
Abstract
Objectives
(1) Develop a novel method for serial assessment of gene and protein expression in laryngotracheal stenosis (LTS). (2) Assess cytokine expression and determine an immunophenotype in LTS.
Study Design
A matched comparison of endolaryngeal brush biopsy samples from laryngotracheal scar and normal airway.
Setting
Tertiary care hospital, 2015-2016.
Methods
Brush biopsy specimens of laryngotracheal scar and normal trachea were obtained from 17 patients with LTS at the time of operating room dilation and were used for protein and RNA extraction. Gene expression of the TH1 cytokine interferon γ (INF-γ), TH2 cytokine interleukin 4 (IL-4), transforming growth factor β, and collagen 1 (Coll1) was quantified with quantitative real-time polymerase chain reaction. Cytokine analysis was performed with flow cytometry with a cytometric bead array.
Results
LTS specimens demonstrated a 13.68-fold increase in Coll1 gene expression versus normal (P < .001, N = 17). Additionally, IL-4 gene expression showed a 3.76-fold increase (P < .001, N = 17) in LTS scar. When stratified into iatrogenic LTS and idiopathic subglottic stenosis cohorts, INF-γ gene expression was significantly increased in idiopathic subglottic stenosis (P = .011). Soluble cytokine measurements were below the limit of detection for reliable quantification and thus could not be assessed.
Conclusions
Brush biopsies from LTS samples can be successfully utilized for RNA extraction and demonstrate the expected increase in Coll1 gene expression associated with LTS. Preliminary gene expression suggests that abnormal collagen production may be mediated by the TH2 cytokine IL-4 and that increased INF-γ expression may represent a key difference between iatrogenic LTS and idiopathic subglottic stenosis. Further analysis of soluble cytokines is needed to confirm these findings.
Laryngotracheal stenosis (LTS) is the pathologic narrowing of the larynx, subglottis, and/or trachea. This narrowing is secondary to excessive scar tissue formation and often leads to dysphonia and/or dyspnea in patients. LTS can result from multiple etiologies—iatrogenic (postintubation injury), autoimmune, radiation induced, or idiopathic—with most cases of LTS being iatrogenic and idiopathic. Distinct clinical profiles exist between iatrogenic LTS (iLTS) and idiopathic subglottic stenosis (iSGS). iSGS primarily affects middle-aged Caucasian females with no underlying autoimmunity or history of previous intubation, while iLTS affects a more heterogeneous population.1,2 Despite recognition of these unique demographics, our understanding of the pathogenesis of LTS and how it varies among etiologies is poorly understood and is a barrier to improving medical therapies for LTS.
Research investigating the pathogenesis of LTS is sparse secondary to the rarity and heterogeneity of the disease. For iLTS, current literature suggests that an initial epithelial and subepithelial injury leads to a prolonged and dysregulated wound-healing response that promotes the deposition of pathologic scar in the airway.3,4 Efforts to characterize the aberrant wound healing in iLTS have utilized in vivo animal models, which demonstrate a critical role for the adaptive immune response in the development of airway stenosis, thus implicating an immune mechanism in the pathogenesis of iLTS.5,6 Underlying mechanisms for the pathogenesis of iSGS are less well defined. Several hypotheses for the pathogenesis of iSGS exist and include changes in estrogen and estrogen-level receptors and microtrauma to the airway; however, these hypotheses have not been clearly demonstrated. 7 More recently, characterization of the local microbiota and immunologic milieu in iSGS has demonstrated unique populations of bacteria and has identified changes in the interleukin 17 (IL-17) signaling axis, thus implicating a potential immunologic mechanism for iSGS as well.7,8
Given the proposed role of the inflammatory system in the pathogenesis of iLTS and iSGS, the development of a method for minimally invasive assessment of inflammation in human LTS would be beneficial in improving our understanding of the immunopathogenesis of this disease. Additionally, characterization of serial changes in inflammation in iLTS and iSGS would provide information about disease progression and could identify a biopredictive marker that would allow for risk stratification and help the clinician and patient guide treatment plans. Ideally, this method would be applicable to an office-based setting so that serial assessment of inflammation after operating room–based intervention could be monitored. Additionally, the platform for this test would be a single modality that provides information at the genetic and posttranslational levels. The goal of this study was to assess the efficacy of a novel brush biopsy technique for measurement of inflammatory cytokines and determination of an immunophenotype in iLTS and iSGS patients.
