
Abstract
Objectives
Document human motions associated with cochlear implant electrode insertion at different speeds and determine the lower limit of continuous insertion speed by a human.
Study Design
Observational.
Setting
Academic medical center.
Subjects and Methods
Cochlear implant forceps were coupled to a frame containing reflective fiducials, which enabled optical tracking of the forceps’ tip position in real time. Otolaryngologists (n = 14) performed mock electrode insertions at different speeds based on recommendations from the literature: “fast” (96 mm/min), “stable” (as slow as possible without stopping), and “slow” (15 mm/min). For each insertion, the following metrics were calculated from the tracked position data: percentage of time at prescribed speed, percentage of time the surgeon stopped moving forward, and number of direction reversals (ie, going from forward to backward motion).
Results
Fast insertion trials resulted in better adherence to the prescribed speed (45.4% of the overall time), no motion interruptions, and no reversals, as compared with slow insertions (18.6% of time at prescribed speed, 15.7% stopped time, and an average of 18.6 reversals per trial). These differences were statistically significant for all metrics (P < .01). The metrics for the fast and stable insertions were comparable; however, stable insertions were performed 44% slower on average. The mean stable insertion speed was 52 ± 19.3 mm/min.
Conclusion
Results indicate that continuous insertion of a cochlear implant electrode at 15 mm/min is not feasible for human operators. The lower limit of continuous forward insertion is 52 mm/min on average. Guidelines on manual insertion kinematics should consider this practical limit of human motion.
Keywords
Cochlear implant (CI) technology has improved steadily over the past decades and is now considered the standard of care to restore hearing in patients with sensorineural hearing loss. The effectiveness of CIs has been documented in numerous prior studies and has improved such that CI patients are able score to 100% on traditional speech perception performance metrics, necessitating more difficult material for testing. 1 More recently, indications for CI have expanded to include patients with residual hearing.2,3
Some patients are able to maintain a capacity for native hearing in the implanted ear after surgery, which results in increased word understanding during noise and improved music appreciation. 4 A level of native hearing retention even after implantation is referred to as hearing preservation. The precise factors correlating with the degree of postsurgical hearing preservation are yet to be understood, but age at implantation, degree of preimplant residual hearing, pharmacologic therapy, surgical technique, electrode design, and others are under investigation. 5 CI criteria expansion has stimulated the development of novel surgical techniques aimed to preserve residual hearing in the implanted ear, specifically in the low frequency range. 4
Current CI surgery involves a mastoidectomy and access to the middle ear via a facial recess approach. Insertion of the CI electrode into the scala tympani is then performed either through the round window or the creation of a separate cochleostomy. 6 Prior work by Carlson et al 7 has established that attempting to limit insertion trauma during the procedure is one key factor in preserving residual hearing; more specifically, it was found that less traumatic insertions, estimated according to the difference between pre- and postimplant audiometric thresholds, enable the preservation of residual hearing. The better preservation of residual hearing is thought to be a surrogate of better cochlear structural preservation during implantation. 7 True atraumatic CI surgery is impossible since by nature, surgery disrupts native anatomy; however, in such a delicate procedure, even minute movement may prove critical. With this in mind, a number of “atraumatic” insertion techniques have been proposed to maximize preservation of residual hearing.8,9 Nonetheless, little consensus exists around one important parameter: insertion speed, which is suspected to play a fundamental role in cochlear trauma. 5 While a number of different insertion speeds have been studied in the literature,10-14 little is understood about a surgeon’s ability to perform a CI insertion at these speeds. Aiming to address this gap in the knowledge, this work presents an analysis of the human kinematics during CI insertion and uses the results to discuss existing insertion speed recommendations.
Previous attempts to determine an optimal CI insertion speed were based on the minimization of parameters such as intracochlear pressure, 10 frictional forces,11,14 insertion forces, 12 and/or hearing preservation. 13 These works are summarized in Table 1 . Multiple studies used robotic inserters for precise insertion speed control,10-12,14 whereas others involved human participants and relied on video analysis to determine the average insertion speed.12,13 This variety of studies and approaches has resulted in a number of different speed recommendations, ranging between 15 and 96 mm/min; however, none of the investigations conducted thus far took into account the limits of human hand motion. Furthermore, these studies did not evaluate micro-motions (ie, the fine and sometimes unrecognizable movements that take place in a surgeon’s hand during the insertion).
