
Abstract
Objective
To analyze rates, risk factors, and complications for 30-day readmission among head and neck cancer (HNC) patients.
Methods
Retrospective review of administrative records from Vizient (Irving, Texas) Clinical Data Base/Resource Manager on HNC patients who underwent a head and neck surgical procedure from January 2013 through September 2015 at 176 academic and community medical centers.
Results
Of the 18,121 patients included in the study, 2502 patients were readmitted within 30 days (13.8%). Mean time to readmission was 11 ± 8.2 days. Cancer of the hypopharynx, oropharynx, pharynx, and larynx all had higher odds of readmission compared to oral cavity (odds ratio [OR], 1.8, 1.7, 1.6, and 1.5; 95% confidence interval [CI], 1.4-2.2, 1.4-1.9, 1.2-2.3, and 1.3-1.7, respectively). Consistent with this, flap procedures and laryngectomy had the highest odds of readmission (OR, 1.4 and 1.3; 95% CI, 1.3-1.6 and 1.0-1.5 vs glossectomy, respectively). The most common surgical causes for readmission were postoperative infection (17.6%) and surgical wound dehiscence (16.8%), which most commonly presented on postdischarge days 4 to 5. Acute cardiac events occurred in up to 15.4% of patients depending on complexity of surgery. Dysphagia and electrolyte disturbances were common (15.8% and 15.4%, respectively); patients with these complications typically presented earlier, between days 3 and 4.
Discussion
Patients with HNC are at high risk of readmission. The cancer subsite and procedure significantly influenced the risk, rate, and reason for readmission.
Implications for Practice
Findings from this study can help quality improvement and patient safety administrators develop interventions that uniquely target HNC populations.
The Centers for Medicare & Medicaid Services (CMS) has identified 30-day readmission rates as an important measure of health care quality and an area to reduce health care costs. 1 The CMS defines readmission as “an admission to a subsection hospital within 30 days of discharge from the same or another subsection hospital.” As the methodology stands now, a hospital’s readmission performance is compared to the national average and adjusted for patient-level risk factors to calculate the hospital’s excess readmission ratio. The Hospital Readmissions Reduction Program, part of the Patient Protection and Affordable Care Act, has begun reducing payments to hospitals with excess readmissions. These penalties underscore the CMS’s continued effort to link hospital reimbursement to quality of patient care and provide financial incentive to intuitions that improve care coordination and postdischarge planning.
The CMS has begun expanding readmission measures to include not only medical but surgical measures as well.1,2 As the CMS continues to expand readmission measures, it is imperative for otolaryngologists to analyze readmissions among head and neck patients to identify benchmark standards to compare readmission measures to guide development of quality improvement measures, identify populations most at risk for unplanned readmissions, and elucidate the risk factors and common causes for readmission. 3
Prior studies have described the negative impact of readmission on postoperative quality of life, 4 mortality, 5 and cost.5,6 At academic centers, median costs from unplanned readmission for patients undergoing head and neck surgery have been reported to be $20,927 (range, $3201 to $178,122). 7 In this regard, improvements in 30-day readmissions can help reduce health care costs and improve postoperative patient care.
There is growing body of publications in recent years to help lay the groundwork for understanding 30-day unplanned readmissions among otolaryngology patients.6,8-16 However, most of these studies lack generalizability to patients with head and neck cancer (HNC) because they are single-institution reports6,9,10 or capture patients from multiple otolaryngology subspecialties,8,9,13 which include significant ambulatory procedures uncharacteristic of the HNC population. Prior studies have identified single-institution 12 and multicenter analysis of readmissions following free flap procedures for HNC patients. 11 Furthermore, laryngectomy patients, a subset of the HNC population, have already been identified as an at-risk population for 30-day unplanned readmission. 10 Therefore, the HNC population represents a unique subset of patients with respect to overall disease burden, critical illness, and postoperative care that necessitates independent analysis to best understand the risk factors and causes of readmissions and guide development of quality improvement measures.
