
Abstract
Objective
Sphenopalatine artery ligation is a commonly employed surgical intervention for control of posterior epistaxis unresponsive to nasal packing. The objective of the present study was to evaluate the outcome of sphenopalatine artery ligation for control of epistaxis at our institution and the impact of timing and other factors on outcome.
Study Design
Case series with chart review.
Setting
Academic tertiary referral center.
Subjects and Methods
Case notes were reviewed for 45 consecutive patients undergoing sphenopalatine artery ligation for control of epistaxis between October 2008 and October 2014.
Results
Forty-one patients had nasal packing prior to sphenopalatine artery ligation, with 33 undergoing ≥2 packings. Postoperatively, 6 patients had rebleeding, which was treated with repacking (n = 4) and return to the operating room (n = 2). The overall success rate of sphenopalatine artery ligation was 87% (39 of 45). Rebleeding rate was not affected by concomitant septoplasty, anterior ethmoidal artery ligation, or postoperative nasal packing. Patients undergoing SPA ligation within the first 24 hours of admission had a significantly shorter hospital length of stay (3 vs 6 days, P = .02) and treatment cost (€5905 vs €10,001, P = .03). Length of stay was not influenced by sphenopalatine artery ligation after ≤1 nasal pack versus ≥2 packs. Timing of sphenopalatine artery ligation did not affect blood transfusion requirement (P = .84).
Conclusion
Sphenopalatine artery ligation is an effective management strategy for surgical control of refractory epistaxis. Early timing of sphenopalatine artery ligation may lead to reductions in length of stay.
Epistaxis is common otolaryngology emergency, with an estimated annual incidence of 108 cases per 100,000. 1 While most patients are successfully treated in an outpatient setting by nonoperative interventions such as nasal cautery or nasal packing, recalcitrant epistaxis may require hospital admission and can be associated with significant morbidity and even mortality. It has been reported that 5% to 15% of patients requiring admission for epistaxis will require surgical management. 2 Surgical intervention is more likely in the setting of posterior epistaxis, constituting 10% of all cases of epistaxis, due to higher failure rate of nasal packing in such cases (26%-52%).3,4
Treatment options for posterior epistaxis that is unresponsive to conventional nasal packing include surgical arterial ligation or radiologic arterial embolization. The promulgation of endoscopic nasal surgery over the last 2 decades has led to major shifts in surgical approaches to epistaxis, away from traditional approaches to the external carotid or internal maxillary artery and toward endoscopic approaches to the sphenopalatine artery (SPA). The SPA is the terminal branch of the maxillary artery, and it provides the main blood supply to the posterior nasal cavity. The SPA enters the nasal cavity from the pterygopalatine fossa through the sphenopalatine foramen, branching as it does to form the septal artery (supplying the posterior nasal septum) and the posterolateral nasal artery (supplying the lateral nasal wall, including the middle and inferior turbinates). 5 Endoscopic endonasal ligation of the SPA was described by Budrovich et al in 1992. 6 Since then, SPA ligation has gained in popularity, affording high success rate for control of epistaxis with low risk of major adverse outcomes.7-10
This study aimed to evaluate the clinical efficacy of SPA ligation for control of epistaxis at our institution and to investigate the impact of timing of SPA ligation on length of stay (LOS) and blood transfusion requirements. Secondary aims were to investigate the impact of concomitant surgical procedures (septoplasty or anterior ethmoidal artery [AEA] ligation) or postoperative nasal packing on SPA ligation success rates.
Materials and Methods
Following approval from the Cork Clinical Research Ethics Committee, a retrospective review was performed for all patients undergoing endoscopic SPA ligation for control of epistaxis in the South Infirmary Victoria University Hospital, Ireland, between October 2008 and October 2014. The South Infirmary Victoria University Hospital is the regional center for ear, nose, and throat (ENT) surgery in the Cork/Kerry region of Southern Ireland, with a population of 700,000, and is the sole referral unit for ENT emergencies.
Inclusion criteria for the present study were all patients undergoing SPA ligation for control of epistaxis during the study period. Cases were identified by review of the operating room register. Case notes of all patients were retrieved and clinical and operative parameters recorded.
