
Abstract
Objective
To evaluate improvement of medical student knowledge of head and neck cancer (HNC) through participation in HNC screening fairs run by medical students.
Study Design
Prospective cohort study of surveys assessing medical students’ knowledge of HNC before and after volunteering at screening fairs.
Setting
Four screening fairs held at the University of Miami Miller School of Medicine during Oral, Head and Neck Cancer Awareness Week.
Subjects
Medical student screening fair volunteers.
Methods
Four HNC screening fairs were organized by medical student volunteers. All students completed a preevent survey assessing baseline knowledge and participated in an otolaryngologist-led training session about HNC and the screening examination. During the screening events, students educated guests about HNC and performed physician-guided history and physical examinations. Finally, students completed identical surveys 1 week and 3 months after the event.
Results
Thirty-four (n = 34) students completed the preevent surveys. At baseline, 59%, 44%, and 24% named tobacco, alcohol, and human papilloma virus as risk factors, compared with 84%, 81%, and 69% on 3 month follow-up, respectively. Out of 6 analyzed questions, the median total number of correctly answered questions improved from 2 on pretest to 5 at 3 months (P < .0001).
Conclusion
Volunteer participation in a HNC screening program improves medical students’ knowledge of HNC risk factors and symptoms. This innovative approach to students’ education via participation and organization of screening events is a useful method of improving their HNC knowledge.
Head and neck cancer (HNC) encompasses tumors of the oral cavity, pharynx, larynx, paranasal sinuses, nasal cavity, and salivary glands. These malignancies are relatively common, with an estimated 55,070 cases 1 diagnosed in the United States in 2014, and they are projected to cause >12,000 deaths this year. 2 Patients with HNC often present to primary care clinics with nonspecific findings, such as otalgia, epistaxis, and throat pain. These presentations may delay the final diagnosis of an underlying tumor. As with other cancers, early detection and diagnosis of HNC have been demonstrated to improve outcomes and decrease overall mortality. 3
Despite this apparent need for HNC awareness, formal otolaryngology education is inconsistent across medical education. Recent studies indicate that the majority of medical schools offer only selective or elective clerkships in the field.4-6 In addition, many medical students report a lack of confidence in executing a thorough head and neck examination.7,8 Given that head and neck complaints constitute a significant portion of primary care visits,9-12 basic exposure to the field and physical examination skills are crucial for all medical students. In total, >47% of US medical graduates pursue a career in a primary care field and will encounter these complaints. 13
Based on this variability in student exposure, there is a substantial need to improve medical student education in otolaryngology, with special attention to HNC. With funding from the 2014 Prevention and Early Detection Community Service Grant from the American Head and Neck Society, we attempted a novel approach to student education for these topics in a clinically oriented setting. We organized 4 medical student-led HNC screening fairs for the local community. During these fairs, medical students who participated had the opportunity to not only perform directed history and physical examinations under physician guidance but also directly educate screening event guests about HNC. By reviewing pre- and postfair surveys of the medical students, we aimed to determine whether this model of student involvement in a HNC screening event increases HNC knowledge among medical students pursuing a variety of specialties.
Methods
Study Design
Four screening fairs were held at the University of Miami Miller School of Medicine during Oral, Head and Neck Cancer Awareness Week (OHANCAW) in April 2015 with the primary goal of screening members of the local community for HNC. A core team of 8 medical students organized the events. To recruit student volunteers, an email was sent to all currently enrolled medical school students through the university’s official email list. Each student who committed to volunteer was asked to fill out a questionnaire that included a preeducational HNC knowledge assessment. The questionnaire was first piloted on 5 individuals not involved in the study for readability and comprehension. The assessment items tested awareness in regard to the top 3 risk factors for HNC, the increasing incidence of human papilloma virus–related tumors, and the duration of symptoms that should incite the consideration of cancer ( Figure 1 ). Questions were also asked regarding exposure and interest in otolaryngology, as well as demographic information. The student volunteers filled out the questionnaire prior to receiving training for the event.
