
Abstract
Objective
Vocal fold scarring, a condition defined by increased collagen content, is challenging to treat without a method of noninvasively assessing vocal fold structure in vivo. The goal of this study was to observe the effects of vocal fold collagen content on optical coherence tomography imaging to develop a quantifiable marker of disease.
Study Design
Excised specimen study.
Setting
Massachusetts Eye and Ear Infirmary.
Subjects and Methods
Porcine vocal folds were injected with collagenase to remove collagen from the lamina propria. Optical coherence tomography imaging was performed preinjection and at 0, 45, 90, and 180 minutes postinjection. Mean pixel intensity (or image brightness) was extracted from images of collagenase- and control-treated hemilarynges. Texture analysis of the lamina propria at each injection site was performed to extract image contrast. Two-factor repeated measure analysis of variance and t tests were used to determine statistical significance. Picrosirius red staining was performed to confirm collagenase activity.
Results
Mean pixel intensity was higher at injection sites of collagenase-treated vocal folds than control vocal folds (P < .0001). Fold change in image contrast was significantly increased in collagenase-treated vocal folds than control vocal folds (P = .002). Picrosirius red staining in control specimens revealed collagen fibrils most prominent in the subepithelium and above the thyroarytenoid muscle. Specimens treated with collagenase exhibited a loss of these structures.
Conclusion
Collagen removal from vocal fold tissue increases image brightness of underlying structures. This inverse relationship may be useful in treating vocal fold scarring in patients.
Optical coherence tomography (OCT) is an imaging technology that uses low-coherence interferometry to create 2-dimensional images.1,2 The attractiveness of this technology lies in its ability to noninvasively image human tissue and obtain an image resolution on the order of 10 µm.3-5 OCT may be clinically relevant as it provide clues into understanding the composition of tissue. As incident light passes through a specimen, the light used to construct an image is lost secondary to optical properties of the tissue, such as absorption, scattering, and reflectance.6,7 Thus, image brightness decreases as a function of depth, and the rate of decay in image brightness is dependent on the content of the tissue of interest.
In the field of laryngology, OCT has potential for aiding the diagnosis and treatment of voice disorders, based on its ability to image tissue without biopsy. OCT has been shown to distinguish benign vocal fold pathologies intraoperatively, such as nodules, cysts, and papilloma.8-10 Additionally, investigators have captured images of laryngeal cancer, characterizing disrupted subepithelial structures.9,11 One study suggested that OCT may be sensitive enough to distinguish changes in vocal fold microstructure that occur during normal childhood development. 12 Others have demonstrated the potential utility in using OCT to more precisely treat vocal fold pathologies with CO2 laser ablation and vocal fold injections, 2 commonly used techniques that rely heavily on the skill of the attending surgeon.13,14
The structure of the normal human vocal fold has been studied via histologic staining as well as confocal and electron microscopy techniques. Through these studies, it has become widely accepted that the human vocal fold consists of an epithelium, a 3-layered lamina propria (superficial, intermediate, and deep), and the thyroarytenoid muscle.15-18
Histologic evidence suggests that the 3-layered lamina propria emerges from a single homogeneous layer over the course of a child’s development.19,20 Findings from OCT have also supported this idea, demonstrating different rates of optical signal decay between younger and older vocal folds. 12 Each layer within the lamina propria is defined by a concentration of collagen, as it is more predominant in the superficial and deep layers relative to the intermediate layer.21-26 Caution should be exercised, however, when interpreting the histology of vocal fold tissue, as the layers within the lamina propria can be difficult to distinguish. 27
Collagen is the most common extracellular matrix protein in the human lamina propria, followed by elastin and hyaluronic acid. 28 In disease states such as vocal fold scarring, collagen content is increased, thereby disrupting the biomechanical properties that allow for phonation. 29 In rat, rabbit, canine, and porcine models of vocal fold scarring, collagen concentration in mechanically injured vocal folds is increased.30-34 Similar findings have been observed in human vocal fold specimens previously undergoing cordectomies for early-stage laryngeal cancer. 35 To our knowledge, the effects of increased or decreased collagen content on OCT vocal fold imaging are unknown. In other tissue settings, such as skin, scarring from surgical incisions, burns, and scleroderma limits the depth to which OCT imaging is effective.36,37 As collagen is abnormally increased in these settings, 38 we sought to determine if a similar relationship between collagen content and underlying image brightness could be demonstrated in OCT imaging of vocal fold tissue.