Insertion Speed Literature Summary.
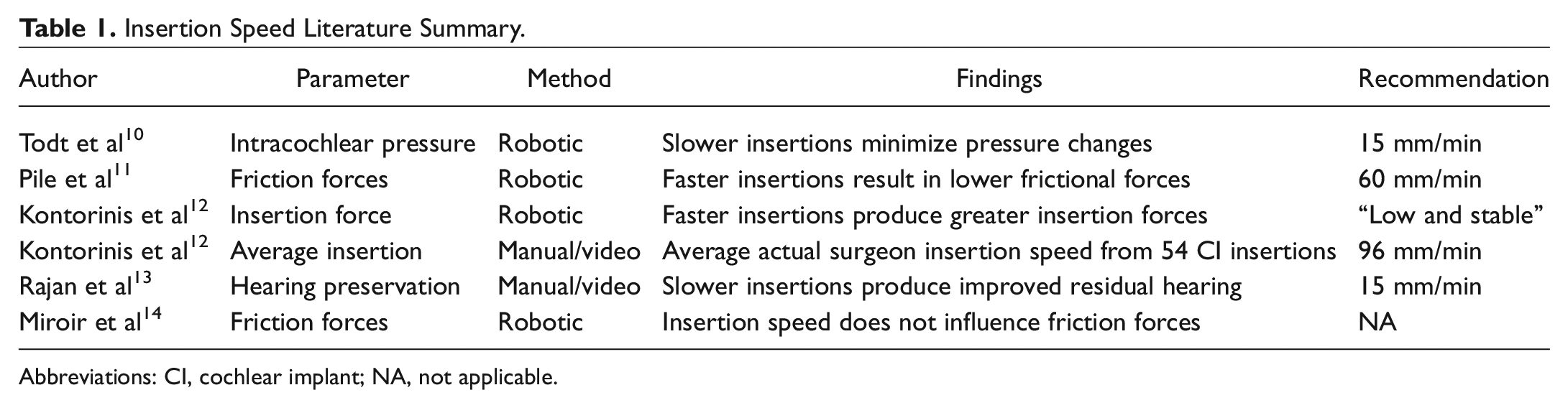
Abbreviations: CI, cochlear implant; NA, not applicable.
To overcome these limitations of prior works, this study investigates the limits and capabilities of manual CI insertion—the information derived here will provide a useful frame of reference to restrict the search range of the optimal insertion speed. To date, no investigation into the micro-motions taking place during CI insertion or a surgeon’s ability to insert at a given reference velocity has been performed. This study documents and characterizes the human motions associated with CI electrode insertion and proposes a lower limit of attainable continuous forward insertion speed.
Methods
This study was evaluated and approved by our institutional review board (IRB). Participants in the study were recruited by phone, email, and/or direct personal communications and included either otolaryngologists who perform CI surgery as part of their practice or otolaryngology residents at an Accreditation Council for Graduate Medical Education–approved residency program. Residents in their first year of training were excluded from the study due to a lack of CI-specific surgical training. Participants were informed about the risks and benefits of participating in the study and signed an IRB-approved informed consent form.
A pair of modified CI forceps, the surgical instrument typically used in CI surgery, were used in the experiments ( Figure 1 ). Reflective marker spheres were mounted to the forceps using a lightweight 3-dimensional printed frame, which enabled tracking of the precise location of the tip of the forceps with an optical tracking system. 15 A Polaris Spectra optical tracking system (Northern Digital, Waterloo, Ontario, Canada) was positioned above the study workspace with a clear view of the forceps ( Figure 2 ). A cube of bone surrogate material with a machined hole (Pacific Research Laboratories, Vashon Island, Washington) was positioned in a temporal bone mount and served to represent the insertion channel. A standard 31-mm, 12-contact electrode array (MED-EL, Innsbruck, Austria) was used in the insertion trials. Study subjects performed the testing seated, as they would in the operating room. The participants were allowed to adjust the location of the temporal bone mount on the work surface to maximize comfort and improve positioning for the insertion of the electrode into the model using their dominant hand. Subjects were allowed to stabilize their dominant hand as they would during an actual CI insertion in the operating room.
