
Abstract
Objective
Options for management of unilateral hearing loss (UHL) in children include conventional hearing aids, bone-conduction hearing devices, contralateral routing of signal (CROS) aids, and frequency-modulating (FM) systems. The objective of this study was to systematically review the current literature to characterize auditory outcomes of hearing rehabilitation options in UHL.
Data Sources
PubMed, EMBASE, Medline, CINAHL, and Cochrane Library were searched from inception to January 2016. Manual searches of bibliographies were also performed.
Review Methods
Studies analyzing auditory outcomes of hearing amplification in children with UHL were included. Outcome measures included functional and objective auditory results. Two independent reviewers evaluated each abstract and article.
Results
Of the 249 articles identified, 12 met inclusion criteria. Seven articles solely focused on outcomes with bone-conduction hearing devices. Outcomes favored improved pure-tone averages, speech recognition thresholds, and sound localization in implanted patients. Five studies focused on FM systems, conventional hearing aids, or CROS hearing aids. Limited data are available but suggest a trend toward improvement in speech perception with hearing aids. FM systems were shown to have the most benefit for speech recognition in noise. Studies evaluating CROS hearing aids demonstrated variable outcomes.
Conclusions
Data evaluating functional and objective auditory measures following hearing amplification in children with UHL are limited. Most studies do suggest improvement in speech perception, speech recognition in noise, and sound localization with a hearing rehabilitation device.
The prevalence of unilateral hearing loss (UHL) in school-aged children ranges from 3% to 6%, depending on the audiologic criteria used to define hearing loss. 1 In the past, it was believed that speech and language development in these children would be unaffected given the presence of 1 normal-hearing ear. However, it has since been shown that this population is at risk for educational problems, with an increased rate of failing a grade, need for additional assistance in the classroom, and perceived behavioral issues.2,3 This may be partly due to children facing difficulty with hearing in noisy classrooms, an environment in which UHL has been shown to especially cause listening problems. 4
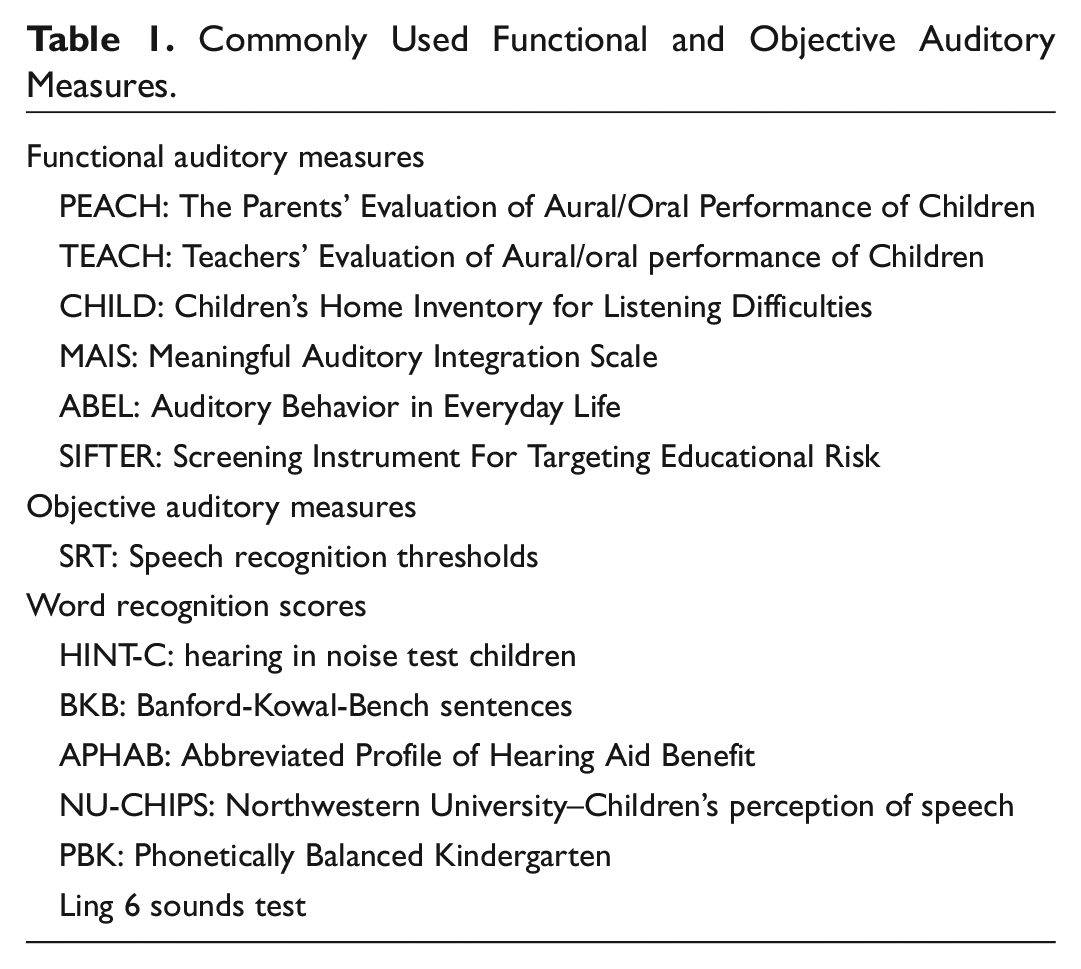