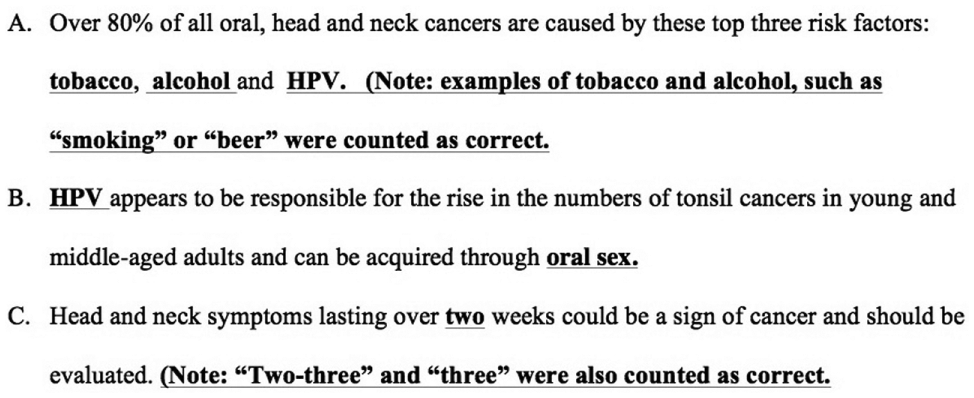
Survey questions to assess knowledge of head and neck cancers (maximum score = 6). HPV, human papilloma virus.
Formal training occurred during a 2-hour education seminar, which included a lecture by otolaryngology faculty detailing basic risk factors, signs, and symptoms of HNC and a demonstration of the HNC screening examination. In addition to learning about HNC during training, student volunteers were assigned to spend part of their shift during the screening event presenting at the education station to guests and/or shadowing otolaryngologists during guest screening examinations. The combination of an informational training session and assignment into volunteer roles that involved both guest education and clinical interaction with faculty served as our model of student involvement designed to increase awareness.
Core team members developed the presentation and accompanying visual aids that student volunteers used to educate guests. At the screening events, volunteers gave 3-minute presentations to each guest using these displays. The presentations were standardized with a presentation guide, and the points covered included those tested on the questionnaire.
To evaluate the short- and longer-term effectiveness of our model of student involvement on student HNC awareness, student volunteers were asked to fill out the postevent survey, which included the original knowledge questions, at 2 time points. The first time point was within the first 3 weeks after the event. Volunteers were then asked 3 months after the event to again fill out the postevent questionnaire. Both postsurveys were administered over email. University of Miami Institutional Review Board approval was obtained to review the questionnaires.
Main Outcome Measures
The main study end points were baseline knowledge of HNC prior to the event as compared with that immediately after the event and 3 months after the event. The null hypothesis was that there was no difference in HNC awareness before and after volunteering in the event.
Statistical Analysis
Frequencies and percentages were presented for all individual demographics. Descriptive statistics were reported for all medical students in total and then further stratified by demographic information (ie, executive board status, education level, and specialty interest). Each fill-in-the-blank response was counted as 1 point, with the highest possible score being 6 points and the lowest being zero points. Focus was placed on 3-month posttest scores because these values demonstrate both learning and retention, as opposed to only learning with immediate posttest scores. Distributional properties of the outcome were examined, and due to violation to the normality assumption, transformation was attempted. A nonparametric approach was chosen for hypothesis testing since normality assumption remained violated after transformation. Knowledge assessment pretest scores were compared with 3-month posttest scores for the entire group and within each subgroup for several binary strata variables, including executive board members, years of education, interest in primary care, and interest in otolaryngology, according to Wilcoxon signed-rank test. Proportions of correct answers for each of the 6 questions were also compared between pretest and 3-month posttest per McNemar’s test. Due to multiple-hypothesis testing, P values were adjusted according to Bonferroni’s method to control for the family-wise error rate, and statistical significance was based on a significance level of 0.05. Analyses were performed with SAS 9.3 (SAS Institute, Cary, North Carolina).