Materials and Methods
Twelve porcine larynges were obtained from 6- to 8-month-old Yorkshire pigs via a local supplier of animal research specimens (Research 87 Inc, Boylston, Massachusetts) and, as such, did not require approval by the Massachusetts Eye and Ear Infirmary Institutional Review Board. Specimens were received fresh and immediately processed. Larynges were split at the midline in the sagittal plane, and each specimen was marked with India ink approximately 0.5 cm anterior and 0.5 cm posterior to the midpoint of the true vocal fold. A commercially available MEMS-VCSEL Swept Source OCT system (central wavelength λ = 1305 nm, model OCS1310V1; Thorlabs, Newton, New Jersey), as previously described,39,40 was used for all OCT imaging. The power emitted from the OCT probe was approximately 19.8 mW. The field of view was 20 × 5.7 × 14.9 mm (1552 × 449 × 1158 pixels). Acquisition time was approximately 30 seconds for each scan.
Four hemilarynges were immediately scanned after India ink marking and subsequently fixed in formalin for 24 hours, embedded in paraffin wax, and sliced into 5-µm slices along the axial plane such that both ink markings were captured within each slice. The specimens underwent picrosirius red (PSR) staining, as previously described, 41 and were photographed at 5× magnification with a Zeiss-AxioPhot Phase/Fluorescence microscope (Zeiss, Thornwood, New York) and Optronics MicroFire CCD camera (Optronics, Goleta, California) under bright-field and circularized polarized light to appreciate collagen content. Images were reassembled with Adobe Photoshop.
To reduce native collagen content, 10 hemilarynges were injected with 5 µL of 2 mg/mL collagenase (C0130; Sigma, St Louis, Missouri) and 5mmol CaCl2 (C1016; Sigma) in phosphate-buffered saline (17-516F; Lonza, Basel, Switzerland) directly into the lamina propria with a 10-µL syringe and 31-gauge needle (7659-01, 7803-03; Hamilton, Reno, Nevada). As a control, 10 hemilarynges were injected with 5 µL of a 5mmol solution of CaCl2 in phosphate-buffered saline. All injections were performed between the India ink markings approximately at the midpoint of the membranous vocal fold. Each specimen was imaged before and immediately after injection to confirm injection into the lamina propria and not between the lamina propria and thyroarytenoid muscle. As injections were performed by hand, it was not possible to ensure consistent injection at a certain depth in the lamina propria. One hemilarynx from the collagenase-treated group and 3 from the control-treated group were discarded, as the injections were unintentionally performed between the lamina propria and thyroarytenoid muscle. Specimens were incubated at 37.5oC to enhance collagenase activity and wrapped in moist gauze to prevent desiccation. OCT imaging was repeated after 45, 90, and 180 minutes. After the final OCT scans, specimens were processed for PSR staining and imaged as described above.
To determine the effects of collagenase injection on the depth to which OCT can image, ImageJ analysis software (National Institutes of Health, Bethesda, Maryland; http://imagej.nih.gov/ij/) was used to extract mean pixel intensity (MPI) for statistical comparisons. For each specimen, an injection site (region of interest at the site of injection) and a noninjection site (region of interest not at the site of injection) were identified on the postinjection OCT images of hemilarynges injected with collagenase or control solution. Identifying noninjection sites for each hemilarynx was necessary to ensure that changes in image brightness were specific to regions of the hemilarynx injected with collagenase and not observed throughout the vocal fold secondary to variance in tissue desiccation between specimens. The locations of each injection site and noninjection site relative to the ink markings were noted in pixels. Within each 3-dimensional scan, a series of 30 consecutive regions of interest, 386 µm × 14.9 mm, was selected for preinjection and 45-, 90-, and 180-minute scans. The ink markings were used as reference points to ensure that the same region of interest was obtained for a single specimen across time points. Pixel intensity was extracted from each region of interest with ImageJ and graphed as a function of depth to create an A-line. Because the collagenase and control injections could not be performed at the same depth across hemilarynges, a reliable reference point consistent across specimens was needed to assess image brightness at a particular depth below the lamina propria. For this purpose, the lamina propria–thyroarytenoid muscle transition point was noted on the image series, and the pixel intensity from the subsequent 644 µm (50 pixels) below was averaged for each region of interest to calculate the MPI. Image contrast, or the relationship between pixel intensity of adjacent pixels, was also extracted with ImageJ. A 100- × 100-pixel region was selected in the midpoint of the lamina propria for 10 consecutive slices in the preinjection and 180-minute scans. The contrasts for the 10 slices were averaged to calculate an overall image contrast for a given sample. Ink dots were used to ensure that the same region was selected between time points.