Currently, there is no consensus on what degree of UHL in children should be amplified, what method of amplification should be used, or what method is most efficacious. 5 Options for management of UHL in children include conventional hearing aids, bone-conduction hearing devices, contralateral routing of signal (CROS) aids, and frequency-modulating (FM) systems. There are various auditory outcome measures used to demonstrate benefit from hearing amplification ( Table 1 ). 6 Examples of commonly used objective measures, usually performed by audiologists, include pure-tone average, speech recognition thresholds, and word recognition scores. Functional measures evaluate more subjective outcomes; these include validated questionnaires or screening tools usually completed by parents, teachers, and children.
Commonly Used Functional and Objective Auditory Measures.
This study aimed to systematically review the current literature to characterize both objective and functional auditory outcomes of hearing rehabilitation in UHL. Specifically, we hypothesized that hearing amplification would result in an improvement in both objective and functional auditory outcomes in children with UHL.
Methods
Study Identification
A search of the PubMed, EMBASE, Medline, CINAHL, and Cochrane Library databases was completed by a medical librarian from inception until January 4, 2016. The search was limited to English language and human subjects and excluded case reports. First, studies describing UHL were identified using the following medical subject headings (MeSH) terms: “unilateral or asymmetric or single-side or one-side (loss or impairment or deafness).” Next MeSH terms that identified objective or functional auditory measures were used to obtain all the articles for a second group. Lastly, only articles describing the pediatric population were identified by using MeSH terms “child or adolescent or pediatric or paediatric or young or infant or newborn or neonatal or preschool or pre-school.” All 3 groups of articles were then cross-referenced. Search terms were adjusted for each database. References of the identified studies were reviewed to locate additional studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) recommendations were used in this review. 7
Eligibility Criteria and Study Selection
