
Abstract
Objective
To describe management and oncologic outcomes for patients who develop locoregional recurrence (LRR) or distant metastasis (DM) following transoral robotic surgery for human papilloma virus (HPV)–positive oropharyngeal squamous cell carcinoma (OPSCC).
Study Design
Case series with chart review.
Setting
Tertiary care referral center.
Subjects and Methods
A total of 286 patients with HPV-positive OPSCC who underwent transoral robotic surgery–based treatment from May 2007 to May 2015.
Results
Of 286 patients (12.2%), 35 met inclusion criteria. Of these, 19 experienced an LRR and 16 developed a DM; 2 patients with LRR subsequently developed DM. In those patients with an LRR, 79% had T1/T2 tumors, and 47% had N0/N1 nodal disease, compared with 75% and 6% in the DM group, respectively. The median time to LRR or DM was 0.6 years (interquartile range [IQR], 0.4-1.0) and 1.8 years (IQR, 1.0-2.1), respectively. Salvage treatment with intent to cure was attempted in 23 patients (16 LRR, 7 DM). The median time from LRR or DM to last follow-up for the 18 patients who were still alive after salvage was 1.9 years (IQR, 0.4-3.8; range, 7 days–6.2 years). Estimated cancer-specific survival rates at 3 years following intent-to-cure treatment were 63% (95% CI, 39-100; number still at risk, 5) in the LRR group and 100% (95% CI, 100-100; number still at risk, 2) in the DM group.
Conclusion
Overall, LRR and DM for HPV-positive OPSCC following transoral robotic surgery–based therapy are infrequent. In our subset of patients who underwent intent-to-cure treatment, cancer-specific survival rates were favorable. Therefore, aggressive salvage treatment for LRR and DM for HPV-positive OPSCC should be recommended for appropriate candidates.
Keywords
Unlike most head and neck cancers, the incidence of oropharyngeal squamous cell carcinoma (OPSCC) is rising. Between 1988 and 2004, the incidence of OPSCC in the United States increased by 225%.1,2 This is now known to be due to the rise in human papilloma virus (HPV)–associated OPSCC, which compromises >70% of all oropharyngeal malignancies. 3 According to the Centers for Disease Control and Prevention, HPV-related OPSCC has surpassed the incidence of cervical cancer and is the most common HPV-related malignancy. 3
Fortunately, HPV-positive OPSCC has been associated with significantly better outcomes than HPV-negative OPSCC. A 2012 meta-analysis pooling data from 42 studies found that HPV-positive status improved overall survival and cancer-specific survival (CSS) in OPSCC by 53% and 74%, respectively. 4 Recurrence rates are also lower, with modern studies showing 3-year recurrence-free survival rates up to 96% for HPV-positive tumors.5-10 Despite the growing body of knowledge surrounding primary treatment for HPV-positive OPSCC, little is known about patient outcomes following locoregional recurrence (LRR) or distant metastasis (DM).
Although recurrent OPSCC has been historically associated with extremely poor outcomes,11,12 recent data have suggested that rates of successful salvage may be rising along with the incidence of HPV-related OPSCC. 13 Patients previously assigned to palliative treatments may now benefit from intent-to-cure treatment. Even select patients with relatively good functional status and distant oligometastatic disease have had reportedly curative treatments.14,15 In addition to this, continued advancements in immunotherapy have led to survival improvements in even refractory metastatic disease. 16 Therefore, the goal of this study was to evaluate the outcomes associated with salvage treatment for patients presenting with LRR or DM following transoral robotic surgery (TORS)–based therapy for HPV-positive OPSCC.
