
Abstract
Objective
With the emergence of transoral robotic approaches, head and neck surgeons are faced with an unfamiliar inside-out head and neck anatomy. This study was performed to describe key anatomic landmarks and surgical considerations of transoral robotic resection of the lateral oropharyngeal wall, the parapharyngeal space, and the base of the tongue.
Study Design
Descriptive transoral anatomic study.
Setting
Academic anatomy laboratory and tertiary academic hospital.
Subjects and Methods
Transoral dissections of the lateral pharyngeal wall, base of tongue, and parapharyngeal space were performed in 5 vascular silicone-injected cadavers to illustrate anatomic landmarks from the inside-out perspective. Lateral neck dissections were also performed to better appreciate the anatomic structures and to be more familiar with intraoperative anatomy.
Results
The neurovascular and muscular structures located in parapharyngeal space, lateral oropharyngeal wall, and base of tongue were described. Surgical significance of key anatomic landmarks was emphasized with high-quality illustrations.
Conclusion
A thorough understanding of transoral anatomy is crucial to perform transoral robotic surgery safely and efficiently. To understand inside-out anatomy of base of tongue, lateral oropharyngeal wall, and parapharyngeal space, cadaveric dissection is highly beneficial and may help to shorten the learning curve for transoral robotic dissections.
One of the main disadvantages of traditional open approaches to resect oropharyngeal tumors is that it requires external incisions and extensive dissection of uninvolved anatomic structures. Minimally invasive approaches such as transoral robotic surgery (TORS) avoid dissection of uninvolved tissues and ensures safe resection of the lateral oropharyngeal wall, base of tongue, and parapharyngeal tumors without requiring an external incision.1-4
One of the main challenges of using TORS is the complex transoral anatomy of the oropharynx and parapharyngeal spaces. Surgeons are most familiar with the lateral-to-medial direction of head and neck anatomy. The robotic surgeon needs to master the inside-out anatomy of these spaces.5,6 Limited transoral robotic experience and poor anatomic knowledge can cause significant morbidities.
The purpose of this study was to describe the inside-out surgical anatomy of the lateral oropharyngeal wall, parapharyngeal space, and base of tongue in silicon-injected fresh cadaveric specimens and to emphasize the key anatomic landmarks for robotic surgeons.
Materials and Methods
The study was approved by the Committee for Oversight of Research Involving the Dead at The Ohio State University Wexner Medical Center. Five fresh cadaveric specimens were used for anatomic dissections at the Anatomy Laboratory toward Visuospatial Surgical Innovations in Otolaryngology and Neurosurgery (ALT-VISION) skull base laboratory. All specimens were prepared via a standardized protocol including vascular silicone injections. 7
A Crowe-Davis oral retractor (Storz, Heidelberg, Germany) was inserted to visualize the oropharynx. All dissections were performed via an endoscopic transoral approach with a 2-surgeon / 3- to 4-hand technique 8 with a 0º lens endoscope (for oropharyngeal dissections) and a 30º lens endoscope (for base-of-tongue dissections) coupled to a camera and monitor system (Karl Storz Endoscopy-America, El Segundo, California). All cadaveric pictures were taken by the same camera system.
First, the lateral pharyngeal wall and its mucosal structures were observed and defined. To define the deep adjacent structures of the lateral oropharyngeal wall, parapharyngeal space, and base of tongue, initial resection was begun with classical tonsillectomy ( Figure 1 ) and then continued with resection of the base of tongue.