Two authors independently completed title and abstract reviews to identify articles of potential interest that met inclusion criteria. Full articles were obtained for the list of abstracts of potential interest and reviewed independently. The lists were then compared, and any conflicts were reconciled after discussion to compose a final list of studies to be included ( Figure 1 ).
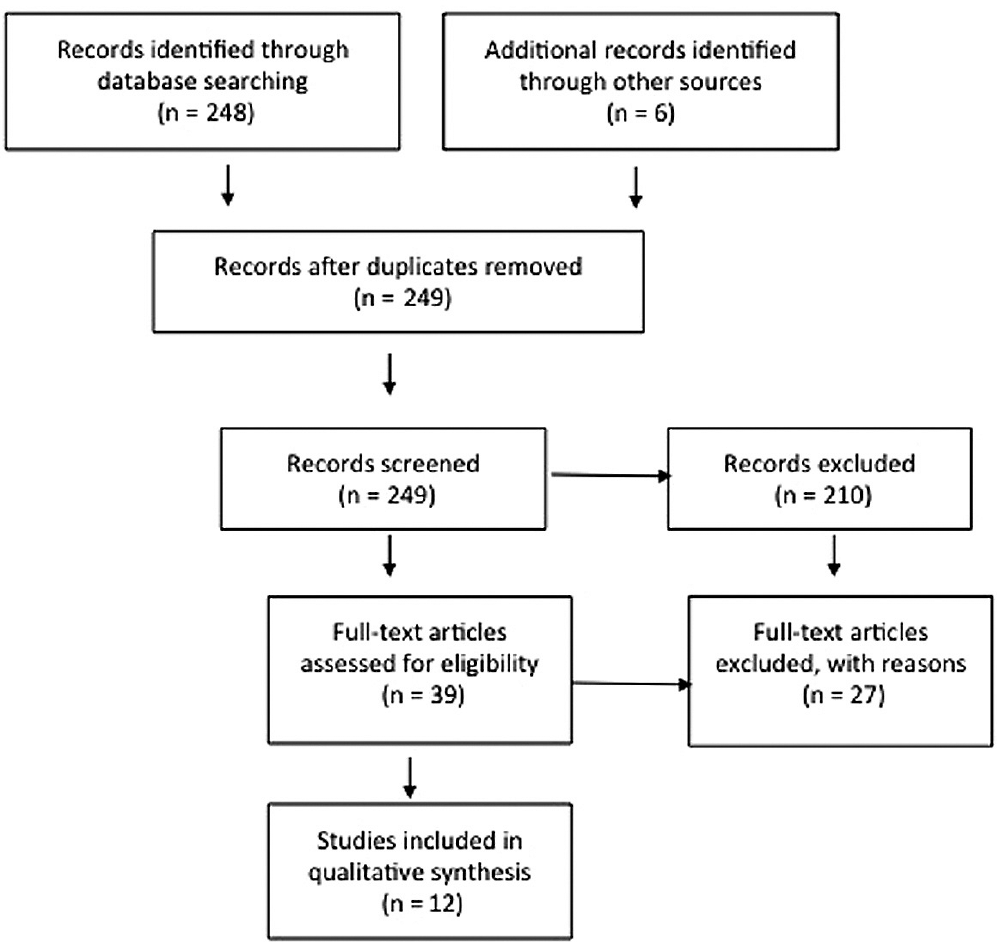
Flow diagram of the literature search based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) recommendations.
Data Extraction
Two authors independently performed data extraction. Data were compared for any conflicts and were reconciled after discussion. Data extracted included degree of hearing loss, measures of auditory outcomes, type of hearing rehabilitation method used, and overall conclusions regarding impact of hearing rehabilitation for UHL on auditory outcomes. Data were grouped by type of hearing rehabilitation method used. Because of the heterogeneity of the data found in the identified studies, a meta-analysis could not be completed.
Evaluation of Risk of Bias
The Newcastle-Ottawa scale is an accepted tool to assess the quality of nonrandomized studies reviewed in systematic reviews. The scale has been developed in collaboration with the University of Newcastle and University of Ottawa; it has been tested and validated in systematic reviews. The Newcastle-Ottawa scale was used to assess the selected studies for risk of bias. 8 The scale uses 3 perspectives: patient and control selection (selection), comparability of cases and controls (comparability), and ascertainment of exposure (exposure). Each study is awarded a maximum of 4 stars for selection, 2 stars for comparability, and 3 stars for exposure or outcome, for a maximum of 9 stars. A study is considered to be at a lower risk of bias with a high number of stars awarded.
Results
A total of 249 studies were initially identified. Following identification of additional records through reference review, 254 total studies were identified. After duplicates were removed, 249 studies remained for analysis. Of the studies, 144 were initially excluded from further analysis based on title review, resulting in 105 studies for abstract review ( Figure 1 ). After abstract review, an additional 66 studies were excluded, leaving 39 studies for full-text review. Twenty-seven of the remaining 39 studies were excluded after manuscript review. The remaining 12 studies were included for data abstraction ( Figure 1 ; Table 2 ).
General Characteristics and Demographic Data of Included Studies.