This study aims to review and analyze nationwide, multi-institutional, 30-day unplanned readmissions in the HNC population. Even among patients with HNC, varying degrees of heterogeneity exist with respect to the location of the primary cancer site and its implications in the type and extent of surgical resection needed to eradicate disease. Therefore, mucosal tumors of the aerodigestive tract spanning proximally from the oral cavity and distally to the hypopharynx each pose a unique set of problems for the patient in terms of the types of complications they are likely to incur. Investigators set out to elucidate the rates and risk factors for readmission, identify the complications resulting in readmission, and characterize the time from discharge to readmission. Together, this report can be used to identify populations most at risk of readmission and where resources should be used to reduce unplanned 30-day readmissions.
Materials and Methods
Study Design
The study is a multicenter retrospective review of all patients with HNC who underwent a head and neck surgical procedure from January 2013 through September 2015. Data were abstracted from the Vizient Clinical Data Base/Resource Manager (formerly University HealthSystem Consortium). This database provides national administrative claims from over 120 medical centers and affiliated hospitals. The database collects information pertaining to the CMS core measures.17,18 Furthermore, the data set has been validated against key encounters and patient-specific variables, which makes it an appropriate database for use in this study. 19
Patient demographics (age, sex, race) and clinical variables (admission source, discharge location/disposition, admission date, discharge date, length of stay, days to readmission, days spent in the intensive care unit, deidentified institutional identification codes, and International Classification of Diseases, Ninth Revision [ICD-9] diagnoses and procedural codes pertaining to indexed and readmitted hospital admissions) were extracted from the clinical database for analysis and comparison. This study was approved by the Vanderbilt University School of Medicine Institutional Review Board (IRB 160339).
Inclusion Criteria
Patients were included in the study if they were (a) >18 years of age at the time of the indexed admission, (b) had an HNC ICD-9 diagnosis code (oral cavity, oropharynx, larynx, hypopharynx, or pharynx) on the index admission, and (c) had a head and neck surgery ICD-9 procedural code (flap procedure, glossectomy, laryngectomy, mandibulectomy, or pharyngectomy) on the indexed admission (Supplemental Table S1, available in the online version of the article). Patients were excluded if they died during the index admission.
Variables and Definitions
In this study, readmission refers to 30-day unplanned hospital readmission. ICD-9 codes from the indexed admission were used to determine primary cancer diagnosis, primary procedure, presence of various pretreatment variables (tracheostomy, gastrostomy, weight loss, dysphagia, and airway obstruction), and presence of various comorbidities (Supplemental Table S1, available in the online version of the article). ICD-9 codes from readmitted cases were then used to identify the postoperative complications. Complications were classified as “medical” or “surgical” as outlined in Supplemental Table S1 (available in the online version of the article). Because each patient could carry multiple cancer diagnoses or procedural codes, each patient was assigned to the single cancer diagnoses and procedure investigators felt carried the highest morbidity. For cancer diagnoses, designation in order of decreasing preference was determined by the authors to be larynx > hypopharynx > pharynx > oropharynx > oral cavity. For primary procedure, designation in order of decreasing preference was determined by the authors to be flap procedure > laryngectomy > mandibulectomy > pharyngectomy > glossectomy. A sensitivity analysis where patients were able to carry multiple cancer diagnoses and procedures was conducted to ensure validity of the above classifications.
Patients were classified as having a glossectomy if they carried an ICD-9 procedural code (ICD-9 PC) for either partial glossectomy (ICD-9 PC 25.2), complete glossectomy not otherwise specified (ICD-9 PC 25.3), and radical glossectomy (ICD-9 PC 25.4). Patients were classified as having a laryngectomy if they carried an ICD-9 PC for a hemilaryngectomy (ICD-9 PC 30.1), complete laryngectomy with thyroidectomy (ICD-9 PC 30.3), and total laryngectomy with radical neck dissection and thyroidotomy (ICD-9 PC 30.4) (Supplemental Table S1, available in the online version of the article).