Patients presenting to the ENT emergency room were assessed by an otolaryngology resident, with nasal packing performed in patients with persistent bleeding not amenable to nasal cautery. The most common initial nasal packs are Rapid Rhino (ArthoCare/Smith & Nephew) or BIPP (bismuth-iodoform paraffin paste). Nearly all patients admitted with epistaxis were treated initially by nasal packing, with SPA ligation reserved for intractable bleeding not controlled by nasal packs. However, there were no consistently applied criteria regarding timing of surgical intervention, which was also influenced by severity of bleeding, availability of operating room, and preferences of treating doctor. Thus, some patients with bleeding after a single nasal packing were managed by repacking the nose by a more experienced doctor and/or with a more effective nasal pack (eg, balloon packs). Others, particularly those with more minor oozing through packs, were initially observed in the expectation that this oozing would settle but subsequently underwent SPA ligation due to persistent oozing.
SPA ligation was performed endoscopically with a 0° telescope. We generally removed the lower half of the uncinate process and performed maxillary antrostomy, with enlargement of same toward the posterior maxillary wall. This is usually accomplished in <5 minutes and greatly facilitates access to the SPA. The SPA and branches are identified emerging from the sphenopalatine foramen after raising mucoperiosteum off the perpendicular plate of palatine bone. Commonly, a ridge of bone (the crista ethmoidalis) obstructs access to the SPA, which is removed with a 2-mm Kerrison rongeur. The SPA was then ligated with a metallic clip or bipolar electrocautery.
Success of SPA ligation was control of epistaxis without requirement for any further interventions. Cases requiring return to the operating room or repacking or cautery on the ward were considered failed cases.
Estimates of costs were based on information obtained from the hospital finance department and supplies department. The estimated cost of inpatient stay was based on mean daily cost of adult ENT inpatient bed of €1342. The estimated cost of SPA ligation was based on mean cost of inpatient endoscopic nasal procedure, including hospital stay of 1.71 days, of €4205. The mean cost of Rapid Rhino packs used for nasal packing in the emergency room or on the ward was €19.68.
