
Abstract
Head and neck cancers are challenging to study because of their relatively low incidence. A large, novel population of patients with head and neck cancers that has not been previously studied and distinct from the referral populations has been identified. The National Cancer Institute–funded Health Maintenance Organization Cancer Research Network is a consortium of 15 nonprofit research centers based in large, vertically integrated health care delivery organizations across the United States. They represent a geographically, racially, and socioeconomically diverse population. These community-based organizations provide care to approximately 10 million individuals and 57,692 patients with head and neck cancer. This pilot study and preliminary analysis seeks to demonstrate the potential this network holds as a resource for clinical cancer research and to identify it as a unique resource that allows for more detailed queries than are currently available to researchers.
Head and neck cancers are challenging to study because of their relatively low incidence. A substantial and novel population of patients with head and neck cancers that has not been previously studied and distinct from a referral population has been identified. This population of patients receives their care exclusively within a health maintenance organization (HMO).
The Cancer Research Network (CRN) is a consortium of 15 nonprofit research centers based in large, vertically integrated health care delivery organizations across the United States ( Figure 1 ). They represent a geographically, racially, and socioeconomically diverse population. These community-based health plans provide care to approximately 10 million individuals. The CRN has been continuously funded by the National Cancer Institute (NCI) since its formation in 1999. The NCI’s goal was to enhance research on cancer etiology, prevention, detection, and management through collaboration with these community-based organizations that served large, stable populations of patients 1 and maintained searchable electronic databases with a rich array of patient information. 2 The structures of these health organizations allow the evaluation of the entire continuum of cancer care from primary care to long-term surveillance.
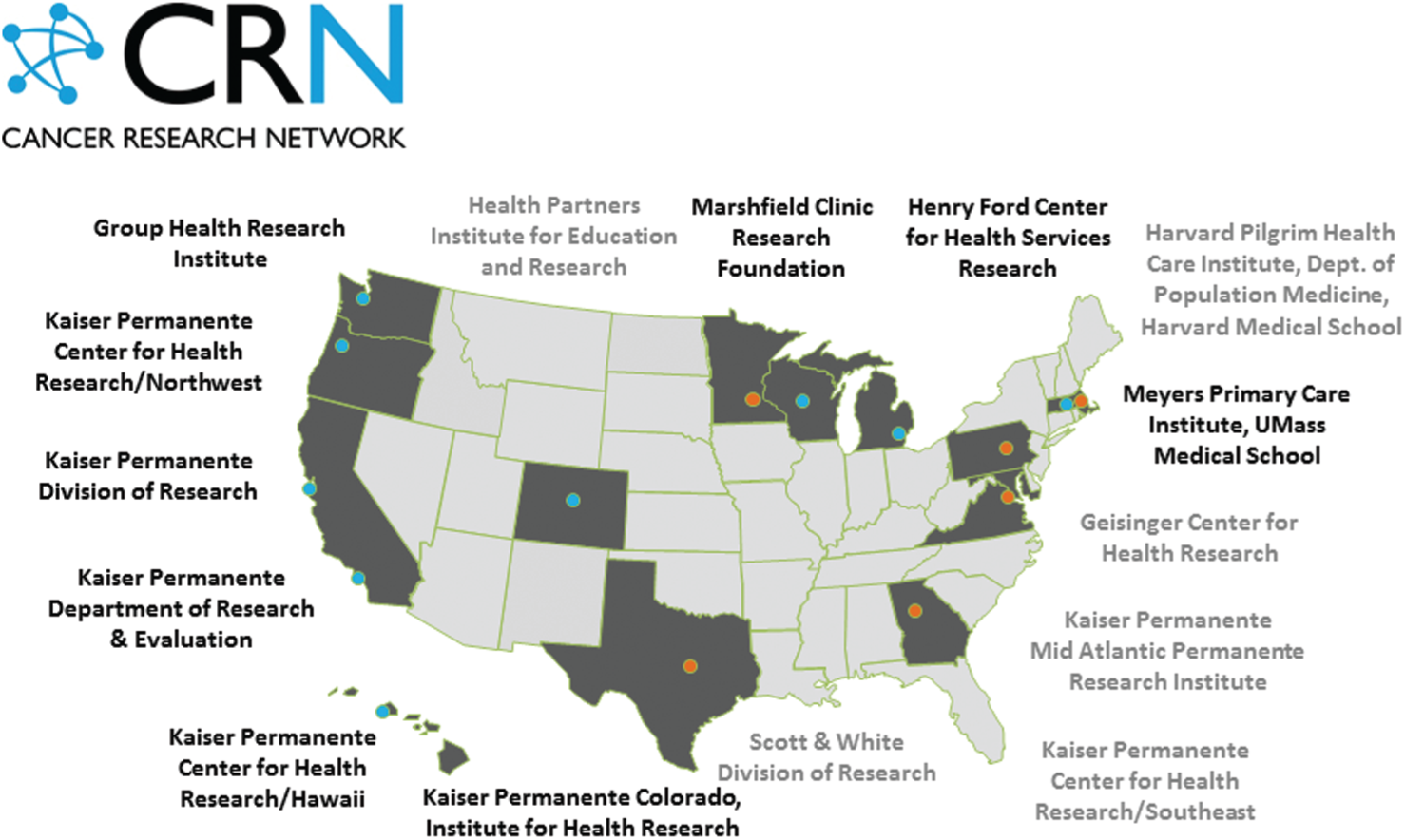
Map of the geographical locations of each Cancer Research Network site and the associated system.
The NCI also funds the maintenance of a network called the virtual data warehouse (VDW), which allows extraction of data from each health plan’s administrative and laboratory databases, tumor registries, and electronic medical records in the CRN. The structure of the database and the available data within the VDW are described in Figure 2 . The VDW has data, which are maintained locally at each site, dating from as early as the 1990s at most sites. This distributed repository of standardized clinical and administrative data contains demographic, pathology, surgery, chemotherapy, radiation, and morbidity/mortality data for each patient. Tumor registry data are updated annually by data abstractors at each site using a standardized coding system that allows for cross-institutional data analysis. Data abstraction and compilation are done by trained programmers in a standard fashion across sites.
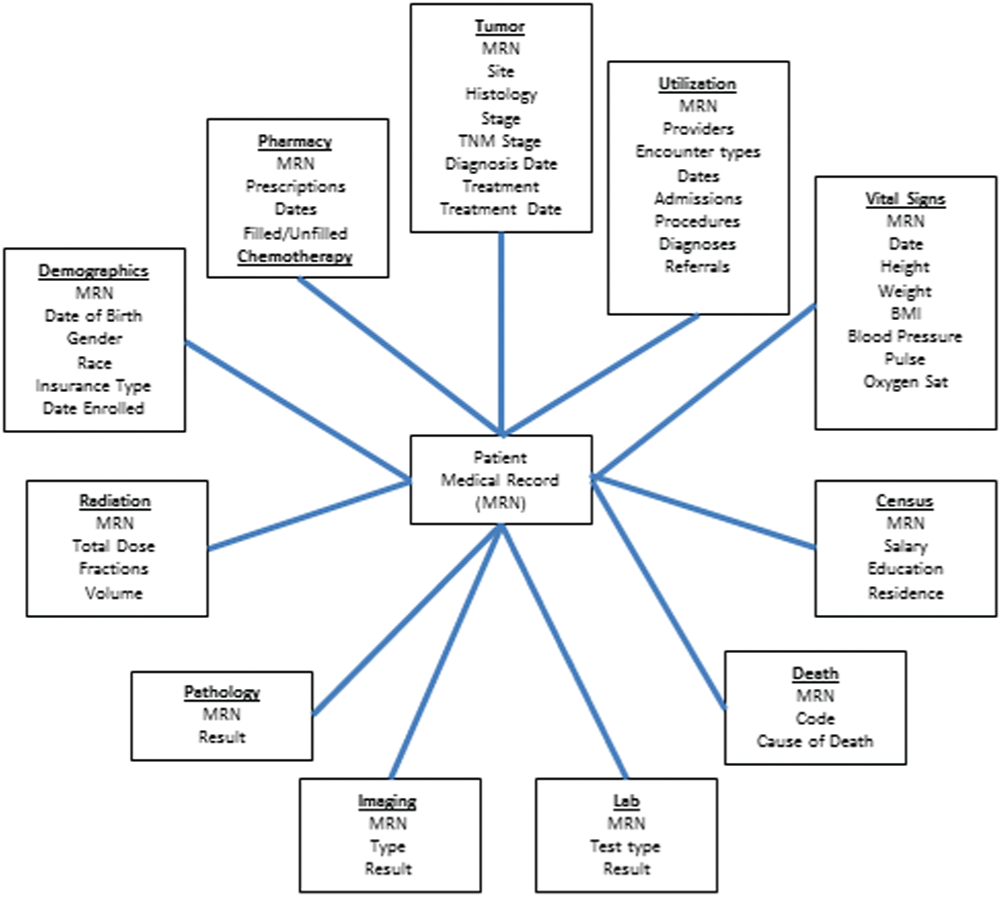
Schematic representation of the Cancer Research Network virtual data warehouse structure. BMI, body mass index; MRN, medical record number.