Methods
Following Mayo Clinic Institutional Review Board approval (14-004693), all patients who underwent TORS for OPSCC between May 1, 2007, to May 31, 2015, were identified in our institution’s retrospectively updated OPSCC REDCap database. Tumor HPV status was considered positive if either HPV in situ hybridization or HPV p16 was positive and considered negative if both were negative. HPV-negative patients and those with a history of prior head and neck squamous cell carcinoma were excluded. Comorbidities at the time of primary treatment were measured with the Adult Comorbidity Evaluation–27 scale.17-19 OPSCC that occurred in or adjacent to the original subsite <5 years following initial treatment were termed local recurrences. 20 Nodal recurrences were termed regional recurrences. LRR includes both local and regional recurrences. Any squamous cell carcinoma diagnosed outside of the head and neck or within the skin was considered a DM. Second primaries were defined as cancers arising in a separate anatomic subsite separated by normal mucosa or arising >5 years after completion of primary treatment and were excluded. 20 Staging was based on the American Joint Committee on Cancer staging system. 21 Final margin status was classified with the residual tumor classification system. 22 R0 was defined as a lack of tumor at the indicated margin with no specific distance criteria. Surgery included TORS plus concomitant ipsilateral or bilateral neck dissections as indicated by primary subsite and clinical staging. 23 Adjuvant radiotherapy was recommended for patients with T4 tumors and N2b/N2c/N3 disease, and adjuvant chemotherapy (trimodal therapy) was recommended for patients with pathologic extracapsular spread. Some patients declined this recommendation. Salvage treatment for LRR and DM included surgical resection, radiation, and/or chemotherapy.
Statistical Methods
Continuous features were summarized with medians, interquartile ranges (IQRs), and ranges; categorical features, with frequency counts and percentages. LRR/DM-free survival following TORS-based therapy and CSS following LRR/DM were estimated with the Kaplan-Meier method; CSS was compared between groups with log-rank tests. Statistical analyses were performed with SAS 9.4 (SAS Institute, Inc, Cary, North Carolina).
Results
A total of 286 patients with HPV-positive OPSCC met criteria for the study. Of this cohort, 35 patients (12.1%) developed an LRR (n = 19, 6.6%) or a DM (n = 16, 5.6%), with combined disease-free survival (LRR + DM) rates at 1, 2, and 3 years following TORS-based therapy of 93% (95% CI, 90-96; number still at risk [NSAR], 231), 87% (95% CI, 83-92; NSAR, 143), and 85% (95% CI, 80-90; NSAR,87), respectively. Demographics for these patients are detailed in Table 1 . There were 9 regional, 6 locoregional, and 4 local recurrences, as well as 16 distant metastases. Two patients initially presenting with LRR subsequently developed DM. The most common site of DM was the lung (75%), followed by the mediastinum, skeletal bone, liver, and skin; 9 patients had a DM at a single anatomic site, 4 at 2 sites, and 3 at 3 sites.
Patient and Tumor Characteristics for 35 Patients Who Developed LRR or DM Following TORS-Based Primary Therapy for HPV-Positive OPSCC.
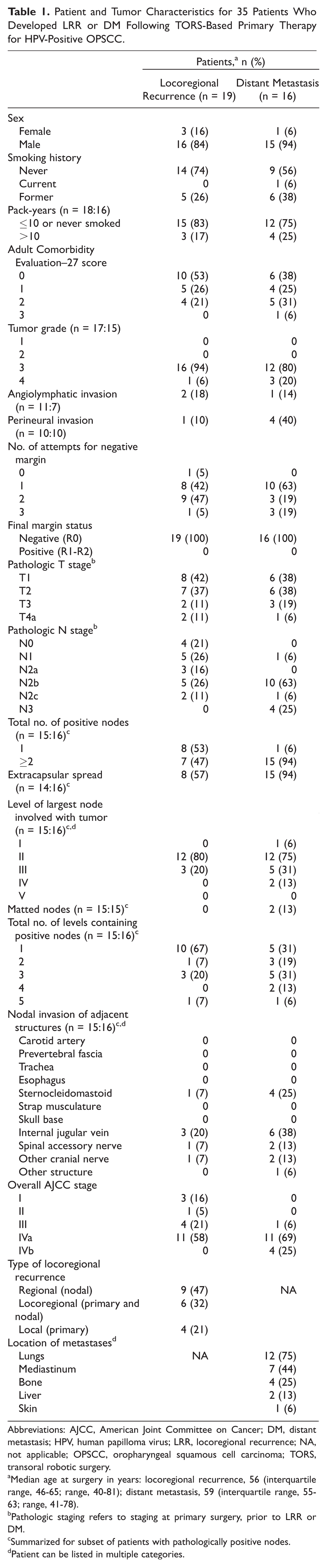
Abbreviations: AJCC, American Joint Committee on Cancer; DM, distant metastasis; HPV, human papilloma virus; LRR, locoregional recurrence; NA, not applicable; OPSCC, oropharyngeal squamous cell carcinoma; TORS, transoral robotic surgery.