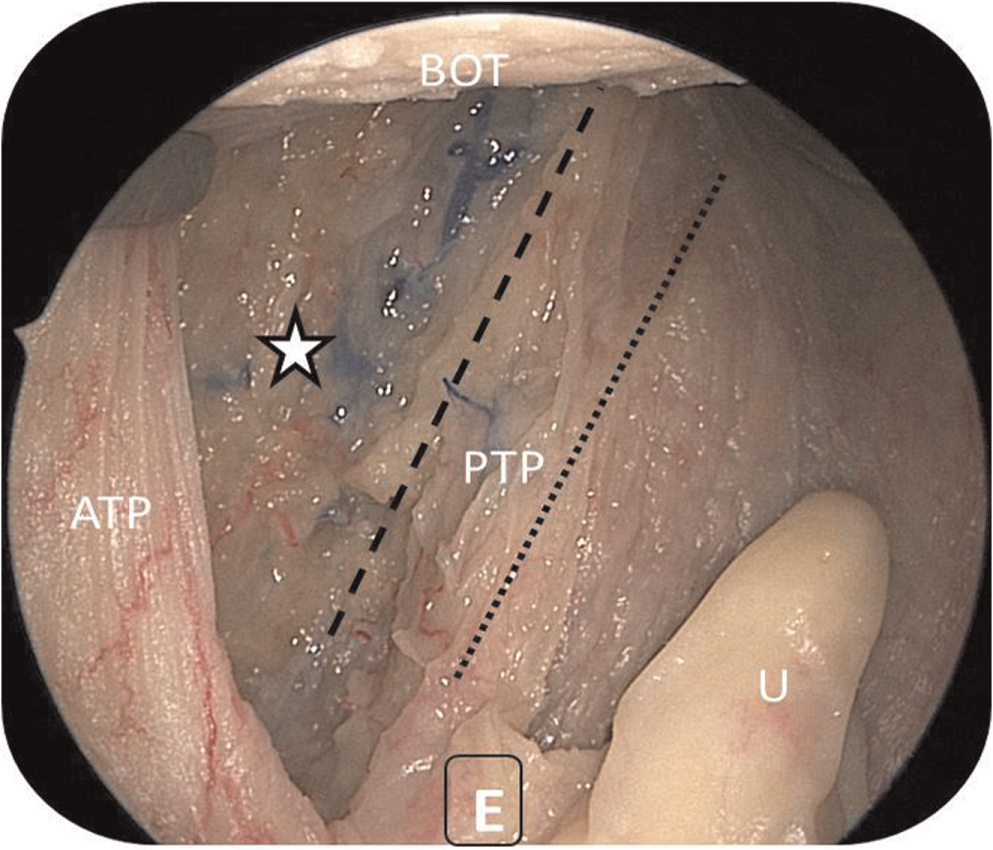
The view of tonsillar fossa after tonsillectomy. ATP, anterior tonsillar pillar; BOT, base of tongue; PTP, palatopharyngeal muscle; U, uvula. Dotted line, palatopharyngeus muscle; dashed line, stylohyoid ligament; star, pharyngobasilar fascia.
In the second part of the dissection, the superior pharyngeal constrictor muscle was incised where it meets the buccinator muscle (at the edge of the anterior tonsillar pillar; Figure 2 ), and then the constrictor muscle was retracted medially and resected. The identification of structures lying within the parapharyngeal space located lateral to the tonsillar fossa was accomplished by removal of the parapharyngeal fat pad ( Figure 3 ).
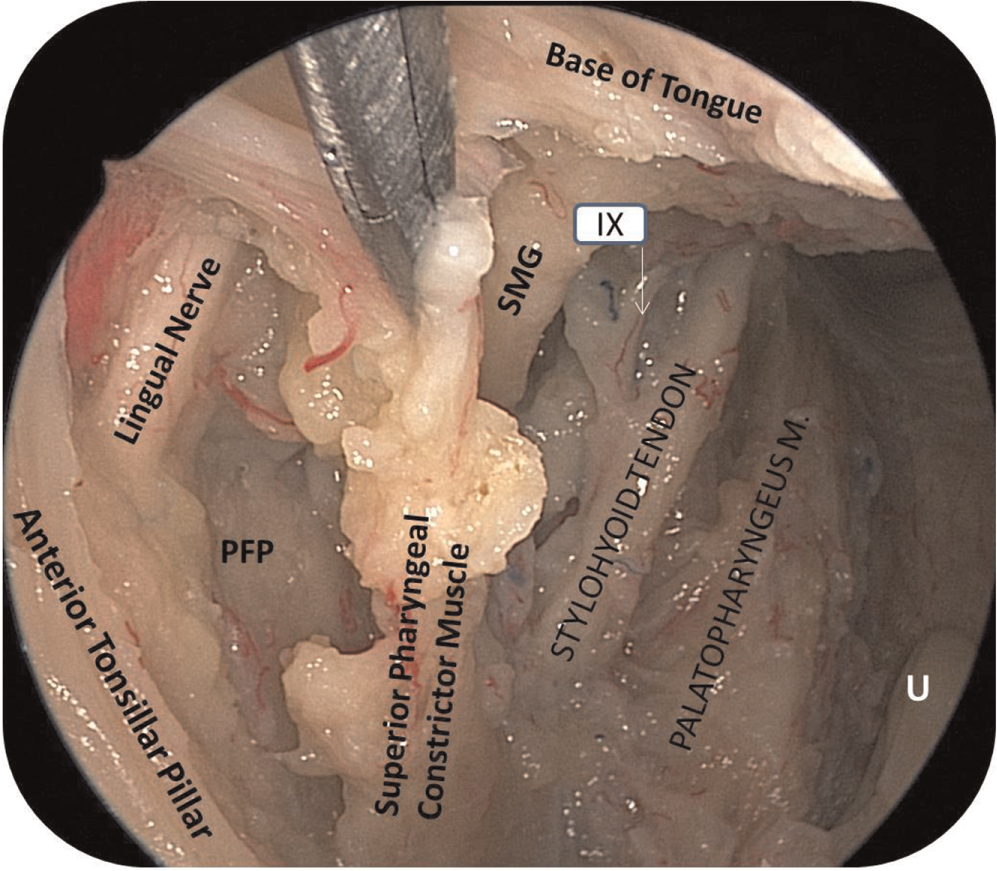
The transoral view of the left parapharyngeal space and its content after resection of pharyngobasilar fascia. IX, glossopharyngeal nerve; PFP, parapharyngeal fat pad; SGM, styloglossus muscle; U, uvula.