Methods
Patient Selection
Brush biopsies of human laryngotracheal scar and normal-appearing areas of the airway were procured during routine dilation of subglottic and tracheal stenosis in 17 consecutive patients with a diagnosis of iSGS or iLTS between 2015 and 2016. All patients in this study signed informed consent, and approval for this study was granted by the Johns Hopkins Institutional Review Board (NA_00078310). Clinical history was abstracted and reviewed for each patient.
LTS Tissue Sampling
Brush biopsies of human laryngotracheal scar and normal-appearing areas of the airway were obtained with a 1.0-mm-diameter bronchial cytology brush (ConMed, Utica, New York). Specimens were procured at the time of routine operating room dilation of subglottic and tracheal stenosis. Brushes biopsy samples were immediately housed in 1.5-mL sterile conical tubes and placed on dry ice until they could be stored at −80°C. Brush biopsy samples were stored for no longer than 4 weeks prior to processing.
Gene Expression Analysis by Quantitative Real-time Polymerase Chain Reaction
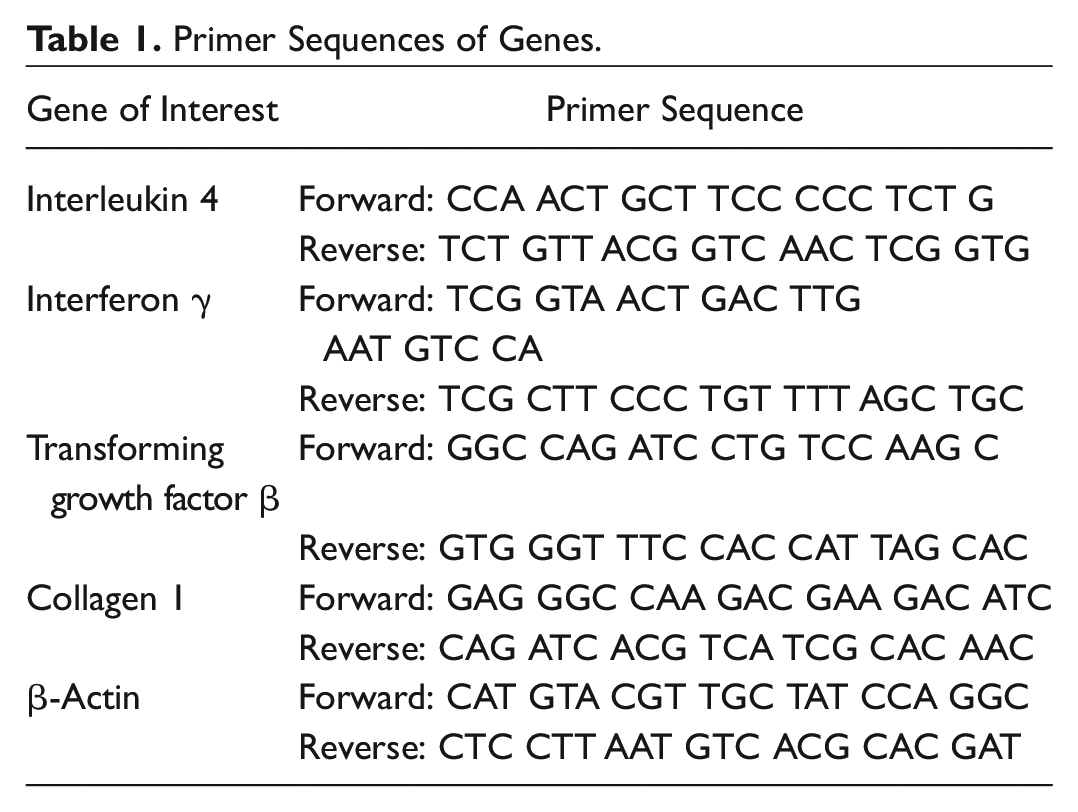
RNA was extracted and purified from brush biopsies with a RNeasy Microkit as part of the AllPrep RNA/Protein kit (Qiagen, Valencia, California). RNA was quantified with a NanoDrop 2000 spectrophotometer (Thermo Scientific, Waltham, Massachusetts) and then used for the creation of complementary DNA. Gene expression was assessed by quantitative real-time polymerase chain reaction (PCR) with a StepOnePlus Real Time PCR system (Life Technologies, Carlsbad, California) and Power SYBR Green Mastermix (Life Technologies). Complementary DNA samples were diluted 1:30, and 1 μL was combined with 10 μL of Mastermix, 8 μL of ddH2O, and 0.5 μL of 10μM forward and reverse primer for the gene of interest (total volume of 20 μL). Each reaction well underwent 40 cycles of a denaturation step at 95°C for 15 seconds, followed by annealing and extension at 60°C for 60 seconds. The cycle threshold for gene product detection (CT) of the gene of interest was normalized against the CT value for the reference gene β-actin (ΔCT) for all samples and then compared with normal controls (ΔΔCT). Gene expression is presented as the relative fold change calculated by 2-ΔΔCT. All samples were investigated in triplicate. Gene expression was quantified for the fibrosis-related gene collagen 1 (Coll1), as well as the cytokines transforming growth factor β, IL-4, and interferon γ (INF-γ; Table 1 ).
