
Abstract
Background
Intractable posterior epistaxis sometimes requires intensive treatment, such as surgery or embolization. Maxillary artery ligation has been widely used for the treatment of intractable posterior epistaxis. It is highly effective, but significant complications may occur, including an oroantral fistula and damage to the infraorbital nerve. Embolization is less invasive and can be performed in poor surgical candidates. However, it has more serious complications, such as facial nerve paralysis and hemiplegia. This investigation evaluates the effectiveness and complications of endoscopic ligation of the sphenopalatine or maxillary artery for the treatment of intractable posterior epistaxis.
Methods
Between April 2003 and March 2007, 46 patients were hospitalized for the treatment of severe posterior epistaxis in our University Hospital. Thirty patients were successfully treated by anterior and/or posterior nasal packing, and five patients were treated by electrocoagulation. Endoscopic ligation was performed under general anesthesia in 11 patients (6 men and 5 women; age range, 50-80 years).
Results
Eight patients underwent endoscopic ligation of the sphenopalatine artery, and three patients underwent endoscopic ligation of the maxillary artery through the middle meatus and posterior antral wall opening. There were no complications, and the patients’ postoperative courses were uneventful. Recurrent epistaxis occurred in one patient on oral anticoagulants 15 months after ligation of the sphenopalatine artery, and it was successfully treated by anterior nasal packing.
Conclusion
Endoscopic ligation of the sphenopalatine or maxillary artery is safer than arterial embolization and is less invasive than transantral ligation of the maxillary artery. This technique appears to be a simple and highly effective surgical treatment for patients with intractable posterior epistaxis.
Keywords
Chandler and Serrins 2 were the first to describe transantral ligation of the maxillary artery in 1965, and it has been widely used for the treatment of intractable posterior epistaxis. It is highly effective, but significant complications may occur, including an oroantral fistula and damage to the infraorbital nerve. 1 Recently, the endoscopic transnasal approach for ligation of the sphenopalatine artery has been reported.3–5 It has a high success rate and no major complications.
In this article, our experience with endoscopic ligation of the sphenopalatine artery for the treatment of severe posterior epistaxis is presented. Endoscopic ligation of the maxillary artery through the middle meatus and posterior antral wall opening is also described. The success rate and complications of these techniques are discussed.
Subjects
Between April 2003 and March 2007, 46 patients (32 men and 14 women) were hospitalized for the treatment of intractable epistaxis at the Department of Otorhinolaryngology, Shiga University Hospital. Thirty patients (65.2%) were successfully treated by anterior and/or posterior nasal packing, and five patients (10.9%) were treated by electrocoagulation. Endoscopic ligation of the sphenopalatine artery or maxillary artery was performed in 11 patients (23.9%; 6 men and 5 women).
Methods
Endoscopic Ligation of the Sphenopalatine Artery
All operations were performed under general anesthesia with controlled hypotension (Fig. 1). To detect the sphenopalatine foramen, the first step is to identify the posterior wall of the maxillary sinus as the landmark. After removing the un-cinate process, the posterior wall of the maxillary sinus is exposed through the opening of the middle meatus. With this landmark in mind, a vertical incision is made inferior to the posterior portion of the middle turbinate. A small mucoperiosteal flap is raised backward and upward, until the sphenopalatine foramen is encountered. 6 The fibroneurovascular sleeve is identified where it protrudes from the sphenopalatine foramen. After isolating the artery, the vascular clips (Hemoclip; Weck Closure Systems Research, Triangle Park, NC) are applied under direct vision. The mucoperiosteal flap is then returned to its original position.
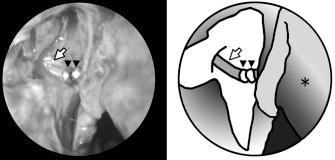
Endoscopic ligation of the right sphenopalatine artery. The right sphenopalatine artery (white arrow) was ligated with titanium clips (arrowhead). Right middle turbinate (asterisk) is shown.
Endoscopic Ligation of the Maxillary Artery
This technique is an endoscopic alternative to usual transantral ligation of the maxillary artery (Fig. 2). After removing the uncinate process, the maxillary sinus is widely opened through the middle meatus. A mucoperiosteal flap is elevated from the posterior wall of the maxillary sinus. The posterior wall is removed with a curette or chisel, and this opening is enlarged with biting forceps and hooks. Then, the posterior layer of the periosteum is opened using a fine instrument. The maxillary artery is exposed in the adipose tissue just beneath the periosteum. After isolating the artery and its branches, such as the sphenopalatine artery and the descending palatine artery, the vascular clips are applied both to the proximal main trunk and to the distal branches of the maxillary artery.