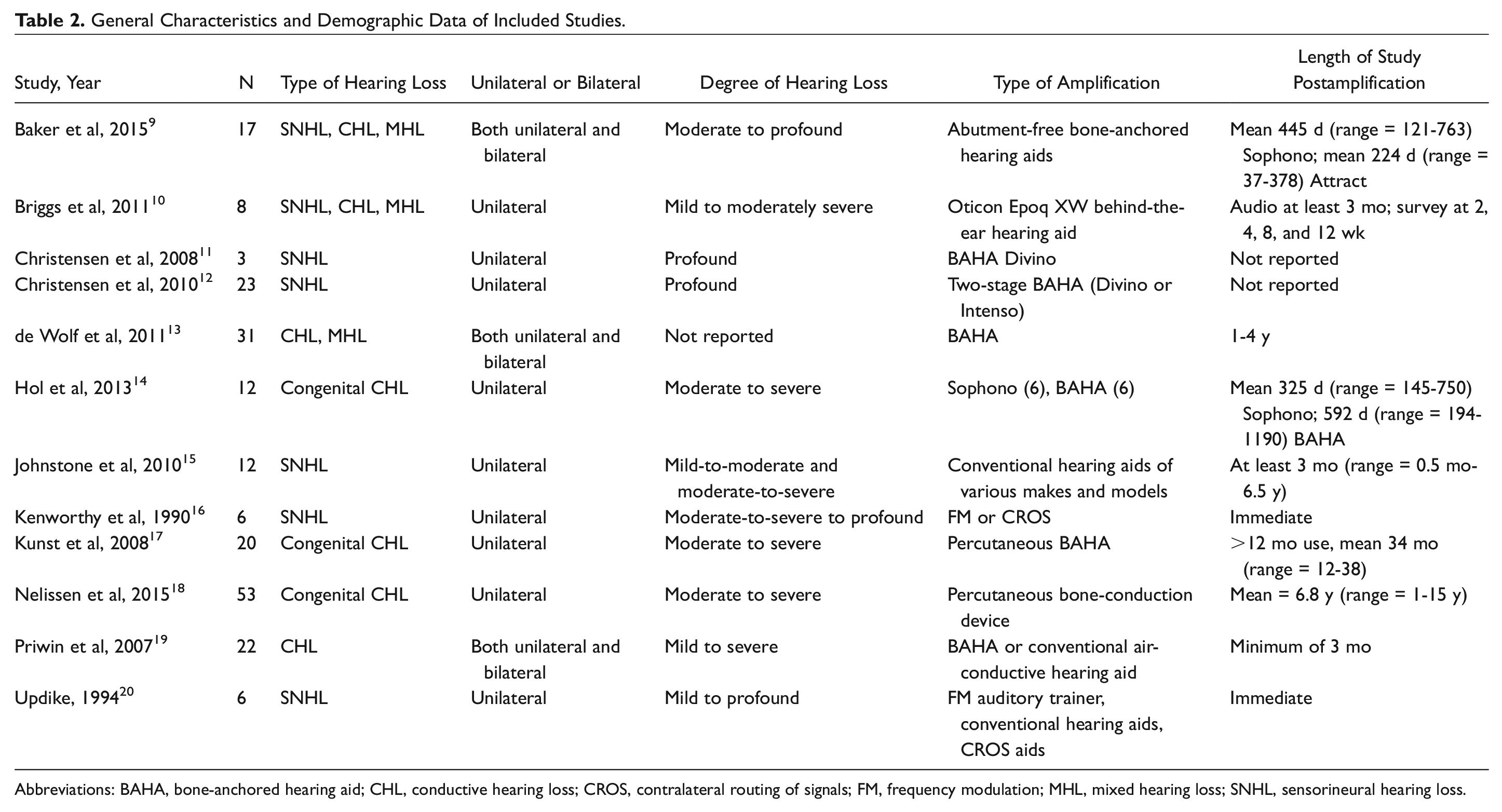
Abbreviations: BAHA, bone-anchored hearing aid; CHL, conductive hearing loss; CROS, contralateral routing of signals; FM, frequency modulation; MHL, mixed hearing loss; SNHL, sensorineural hearing loss.
Outcomes for Surgically Implanted Hearing Aids
Seven studies evaluated the outcomes following surgical implantation of bone-conduction hearing devices in 128 patients, including BAHA and Sophono ( Table 3 ).9,11-14,17,18 All studies had an objective audiologic measure as an outcome, including pure-tone average, speech recognition threshold, and hearing in noise test scores. All of these studies demonstrated benefit of implantable hearing aids. The study by de Wolf et al 13 measured only objective outcomes, and these authors also concur that bone-anchored aids can be beneficial for children with UHL. These authors, however, suggest a more guarded approach to decision regarding surgical implantation and recommend a headband trial first. 13
Outcomes for Surgically Implanted Hearing Aids.