Primer Sequences of Genes.
Flow Cytometry of Inflammatory Cytokines
Protein was extracted from brush biopsy samples with RIPA buffer (50mM Tris-HCL, 150mM NaCl, 2% NP-40, 1% Na deoxycholate, 0.2% SDS), 10µM PMSF, 50µM EGTA, 10µM Na orthovanadate, 0.5 mM Na fluoride, and 1% cOmplete Protease Inhibitor Cocktail (Sigma-Aldrich, St Louis, Missouri). Protein concentrations were determined with a standard curve assay. A panel of 6 cytokines—IL-2, IL-4, IL-6, IL-10, tumor necrosis factor, and INF-γ—were detected with a commercially available cytometric bead array (BD Biosciences, San Jose, California) and analyzed with a Accuri C6 Plus Flow Cytometer (BD Biosciences). Data were normalized and quantified on a standard curve.
Statistical Analysis
Differences between LTS scar and normal trachea samples were compared with a nonparametric Wilcoxon matched-pairs signed-rank test. A Mann-Whitney test was used to assess differences between the iSGS and iLTS subgroups. Results are displayed as mean fold change and 95% CI. A type I error rate (α) <0.05 was considered statistically significant. A Bonferroni correction (α/m) was applied to adjust for multiple hypotheses (m = 3), making the level of statistical significance in this study at a P value <.0167. Data analysis was performed with Prism software (GraphPad Software Inc, La Jolla, California).