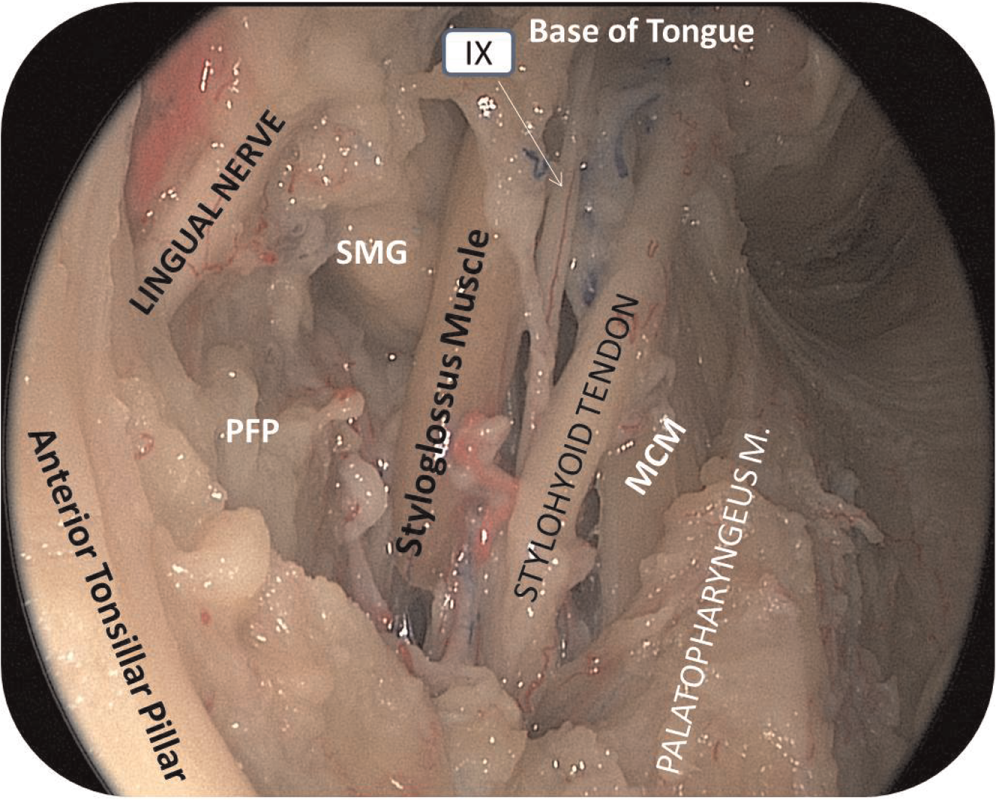
The view of the deep parapharyngeal space after resection of the superior constrictor pharyngeus muscle and partial removal of the parapharyngeal fat pad. IX, glossopharyngeal nerve; MCM, median constrictor pharyngeus muscle; PFP, parapharyngeal fat pad; SMG, submandibular gland.
Lateral neck dissections were also performed to confirm the structures that were identified transorally in parapharyngeal space. This facilitates the orientation of surgeons to the new perspective of anatomy ( Figure 4 ).