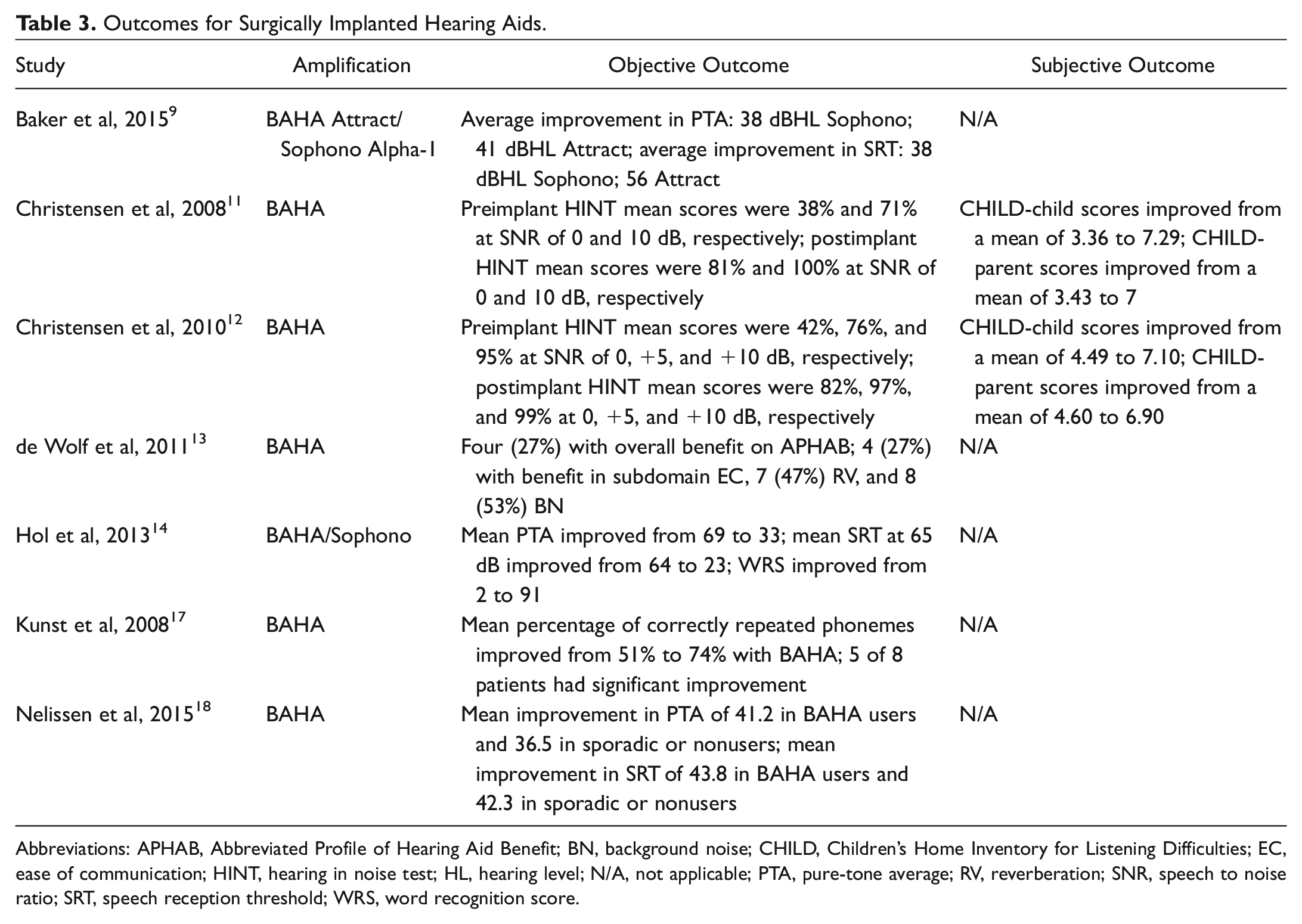
Abbreviations: APHAB, Abbreviated Profile of Hearing Aid Benefit; BN, background noise; CHILD, Children’s Home Inventory for Listening Difficulties; EC, ease of communication; HINT, hearing in noise test; HL, hearing level; N/A, not applicable; PTA, pure-tone average; RV, reverberation; SNR, speech to noise ratio; SRT, speech reception threshold; WRS, word recognition score.
Two of 7 studies had a functional measure as an outcome, including Children’s Home Inventory for Listening Difficulties (CHILD) scores.11,12 These studies also demonstrated benefit of implantable hearing aids.
One study demonstrated a difference in outcomes for congenital versus acquired hearing loss. 17 In the 2 studies that compared BAHA to Sophono, implantation of either device resulted in objective improvement, but in both studies, the BAHA had a greater audiologic benefit than the Sophono.9,14
Outcomes for Nonsurgical Intervention
Five studies evaluated the impact of nonsurgical intervention in UHL in 32 patients, including use of an FM system, a conventional hearing aid, and a CROS hearing aid ( Table 4 ).10,15,16,19,20 All 5 studies used objective outcome measures, including Bamford-Kowal-Bench scores, audiometry, and sound localization scores. Functional measures were used for the outcome in only 1 study. 10
Outcomes for Nonsurgical Intervention.