Results
Demographics
Brush biopsy specimens were collected from a total of 17 patients with a diagnosis of iLTS (n = 9) or iSGS (n = 8). The average age of this group was 43.8 years. The majority of patients in this group were Caucasian (82.1%) and female (94%; Table 2 ). There were no significant differences in age, sex, or race between the iatrogenic and idiopathic cohorts of patients. There was an increased propensity of patients who were tracheostomy dependent in the iatrogenic cohort (55% vs 0%, P = .03)
Demographic Data of Study Patients. a
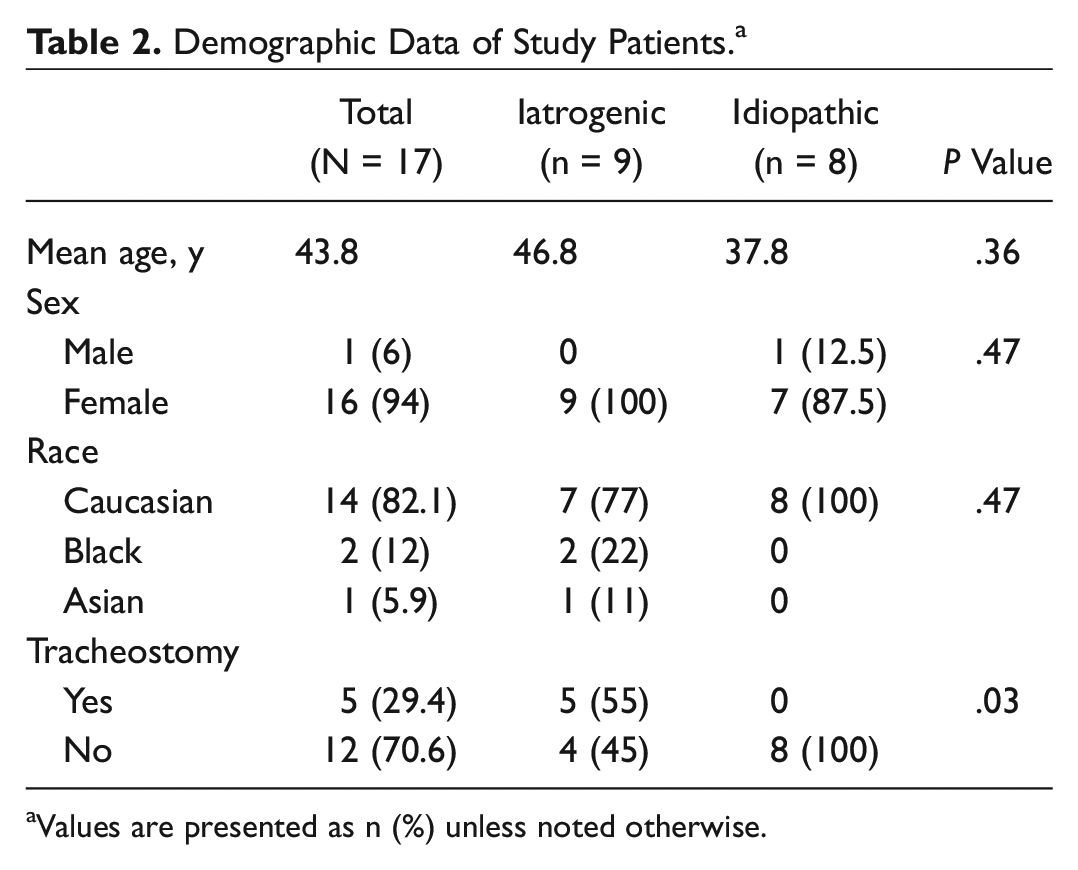
Values are presented as n (%) unless noted otherwise.
Coll1 Gene Expression Is Increased in Areas of LTS Scar
Endolaryngeal brush biopsy was successfully and safely obtained in all 17 patients undergoing operating room dilation without complication. Sufficient RNA quantity and quality was obtained for gene expression analysis in all samples. Quantification of RNA ranged from 10 to 100 μg/μL per sample. Analysis of brush biopsy samples for Coll1 gene expression revealed a 13.68-fold increase (N = 17, P < .001, 95% CI: 4.29-43.65) in LTS scar as compared with normal trachea ( Figure 1A ). There was no significant difference in Coll1 gene expression between the iSGS and iLTS subgroups. However, while both groups demonstrated increased Coll1 gene expression in LTS scar versus matched controls, statistical significance was demonstrated in only the iSGS subgroup (n = 8, P = .001, 95% CI: 6.72-157.91; Figure 2A ).