Results
Demographics
A total of 34 medical students completed the preevent survey, with 32 completing both postevent questionnaires. Of these, 8 students were part of the core team who organized the event ( Table 1 ). Twenty-three were first-year medical students, and 10 were second-, third-, and fourth-year medical students. Approximately 42% of students were interested in pursuing a primary care specialty, whereas 30% were interested in pursuing otolaryngology as a specialty. Medical students were involved with teaching and/or assisting screenings with each of the 248 guests screened over the course of the event.
Demographic Data of Medical Student Participants.
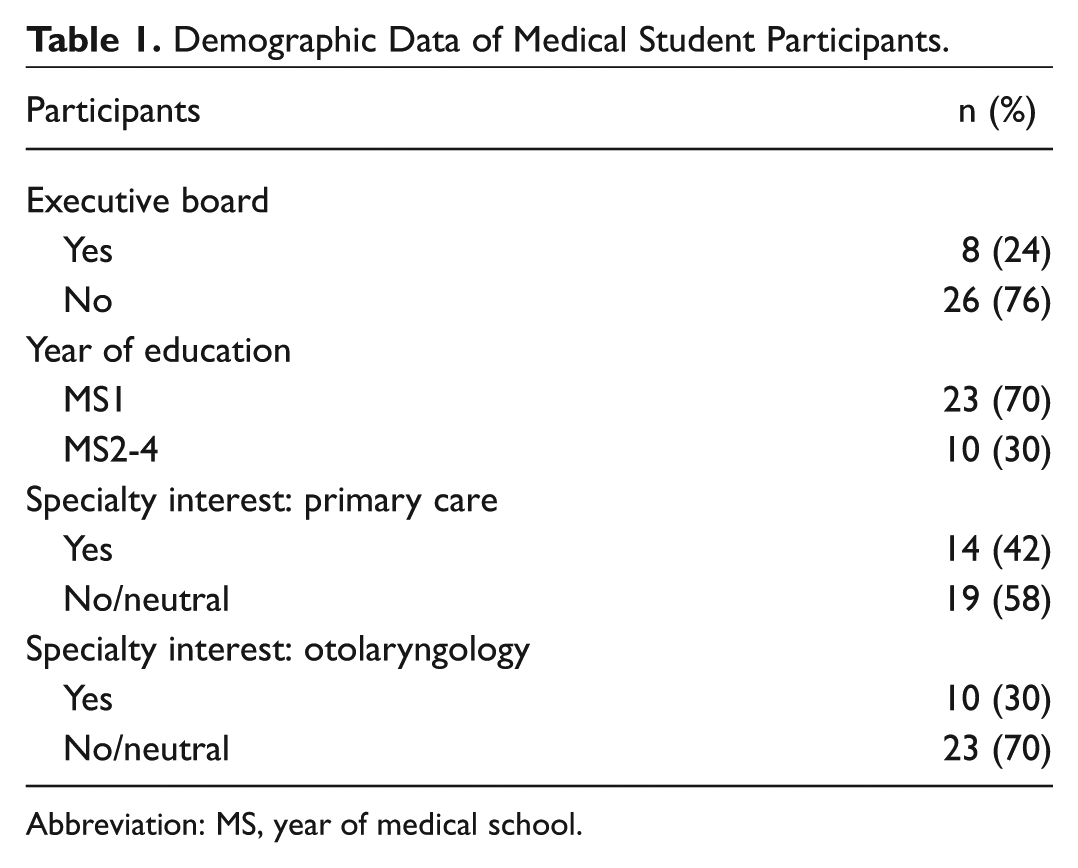
Abbreviation: MS, year of medical school.
Forty-seven percent of students reported feeling “not very confident” or less in examining the oral cavity for cancer prior to the event, compared with 9% after the event. Confidence in the ability to feel and find lymph nodes in the neck was “not very confident” or less for 18% prior to the event, compared with 3% afterward. Sixty-five percent had never worked with an otolaryngologist in a clinical setting, and 79% reported feeling that the event made them feel more comfortable seeking mentorship from otolaryngology faculty and residents. When asked why they decided to participate, >90% of students reported that they wanted to increase their knowledge about HNC and/or learn how to perform the screening examination; other reasons cited were to gain exposure to otolaryngology and to participate in community outreach.