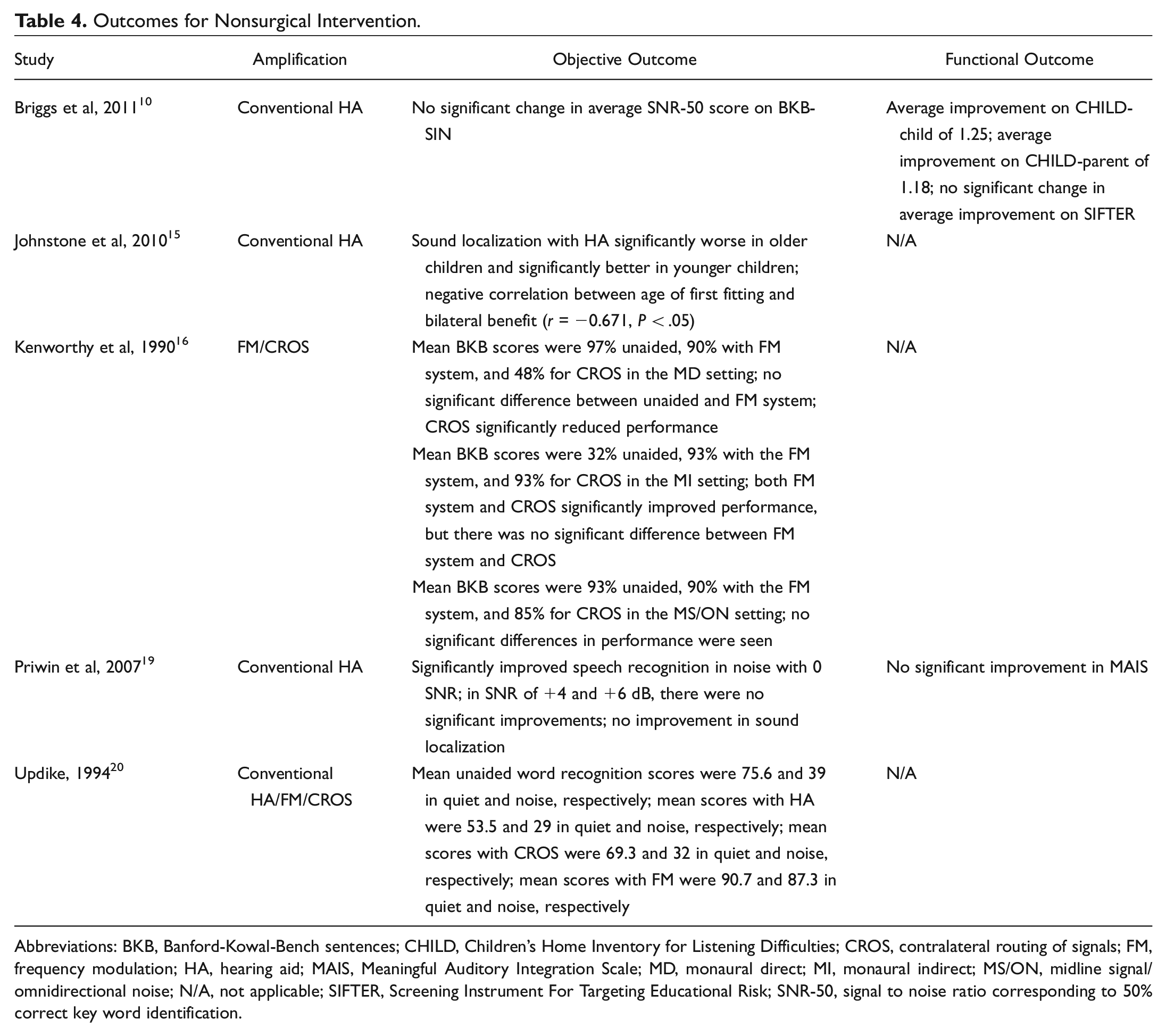
Abbreviations: BKB, Banford-Kowal-Bench sentences; CHILD, Children’s Home Inventory for Listening Difficulties; CROS, contralateral routing of signals; FM, frequency modulation; HA, hearing aid; MAIS, Meaningful Auditory Integration Scale; MD, monaural direct; MI, monaural indirect; MS/ON, midline signal/omnidirectional noise; N/A, not applicable; SIFTER, Screening Instrument For Targeting Educational Risk; SNR-50, signal to noise ratio corresponding to 50% correct key word identification.