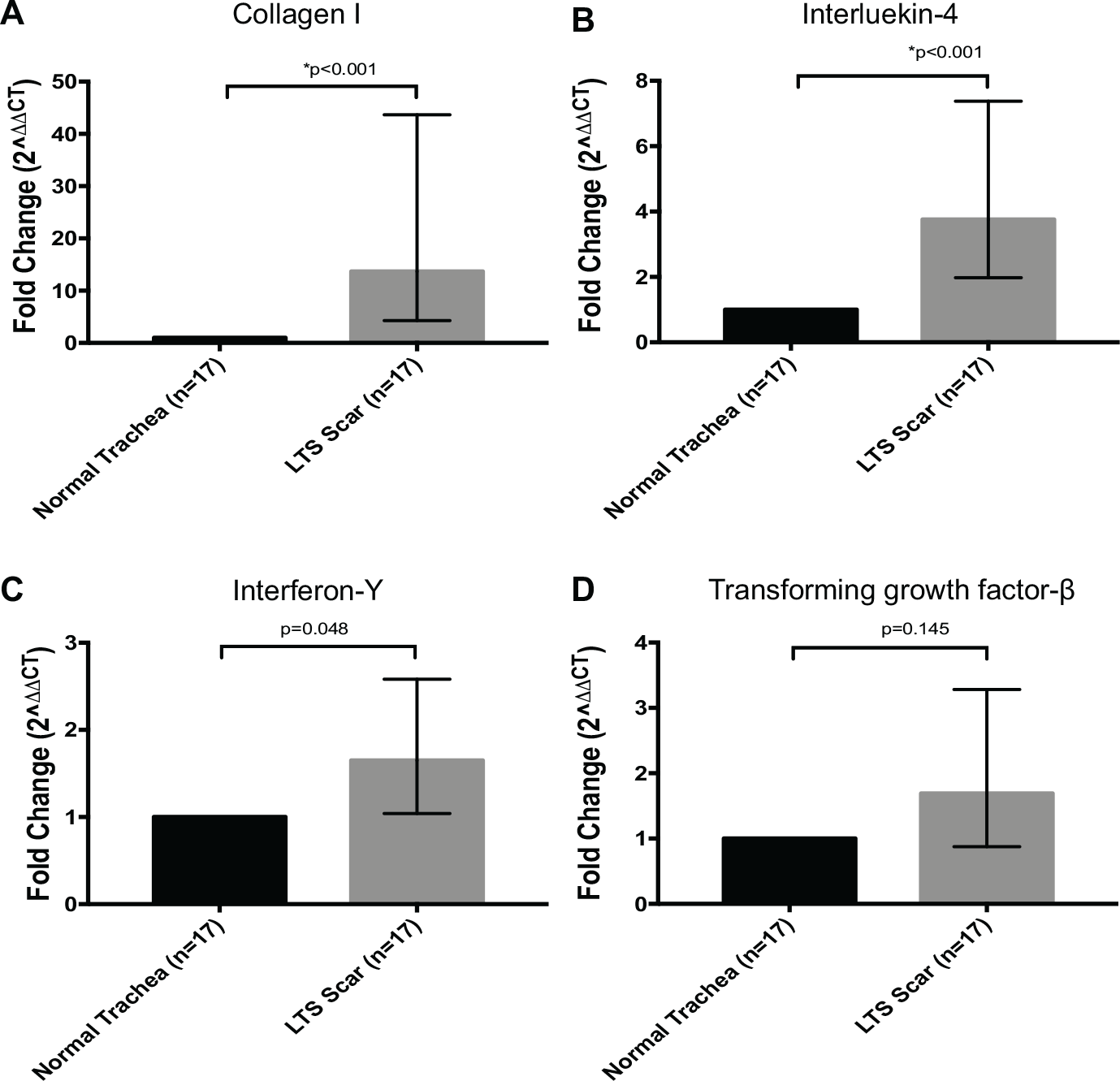
Immune and fibrosis-related gene expression in endolaryngeal laryngotracheal stenosis (LTS) brush biopsy samples. Expression profiles of immune and fibrosis-related genes in LTS scar and normal-appearing airway for 17 LTS patients: A, collagen 1; B, interleukin 4; C, interferon γ; D, transforming growth factor β. Error bars represent 95% CI. *P < .05.
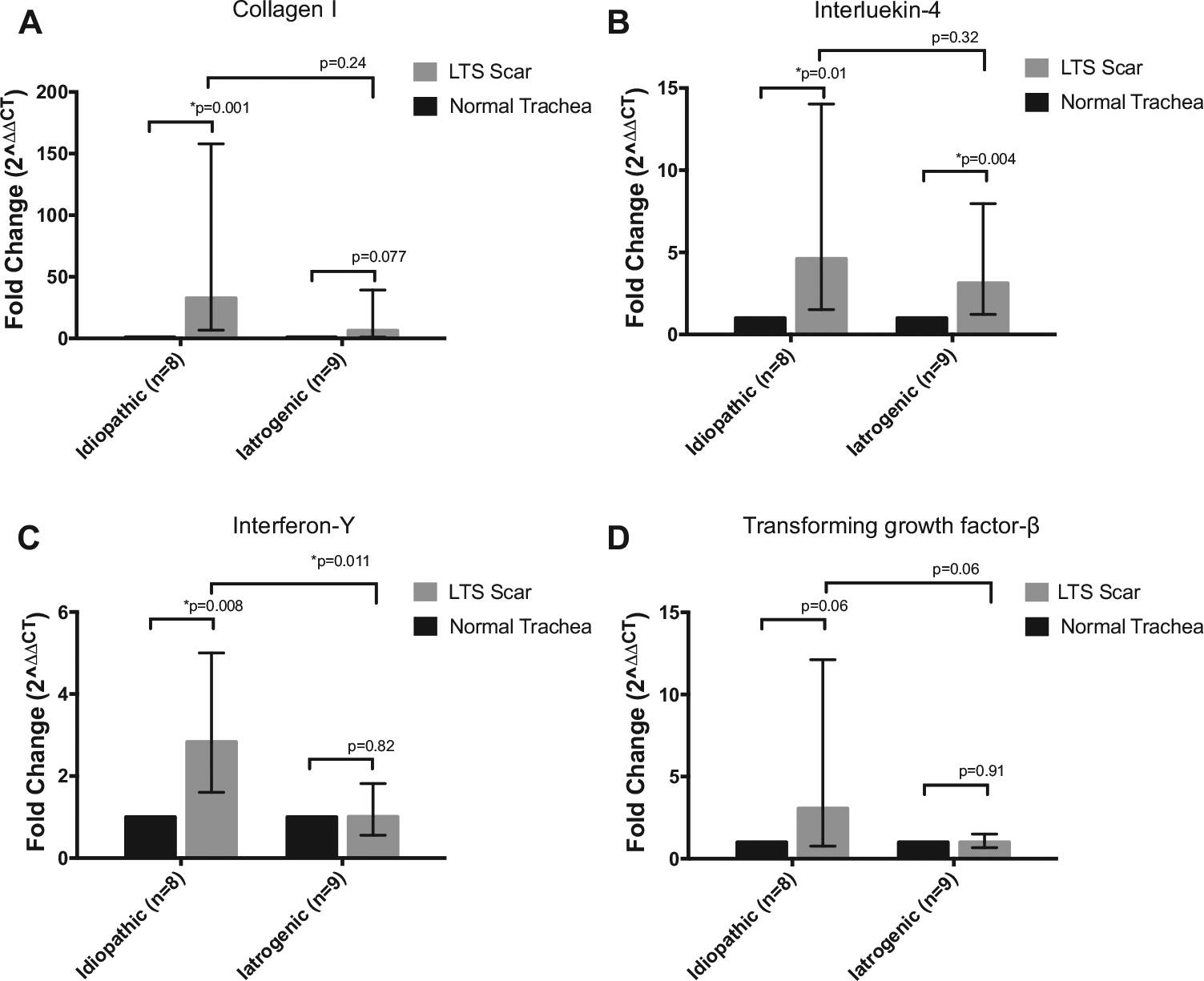
Immune and fibrosis-related gene expression in idiopathic subglottic stenosis and iatrogenic laryngotracheal stenosis (LTS) endolaryngeal brush biopsy samples. Expression profiles of immune and fibrosis related genes from LTS scar and normal appearing airway in idiopathic subglottic stenosis and iatrogenic LTS: A, collagen 1; B, interleukin 4; C, interferon γ; D, transforming growth factor β. Error bars represent 95% CI. *P < .05.
IL-4 Expression Is Increased in Areas of LTS Scar
Gene expression analysis of CD4+ T-cell-related cytokines revealed an upregulation of key cytokines. In this series of patients, the TH2-related cytokine IL-4 had a 3.76-fold increase in gene expression (N = 17, P < .001, 95% CI: 1.97-7.38) in terms of the