Questionnaire Analysis
The questionnaire included 3 questions and a total of 6 answers. The maximum possible score was 6 points, with each answer scored independently. As a group, medical students demonstrated statistically significant learning for all questions but 1 that were analyzed ( Table 2 ). The largest improvement from pretest to 3-month posttest was seen for question C, regarding knowledge of concerning symptom duration (21% to 78%, P = .0001), while the smallest improvement was seen for question A answer “Alcohol” (41% to 81%, P = .0275). The change for question A answer “Tobacco” (53% to 84%, P = .0586) was not statistically significant. As a group, there was improvement of median total score from 2 before the event to 5 three months after the event (P < .0001; Table 3 ). Improvements were also seen for particular demographic cohorts, such as those individuals not on the core team who organized the event (P < .0001), first-year medical students (P < .0001), and those students not interested in pursuing otolaryngology as a specialty (P < .0001).
Pre- and Postevent Score Comparison.
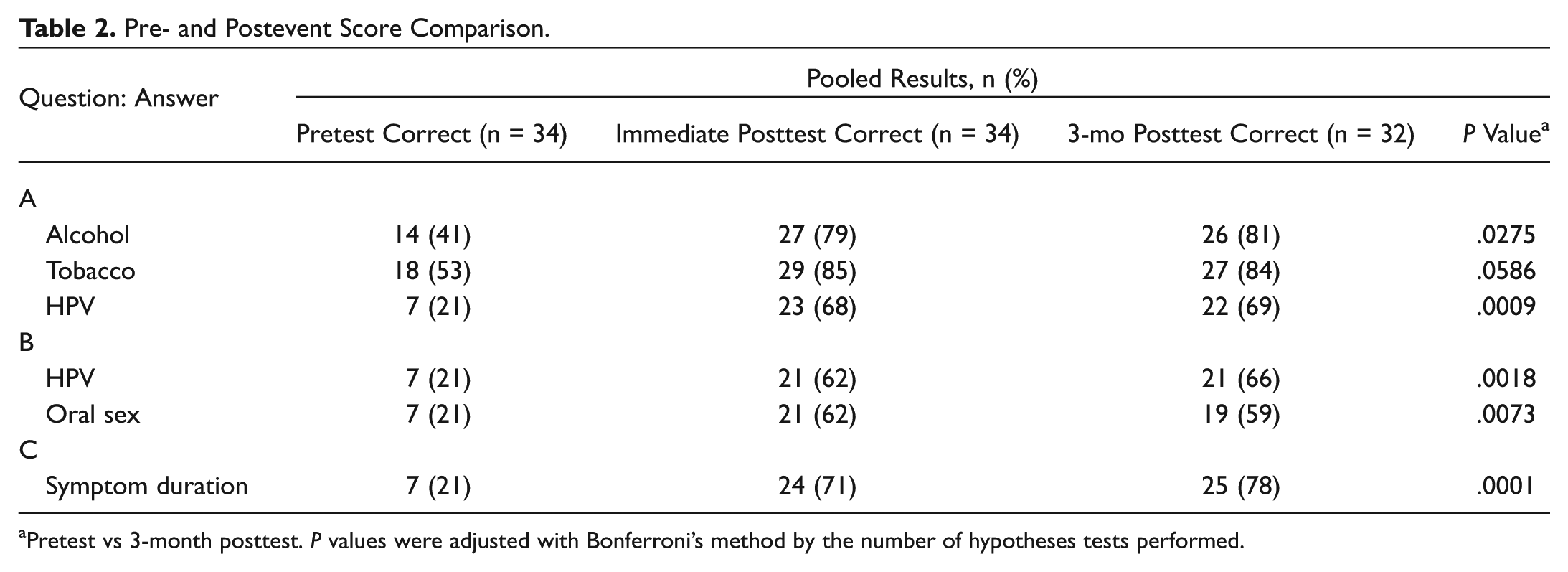
Pretest vs 3-month posttest. P values were adjusted with Bonferroni’s method by the number of hypotheses tests performed.