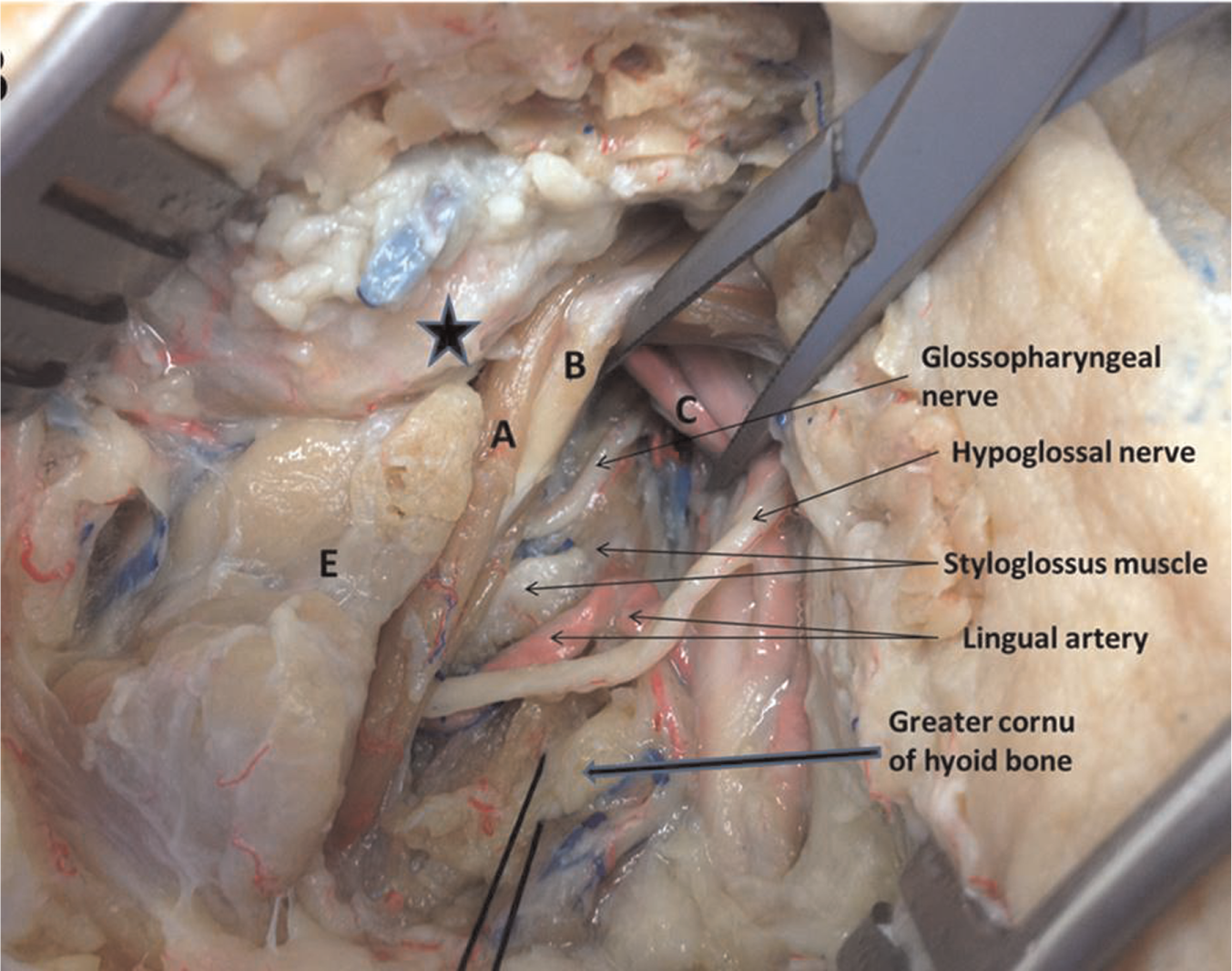
Parapharyngeal structures at the level of tonsillar fossa from lateral aspect of the neck. A, stylohyoid muscle; B, posterior belly of digastric muscle; C, facial artery; E, submandibular gland. Star, corner of mandible.
Results
During the initial resection, the tonsillar branch of glossopharyngeal nerve, the tonsillar branch of the facial artery, and the tonsillar vein were identified. Following the initial resection, pharyngobasilar fascia, the trajectories of the stylohyoid ligament and the palatopharyngeus muscle were then identified ( Figure 1 ). After the resection of pharyngobasilar fascia ( Figure 1 ), the superior pharyngeal constrictor muscle was identified as forming the lateral wall of tonsillar fossa superiorly. Middle pharyngeal constrictor and styloglossus muscles and the stylohyoid ligament were identified as constituting the inferior part of tonsillar fossa ( Figures 2 , 3 ). The trajectory of the styloglossus muscle and the stylohyoid ligament was observed in between superior and middle pharyngeal constrictor muscles in a posterolateral-to-anteromedial fashion ( Figures 2 , 3 ). The styloglossus muscle courses from lateral-to-medial and posterior-to-anterior directions toward the base of tongue and interdigitates with intrinsic longitudinal lingual muscle fibers ( Figure 4 ). The stylohyoid ligament is located between stylopharyngeus and styloglossus muscles and inserts to the hyoid bone medially ( Figures 2 , 3 ). The stylopharyngeus is a slender muscle, cylindrical above, flattened below. It extends downward posterolaterally to the stylohyoid ligament and passes between superior and middle pharyngeal constrictor muscles; some of its fibers merge with palatopharyngeus muscle fibers and middle pharyngeal constrictor muscle fibers as well as pharyngeal mucosa.
The lingual artery travels in an anteromedial direction from its origin toward the lateral base of the tongue. At its origin, the lingual artery lies deep laterally to the middle pharyngeal constrictor muscle between the posteroinferior aspect of the stylohyoid ligament and greater cornu of the hyoid bone posteriorly. At the junction of styloglossus muscle and the base of tongue, the lingual artery passes lateral and beneath styloglossus muscle ( Figure 5 ). Dorsal lingual branches of the lingual artery can be observed medial to styloglossus muscle ( Figure 6 ).