entire population ( Figure 1B ). When stratified into iSGS and iLTS subgroups, IL-4 expression in each group remained significantly elevated when compared with matched normal controls. There was no difference in IL-4 expression between the iSGS group (fold change = 4.61, n = 8, 95% CI: 1.51-14.02) and iLTS group (fold change = 3.12, n = 9, 95% CI: 1.22-7.96; Figure 2B ), reported as average fold change against matched normal controls.
INF-γ Expression Is Increased in Areas of Idiopathic LTS Scar
Analysis of the TH1-related cytokine INF-γ revealed a nonsignificant increase in LTS specimens as compared with matched normal controls (fold change: 1.57, N = 17, 95% CI: 1.04-2.58, P = .048; Figure 1C ). However, the iSGS group demonstrated a significant elevation in INF-γ gene expression against matched normal controls (fold change = 2.83, n = 8, 95% CI: 1.60-5.00,). Furthermore, INF-γ expression in the iSGS samples was significantly higher than iLTS samples (fold change = 0.948, n = 9, 95% CI: 0.56-1.82, P = .011; Figure 2C ). There was no significant difference in INF-γ expression in iLTS samples versus matched normal controls (P = .82). Gene expression analysis of the profibrotic cytokine transforming growth factor β did not result in a significant difference between groups as well as against matched controls ( Figures 1D and 2D ).