Statistical Analysis
The MPIs derived from injection sites in collagenase-treated hemilarynges were compared with those derived from injection sites of control-treated hemilarynges. Additionally, the MPIs derived from the injection sites were compared with those derived from noninjection sites in both groups of hemilarynges to ensure that changes in MPI were specific to regions injected with collagenase. A 2-factor repeated measure analysis of variance was performed in each comparison to see (1) mean change in MPI over 180 minutes, (2) difference between the compared groups, and (3) interaction between time and group effect. A reduced P value of 0.017 was used to determine statistical significance to account for the multiple comparisons performed in this study. To compare the fold change in image contrast between control and collagenase injections, a t test for 2 samples with unequal variances was performed to assess significance.
Results
PSR staining of porcine vocal fold cut in the axial plane reveals long-coiled collagen filaments that orient in the anterior-posterior direction ( Figure 1 ). Viewing the slide in bright field ( Figure 1 , top panel) allows for appreciation of the epithelium (yellow), lamina propria (red), thyroarytenoid muscle (yellow), and ink markings (black). Viewing under polarized light ( Figure 1 , middle panel) highlights the collagen structure (gold), demonstrating densely packed collagen anteriorly near the anterior commissure and posteriorly near the arytenoid cartilage. The filamentous collagen structure is most apparent at the midmembranous vocal fold, where a dense layer of collagen exists just beneath the epithelium, becomes more sparse, and becomes dense again just above the thyroarytenoid muscle. The corresponding OCT image is presented with epithelium, lamina propria, thyroarytenoid muscle, and ink dots ( Figure 1 , bottom panel).
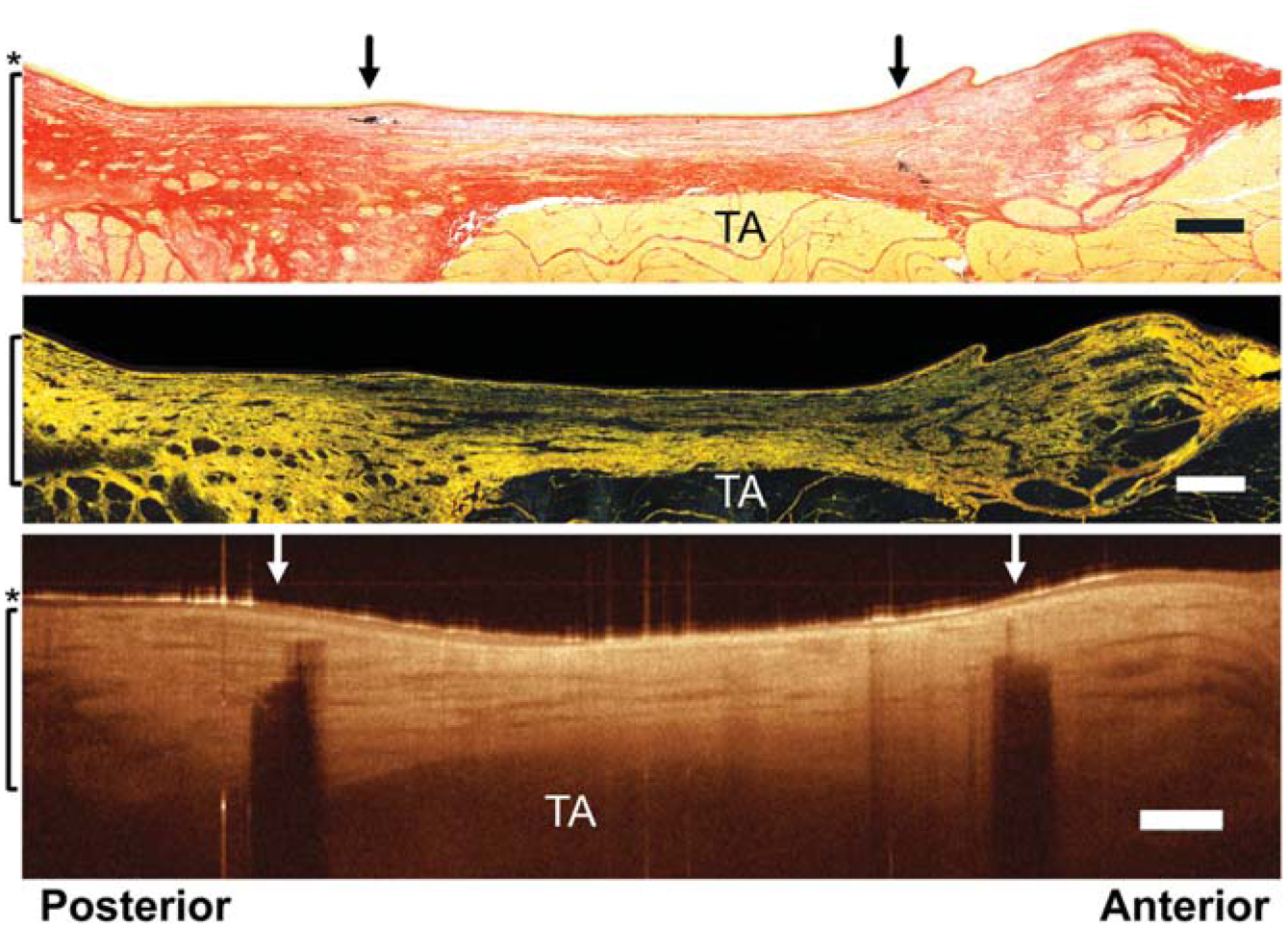