Pre- and Postevent Score Comparison within Subgroups.
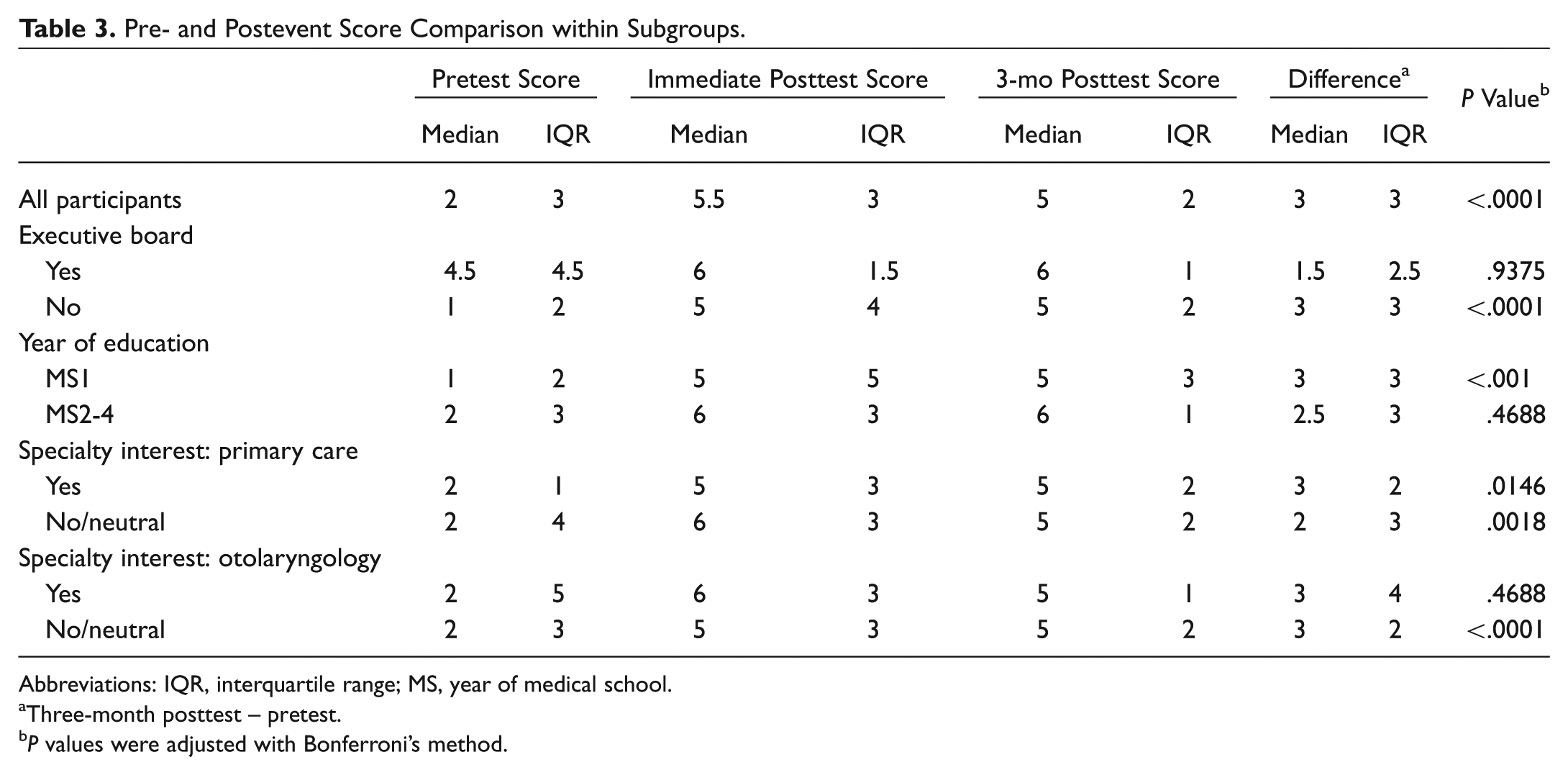
Abbreviations: IQR, interquartile range; MS, year of medical school.
