. This can serve as a key referable document at times of uncertainty. However, in reality, patients and referring physicians may not be aware of the type of implant used at the time of surgery, especially implants placed several decades ago. It is also important to note that there have been reports of MRI errors, such as death from displacement of an aneurysm clip, in cases where implanted devices have been reported as nonferromagnetic. 47
To be in compliance with safety measures, patients may be provided with MRI labeling information cards for cochlear implants, osseointegrated cochlear stimulators, middle ear implantable hearing devices, and other similar implants. This card should be presented to the appropriate medical personnel when necessary. Regardless of the presence or absence of an MRI labeling card, it is imperative that the MRI facility contact the manufacturer of the device as there may be necessary precautions to take when performing an MRI on a patient with any of the aforementioned devices. Alternatively, the website www.MRIsafety.com has information for thousands of implants and devices and is often used to address MRI safety and patient management.
Based on our review, not all manufacturers had easy website access to MRI labeling information for their otologic implants. Companies with a link labeled as “safety information” allowed easier access to MRI information. In certain cases, the information was outdated and/or the labeling terminology was incorrect. We suggest that all manufacturers provide a link to MRI labeling information on their main page. Contact information to discuss MRI issues for devices should be readily available. We also suggest that all implants marketed by the company, past or present, be mentioned and labeled with MRI information.
As new information becomes available from studies and changes in FDA regulations, we suggest implementing a way for manufacturing companies to update patients. A national registry of patients with implanted devices should be considered. Manufacturers would be obligated to update their MRI safety status for each device, which would get linked to patients registered with their device. As MRI is becoming a more commonly used imaging modality in the medical field, the need for such databases can be justified. Websites that are available with MRI information on implantable devices should be cautiously used by medical professionals based on source reliability and accuracy.
Implications for Practice
The MRI labeling status of otologic implants depends on magnetic field interactions and heating issues. Knowledge of the MRI-specific guidelines for the commonly used otologic implants is important. In the United States, guidelines for MRI are not always the same as in Europe and other parts of the world. Prior to performing an MRI on patients with otologic implants, their MRI labeling cards should be reviewed and the manufacturing companies should be contacted.
This review can serve as a simple reference for current MRI information for otologic implants in the United States. Over time, updated reviews on MRI issues for otologic implants are necessary. It is vital for physicians to be aware of references that provide the most up-to-date MRI information on otologic implants.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Certain aspects of the contents of this manuscript were presented as a poster at the 2012 AAO-HNSF Annual Meeting and OTO EXPO; September 9-12, 2012; Washington, DC and at the 2013 Annual Meeting of the Pennsylvania Academy of Otolaryngology; June 14-15, 2013; Bedford, Pennsylvania.