Protein Quantification and Flow Cytometric Assessment of Cytokines
Based on the technique described, protein was extracted and purified from brush biopsy samples. Protein concentrations ranged from 3.87 to 43.89 mg/mL per sample. However, measurement of the TH1- and TH2-related cytokines IL-2, IL-4, IL-6, IL-10, tumor necrosis factor α, and INF-γ with flow cytometry revealed that cytokines in the protein extracted from the brush biopsy were below detectable levels and thus not quantifiable.
Discussion
In this study, we demonstrate a novel method for endolaryngeal sampling of the epithelial and subepithelial immune microenvironment in LTS. Based on this method, the changes in gene expression of immunologic markers in LTS tissue can be quantified in a minimally invasive fashion. Given that LTS is chronic fibroinflammatory disorder, characterization of the molecular and immunologic changes that potentiate this disease process is vital to improved understanding of its pathogenesis and has the potential to improve treatment strategies for LTS. Additionally, correlation of changes in key markers of inflammations in LTS to disease status could lead to the identification of a novel biopredictive marker capable of influencing treatment decisions.
The endolaryngeal brush biopsy technique described in this study was able to consistently obtain adequate genetic material for PCR analysis. Based on this technique, all samples from LTS scar and normal-appearing trachea had adequate RNA for the creation of complementary DNA for PCR analysis. Given that LTS is a disease hallmarked by increased collagen deposition, the robust increase in Coll1 gene expression in the LTS samples, as compared with normal controls, serves as validation that our method is accurately capturing diseased and normal trachea. Additionally, when the overall cohort was stratified into idiopathic and iatrogenic subgroups, albeit nonsignificant, the iatrogenic subgroup had lower levels of Coll1 gene expression versus the idiopathic group and did not meet significance when compared with matched normal controls. These trends may reflect that iLTS is a less active process at the time of operative dilation, while iSGS continues to have ongoing inflammation and fibroblast activation. However, further investigation is needed to confirm these findings.
When the gene expression of T-cell-related cytokines of interest was analyzed, this study’s cohort revealed a significant increase in IL-4 expression in LTS scar versus normal controls ( Figure 1B ), and these differences were maintained in both subgroups upon stratification ( Figure 2B ). Given that IL-4 is a secreted cytokine with a range of function—including immunosuppression, TH2 T-cell and M2 macrophage differentiation, and chronic fibrosis—this result was an anticipated finding.9,10 The association of IL-4 with multiple fibroproliferative diseases, such as idiopathic pulmonary fibrosis, cardiac fibrosis, and systemic sclerosis, has prompted investigations to identify its role in fibrosis.11-13 In idiopathic pulmonary fibrosis, disease progression is associated with persistent IL-4 elevation. 14 Additionally, in vitro models have demonstrated the ability of IL-4 to regulate fibroblast function, including promoting myofibroblast differentiation, collagen deposition, and proliferation. 15 However, in vivo models investigating the effects of IL-4 in fibrosis have not been transparent. IL-4 has a demonstrated critical anti-inflammatory role that promotes survival after initial injury in bleomycin-induced models of idiopathic pulmonary fibrosis but conversely potentiates the long-term deposition collagen that hallmarks disease progression. 10 While the exact role of IL-4 in fibrosis remains to be fully elucidated, its increase expression in LTS tissue in this study indicates that a similar immunologic mechanism between LTS and other fibroproliferative diseases may exist, but further investigation is needed.