Median age at surgery in years: locoregional recurrence, 56 (interquartile range, 46-65; range, 40-81); distant metastasis, 59 (interquartile range, 55-63; range, 41-78).
Pathologic staging refers to staging at primary surgery, prior to LRR or DM.
Summarized for subset of patients with pathologically positive nodes.
Patient can be listed in multiple categories.
Patient and Tumor Characteristics
Most patients in both groups (84%, LRR; 94%, DM) were males, with median ages of 56 and 59 years, respectively (ranges: 40-81, LRR; 41-78, DM). The majority (83%, LRR; 75%, DM) had ≤10 pack-years of smoking. Those who experienced an LRR had fewer comorbidities, with Adult Comorbidity Evaluation–27 scores of 0 or 1 (corresponding to no or mild comorbidities) among 79% of patients, compared with 63% of the DM group.
Approximately 71% of tumors were tonsil primaries, and the remaining 29% were base of tongue (BOT) primaries. T stages were similar between groups, with approximately 79% and 76% of patients in the LRR and DM groups having early T-stage tumors (T1/T2), respectively. Nodal stage was higher in the DM group, with 94% presenting with advanced nodal disease (N2/N3), compared with 53% in the LRR group. On pathologic analysis, perineural invasion and extracapsular spread were more common in the DM group (40% and 94%, DM; 10% and 57%, LRR). Nodal invasion of adjacent structures was present in only 16% (3 of 19) of the LRR group, compared with 50% (8 of 16) of the DM group.
Primary Treatment
All patients underwent TORS via the da Vinci S or Si surgical system (Intuitive Surgical, Inc, Sunnyvale, California). Negative surgical margins (R0) were achieved in all 35 patients, with a median of 1 attempt being required to attain the negative margin. Approximately 68% of those who developed LRR had surgery alone, whereas 81% of the DM group had trimodal therapy. In more than half (57%) of the patients who underwent surgery alone, adjuvant radiation or chemoradiation was recommended but refused by the patient.
Intent-to-Cure (Salvage) Treatment
A total of 23 patients (16 of 19, LRR; 7 of 16, DM) underwent intent-to-cure (salvage) treatment, with the remainder (3 of 19, LRR; 9 of 16, DM) receiving palliative treatment, supportive care, or unknown treatment. A full summary of all patients who underwent salvage treatment can be seen in Table 2 .
Summary of 23 Patients Who Underwent Intent-to-Cure (Salvage) for LRR, DM, or Both.