Although the subsite of pharynx does not reflect use of traditional HNC subsite staging, ICD-9 diagnosis code 149 allows for a diagnosis to capture an “unspecified neoplasms of the pharynx, Waldeyer’s ring, and other ill-defined sites within the pharynx.” Investigators decided to include this subsite for consistency in how diagnoses are coded under ICD-9 and to be as inclusive and thorough given these constraints. Patients with cancer of the pharynx were not attempted to be categorized as having nasopharyngeal, oropharyngeal, or hypopharyngeal cancer due to possible misclassification.
Data Analysis
The primary outcome of interest was unplanned 30-day hospital readmission, defined as an admission to any service in the hospital within 30 days of discharge from the indexed admission. All statistical analysis was completed on Stata 14.0 software (StataCorp, College Station, Texas). Two-tailed t test was used to compare continuous variables between groups. The Pearson χ2 was used to compare categorical variables between groups.
Univariate (unadjusted) logistic regression was performed to identify predictors of readmission (Supplemental Table S2, available in the online version of the article). Variables significant at the .05 α level were then included in a multivariate regression model to estimate adjusted odds ratio (OR) and 95% confidence intervals (95% CIs) for 30-day readmission. All statistics were 2-tailed and considered statistically significant if P < .05.
Kernel density estimation (KDE) was used to determine frequency for the delay in days between discharge and readmission stratified by complications at readmission. The area under the curve estimates the probability of an individual experiencing readmission during a given time interval.
Results
Patient Demographics and Readmission Rates
A total of 18,121 patients were included in the study. The majority of the cohort was male (70.4%) and of white race (80.5%). Most patients had cancer of the oral cavity (62.1%), followed by the larynx (22.8%) and oropharynx (9.8%). Approximately one-third of patients had a flap procedure (37.1%), followed by glossectomy (31.0%), laryngectomy (13.9%), mandibulectomy (12.4%), and pharyngectomy (5.7%). Of the patients who met inclusion criteria, 8309 (45.9%) also received a neck dissection ( Table 1 ).