Data analysis was based on XLSTAT 2015.1.03 (Addinsoft, France). A Fisher exact test was used on 2 × 2 contingency tables. As data regarding LOS and costs were skewed to the right, comparisons between groups were performed with the nonparametric Mann-Whitney test. Semielective cases of SPA ligation were excluded from analysis of impact of SPA timing on outcomes.
Results
Patient Demographics
During the study period, 45 patients (36 male, 9 female) underwent SPA ligation at our institution. Mean age was 62.6 ± 15.6 years. Most patients (n = 35, 77.8%) had at least 1 medical comorbidity. Nineteen patients (42%) were on oral antiplatelet or other anticoagulant therapy at the time of presentation ( Table 1 ).
Patient Demographics. a
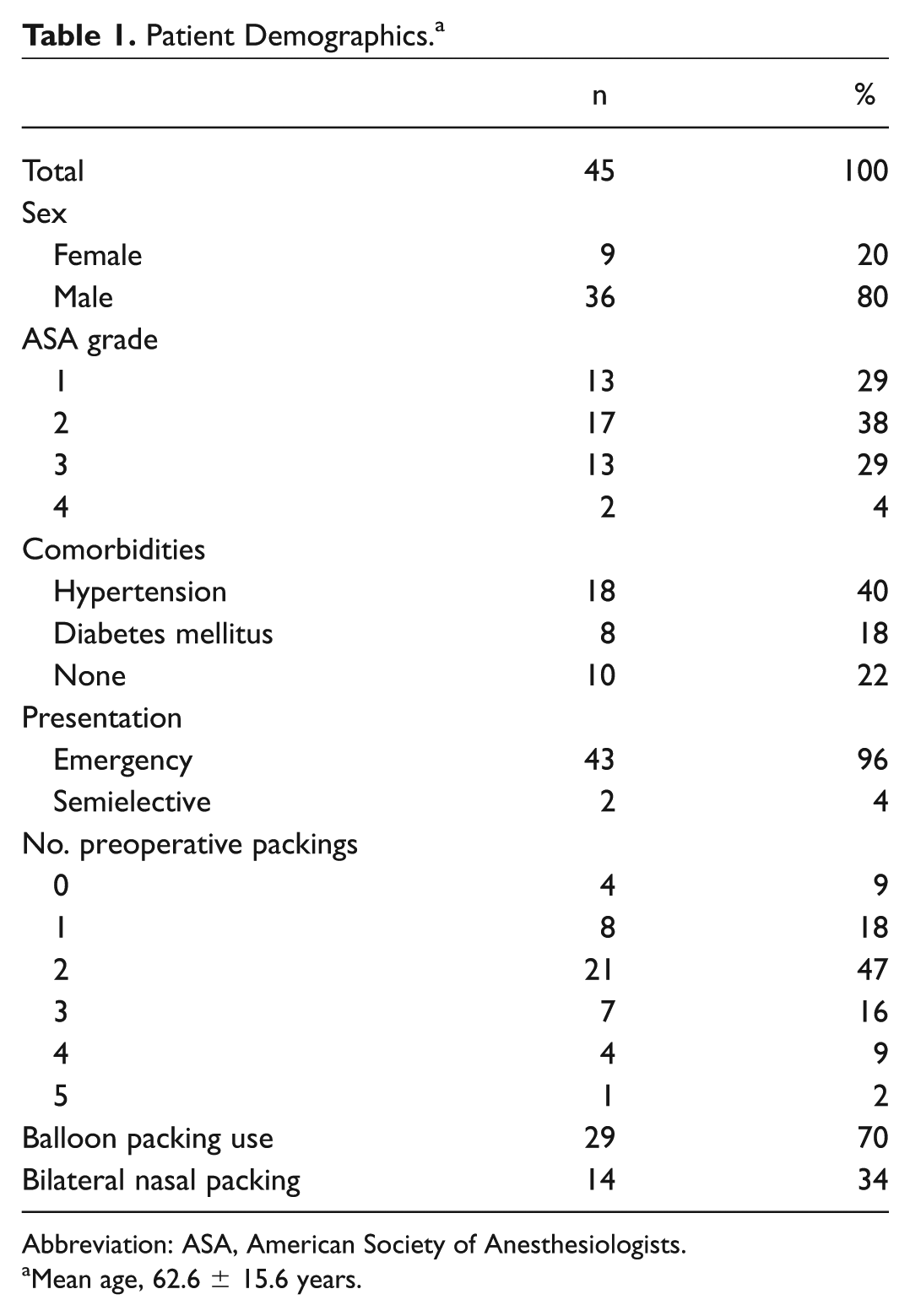
Abbreviation: ASA, American Society of Anesthesiologists.
Mean age, 62.6 ± 15.6 years.
Preoperative Parameters
Forty-three patients presented as emergencies. Two patients underwent SPA ligation as a semielective procedure for recurrent epistaxis requiring hospital admission. These patients were excluded from analysis of impact of SPA timing on outcomes. Forty-one patients had undergone nasal packing at initial presentation, with 33 undergoing ≥2 preoperative nasal packings. Fourteen patients (34%) required nasal packs to be placed bilaterally, and 29 (70%) required balloon packs. Three patients had other surgical procedures prior to SPA ligation (1 septoplasty and cautery, 2 AEA ligation). One patient had undergone radiologic bilateral internal maxillary artery embolization prior to SPA ligation.
Operative Parameters
Mean time to ligation from hospital admission was 2.8 ± 2.2 days (median, 2 days). There were no significant differences between patients undergoing SPA ligation within 1 day and those undergoing ligation after 1 day in terms of age (P = .47), sex (P = .71), antiplatelet/anticoagulant use (P = .55), American Society of Anesthesiologists grade (P = .29), number of preoperative packs (P = .82), or preoperative haemoglobin concentration (P = .89). One patient underwent bilateral SPA ligation; 11 (26.6%) underwent concomitant septoplasty. One further patient underwent concomitant AEA ligation. The majority of arteries were ligated with clipping alone (n = 31, 69%). Bipolar diathermy alone was used in 8 cases (18%). Floseal (Baxter Healthcare Corporation, Deerfield, Illinois) was applied to the surgical site at the end of SPA ligation in 3 (6.7%) cases. Ten patients (22.2%) underwent nasal packing at the end of the procedure. Procedural details are presented in Table 2 .