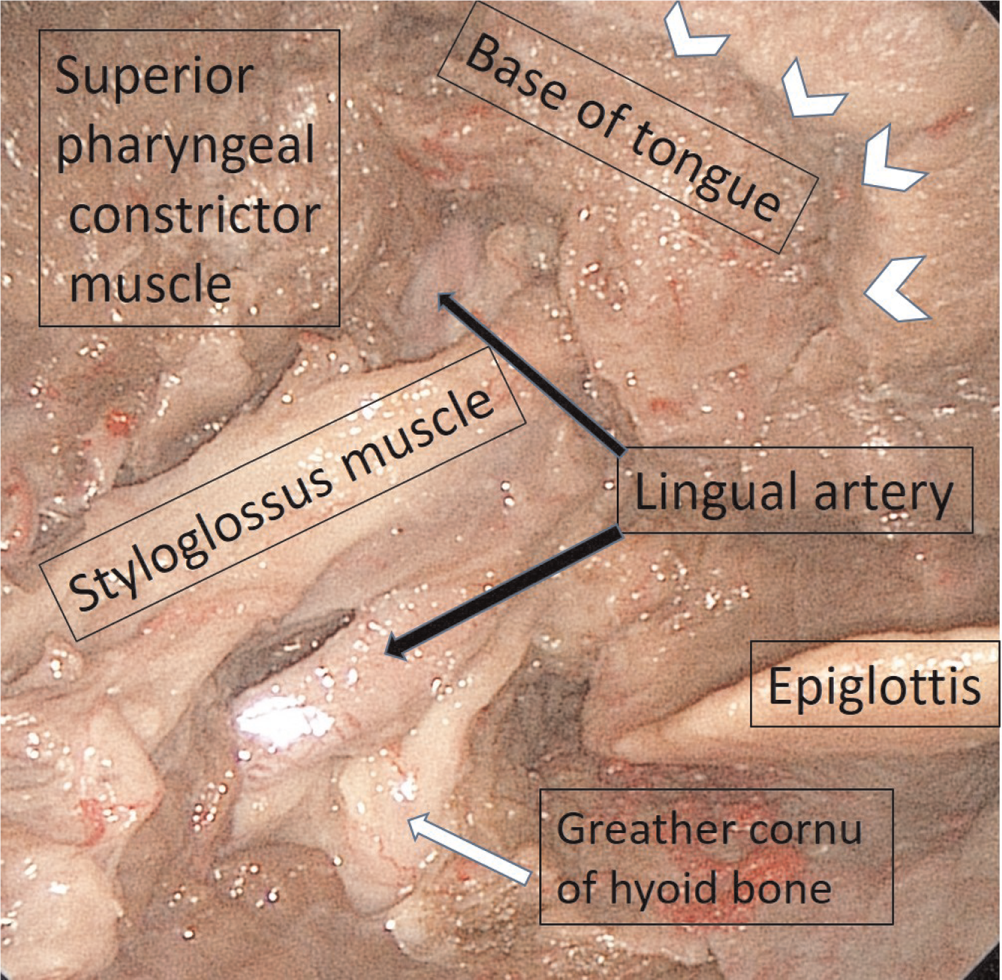
The view of deep lingual musculature and tonsillar fossa after resection of left palatine tonsil and left side of the base of tongue. Arrowheads, resection margins of the base of tongue.