Demographics and Population Characteristics. a
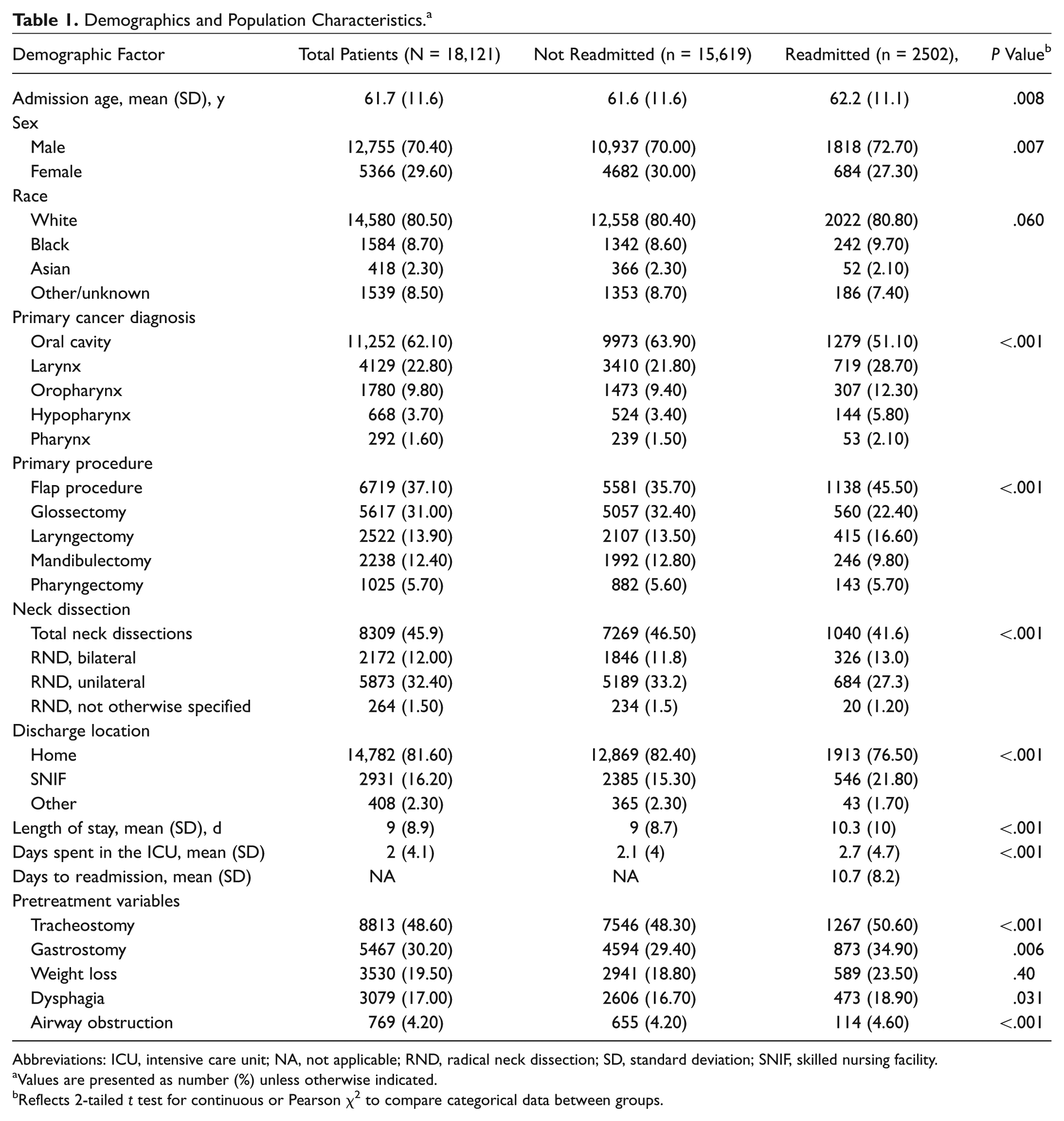
Abbreviations: ICU, intensive care unit; NA, not applicable; RND, radical neck dissection; SD, standard deviation; SNIF, skilled nursing facility.
Values are presented as number (%) unless otherwise indicated.
Reflects 2-tailed t test for continuous or Pearson χ2 to compare categorical data between groups.
A total of 2502 patients were readmitted within 30 days for an overall reported readmission rate of 13.8%. However, readmission rates varied by the cancer diagnosis and the procedure type. Patients who had cancer of the hypopharynx (21.6%) and pharynx (18.2%) had the highest rate of readmission. In addition, patients who underwent a flap procedure or a laryngectomy had the highest rates of readmission compared to other procedures (16.9% and 16.5%, respectively). Patients who had cancer of the oral cavity (11.4%) or had a glossectomy (10.0 %) had the lowest rate of readmission in each subgroup. Patients who underwent unilateral radical neck dissection were readmitted at 11.6% while those who underwent bilateral radical neck dissection were readmitted at 15.0%.
Readmission and Comorbidities
On multivariate regression analysis, patients who had cancer of the hypopharynx had the highest odds of 30-day readmission (OR, 1.8; 95% CI, 1.4-2.2), followed by the oropharynx (OR, 1.7; 95% CI, 1.4-1.9), pharynx (OR, 1.6; 95% CI, 1.2-2.3), and larynx (OR, 1.5; 95% CI, 1.3-1.7) vs those with cancer of the oral cavity. Compared to patients who had a glossectomy, those with a flap procedure (OR, 1.4; 95% CI, 1.3-1.6) and laryngectomy (OR, 1.3; 95% CI, 1.0-1.5) had the highest odds of readmission. Discharge to a skilled nursing facility (OR, 1.3, 95% CI, 1.1-1.4) was associated with a higher likelihood of readmission compared to those discharged home. Unilateral radical neck dissection was found to be protective against readmission vs those who did not undergo radical neck dissection (OR, 0.75; 95% CI, 0.7-0.8) on univariate analysis. However, neither unilateral nor bilateral radical neck dissection were found to significantly increase or decrease odds of readmission on multivariate analysis ( Table 2 ).