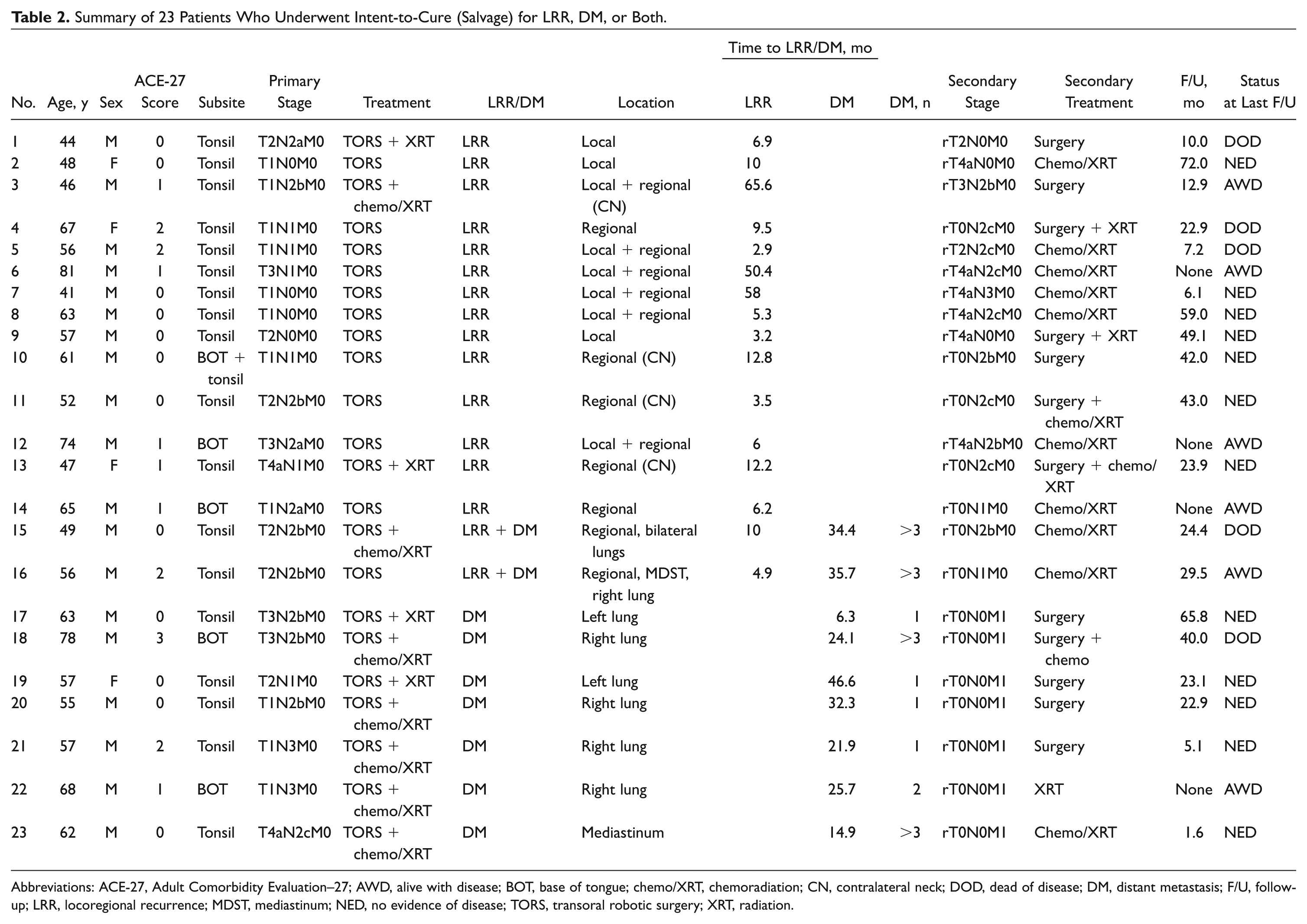
Abbreviations: ACE-27, Adult Comorbidity Evaluation–27; AWD, alive with disease; BOT, base of tongue; chemo/XRT, chemoradiation; CN, contralateral neck; DOD, dead of disease; DM, distant metastasis; F/U, follow-up; LRR, locoregional recurrence; MDST, mediastinum; NED, no evidence of disease; TORS, transoral robotic surgery; XRT, radiation.