Recent evidence investigating different etiologies of LTS suggests key differences in the pathogenesis of iSGS and iLTS. In iSGS, the IL-23/IL-17A signaling axis has been demonstrated to be upregulated when compared with iLTS, which suggests differences in the pathogenesis of this disease as it relates to the immune response. 16 The differences in INF-γ expression between the 2 subgroups of LTS in this study further supports that different underlying immunologic mechanisms in iSGS and iLTS exist. In the current study, when samples were stratified into idiopathic and iatrogenic subgroups, gene expression of INF-γ was significantly elevated in the iSGS group. While the source of this increased INF-γ expression cannot be determined, gamma-delta T cells (which have been shown to be increased in iSGS) are potent producers of INF-γ and may explain this observed increase.16,17 Another potential explanation for the increase in INF-γ expression in iSGS is the propensity for bacterial colonization by Mycobacterium species in iSGS. 8 Previous studies have demonstrated that Mycobacterium antigenicity invokes a robust release of INF-γ from T cells, natural killer cells, and macrophages.18,19 Like IL-4, the role of this increased INF-γ expression in iSGS is also unclear. Interestingly, INF-γ has been thought to be an antifibrotic cytokine that is deficient in many fibroproliferative diseases; thus, increasing INF-γ has been a strategy behind many interventions aimed at reducing fibrosis.20 -23 This seemly contradictory finding in iSGS necessitates further studies to define the role of INF-γ in iSGS.
The use of the novel brush biopsy technique introduced in this study offers a facile approach for immunologic sampling in LTS that minimizes the trauma associated with conventional biopsies and has potential for office-based application through the working channel port of a bronchoscope. Currently, molecular and immunologic assessment of LTS is restricted by the ability to obtain samples only at the time of operating room–based intervention, a point that does not likely capture the key molecular and inflammatory changes that potentiate restenosis in the weeks following intervention. Given the potential of this novel technique to be used during office-based bronchoscopy, temporal assessment of inflammation in the period following intervention is possible. Additionally, as increased data are obtained, correlation to clinical data (eg, dilation interval and tracheostomy dependence) has the potential reveal a biopredictive marker capable of prognostic or diagnostic use. For example, in our cohort, we identified a male patient with iSGS due to negative autoimmune serology and no history of intubation. Cases of iSGS among male patients are unusual, given that iSGS is a nearly uniform group composed of middle-age Caucasian females. Interestingly, this individual’s brush biopsy cytokine profile did not reveal a robust increase in INF-γ gene expression, as was observed in the rest of this cohort and which potentially indicates a different disease status for this patient. While this is solely speculation at this point and further testing is needed to interrogate the role of INF-γ as a biomarker for iSGS, it does reinforce that diagnose is not always clear in LTS and that there is a need for ancillary testing that can aide in diagnosis.
While the gene expression of many key cytokines and immunologic markers can be assessed with this minimally invasive brush biopsy technique, its does have limitations. This technique currently does not allow for accurate quantification of secreted cytokines or other proteins. The importance of reliable quantification of soluble cytokines confirms gene expression data and provides comprehensive insight into how changes in immune signaling affect the microenvironment of LTS scar. A potential alternative technique for endolaryngeal cytokine sampling is the use of gel foam sponges to collect surface secretions in the area of disease.24,25 While this established endolaryngeal technique is applicable to LTS, it is not applicable to an office-based setting, and secretion analysis reflects only surface cytokines and does not garner insight into the immune response in the subepithelial layers. Additionally, it should be recognized that the data generated in this study are based on a relatively small sample size with large confidence intervals that indicated wide variability among patients. To increase the reliability of the data presented, continued investigation of a larger cohort is needed to confirm these preliminary findings. Moreover, the inclusion of an additional control group of patients without LTS would be beneficial. Given this, continued optimization of our endolaryngeal sampling method to allow for quantification of soluble cytokines, as well as testing in a larger cohort, is needed to further improve our understanding of the inflammatory changes underlying this disease.
Conclusions
Endolaryngeal brush biopsy is a minimally traumatic and feasible approach for assessing gene expression of the immune microenvironment in LTS. This office-based method could allow for temporal assessment of inflammation in LTS and lead to identification of a novel biomarker capable of determining disease severity and prognostication. An improved method for measurement of secreted cytokines is needed, as it would improve the reliability of this sampling method. The data from this study indicate increased expression of IL-4 in idiopathic and iLTS samples and increased expression of INF-γ in idiopathic LTS samples. The difference in the expression of INF-γ between iSGS and iLTS further promotes the idea that different underlying mechanisms influence these histologically similar diseases. Additionally, INF-γ could represent a potential biomarker for iSGS, but these results need to be confirmed at the protein level, with continued investigation needed into the role of these cytokines.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the 2016 AAO-HNSF Annual Meeting & OTO EXPO; September 18-21, 2016; San Diego, California.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.