Picrosirius red histology and optical coherence tomography of porcine tissue. Bright field (top), polarized light (middle), optical coherence tomography (bottom). Arrows, ink markings; brackets, lamina propria; asterisk, epithelium. TA, thyroarytenoid muscle. Scale bars = 500 µm.
Collagenase and control solution were injected into the lamina propria ( Figure 2A ). Serial OCT imaging of specimens injected with collagenase revealed a brighter underlying thyroarytenoid muscle at the injection site relative to control specimens. When the injection sites of vocal folds treated with collagenase (solid black line) were compared with those treated with control solution (solid gray line), there was a statistically significant increase in MPI with respect to site effect, time effect, and interaction effect (P < .0001; Figure 2 ). The MPI of collagenase-treated injection sites significantly differed from those of control-treated injection sites at 45 minutes (P = .0028), 90 minutes (P < .0001), and 180 minutes (P < .0001). In collagenase-treated hemilarynges, image analysis revealed a statistically significant increase in MPI at injection sites (solid black line) as compared with the noninjection sites (dashed black line) with respect to site effect, time effect, and interaction effect (P < .0001; Figure 2B ). MPI at injection sites was greater than that at noninjection sites at 45 minutes (P < .0001), 90 minutes (P < .0001), and 180 minutes (P < .0001). This was not observed in the serial OCT images of specimens injected with the control solution ( Figure 2 ). There was no significant change over time in MPI (P = .3852), no significant site effect on MPI (P = .7644), and no significant interaction between time and region-of-interest site (P = .0543). Closer examination of the lamina propria at the injection site in collagenase-treated specimens revealed the emergence of linear structures running anterior to posterior through the vocal fold after 180 minutes ( Figure 3A ). Texture analysis revealed a significant increase in relative change in contrast in collagenase-treated specimens versus control-treated specimens (P = .002; Figure 3B ).