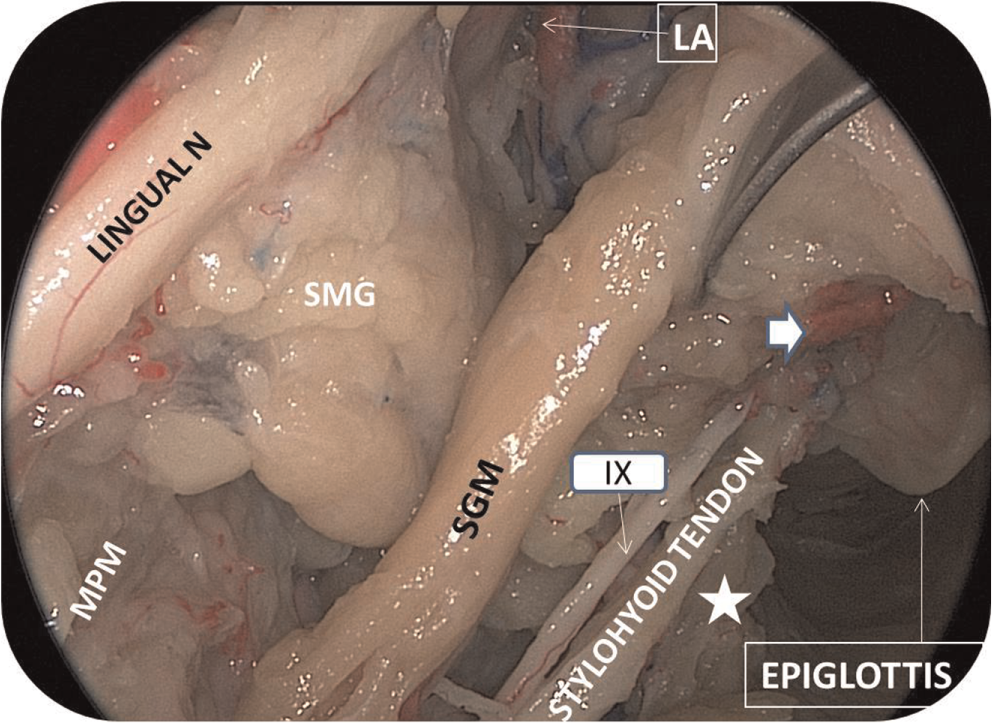
The trajectory of lingual artery and the structures lying deep to parapharyngeal space. IX, glossopharyngeal nerve; LA, lingual artery; MPM, medial pterygoid muscle; SGM, styloglossus muscle; SMG, submandibular gland. Arrow, dorsal branch of lingual artery; star, greather cornue of hyoid bone.
The glossopharyngeal nerve crosses the stylopharyngeus muscle posteriorly and is situated inferomedially in between the stylohyoid ligament and the styloglossus muscle. It can branch off within the tonsillar fossa ( Figure 2 ). These branches travel posteroinferiorly in the tonsillar fossa toward the base of tongue.
Following the second part of the dissection (dissection of superior pharyngeal constrictor muscles) ( Figure 2 ), the parapharyngeal fat pad was noted lateral to the pharyngeal constrictor muscles ( Figure 3 ). Muscular and vascular structures located in the parapharyngeal space were exposed after removal of the fat pad. The inferomedial wall of the parapharyngeal space is bounded by the lateral aspect of the tonsillar fossa (superior and medial pharyngeal constrictor muscles). The lateral wall of the parapharyngeal space at the level of the tonsillar fossa is limited by the medial pterygoid muscle and mandibular ramus ( Figure 7 ).
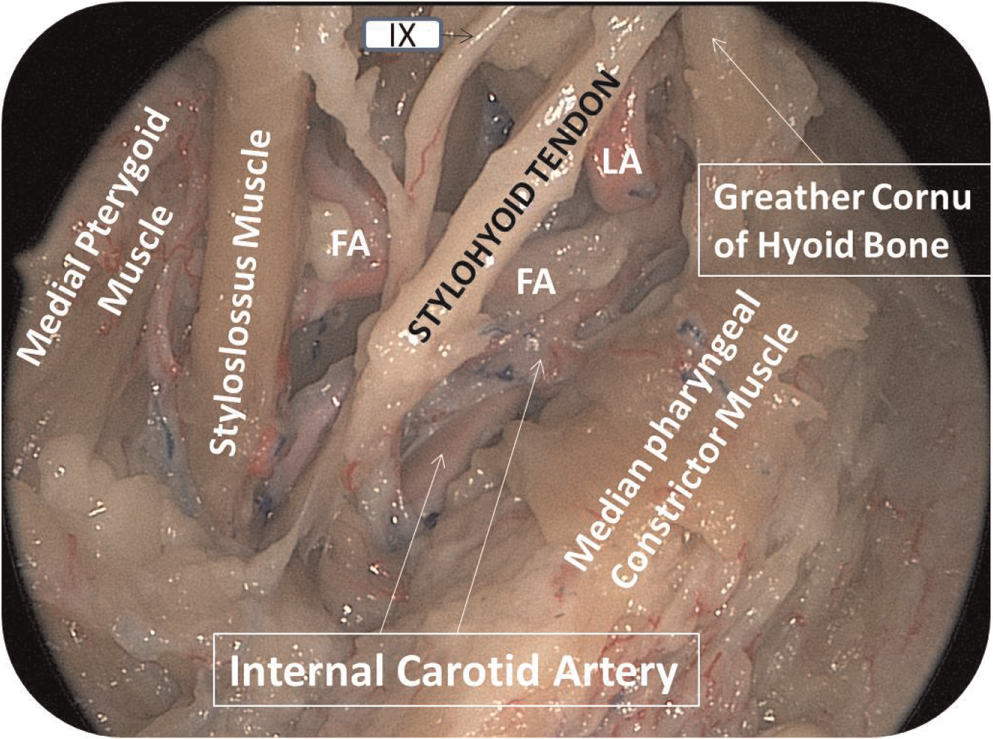
The view of the structures lying deep to parapharyngeal space after removal of parapharyngeal fat pad. FA, facial artery; IX, glossopharyngeal nerve; LA, lingual artery.