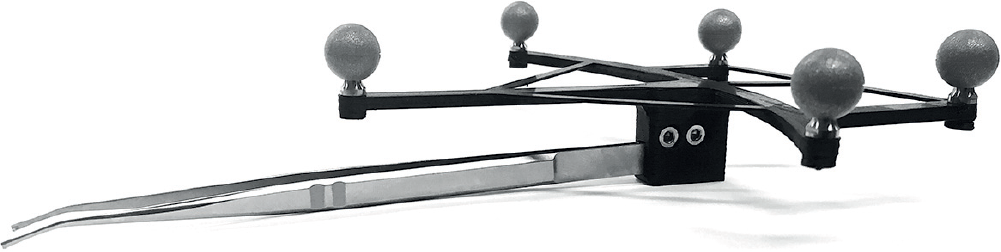
Standard pair of cochlear implant forceps used during implantation surgery that have been fitted with a ridged 3-dimensional printed frame and fiducial optical tracking spheres.
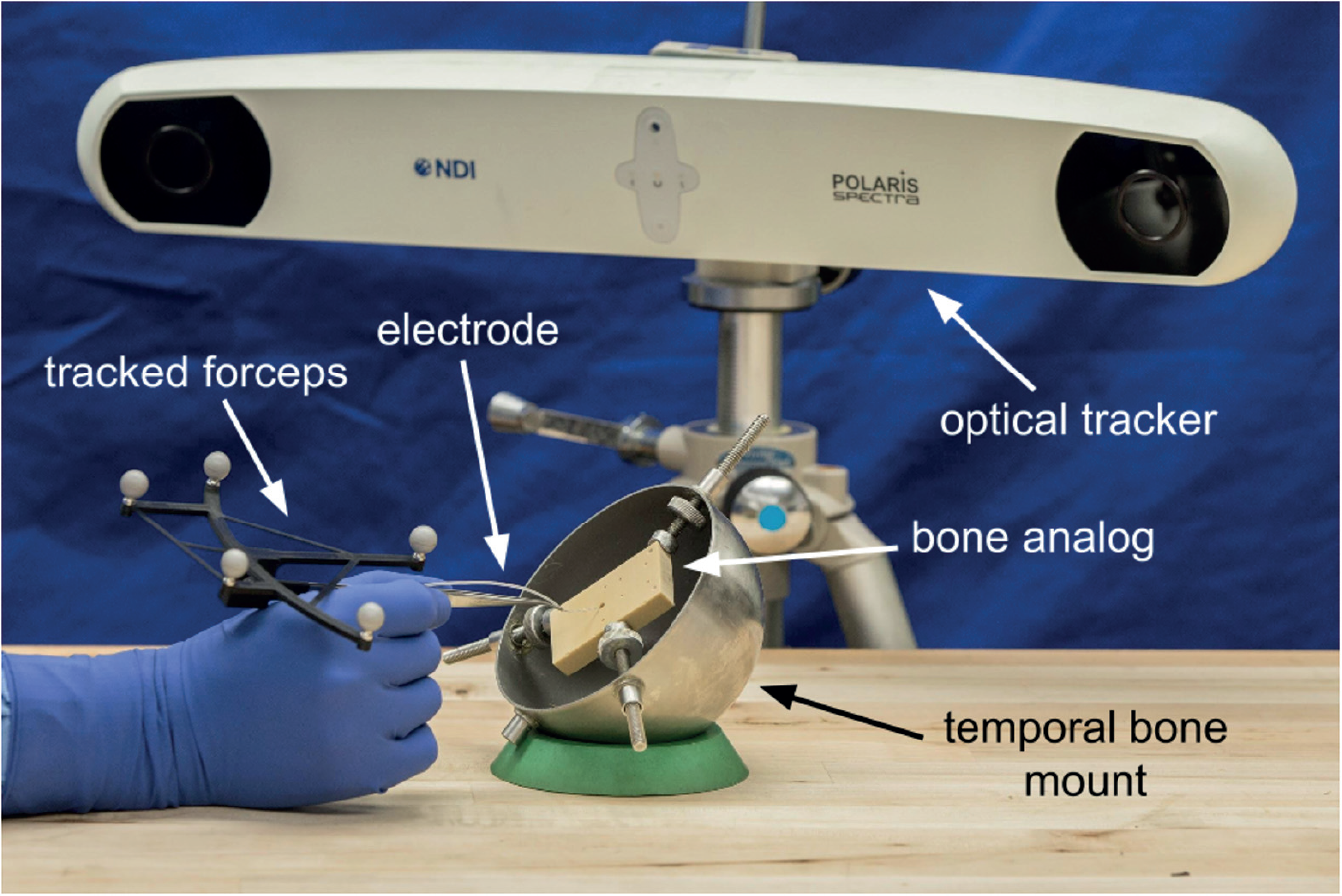
Experimental setup and cochlear implant forceps. The participant is seated and performs insertions of the electrode while movements are tracked and recorded by the optical tracking system.