Adjusted Odds Ratio of All-Cause 30 Day-Readmission among Head and Neck Cancer Patients following Surgery. a
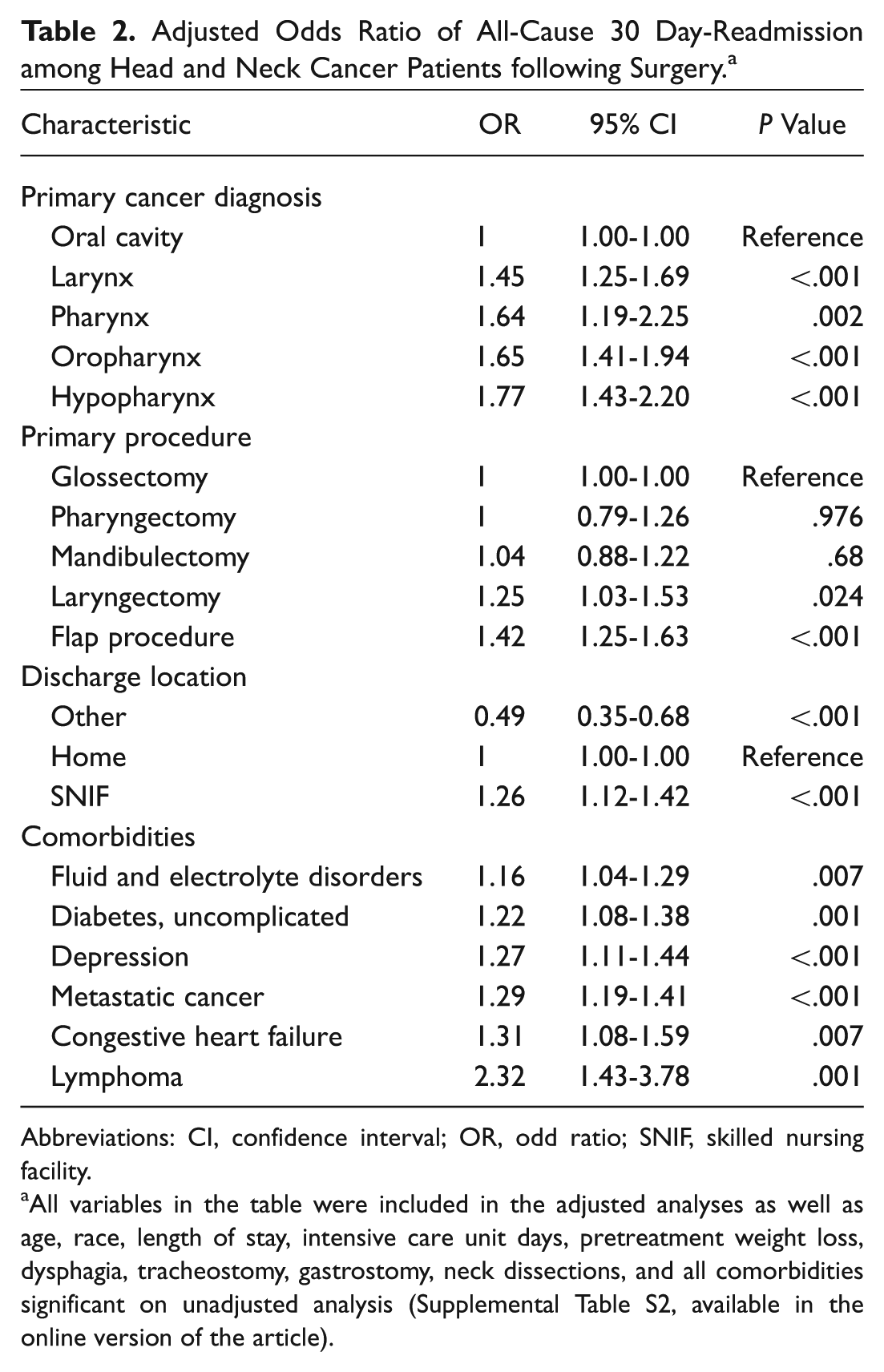
Abbreviations: CI, confidence interval; OR, odd ratio; SNIF, skilled nursing facility.