Of the 16 patients with LRR who underwent salvage, 19% (3 of 16) had a local recurrence alone; 44% (7 of 16), regional recurrence alone; and 37% (6 of 16), both local and regional recurrence. The majority of patients with LRR (8 of 12, 67%) who had been initially treated with surgery alone were treated with combined chemotherapy and radiation when they had recurrences. Surgery was added in cases of easily resectable regional metastasis (3 of 12, 25%) and in 1 case of an advanced local recurrence. In patients who had initially received adjuvant radiation or chemoradiation, surgery was almost always (3 of 4, 75%) a part of their LRR treatment regimens. The 1 exception (patient 15; Table 2 ) had an unresectable regional recurrence within the deep parotid gland extending superiorly and fixed to the skull base, and nonsurgical therapy was recommended.
All 7 patients with DM who underwent intent-to-cure treatment had either lung or mediastinal metastases. Just over half (4 of 7, 57%) of these patients had solitary lung metastases and underwent wedge resection alone as treatment. One patient (patient 18; Table 2 ) had 2 lung metastases, which were resected, but quickly developed multiple other pulmonary metastases, and chemotherapy was added to his care. The remaining 2 patients had >1 lung or mediastinal metastasis and underwent nonoperative therapy (radiation or chemoradiation).
Oncologic Outcomes
The median time to LRR and DM was 0.6 years (IQR, 0.4-1.0; range, 0.2-5.4) and 1.8 (IQR, 1.0-2.1; range, 0.4-3.8), respectively. One patient did not have any follow-up after LRR. Of the remaining 34 patients, there were 11 deaths at a median of 1.3 years following LRR or DM (IQR, 0.8-2.9 years; range, 0.3-3.4 years), including 5 in the LRR group and 6 in the DM group. All deaths were attributed to OPSCC. The median time from LRR or DM to last follow-up for the 23 patients who were still alive was 1.1 years (IQR, 0.1-3.8; range, 7 days–6.2 years). Estimated CSS rates at 1, 2, and 3 years were as follows: for the LRR group, 79% (95% CI, 60-100; NSAR, 10), 70% (95% CI, 49-100; NSAR, 7), and 58% (95% CI, 35-97; NSAR, 5); for the DM group, 92% (95% CI, 77-100; NSAR, 9), 71% (95% CI, 48-100; NSAR, 5), and 57% (95% CI, 32-100; NSAR, 4; P = .43). CSS in both the LRR and DM groups is illustrated in Figure 1 .
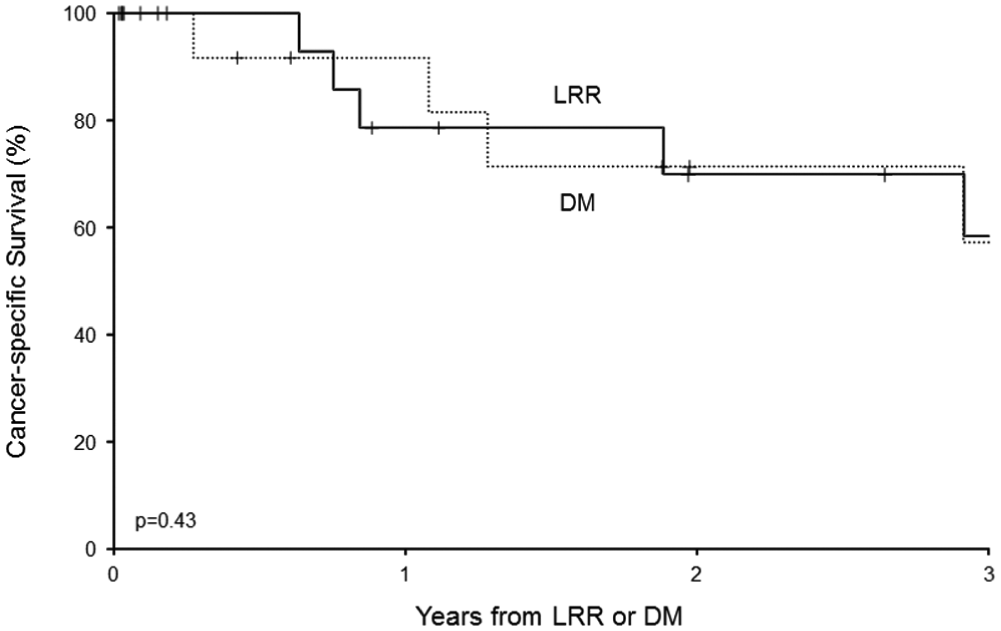
Cancer-specific survival from date of diagnosis of recurrent disease for all patients who developed a locoregional recurrence (LRR) or distant metastasis (DM; P = .43). All patient deaths were from their cancer; therefore, this figure also represents overall survival.