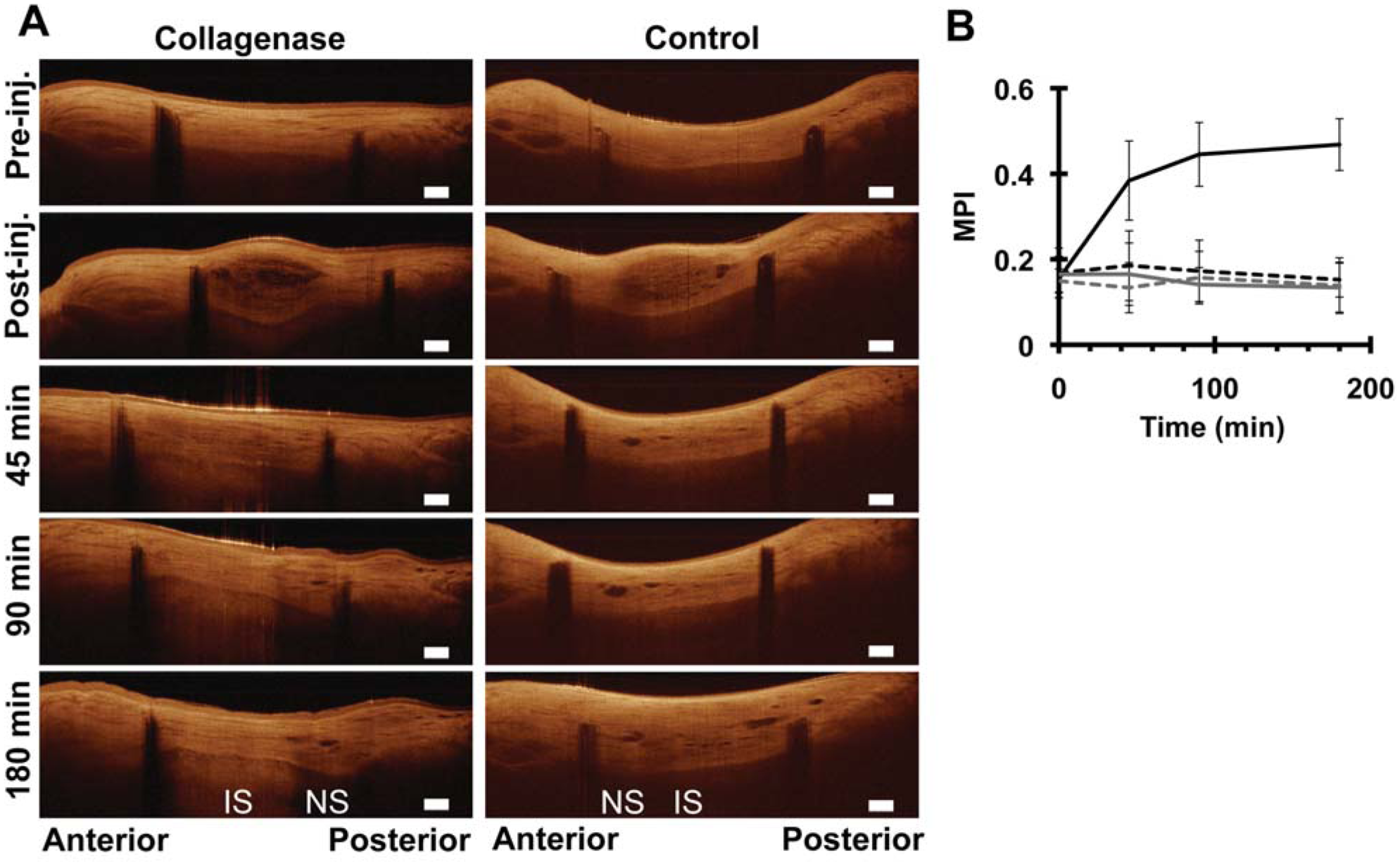
(A) Optical coherence tomography of vocal folds injected with collagenase or control solution. IS, injection site; NS, noninjection site; post-inj, postinjection; pre-inj, preinjection. Scale bars = 500 µm. (B) Mean pixel intensity of collagenase-IS (solid black), collagenase-NS (dashed black), control-IS (solid gray), and control-NS (dashed gray).