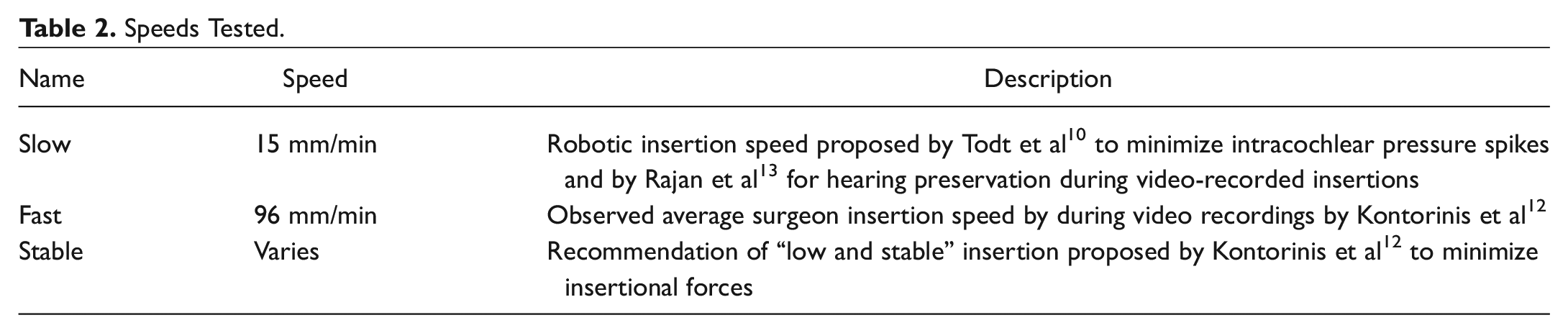
As part of the experiments, participants were asked to insert the CI electrode using 3 different reference speeds, which were chosen from prior recommendations in the literature. These experimental conditions are summarized in Table 2 . The slowest reference speed was set at 15 mm/min, based on recommendations to reduce intracochlear pressure changes and preserve residual hearing.10,13 The fastest condition was 96 mm/min, the estimated average clinical insertion speed. 12 Finally, the last condition, which was designated as “stable,” was defined as “as slow as possible without stopping forward motion,” following the recommendations of Kontorinis et al 12 to minimize insertion forces. These reference speeds will, throughout the manuscript, be referred to as “slow,” “fast,” and “stable,” respectively.
Speeds Tested.
At the beginning of each insertion trial, the surgeon gripped the electrode and positioned it at the opening of the simulated cochleostomy. Rather than instructing the study subjects to insert at a given speed (eg, “Insert at 96 mm/min”), they were provided an insertion time that correlated to the reference velocity and the length of electrode (eg, “Insert over 18 seconds”). For the insertions with set reference velocities (slow and fast), a verbal prompt at 25%, 50%, 75%, and 100% of the elapsed insertion time allowed participants to gauge their insertion progress while remaining focused on the insertion itself. A 5-second verbal countdown was given, at which point the participant began advancing the electrode into the cochleostomy. The participants were instructed to insert as smoothly as possible without stopping while completing the insertion during the given time. Each of the participants performed 3 insertions per reference velocity, for a total of 9 insertions per surgeon. The optical tracking system recorded the motion of the forceps during each insertion at a sample rate of 60 Hz.