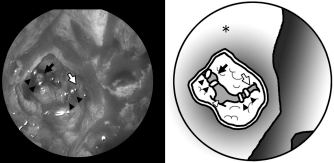
Endoscopic ligation of the right maxillary artery. The right maxillary artery (black arrow) and sphenopalatine artery (white arrow) were ligated with titanium clips (black arrowhead) through the middle meatus and posterior antral wall. Posterior wall of right maxillary sinus (asterisk) and descending palatine artery (white arrowhead) are shown.
Results
Endoscopic ligation of the sphenopalatine artery was performed unilaterally in seven patients and bilaterally in one patient with Osler's disease. For clipping the artery, the Hemoclip developed for neurosurgery was used. It requires large forceps and sometimes can not be used for ligation of the sphenopalatine artery in patients with a narrow nasal cavity. When the nasal cavity was too narrow to use the Hemoclip, endoscopic ligation of the maxillary artery was chosen in three patients. It was possible to identify the sphenopalatine artery and the maxillary artery in all cases, with successful outcomes using these surgical techniques alone. External ligation of the ethmoidal arteries was not required. There were no complications during or after the surgery, and the patients’ postoperative courses were uneventful. Recurrent epistaxis occurred in one patient (9.1%) on oral anticoagulants 15 months after ligation of the sphenopalatine artery and was successfully treated by anterior nasal packing.
Discussion
Budrovich and Saetti 3 were the first to report endoscopic ligation of the sphenopalatine artery in 1992. Recently, it has become a safe and effective surgical technique for the treatment of posterior epistaxis. Some minor complications, including nasal crusting, acute sinusitis, and paresthesiae of the palate and nose, have been noted, but no major complications have been reported.7,8
Endoscopic coagulation of the sphenopalatine artery has also been reported. 9 Occlusion of an artery with transsection and coagulation of both bleeding ends has been recommended, because an artery treated with coagulation only may recanalize within a few days. We feel that clipping of the artery is safer than coagulation, because inadequate coagulation leaves the vessel still patent. In addition, there is the risk of retraction of the bleeding pedicle into the pterygopalatine fossa.
This is the first report to describe endoscopic ligation of the maxillary artery through the middle meatus and posterior antral wall opening. Endoscopic ligation of the maxillary artery was used for patients with a narrow nasal cavity. If appropriate clip applicators are available, endoscopic ligation of the sphenopalatine artery can be performed in all patients. However, this technique will be useful for the treatment of epistaxis arising from the sphenopalatine foramen, and it is possible without removing the packing of the posterior middle meatus. This technique will be also helpful for endoscopic resection of nasal tumors to reduce intraoperative bleeding.
The maxillary artery and the sphenopalatine artery are important for the posterior part of the nose, both on the lateral wall and on the septum. 10 Posterior epistaxis can be controlled by ligation of these arteries. Ethmoidal arteries are responsible for epistaxis from the superior portion of the nasal cavity. If ligation of the sphenopalatine or maxillary artery is not effective, although it is very rare, external ligation of the ethmoidal arteries may be the next choice of surgical treatment. In our experience, external ligation of the ethmoidal arteries was not needed.
Cross circulation from the contralateral maxillary artery may cause recurrent bleeding. The dominant maxillary artery was observed in >50% of cases on cadaveric dissections. 11 If the maxillary artery of the affected side is too fine, ≤4 mm in diameter, bilateral ligation may be necessary to prevent late bleeding. In our experience, bilateral ligation of the spheno-palatine artery was only performed in a patient with Osler's disease who had bilateral intractable bleeding.
In the present study, there were no complications, and the success rate (91%) was higher than that with selective arterial embolization, which rarely had serious complications such as hemiplegia and facial nerve paralysis. This success rate is coincident with that of other reports using transantral ligation of the maxillary artery and endoscopic ligation or coagulation of the sphenopalatine artery. 1
Conclusion
Endoscopic ligation of the sphenopalatine or maxillary artery is a simple and safe technique with a high efficacy that should be considered early in the management of intractable posterior epistaxis.