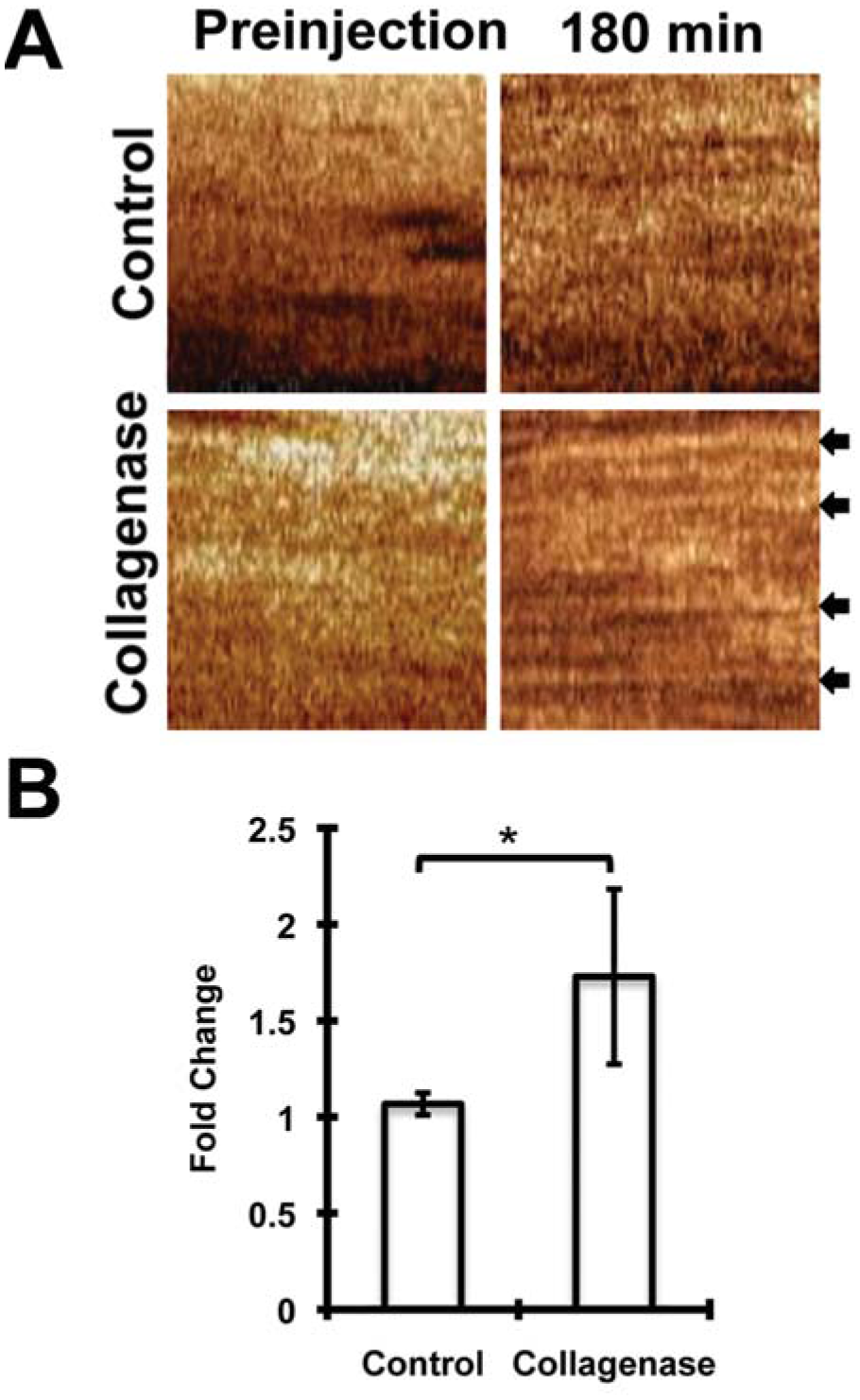
(A) Representative 100- × 100-pixel regions of interest from lamina propria used to perform texture analysis. Arrows highlight fiber-like structures. (B) Fold change in contrast was greater in collagenase-treated specimens. *P < .05.
After the 180-minute incubation period, vocal folds injected with collagenase, not control solution, exhibited translucency of the structures overlying the thyroarytenoid muscle at the injection site ( Figure 4A ). PSR staining of vocal folds injected with collagenase demonstrated less prominent filamentous collagen structures throughout the lamina propria at the injection site ( Figure 4B ). Vocal folds injected with control solution remained relatively unchanged ( Figure 4C ), maintaining dense filamentous collagen structures immediately under the epithelium as well as overlying the thyroarytenoid muscle.