A total of 23 patients underwent intent-to-cure treatment, 16 with LRR and 7 with DM. Of these, 5 died from disease (4, LRR; 1, DM) at 0.6, 0.8, 1.9, 2.9, and 3.4 years following LRR or DM. Eight of 16 (50%) patients with LRR and 5 of 7 (71%) patients with DM had no evidence of disease at last follow-up. The median time from LRR or DM to last follow-up for the 18 patients who were still alive was 1.9 years (IQR, 0.4-3.8; range, 7 days–6.2 years). Estimated CSS rates at 1, 2, and 3 years following intent-to-cure treatment were as follows: in the LRR group, 85% (95% CI, 67-100; NSAR, 10), 75% (95% CI, 54-100; NSAR, 7), and 63% (95% CI, 39-100; NSAR, 5); in the DM group, 100% (95% CI, 100-100; NSAR, 4), 100% (95% CI, 100-100; NSAR, 2), and 100% (95% CI, 100-100; NSAR, 2), respectively. CSS following intent-to-cure treatment in both the LRR and DM groups is illustrated in Figure 2 . CSS was not compared statistically between the groups in this subset, since only 5 deaths from disease were observed.
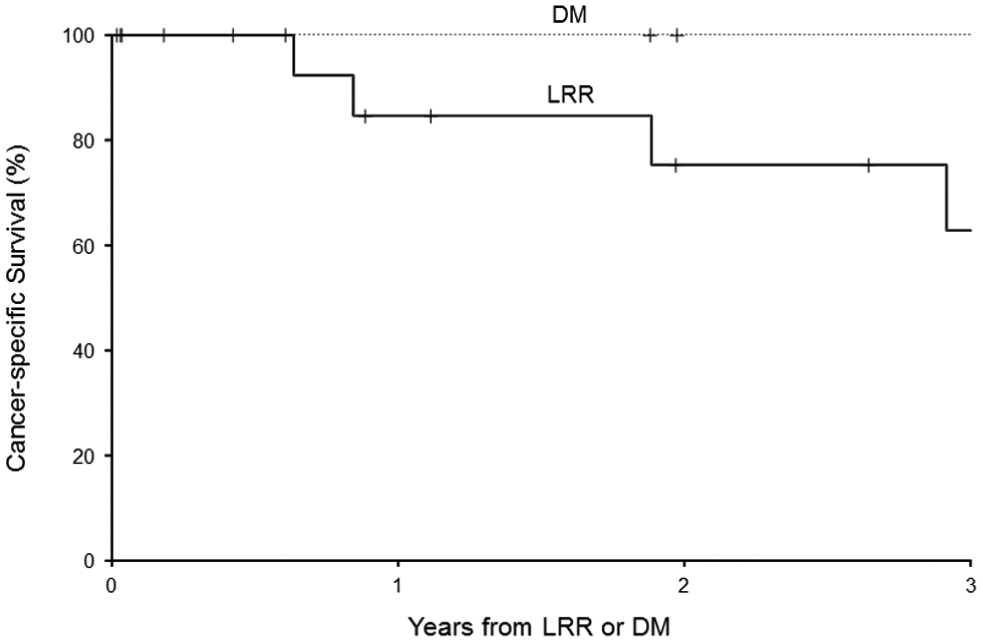
Cancer-specific survival from date of diagnosis of recurrent disease for all patients undergoing intent-to-cure (salvage) treatment following locoregional recurrence (LRR) or distant metastasis (DM). All patient deaths were from their cancer; therefore, this figure also represents overall survival.