Briggs et al 10 examined both functional and objective outcomes in mild to moderately severe hearing loss with conventional hearing aids and concluded that there was no significant benefit or harm to hearing aids. However, the study did note a significant improvement in the CHILD score, a functional outcome measure, with amplification. CHILD is a questionnaire to measure communication needs specifically in the home environment. Two other studies examining hearing aids did find improvement in objective outcomes following amplification, specifically hearing in noise and sound localization.15,19 One study demonstrated a negative correlation between age of hearing aid fitting and bilateral benefit (r = −0.671, P < .05), indicating that earlier fitting led to improved outcomes. 15
Two studies focused on CROS hearing aids and FM systems.16,20 Updike 20 found CROS hearing aids to be detrimental, with worsened scores on objective auditory outcomes, especially in noisy environments. Kenworthy et al 16 found CROS to be helpful with objective outcomes only in specific classroom settings. The 2 studies involving the FM system as an intervention demonstrated benefit of FM system on objective measures.16,20
Assessment of Risk of Bias
Overall, the studies ranged from as low as 2 stars up to 8 stars, with an average of 4.9 stars. Only 1 study rated at 8 stars; most were 6 stars (5studies). These results would suggest moderate risk of bias overall with the reviewed studies. This risk of bias assessment is not surprising considering that there were no randomized studies and a relative lack of comparison studies. In addition, prospective studies had very small patient cohorts ( Table 5 ).
Assessment of Risk of Bias Using the Newcastle-Ottawa Scale. a
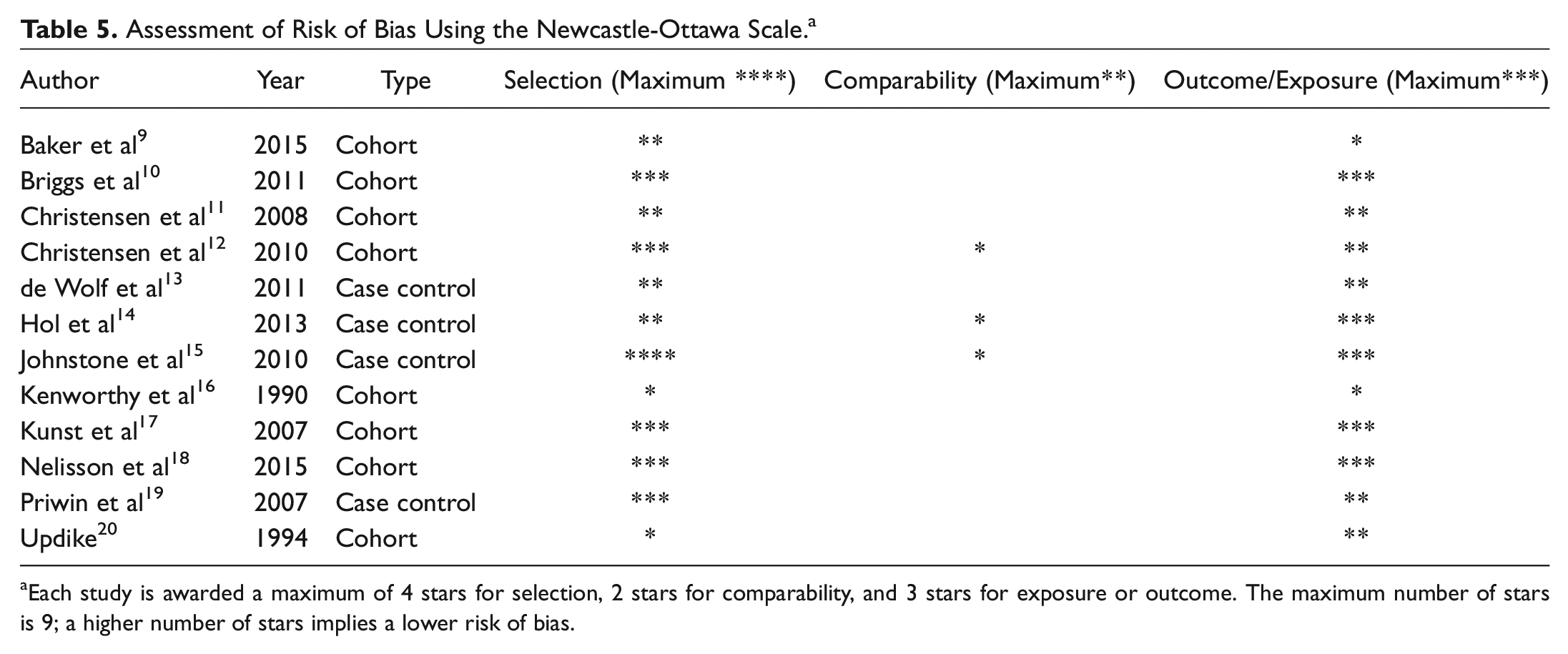
Each study is awarded a maximum of 4 stars for selection, 2 stars for comparability, and 3 stars for exposure or outcome. The maximum number of stars is 9; a higher number of stars implies a lower risk of bias.