All variables in the table were included in the adjusted analyses as well as age, race, length of stay, intensive care unit days, pretreatment weight loss, dysphagia, tracheostomy, gastrostomy, neck dissections, and all comorbidities significant on unadjusted analysis (Supplemental Table S2, available in the online version of the article).
Of the 31 different comorbidities initially evaluated for risk of readmission, 6 were found to significantly predict readmission after adjusted multivariate analysis. Congestive heart failure, uncomplicated diabetes, lymphoma, metastatic cancer, fluid/electrolyte disorders, and depression were all significantly associated with increased likelihood of readmission. Neither age, sex, race, length of stay (LOS) >5 days, intensive care unit (ICU) days >7 days, nor any of the pretreatment variables were found to significantly affect risk of readmission within 30 days ( Table 2 ).
We determined order of cancer site and surgical procedure preference by review of prior literature, which demonstrated that patients who underwent flap procedure and/or a laryngectomy to be at high risk of readmission, whereas patients who had undergone glossectomy were at a lower risk. With respect to mandibulectomy, of the 2238 patients who carried a mandibulectomy code, only 24 patients (1.1%) also carried a laryngectomy. Thus, we felt that giving preference to laryngectomy over mandibulectomy would not significantly affect findings. A sensitivity analysis where patients were able to carry multiple cancer sites and procedural codes demonstrated similar findings to those presented above and validated our methods (Supplemental Table S3, available in the online version of the article).
Reasons for Readmission
The most common complications on readmission were evaluated and stratified by type of procedure and the location of the patient’s cancer. Overall, postoperative infection was the most common reason for readmission (17.6%), followed by surgical wound dehiscence (16.8%), dysphagia (15.8%), fluid/electrolyte abnormalities (15.4%), and acute cardiac event (13.3%). The most common surgical causes of readmission were found to be postoperative infection, wound dehiscence, postoperative fistula, hemorrhage, hematoma or seroma, and tracheostomy complications. The most common medical causes of readmission were dysphagia; fluid, electrolyte, and acid-base disturbances; acute cardiac events; pneumonia; acute renal failure; and sepsis ( Figure 1 ). Rates of various surgical and medical postoperative complications varied depending on the procedure and cancer site ( Table 3 ).