To study head and neck cancers within the CRN, a working group from several health care institutions around the country was formed from within the network. Once established, a pilot study to determine the potential for further study within this network was executed.
A general query of all sites within the CRN VDW was conducted with the following search criteria: patients with cancer with all histologic types of the upper aerodigestive tract (larynx, pharynx, oral cavity, nasal cavity), salivary glands, and thyroid/parathyroid glands diagnosed between 1990 and 2013. Dermatologic malignancies were excluded. In total, 57,692 patients with cancer were identified. Of the patients with head and neck cancer, there were approximately 14,228 with thyroid/parathyroid gland cancer, 9331 with laryngeal cancer, 3485 with salivary gland cancer, 11,883 with oropharyngeal cancer, and 14,347 with oral cavity cancer.
A preliminary analysis of the local VDW at Henry Ford Health System was done to demonstrate the capability and ease in which statistical inference could be performed. Patients with head and neck cancer were queried for oropharyngeal squamous cell cancers within the CRN Henry Ford VDW spanning from 1995 to 2013; a total of 572 patients were identified. Analysis of overall patient survival relative to race and sex was completed using Kaplan-Meier curves. Statistical significance was considered positive if P < .05. Using the data set, we identified statistically significant racial differences in patient survival. Blacks had worse survival prognosis, but sex conferred no survival advantage ( Figure 3 ) in this preliminary analysis.
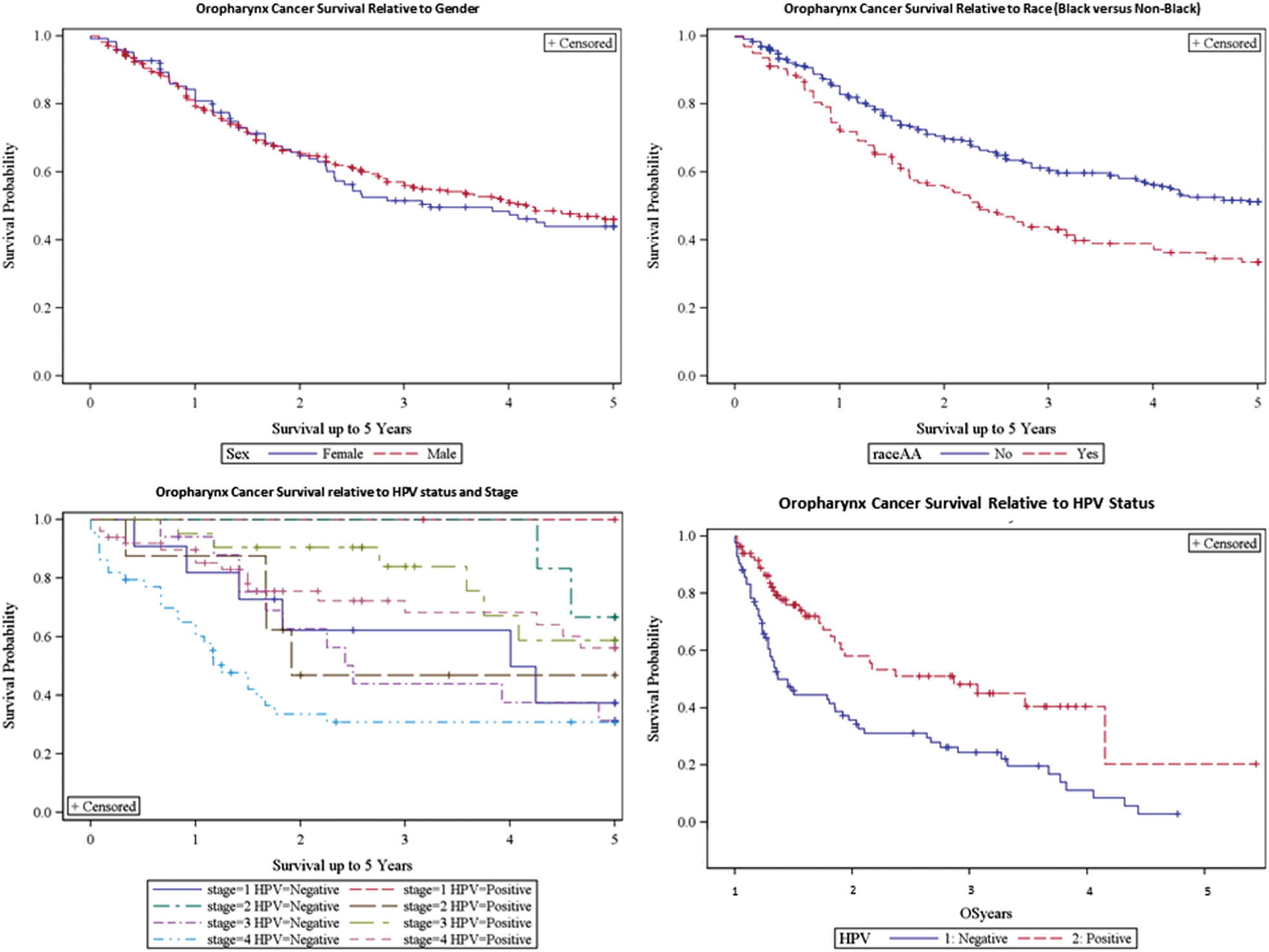
(a) Squamous carcinoma of oropharynx (SCOOP) patient survival by sex (P < .07). (b) Black race compared with nonblack race (P < .001). (c) Incorporation of human papillomavirus (HPV) status into tumor staging system (P < .001). (d) HPV status and overall survival for SCOOP patients (P < .001).
In addition to preliminary analyses of the existing VDW data, the VDW was used as a registry for further query into the primary electronic medical record for patients who had human papillomavirus (HPV) testing performed on their tissue; 168 patients were identified who had undergone HPV testing by querying the pathology reports for each patient in the primary medical record. Human papillomavirus positivity conferred a survival advantage for those patients in this preliminary analysis ( Figure 3 ).