Three-month posttest – pretest.
P values were adjusted with Bonferroni’s method.
Discussion
HNC is a significant cause of mortality in the United States and can present with nonspecific findings. Despite this, multiple studies have demonstrated that medical students have insufficient knowledge and skills to appropriately screen for these malignancies. Mohyuddin et al 14 conducted a broad assessment of HNC knowledge among first- and fourth-year US medical students. Their survey included questions regarding risk factors, signs, symptoms, screening recommendations, and physical examination techniques. The results showed poor baseline knowledge in first-year medical students, with only 18% to 27% and 67% correctly identifying heavy alcohol consumption and tobacco, respectively, as major risk factors for HNC. Furthermore, 88% of first-year students could not correctly identify all 7 of the signs, symptoms, and risk factors listed in the survey. Among fourth-year students, this value was found to be 30%.14,15
Our preevent surveys appear to corroborate this baseline knowledge deficit. Only 44% and 59% of our students identified alcohol and tobacco, respectively, as major HNC risk factors. Additionally, less than a quarter of students correctly identified human papilloma virus as a potential risk factor ( Table 2 ). Overall, these results demonstrate the necessity of targeted HNC education and may contribute to the fact that 93% of medical students report feeling that they have insufficient knowledge regarding early detection of oral cancer. 15
These deficits may be partially explained by the wide variability in otolaryngology education across medical schools. Campisi et al noted that 62.5% of Canadian medical schools do not include a mandatory otolaryngology rotation in their curricula. 16 In the United States, this figure is similar at 66.4%. 9 Although greater than half of these schools offer an elective rotation, only 19.5% of students opted to participate in one. Even for schools that do require an otolaryngology rotation, these experiences are limited and average <5 days.16,17 Because these rotations likely cover a variety of otolaryngology subspecialties, an even smaller portion of time may be specifically devoted to the topic of HNC. At our institution, otolaryngology preclinical teaching is relatively brief and incorporated into broader modules focusing on the respiratory system and oncology, and clinical otolaryngology experience is offered only as an elective.
Even when students do learn about otolaryngology, the quality of teaching is inconsistent. 18 A British survey of students who completed a weeklong rotation showed that only 66% and 63% were taught how to properly conduct ear and neck examinations, respectively. Less than a third of those students reported being taught a nasal, oral cavity, or throat examination. 19 This inconsistency in physical examination training likely contributes to the fact that only 18.4% of fourth-year medical students felt adequately trained to do a focused examination for HNC. 12 In the long term, this may lead to students being less likely to perform a thorough screening examination and diagnose a potential HNC.
These HNC knowledge deficits and lack of exposure to the field often persist for physicians after medical school, especially for those in primary care fields. The percentage of primary care chief complaints related to otolaryngology has been widely reported at between 10% and 20%.9-11,20 Despite this high incidence, a survey conducted by Hu et al demonstrated that many primary care physicians were routinely unable to identify common presentations and indications for otolaryngology procedures. 20 Furthermore, Clamp et al 21 reported that 75% of general practitioners indicate that they would welcome additional training in the field.
Although most patients with head and neck symptoms are unlikely to be diagnosed with a malignancy, primary care physicians must be able to accurately screen and rule out the possibility of HNC for patients with a suspicious presentation or risk factors. 22 This further demonstrates the importance of improving otolaryngology education of all medical students, including those planning to go into other fields. In our study, >41% of medical student volunteers reported being most interested in a career in primary care ( Table 1 ). Thus, the screening fair education model may appeal to a broader range of medical students who might not otherwise be exposed to otolaryngology or HNC education.
Overall, our study examined results of preevent, immediate postevent, and 3-month postevent questionnaires with 6 questions about common HNC risk factors and symptom duration. Based on these surveys, our innovative model of student participation in a HNC screening fair showed promising improvements in medical student knowledge. For all students as a group, the median number of HNC survey questions that were correctly answered increased from 2 in the preevent survey to 5.5 in the immediate postevent survey. Our 3-month survey median of 5 demonstrates that medical students effectively retained this knowledge. Of note, despite different baseline levels of knowledge, these 3-month gains were present for both underclass students (1 to 5) and upperclass students (2 to 6). Importantly, students interested in primary care fields obtained similar levels of final knowledge (5) when compared with the students specifically favoring a career in otolaryngology (5; Table 3 ).