Data recorded from each insertion consisted of coordinates for the position of the forceps’ tip at each sample point. The target registration error in the measurement was calculated to be less than 0.3 mm based on the arrangements of the fiducial markers and optical tracking system accuracy. 15 Data analysis was conducted with MATLAB (MathWorks, Natick, Massachusetts): the position data were smoothed to eliminate signal noise using a linear regression smoothing function; then, the following 3 metrics were calculated: time at reference speed, stopped time, and number of reversals. The time at reference speed is defined as the amount of time the participant’s speed was within 20% of the indicated reference speed. This parameter was chosen to represent the surgeon’s ability to accurately insert at a given reference speed. The stopped time is the percentage of insertion time during which the electrode was not making forward progress. Finally, the number of reversals is the number of times that the subject changed from forward motion to backward motion during the insertion. The nonparametric Wilcoxon rank sum test was used for statistical analysis since a normal distribution of this small sample size could not be assumed. In addition, the Wilcoxon rank sum test allowed for comparison between 2 specific conditions rather than the more generalized Kruskal-Wallis test (the nonparametric equivalent of analysis of variance testing). However, since multiple comparisons were made, a more conservative level of significance was selected based on the Bonferroni correction for multiple tests. Comparisons between the calculated parameters for each reference insertion speed (time at reference speed, stopped time, and number of reversals) were performed using a Wilcoxon rank sum test with P < .01 set as the cutoff for statistical significance.
Results
Fourteen total surgeons were recruited and agreed to participate in the insertion testing. Four of these were attending surgeons who routinely perform CIs, 2 were neurotology fellows, and the remaining 8 were otolaryngology residents. Each participant performed 3 repetitions for each of the 3 reference speeds, resulting in a total of 126 tracked insertions. All participants were included in the final data analysis.
Sample data from a single surgeon’s insertions are illustrated in Figure 3 , while aggregate metrics for all participants are summarized in Table 3 . The percent time at reference speed results for each insertion are shown in Figure 4 . The mean insertion speed for the stable insertions was 52.3 mm/min with a standard deviation of 19 mm/min. The differences between the fast and slow insertions were statistically significant (P < .01) for all metrics. There was no statistical difference in the time at reference speed between the fast and stable insertions (P = .89). In addition, there was no statistical difference in performance metrics between attending surgeons and those in training at the 3 insertion speeds tested.
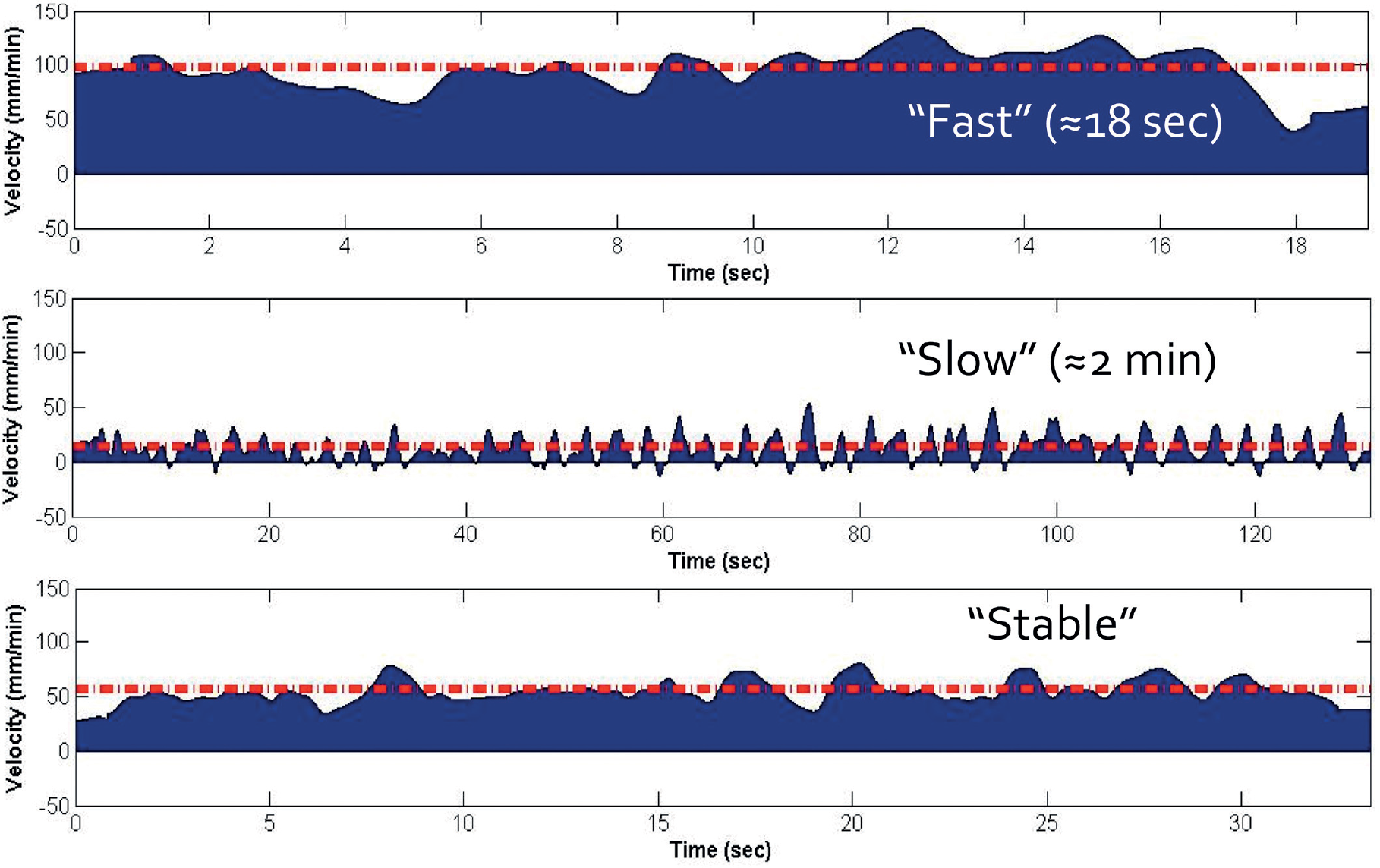
Single participant sample velocity profiles highlighting differences between each reference speed. The dashed data line shows the reference speed for insertion. Velocities below the x-axis represent backward motion (reversal).
Results According to Reference Speed.


Actual insertion speed vs percent time within 20% of the prescribed reference speed for each insertion performed and grouped by prescribed reference speed.
Discussion