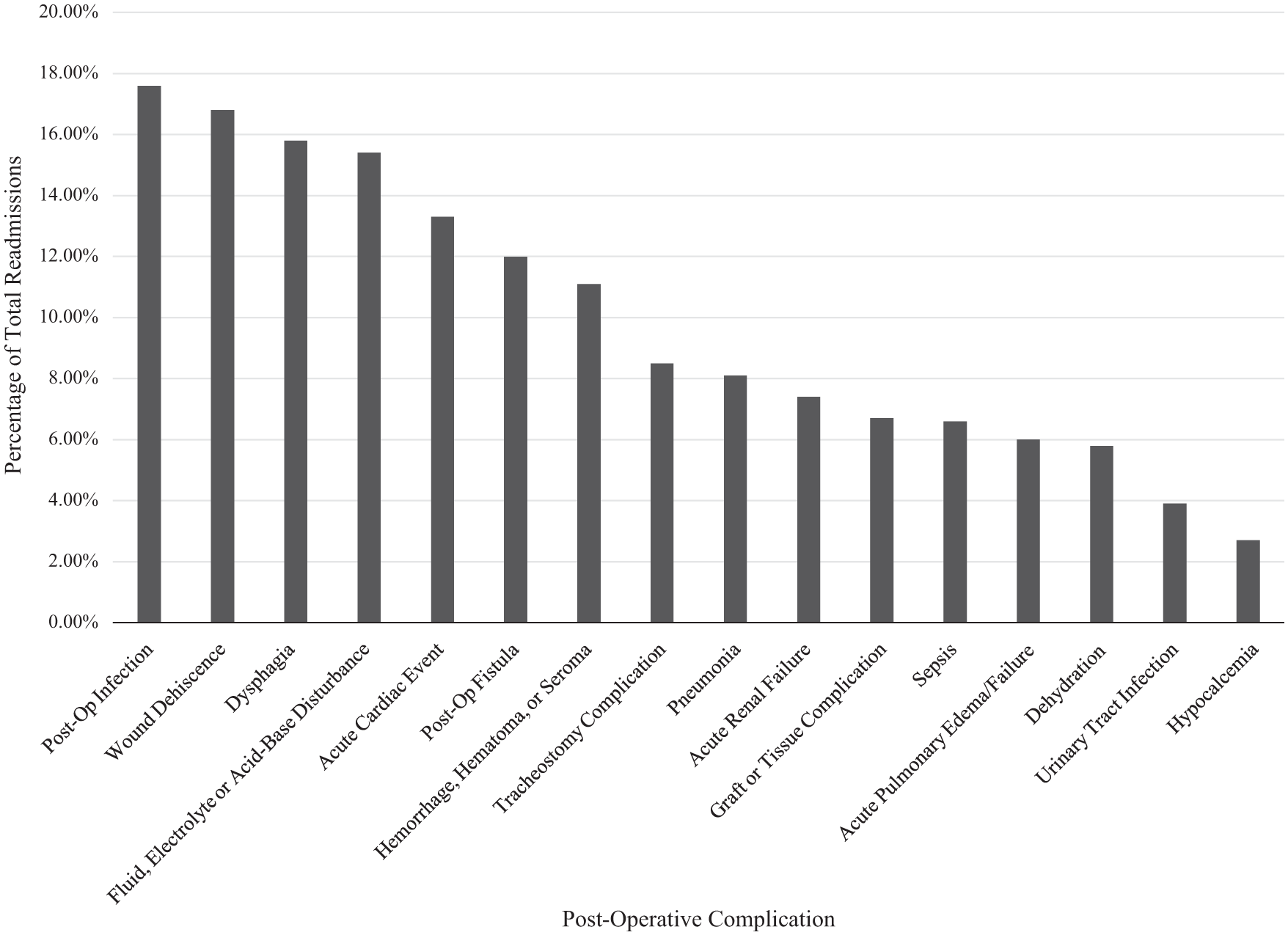
Overall frequency of complications upon 30-day readmission.
Most Common Postoperative Complications on Readmission by Procedure and Cancer Site.