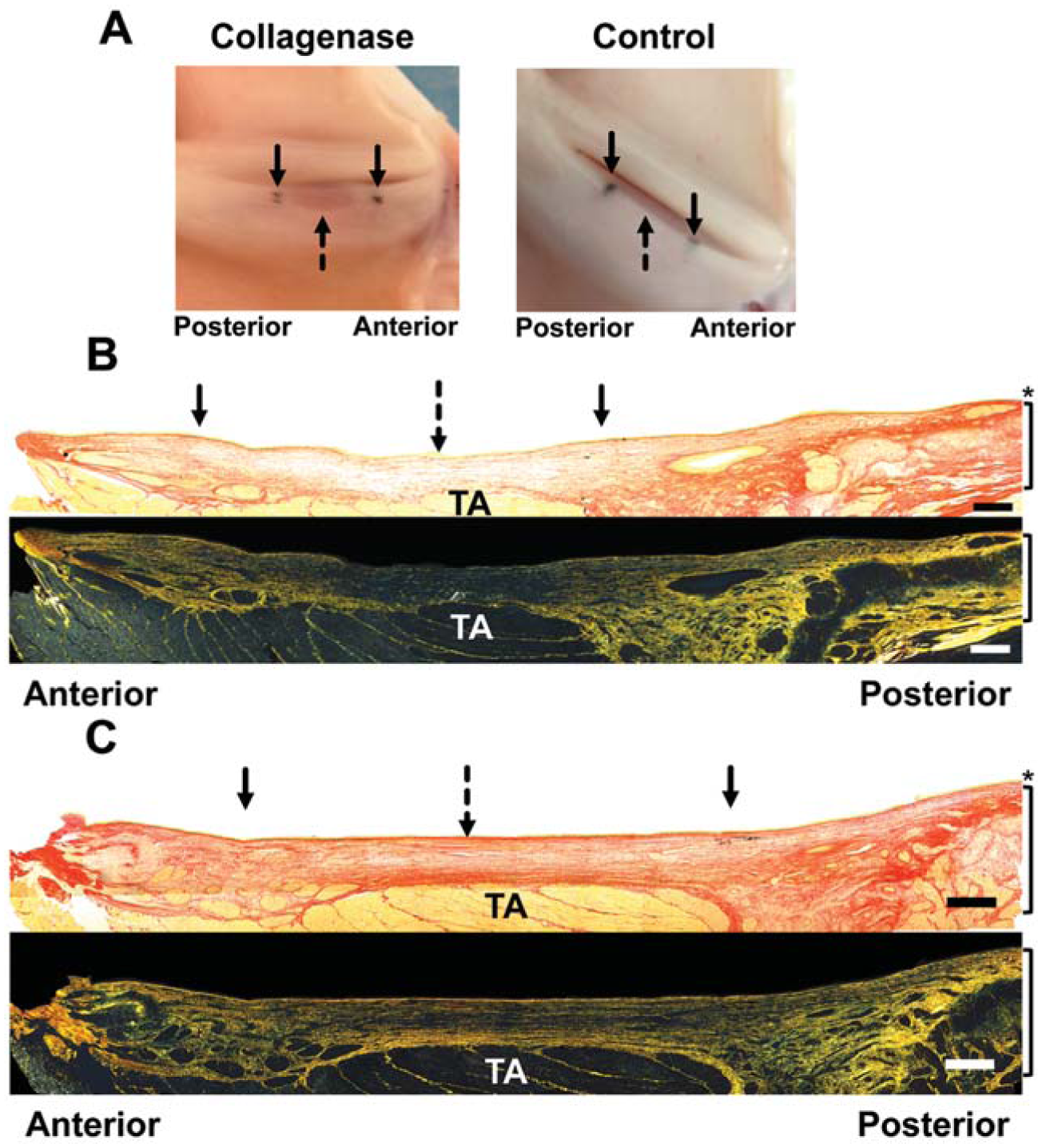
(A) Gross vocal fold tissue. Histology of (B) collagenase- or (C) control-treated site. Solid arrows, ink; dashed arrows, injection sites; brackets, lamina propria; asterisk, epithelium. TA, thyroarytenoid muscle. Scale bars = 500 µm.
Discussion
In this study, we demonstrate that collagen content within vocal fold tissue limits underlying image brightness. By removing collagen bundles from the lamina propria, the average brightness of the underlying thyroarytenoid muscle increases. This observation is likely a result of more laser power penetrating deeper into the tissue due to less overlying collagen material present to absorb and scatter the optical signal. These findings in vocal fold tissue coincide with observations made in skin where more collagen limits OCT image brightness.36,37 These findings further support an inverse relationship between collagen content and the depth by which OCT imaging is effective and suggest that underlying image brightness may be decreased in scarred vocal folds relative to those with normal collagen content. Thus, image brightness of vocal fold imaging may become clinically relevant in diagnosing and treating vocal fold disorders defined by altered collagen content such as vocal fold scarring.