The curves of the internal maxillary, facial, and lingual arteries were located lateral to the stylopharyngeus and styloglossus muscles and the stylohyoid ligament within the parapharyngeal space. These vascular structures are bounded laterally by posterior belly of digastric and stylohyoid muscles ( Figure 8 ).
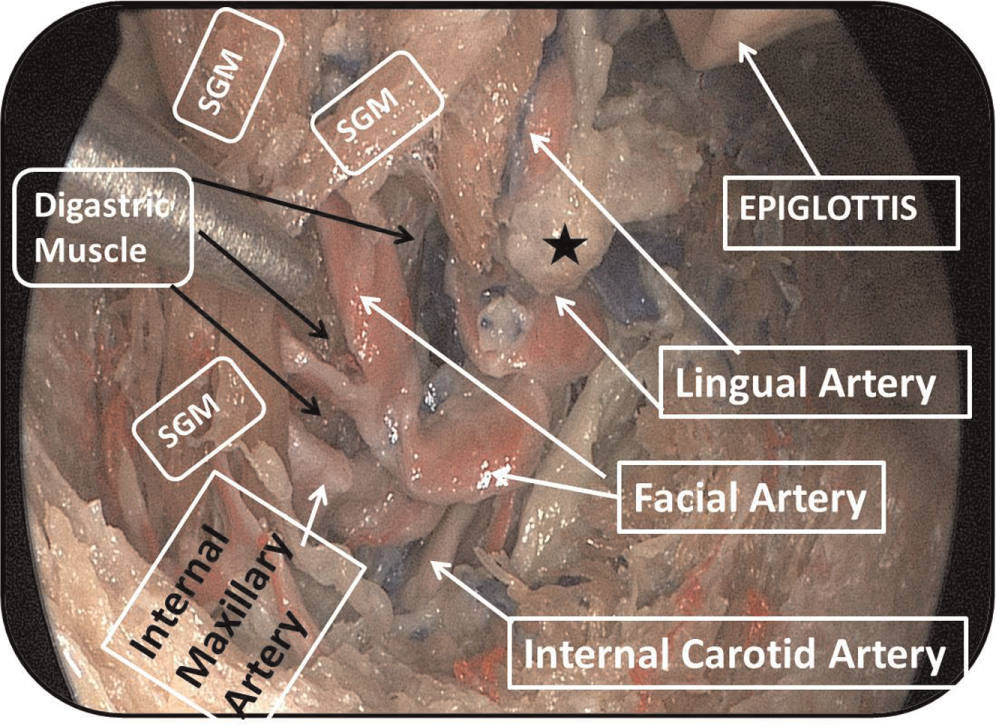
The view of digastric muscle lateral to vascular structures located within parapharyngeal space. SGM, styloglossus muscle (double insertion). Star, greater cornu of hyoid bone.
Although the trajectory of the internal carotid artery (ICA) may vary individually, it is consistently located posterolateral to the stylopharyngeus muscle, the styloglossus muscle, the stylohyoid ligament, and the branches of external carotid artery (lingual, facial, and internal maxillary arteries; ( Figure 7 ). The styloglossus muscle had 2 insertions in 1 case ( Figure 8 ).
The lingual nerve was identified lateral to the superior pharyngeal constrictor muscle where it crosses the medial pterygoid muscle anterolaterally ( Figures 2 , 3 ).
The submandibular gland was observed inferolateral to the styloglossus and palatoglossus muscles, inferior to the medial pterygoid muscle ( Figures 3 , 6 ).
Discussion
Classical head and neck anatomy is taught from the outward-to-inward perspective. Since TORS has been widely used for oropharyngeal cancers, inside-out anatomic orientation of this region has become increasingly important. Improved transoral anatomic knowledge of lateral oropharyngeal wall enhances the surgeon’s ability to resect tumors transorally with safe margins, and it reduces complications.5,9-11
A transoral view of deep structures located in the lateral pharyngeal wall and in the parapharyngeal space has not been previously described in silicone-injected cadavers. 12 In this study, muscular, vascular, and neural structures located in the lateral pharyngeal wall, parapharyngeal space, and base of tongue have been described via an endoscopic transoral approach in silicone-injected cadaveric specimens. This study provides surgeons with the relevant anatomy of this complex space and its key features for a transoral robotic surgical intervention. It highlights the surgical anatomy of these structures from a medial-to-lateral standpoint, which is paramount for the robotic surgeon.