These improvements were likely due to a combination of several aspects of our volunteer experience. Reports by Kuan et al and Cannick et al have shown that faculty-led didactic and physical examination demonstrations can lead to lasting improvement in medical student comfort and skill level with the head and neck examination.7,23 Thus, we believe that our required 2-hour training session preceding the event was a crucial experience for our medical student volunteers and may lead to increased levels of confidence in performing the head and neck physical examination.
Additionally, our system of having medical students repeatedly educate groups of screening event guests about HNC risk factors and symptoms likely contributed to their improvement and retention of this information. Finally, our 4 fairs were organized to allow students to work with faculty and residents in a one-on-one fashion during each screening encounter. As Kelly et al 5 noted that otolaryngology faculty report limited time and the ineffectiveness of a large student:teacher ratio as their greatest barriers to teaching medical students, this educational structure may provide a unique opportunity for personalized teaching in a clinically oriented setting. Given these factors, we believe that our method of creating a medical student–led volunteer effort to host HNC screening fairs provided a novel and effective opportunity for student education about both HNC and general otolaryngology physical examination skills.
In addition, because previous studies by Gourin et al 24 and Shuman et al25,26 found that free screening events do not typically attract a high-risk population or diagnose many malignancies, HNC screenings should be tailored toward a population with risk factors or low socioeconomic status to be most effective for early detection of tumors. Recruitment of these populations was a focus of our event, and students were involved in the development and implementation of recruitment strategies targeting this group. Our experience incorporating medical student and participant education into the screening offers an additional avenue to create an impact from these events. We believe that by including educational goals and encouraging medical students to lead the effort of organizing screening events, the overall number and impact of OHANCAW efforts can be improved.
One limitation of our study is the relative overrepresentation of first-year medical students in our sample, which may contribute to the low baseline knowledge values observed. Our study is vulnerable to selection bias since our voluntary participation may have attracted students with baseline knowledge levels that differ from those of their peers. Also, because our study compared preparticipation surveys with postparticipation surveys, we are not able to separately assess the educational values of the otolaryngologist-led training session and direct participation in each screening fair activity, such as examining or educating event guests. Due to the presence of different volunteers at the 4 sites, we could not standardize each volunteer’s experience in regard to relative amount of time spent conducting history and physical examinations as compared with time spent on educating guests about HNC. It is possible that the variability in these assigned responsibilities over the course of 4 fairs may have influenced our results. An additional limitation was that our questionnaire was a nonstandardized instrument. Because our study had only 34 student volunteers, additional studies with larger groups of students may be required to elucidate the full impact of screening event participation on medical student knowledge. Future investigation with a comparison group of matched students who did not participate in the screening would allow for further evidence to support that student increases in knowledge after the event are attributable to their participation. As a next step to characterize the impact of introducing this program as a standard part of the curriculum, a future study would be to incorporate the tutorial into the curriculum and compare the knowledge between those who then participate in screening clinics and those who do not. Given the positive feedback that we received from participating students, we do believe that OHANCAW has the potential to be a welcomed and informative experience for medical students at other institutions, and we hope that our study stimulates further work in this area.
Conclusion
Baseline knowledge about HNC continues to be low among medical students. Since many HNC patients present first to healthcare providers who do not specialize in otolaryngology there is a need for students pursuing all specialties to receive additional education about these topics. This novel method of education through medical student participation in HNC screening fairs during OHANCAW successfully attracted and increased HNC knowledge among students who plan on entering a variety of specialties. This model of medical student education and volunteering can be effectively and quickly implemented at other institutions that currently participate in OHANCAW.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank Michelle Caunca, Nikitha Gangasani, and Ryan Vandenberg for their help as executive board members in organizing the event. We also thank Nosayaba Osazuwa-Peters at Saint Louis University for sharing survey questions for use as part of the questionnaire.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.