Procedural Details. a
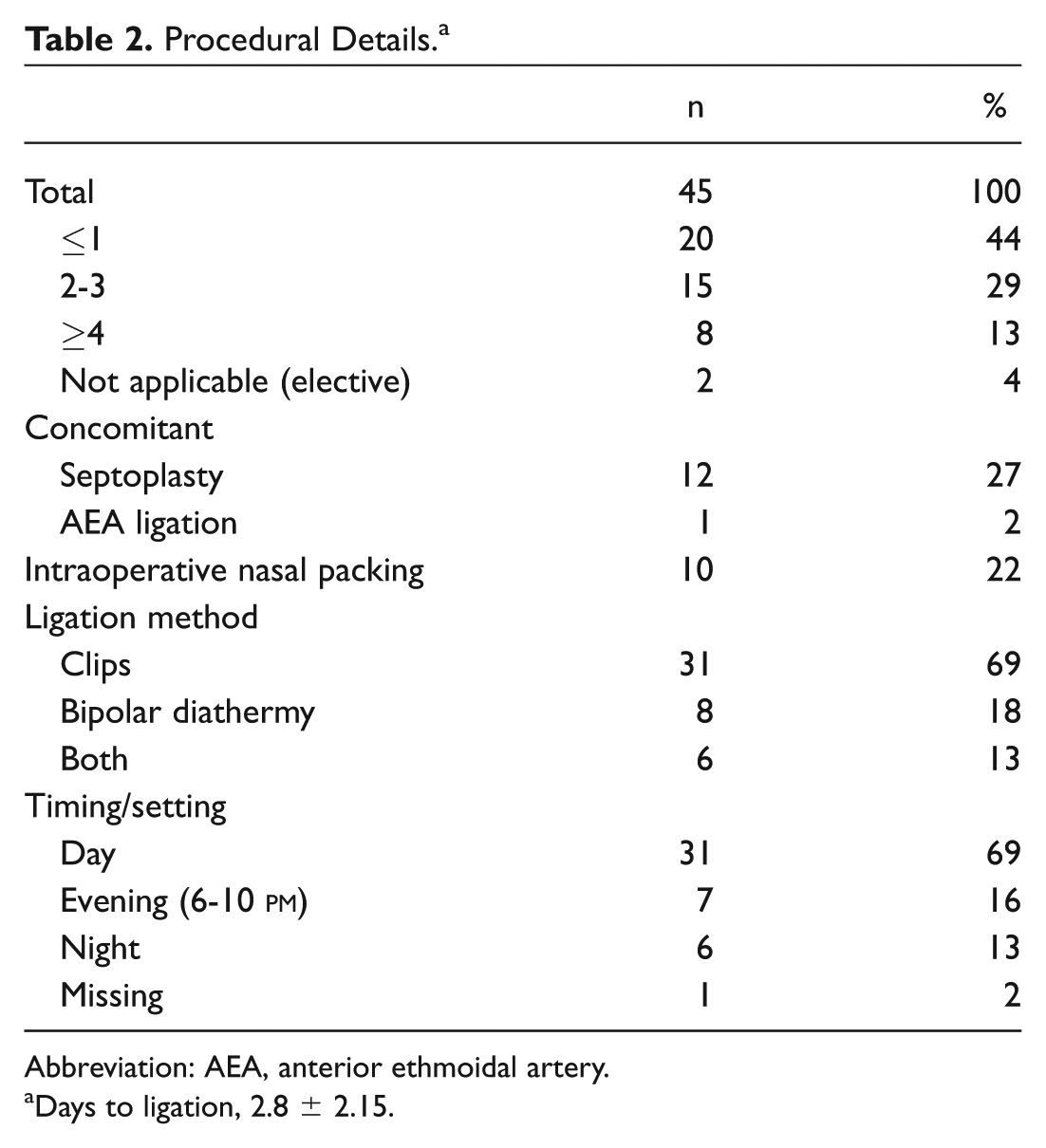
Abbreviation: AEA, anterior ethmoidal artery.
Days to ligation, 2.8 ± 2.15.