Despite the positive findings presented here, there are limitations in the conclusions that can be made. First, the collagenase used in this experiment is a type I collagenase derived from Clostridium histolyticum. It aggressively removes Gly-X-Y amino acid triplets from the C-terminus of each collagen filament that composes the triple helical collagen structure.42,43 As this is a calcium-dependent enzyme, it is likely that complete collagen degradation was not achieved in every specimen. Therefore, drawing conclusions on how vocal folds without collagen appear on OCT is difficult on the basis of these results alone. Additionally, it is unclear how PSR staining may function in partially digested collagen. For these reasons, the identity of the fiber-like structures that emerge in collagenase-treated lamina propria is unclear. These could represent residual collagen fibrils that were not completely digested, or they could represent other extracellular matrix components, such as elastin. Notably, this study used MPI as an indirect measure of overlying collagen content, and using swept-source OCT alone cannot distinguish collagen from other extracellular matrix proteins. Future studies might incorporate polarization-sensitive OCT, which can distinguish collagen content by detecting tissue birefringence inherent to collagen molecules.9,11 Additionally, alternative imaging technologies, such as nonlinear laser scanning microscopy, have more directly described collagen content within the lamina propria.44,45 Another limitation is the possible inconsistency of injection depth. As these injections were performed by hand, it is unclear if the majority of the injection was directed into the superficial, intermediate, or deep layer of the lamina propria. The histology presented in Figure 4B and C shows that collagen content was removed throughout the lamina propria, suggesting that smaller amounts of collagenase may need to be used to observe the effects of selectively removing collagen from the superficial or deep layers. However, OCT has not been able to identify the layers of the lamina propria to date, so targeted injection into specific regions of the lamina propria is not currently possible. 12 Regardless, these findings do support the basic principle that collagen content is inversely related to underlying image brightness. Next, collagen is not the only extracellular matrix molecule to be increased or decreased in scarred vocal folds.34,46 Hyaluronic acid is decreased in a number of animal models of vocal fold scarring, and elastin is another prominent extracellular matrix protein found in vocal fold tissue. Additional studies evaluating the relationship between the content of these molecules and OCT imaging will need to be explored.
The findings of this study point toward numerous directions for future research. Now that collagen content has been shown to limit depth of OCT imaging, other extracellular matrix molecules commonly found in vocal fold lamina propria, such as hyaluronic acid and elastin, should be tested. 28 With enzymatic degradation, more elaborate studies can be performed to observe if decreases in collagen and hyaluronic acid or elastin have synergistic effects on image depth. Next, given the numerous animal models of vocal fold scarring previously described and the advances in OCT technology that allow for intraoperative imaging, the conclusions drawn from this ex vivo study should be put to the test in vivo.8-12,34 If normal vocal folds exhibit brighter OCT imaging than that of scarred vocal folds in animal models, human subjects with vocal fold scarring should be imaged. Next, numerous therapeutics have been tested to treat vocal fold scarring in animal models and in humans. Prior attempts to treat vocal fold scarring include the use of steroids, mitomycin-C, and hyaluronic acid, while newer agents—such as platelet-derived growth factor, granulocyte-macrophage colony-stimulating factor, and hepatocyte growth factor—have displayed promising results in animal models.43,47,48 OCT imaging may allow for understanding changes in vocal fold structure in response to these therapies, something not previously achievable in humans without tissue biopsies. OCT could therefore help to understand changes in vocal fold structure in response to experimental therapies to aid in interpreting voice outcomes. Last, the use of C histolyticum–derived collagenase to remove collagen from vocal fold tissue in this study highlights its potential therapeutic use in decreasing collagen content in scarred vocal folds. Vocal fold scarring in animal models and humans results in increased collagen content, so attempts to eliminate collagen would be a logical step in restoring normal lamina propria structure.30-35 In other disease processes defined by abnormal scar tissue, C histolyticum–derived collagenase is already in clinical use. A prospective, randomized, double-blind, placebo-controlled clinical trial proved its effectiveness in treating Dupuytren’s contractures, and ongoing studies are applying its use to Peyronie’s disease with promising results.49,50 Thus, future studies might focus on understanding the enzyme kinetics of collagenase in vocal fold tissue and exploring the use of known collagenase inhibitors to “turn off” the enzyme when the desired viscoelastic properties have been restored.
In summary, OCT is an exciting technology that, with further investigation, may become clinically useful in the field of laryngology. We show that OCT is capable of distinguishing vocal fold tissue with variable collagen content. These results, along with the results of other studies, support the notion that overlying collagen content is indirectly related to the OCT image brightness. Therefore, OCT may become a useful tool in the diagnosis and management of disorders resulting in abnormal collagen content such as vocal fold scarring.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2015 AAO-HNSF Annual Meeting & OTO EXPO; September 27-30, 2015; Dallas, Texas.