Discussion
Both objective and functional auditory outcomes measures play a role in measuring the efficacy of hearing amplification devices ( Table 1 ). In this systematic review, 12 studies were reviewed that examined either functional or objective auditory outcomes following hearing rehabilitation in children with UHL.
Bone-conduction hearing devices were the most commonly studied hearing rehabilitation device, with 7 studies focusing on this method.9,11-14,17,18 Overall, all the studies demonstrated that bone-conduction hearing devices either showed improved or significantly improved objective and/or functional outcomes in UHL. Current Food and Drug Administration criteria for bone-conduction hearing devices implantation in children are age greater than 5 with single-sided deafness or unilateral conductive or mixed hearing loss unable to be aided by conventional hearing aids. Most of the studies in this systematic review performed the bone-conduction hearing devices in the setting of moderate to severe or profound UHL.
Considering the fact that these implants were most commonly performed in children with more severe UHL, it is not surprising that the studies reported benefit with this hearing rehabilitation method. These children with more severe UHL would suffer the most, because of increased difficulty with listening in educational or home settings, and in turn, they would benefit the most from correction of this disability. However, given that this is a surgical procedure, a preoperative trial with a soft-band device should be considered.
While bone-anchored aids are commonly used for severe to profound UHL, mild to moderate UHL is often treated with conventional hearing aids, CROS hearing aids, and/or FM systems. Of the nonsurgical hearing rehabilitation methods, conventional hearing aids seem to benefit children with mild to moderately severe hearing loss and should be considered for treatment in this setting. The benefits of CROS hearing aids are inconclusive. On the other hand, FM hearing systems clearly have shown to be beneficial and should be strongly considered in the classroom for children with UHL.
FM systems have historically been the conventional choice for children with mild to moderate UHL; interestingly, this recommendation is based on findings in 2 studies, with a total of 12 patients.16,20 The American Academy of Audiology protocol for amplification in children with mild to moderate UHL advocates for FM system use. The protocol, however, does not present a strongly supportive position on using conventional amplification with hearing aids; instead, the protocol suggests that it maybe indicated in some children based on preferences of child/family, audiological, developmental, communication, and educational factors. 21 In our review, the data are limited but do show benefit with conventional hearing aids even with these mild to moderate UHL patients. Further studies are clearly needed to evaluate the role of conventional hearing aids and FM systems in this subset of patients.
Interestingly, Johnstone et al 15 found a significant correlation between age at intervention and sound localization benefit; specifically, children who were fit earlier showed more benefit. This is similar to the finding by Kunst et al 17 showing improved outcomes with bone-conduction hearing devices in acquired UHL. Both of these studies lend support to the widely accepted notion that auditory deprivation can compromise auditory outcomes after hearing rehabilitation; therefore, early intervention may be crucial to attain optimal results. 22
This systematic review is limited by the lack of high-quality studies pertaining to this topic, with no randomized studies available for review and by small patient populations in many of the prospective studies reviewed. This limitation is highlighted in results of risk of bias assessment in which many of the studies were assessed to be either moderate to high risk for bias. It is particularly important to note the paucity of literature on outcomes for nonsurgical interventions for UHL. In addition, the auditory measures were not consistent across the studies reviewed. Future studies should attempt to measure and compare the same functional and objective auditory outcomes for all of the available devices for hearing rehabilitation. Attempting to stratify the best option for amplification by degree of hearing loss would also be of great utility.
Conclusions
Data evaluating functional and objective auditory outcomes following hearing amplification in children with UHL are limited. However, most of the studies reviewed suggest improvement in these measures with bone-conduction hearing devices in the setting of moderate to profound UHL. No conclusion can be drawn on the benefit of CROS hearing aids. In patients with mild to moderate UHL, FM systems seem to benefit children in the educational setting. Although evidence is limited, conventional hearing aids also seem to benefit these children, and further studies are needed to elucidate this benefit.
Author Contributions
Disclosures
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
This article was presented at the American Society of Pediatric Otolaryngology; May 2017; Austin, Texas.