This pilot study confirms that the HMO CRN has the potential for population-based studies of patients with head and neck cancers. Once a head and cancer cohort is established, this will be a powerful resource for both retrospective and prospective studies. Several unique aspects of this patient population can be leveraged for research. Since this patient population is within vertically integrated health systems, one unified medical record allows for queries that are not possible in other databases. This patient population is a community-based and completely insured population that can provide information on cancer treatment outcomes outside academic centers and clinical trials. Since all patients are insured, variations in outcome due to differential access to health care are largely avoided. Last, the setting of these health plans allows the deployment of interventions and real-time monitoring of their effects. For instance, adherence to guidelines for breast cancer treatment and outcomes after lumpectomy was studied in the HMO CRN. It was found that adherence was poor and an intervention was deployed within the health systems that could be monitored for its effectiveness.3,4 These studies are not possible with other databases such as the Surveillance, Epidemiology, and End Results (SEER) program.
Retrospective comparative effectiveness research within the CRN is subject to selection bias and confounding by indication. These require proper statistical assistance when analyzing data. Multivariate risk analysis, propensity score analysis, and instrumental variable analysis are methods to handle selection biases. In summary, the CRN is an untapped resource for head and neck cancer research. Investigators who are interested in collaborating can contact the head and neck working group. This study was approved by the Henry Ford Hospital Institutional Review Board.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Rick Krajenta, Christine Johnson, PhD, MPH, Virginia P. Quinn, PhD, MPH, and Lawrence H. Kushi, ScD.
No sponsorships or competing interests have been disclosed for this article.