Discussion
Most patients with HPV-positive OPSCC do remarkably well, with 3-year CSS reported as >90% in some TORS studies.6,10 However, somewhere between 4% and 23% of all patients will experience a recurrence within 2 to 3 years of initial treatment, most commonly as a locoregional failure.5-10 The rate of DM after primary treatment is slightly lower, at 2% to 12%, depending on the study.10,14,15,24-27 In our cohort, we found overall rates of LRR and DM to be 6.6% and 5.6%, respectively. These rates are applicable to all patients who meet criteria for TORS-based therapy, but they should not be applied to those whose disease is so advanced that they require more aggressive surgical options or are deemed unresectable. As the head and neck community continues to push for de-escalation of therapy for select patients with HPV-positive OPSCC, it is critical to understand not only the rates of LRR and DM but also the outcomes associated with salvage therapy.
Prior to the era of HPV-related OPSCC, salvage rates for recurrent OPSCC were dismal. In 1974, Gilbert and Kagan described recurrence patterns for head and neck cancers in a landmark review article. 11 They reported salvage rates for cancers in the “tonsil region” to be extremely low, at 3.5% to 18.9%. More than 25 years later, a combined prospective study and meta-analysis showed only slight improvement from the 1970s, reporting 2-year recurrence free survival rates of 24% to 28% following salvage surgery. 12 These authors ultimately questioned the utility of salvage surgery in many patients with recurrent OPSCC. However, more recently, a meta-analysis and systematic review compared overall survival rates from 22 studies examining patients with locoregionally recurrent OPSCC. 13 The pooled 3-year overall survival was similar to previous studies, at 26%; however, when they separated the studies by time, they found that 5-year overall survival increased to around 50% in studies performed after the year 2000. Our findings further support this improvement in survival in the modern era, as our 3-year CSS rate was 71% in patients who underwent salvage therapy.
The decision to pursue salvage for LRR depends on size, location, and extent of the recurrence, as well as the prior treatment received by the patient and the patient’s performance status. In our cohort, only 3 of 19 patients with LRR did not undergo salvage, with 2 of these receiving unknown treatment at outside institutions and 1 receiving supportive cares due to significant medical comorbidities and poor performance status. An association between higher T-stage recurrences and poorer surgical salvage outcomes was described in a retrospective study of 175 patients who underwent salvage surgery after failed primary radiation. 28 Zafereo et al also noted that increasing T stage of recurrences had a negative impact on survival in patients undergoing salvage surgery, although this relationship did not quite reach statistical significance (P = .07). 29 We did not see this association in our cohort, likely because most of our patients (6 of 7, 86%) with higher T-stage (T3/T4) recurrences were initially treated with surgery alone and were therefore chemotherapy and radiation naive. These patients did relatively well with salvage (5 of 6, chemoradiation; 1 of 6, surgery + radiation), with 4 patients having no evidence of disease (0.8, 4.3, 5.0, and 6.2 years of follow-up) and the other 2 patients classified as alive with disease because they are currently undergoing treatment.
Similarly, higher N-stage recurrences have been associated with worse survivals.13,28 While 75% (3 of 4) of patients in the LRR group who died from their cancer had advanced nodal recurrences (N >1), some patients with more advanced N stages did well in our cohort. Specifically, patients who had regional recurrences in contralateral, untreated necks (rT0N2c) did very well, with all 3 of these patients having no evidence of disease at 2.0, 3.4, and 3.8 years of follow-up. We therefore recommend neck dissection with or without postoperative radiation or chemotherapy in cases of delayed contralateral neck nodal metastases.