Surgical Outcomes
Thirty-nine patients had no further bleeding, giving a success rate for SPA ligation of 87%. Six patients had further bleeding. This was treated by repacking on the ward in 4 patients (1 bismuth-iodoform paraffin paste, 3 Merocel [Medtronic Inc]) and by return to the operation room in 2 patients. Operative procedures on these 2 patients were ipsilateral AEA ligation (n = 1) and ipsilateral AEA artery plus internal maxillary artery ligation (n = 1).
There was no significant difference in rebleeding rates according to use of postoperative nasal packs (10% vs 15%, P > .99) or performance of concomitant septoplasty (9% vs 16%, P > .99). Use of antiplatelet or anticoagulants prior to admission did not influence rebleeding rates after SPA ligation (16% vs 12.5%, P > .99). The rate of rebleeding among patients undergoing early SPA ligation (≤1 day of admission) was 25% (5 of 20) versus 4% (1 of 23) among patients undergoing delayed SPA ligation (>1 day after admission, P = .08).
Mean LOS was 5.4 ± 3.0 days (median, 5 days). The median LOS among patients undergoing early SPA ligation (≤1 day of admission) was 3 days versus 6 days in patients undergoing SPA ligation >1 day after admission (P = .02). There was no significant difference in LOS between patients undergoing SPA ligation after ≤1 nasal pack (median, 4.5 days) and those undergoing SPA ligation after ≥2 nasal packs (5 days; P = .84).
Thirteen (28.9%) patients required blood transfusion. Blood transfusion was generally avoided as much as possible. The decision to transfuse was made on an individual basis, taking into consideration age of patient, estimated blood loss, hemoglobin concentration, cardiac comorbidity, vital signs, and other symptoms. Median LOS among patients receiving blood transfusion was significantly longer than that among patients not requiring transfusion (8 vs 4 days, P < .001). There were no significant differences in blood transfusion requirements between patients undergoing SPA ligation ≤1 day after admission and >1 days after admission (20% vs 39%, P = .2) and between those undergoing SPA ligation after ≤1 nasal packing and after ≥2 packings (18% vs 31%, P = .7, respectively).
There were no reported operative complications.
Cost Analysis
The median cost of treatment for patients undergoing early SPA ligation was €5905 (range €3252-€20,738) and for patients undergoing late SPA ligation, €10,001 (range, €5678-€22,119). The difference in cost was significant (P = .03).
Discussion
The surgical management of epistaxis has evolved over the past few decades. With the expansion of endoscopic endonasal surgery, SPA ligation has become a popular choice for surgical control of posterior epistaxis. In the present paper, we report a success rate of SPA for treatment of epistaxis of 87%. Reported success rates of SPA ligation in the literature range from 87% to 98%. It is possible that some of the variability in reported success rates is related to the differing definitions of “success” (repeat epistaxis requiring packing vs repeat epistaxis requiring return to operating room), as well as variations in the size of patient cohorts included and variable severity of epistaxis cases undergoing SPA ligation.8,11,12 Early studies on small patient cohorts (n ≤ 12) reported success rates of 100%.9,13,14 George et al reported a success rate based on return to operating room of 89% (17 of 19). 15 To our knowledge, only 1 study reported on a sample size greater than the one described herein (n = 50) and reported a success rate of 87%. 16 Kumar et al reported a success rate of 98% for SPA ligation across 11 case series and 128 patients but failed to comment on the accepted definition of “failure.” 8
Reasons for failure of SPA ligation may include slipping of surgical clips, failure to identify all branches of the SPA,17,18 or bleeding from branches of the internal carotid artery (AEA or posterior ethmoid artery). With this in mind, it is critical to identify and ligate all branches of the SPA or to ligate the SPA proximally prior to branching. The latter maneuver is facilitated by removal of bone toward the pterygopalatine fossa with a Kerrison rongeur. The number of branches of the SPA varies from 1 (ie, no branching) to 2 or 3 branches, with a frequency of 62%, 32%, and 5%, respectively. 19 Unfortunately, the number of branches of the SPA identified and ligated in the present study was not always consistently documented, and so we could not analyze the impact of this on outcomes in the present series.