Prior research shows that slower CI insertion speeds may be superior at preserving residual hearing, which is thought to be correlated with decreased insertional resistance and diminished intracochlear trauma. 13 However, limited data exist regarding whether human operators are actually able to achieve the speeds described and what consequences may be associated with such slow motion. For example, we found that the slowest insertion speed is associated with the largest number of insertion reversals. The consequence of these reversals is unknown but likely involves the electrode sliding back and forth over intracochlear tissue, potentially leading to tissue damage.
To understand the reason why noncontinuous motion leads to increased tissue damage requires a basic understanding of frictional forces. In the classical model, the impact of friction on motion consists of 2 components—static and kinetic friction. Static friction results from interactions between the stationary molecules of each contact surface and is usually greater than kinetic friction 16 resulting in more force being necessary to put an object in motion than is needed to maintain that motion. This concept can be easily understood by thinking of moving a heavy piece of furniture across the floor. Much force is required to overcome the static friction and begin moving the object, and less force is required to keep the object in motion overcoming kinetic friction.
In the case of noncontinuous CI insertion, the surgeon must repeatedly overcome the larger static friction force imparting more force onto the cochlea, likely resulting in unrecognized intracochlear trauma. This concept has been previously proposed by other investigators.14,17 What is unknown is whether the increased frictional forces associated with slow, noncontinuous insertions are more harmful to intracochlear tissue then the potentially larger intracochlear pressures associated with faster, continuous insertions. 10
During the stable insertions, calculated metrics were similar to those of the fast insertion. Specifically, the percentage of insertion at the correct reference speed was similar to the fast insertion despite the stable insertions being performed at almost half the speed. Based on the performance metrics, the speed produced by the stable insertions likely represents a speed at which surgeons are able to insert at a constant forward velocity while avoiding the detrimental effects of static friction. If future studies definitively show that slower insertion speeds are associated with improved audiological outcomes, automated (aka robotic) assistance during CI insertion may be necessary.
This study is not without limitations, including the number of participants and their association with the same academic medical center. With this limited sample size, statistically different insertion parameters between those in training compared with those in clinical practice did not exist. It is possible that a surgeon’s limited ability to insert a CI electrode at a constant velocity may be a function of human limits rather than correlating with level of experience or training. However, given the limited sample size, the study was underpowered to draw conclusions relating to level of training and insertion abilities. This, in addition to the concern that our data may not be representative of a larger population, emphasizes the need for further research on the subject.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2016 AAO-HNSF Annual Meeting and OTO EXPO; September 18-21, 2016; San Diego, California.