When deciding on whether to pursue surgical versus nonsurgical salvage modalities, one should consider the patient’s previous treatment, the resectability of the recurrence, and the morbidity of both modalities. As mentioned, for patients with no history of previous radiation or chemotherapy, nonoperative salvage can be highly effective and should be strongly considered regardless of the stage of the LRR. When the primary treatment did include radiation or chemoradiation, the patients in the current study almost all had surgery as part of their salvage treatment; however, due to the low number of LRRs in this study, it is difficult to draw meaningful conclusions about the efficacy of surgical versus nonsurgical salvage in the context of previous radiation. A recent systematic review and meta-analysis reported superior 5-year overall survival after surgical salvage versus reirradiation (26% vs 16%, P < .001), although this difference may be mostly related to selection bias. 13
Historically, DM from head and neck cancer squamous cell cancer has been associated with a dismal prognosis, with 1-year survival after diagnosis reported to be as low as 7%. 30 However, with the HPV epidemic of OPSCC, it is possible that younger, healthier patients with HPV-positive metastases may respond better to treatment. In fact, salvage for pulmonary metastases in patients with HPV-positive OPSCC has been reported, although CSS in these studies was low (11%-16%).14,15 Interestingly, in the current study, the 3-year CSS in the DM group was 57%. The best candidates for salvage after DM are patients with relatively good functional status with a solitary lung metastasis. All 4 patients in our cohort who met these criteria underwent wedge resection of their metastasis alone and have no evidence of locoregional or distant disease with 0.4, 1.9, 2.0, and 5.4 years of follow-up. It is less clear whether patients with multiple pulmonary or mediastinal metastases benefit from salvage, as 1 of these patients in our cohort died from cancer at 3.4 years and the other 2 patients have inadequate follow-up (1 week and 7.3 months).
Some limitations of the current study should be noted. The focus of this study is a highly selected group of patients who were good candidates for salvage treatment from an oncologic and medical comorbidity standpoint; therefore, selection bias plays a role in the reported survival outcomes. Other limitations include the retrospective nature of this study, a small overall number of LRRs and DMs, and initial undertreatment of some patients with more advanced disease who refused adjuvant therapy. Finally, we have a relatively short follow-up (median, 1.9 years; IQR, 0.4-3.8; range, 7 days–6.2 years), which should be considered when interpreting our survival analyses. With more and more emphasis on de-escalation of therapy for HPV-related OPSCC, the importance of long-term follow-up should be emphasized. While most LRRs and DMs were found within the first 2 years after primary treatment, some presented up to 4 to 5 years posttreatment.
Conclusion
The oncologic utility of performing salvage treatments in recurrent and metastatic OPSCC has been questioned in the past. 12 However, with the HPV-OPSCC epidemic, the patients developing LRR and DM are younger and healthier, have a longer baseline life expectancy, and theoretically may have tumors that are more sensitive to salvage treatment. Of the 6.6% and 5.6% of patients with HPV-positive OPSCC who respectively developed LRR and DM in our cohort, the CSS for those undergoing salvage was 63% and 100% at 3 years. These data indicate that salvage treatment for LRR and DM for HPV-positive OPSCC can and should be recommended to patients who are candidates for salvage therapy. Ideal candidates for salvage after LRR include most patients who have not had prior radiation or chemotherapy treatment and patients who have regional recurrences in contralateral untreated necks. The best candidates for salvage after DM are patients with solitary pulmonary metastasis amenable to wedge resection. Further study is needed to understand the functional outcomes and morbidity associated with salvage therapy.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2016 AAO-HNSF Annual Meeting & OTO EXPO; September 18-21, 2016; San Diego, California.