Other suggested measures to minimize rebleeding after SPA ligation include postoperative nasal packing and concomitant AEA ligation. The results of this study suggest that routine nasal packing at the end of the procedure does not influence rebleeding rates and, as such, is not routinely necessary. Regarding concomitant AEA ligation, Asanau et al conducted a retrospective comparison of bilateral SPA ligation alone (group A, n = 20) and bilateral SPA ligation with concomitant bilateral AEA ligation (group B, n = 25). 20 Only 1 patient in group A required subsequent AEA ligation. In the present study, 3 patients underwent AEA ligation either prior to or concomitant with SPA ligation. Of the remaining 40 emergency patients, only 2 (5%) required return to the operating room for AEA ligation. This findings suggest that the risk of rebleeding after SPA ligation due to not performing concomitant AEA ligation is low. Considering the additional potential morbidity of AEA, we thus advocate that routine AEA ligation at the same time as SPA ligation is not necessary, provided that bleeding is well controlled at the time of completion of SPA ligation.
The optimum timing of SPA ligation—based on consideration of patient outcomes and cost of care—is controversial. Lakhani et al proposed the Wexham criteria, a set of guidelines to facilitate patient selection and timing for SPA ligation. 21 In brief, the Wexham criteria are as follows: posterior nasal packing by an ENT specialist registrar or equivalent, blood transfusion requirement or a drop in hemoglobin >4 g/dL, recurrent epistaxis (>3) requiring repeated packing during admission, and repeated hospital admission for recurrent epistaxis (>3 episodes in a 3-month period). However, Moshaver et al recommended early SPA ligation based on their findings of significant reduction in cost and length of hospitalization for patients undergoing immediate SPA ligation, in comparison with conventional nasal packing after failure of Merocel nasal packs. 22
In the present study, patients undergoing early SPA ligation (≤1 day after admission) had a significantly shorter LOS than did those undergoing SPA ligation >1 day after admission. There was no difference in blood transfusion requirements. We also found a significant cost reduction for patients undergoing early SPA ligation. However, it should be cautioned that our cost analysis were estimates based on the average cost of inpatient endoscopic nasal surgery procedures and average adult ENT inpatient bed cost, rather than specific costing of SPA ligation. To our knowledge, there has not been a published comparison of cost-effectiveness of early versus late SPA ligation. However, our results are consistent with the findings of a National Inpatient Sample review that demonstrated a benefit for early intervention for epistaxis (surgery or embolization) with respect to LOS and total charges. 23
There was a trend for more surgical failures among patients undergoing early SPA ligation; however, this was not significant. It is likely that given the use of SPA as a second-line procedure at our institution, it is possible that the early SPA cohort contained a greater number of very severe cases, which may have biased this comparison. Cases with rebleeding composed most of the LOS outliers in the early SPA ligation group, along with 2 other patients developing medical complications. However, the more timely discharge of the remaining patients in this group meant that the median LOS remained significantly less than that of patients undergoing later SPA ligation.
Alternatives to surgical intervention for recalcitrant epistaxis include percutaneous arterial embolization. Arterial embolization has been shown to be effective for treatment of recalcitrant epistaxis.
24
However, this approach requires a specialist interventional radiologist and is available to our patient cohort only between 9
Limitations of this study include the retrospective nature and heterogeneous patient cohort. In addition, the cohort size was relatively small. However, this series nevertheless constitutes one of the largest reported cohorts of patients undergoing SPA ligation. Finally, as most patients were not routinely followed up after hospital discharge, it was not possible to comment on long-term sequelae or outcomes. However, given that our unit contains the only ENT emergency department in the region, it is almost certain that any patients rebleeding after hospital discharge would have been rereferred back to us.
However, strengths of the study include the fact that nearly all patients undergoing SPA ligation had genuinely intractable epistaxis, as evidenced by the large number of patients undergoing multiple nasal packings prior to surgery, with 70% requiring balloon packs and nearly 30% requiring blood transfusion. The success rate of SPA ligation of 87% in this cohort, even without requirement for nasal packing at the end of the procedure, would thus strongly support the effectiveness of SPA ligation in refractory epistaxis.
Conclusion
SPA ligation is a safe and effective method for treatment of intractable epistaxis and should be considered early in the management of epistaxis arising from posterior bleeds. We found early SPA ligation to lead to significant reductions in hospital LOS but not blood transfusion requirements.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.