The tonsillar fossa is bounded anteriorly by the palatoglossus and posteriorly by the palatopharyngeus muscles, which form the anterior and posterior tonsillar pillars, respectively. The tonsillar bed is mainly made up of the superior pharyngeal constrictor muscle and overlying pharyngobasilar fascia ( Figure 1 ). The stylopharyngeus muscle is located in the posterior aspect of the tonsillar bed. The stylohyoid ligament, middle pharyngeal constrictor, and styloglossus muscles also contribute to the inferior part of tonsillar bed.13,14
The tonsillar bed is the most lateral plane in radical tonsillectomies ( Figure 1 ).12,15 The anterior tonsillar pillar is the border between the retromolar trigone and the tonsillar fossa. The lack of substantial tissue between these 2 areas may allow tonsillar tumor extension to the retromolar trigone or vice versa.16,17
Fixed tonsillar tumors implies invasion of the superior pharyngeal constrictor muscle. 18 Once the tumors extend beyond the constrictor muscles, the parapharyngeal space is then involved. Further extension of tumors through the parapharyngeal space may cause invasion of vital structures such as the ICA and the skull base. 14
When the superior pharyngeal constrictor muscle is transected and reflected laterally, the contents of parapharyngeal space—including the lingual, facial, and ascending pharyngeal branches of the external carotid artery—are visualized within the parapharyngeal fat pad ( Figures 4 , 7 , 8 ).19,20
The main trunk of the glossopharyngeal nerve curves anteromedially around the lateral border of the stylopharyngeus muscle and courses in between the superior and medial pharyngeal constrictor muscles.14,21,22 At the tongue base junction, the main trunk of the glossopharyngeal nerve lies posterior to the styloglossus muscle. 20 One may see it in between the stylohyoid ligament and the styloglossus muscle before dividing into several branches and innervating the lateral pharyngeal wall and the base of tongue ( Figures 2 , 3 ). Identification and preservation of the stylohyoid ligament and the styloglossus muscle while dissecting the lateral pharyngeal wall will prevent glossopharyngeal nerve injury. Thus, postoperative swallowing and taste sensation may be preserved.12,23
One of the main concerns during TORS is injury to the lingual artery. 24 Understanding the anatomy of the lingual artery is crucial to prevent brisk bleeding during base-of-tongue resection. The lingual artery arises from the external carotid artery and courses lateral to the greater cornu of the hyoid bone and deep to the stylohyoid ligament, lateral to the middle pharyngeal constrictor muscle. The lingual artery may form a loop between the greater cornu of the hyoid and the styloglossus muscle. Then it crosses inferiorly and laterally to the styloglossus muscle ( Figure 5 ) before giving off dorsal and deep lingual branches. 14 The robotic surgeon can avoid injury of this artery by limiting the dissection medial to the stylohyoid ligament and the styloglossus muscle. In case of injury and ligation of one of the lingual arteries, the contralateral artery may provide sufficient blood supply to the tongue due to the rich anastomotic network ( Figure 6 ).25-27
Some anatomic variations may be encountered in vascular and muscular structures in the oropharynx. 28 We observed in 1 cadaver a double insertion of the styloglossus muscle at the level of the base of tongue ( Figure 8 ). Surgeons should be aware of these anatomic variations to prevent complications.
The ICA originates from the common carotid artery at the level of C3-C5 cervical vertebrate and lies 2 to 3 cm posterolateral to the posterior pharyngeal wall mucosa. 29 In 10% to 40% of the cases, the ICA has anatomic variation in its course, including kinking, coiling, and curving.30-32 However, the most important landmark for ICA during robotic surgery is the plane formed by the stylohyoid ligament, styloglossus, and stylopharyngeus muscles. The ICA lies posterolaterally to this plane in the parapharyngeal space. Also it is located posterolaterally to the branches of the external carotid artery (lingual, facial, internal maxillary arteries). Therefore, radiologic evaluation of the ICA is crucial before TORS ( Figures 7 , 8 ). 11
The lingual nerve may be injured during radical tonsillectomy at the anterior border of the medial pterygoid muscle ( Figures 2 , 3 ). 20 Resection of tonsillar tumors extending to the retromolar trigone may increase the risk of lingual nerve injury.
Conclusion
The lateral pharyngeal wall, parapharyngeal space, and base of tongue have a complex topographic anatomy. A thorough understanding of transoral anatomy is crucial for surgeons to perform TORS safely and efficiently. The stylohyoid ligament is the main anatomic landmark during TORS. It allows the surgeon to identify critical neurovascular structures safely especially when the anatomy is distorted by tumors or bleeding during TORS. Transoral cadaveric dissections are highly beneficial to become familiar with the complex anatomy of the oropharynx and may shorten the learning curve for TORS.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented as a poster at the 2014 AAO-HNSF Annual Meeting & OTO EXPO; September 21-24, 2014; Orlando, Florida.