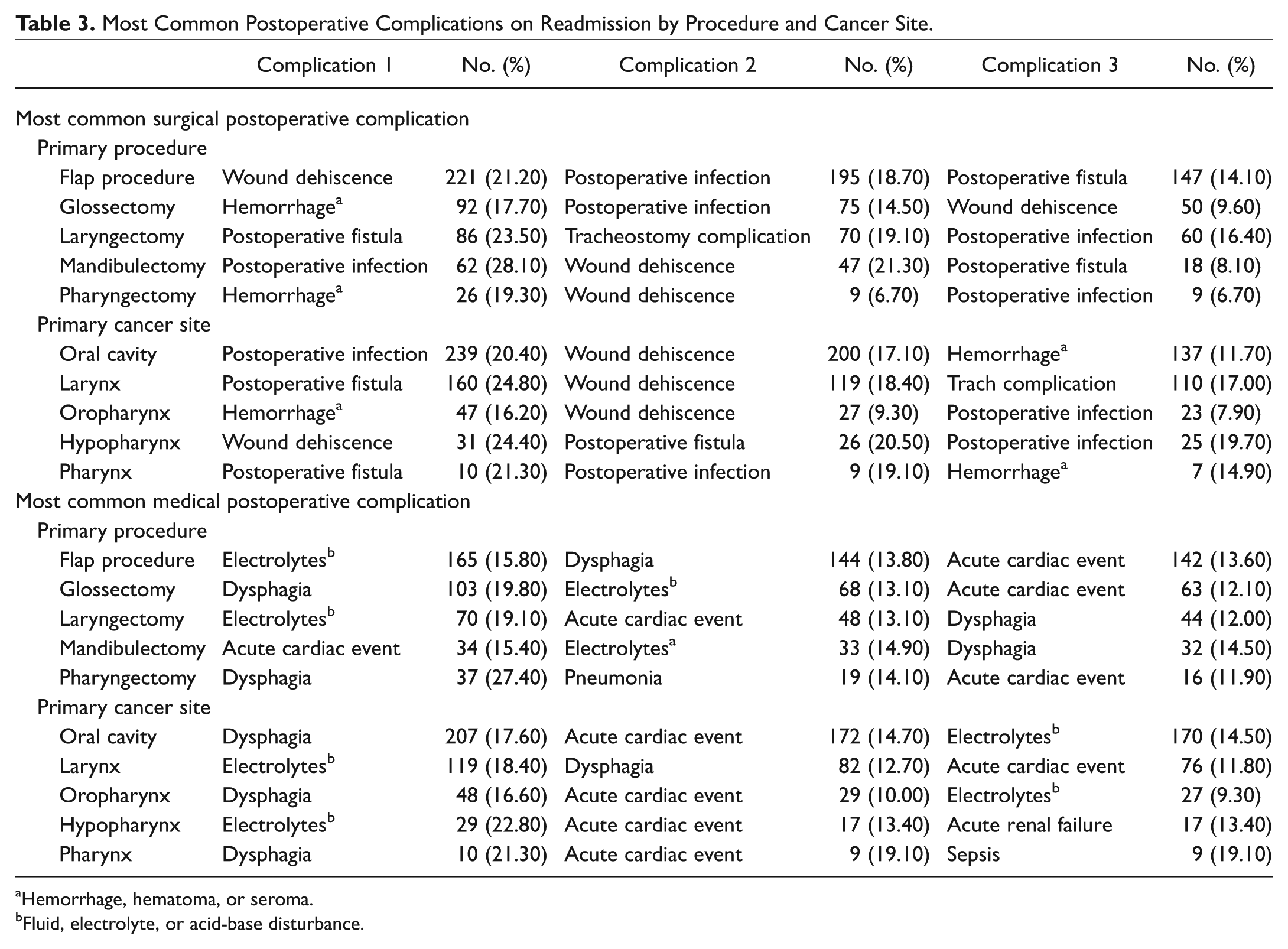
Hemorrhage, hematoma, or seroma.
Fluid, electrolyte, or acid-base disturbance.
Days to Readmission and Kernel Density Estimates
Overall, the time from discharge to readmission (mean ± SD) was 10.7 ± 8.2 days. However, patients with a free flap were readmitted significantly earlier than patients without a free flap (9.8 ± 7.7 days vs 11.0 ± 8.2 days, respectively; P = .002). Although the median number of days to readmission was 9 (interquartile range [IQR], 4-15), the peak and interval time to readmission varied depending on the postoperative complication. Patients with a flap procedure (pedicle and free tissue transfer) were readmitted 10.1 ± 7.9 days from discharge (mean postoperative day = 21.8 days). Table 4 demonstrates the length of stay, postoperative day, and days from discharge to readmission by procedure and surgical complication to better elucidate temporal trends in days to readmission. Admissions complicated by hemorrhage, hematoma, or seroma were more likely to present between postdischarge days 3 and 4 (median, 6; IQR, 3-11), earlier than all other postoperative complications. This correlated to readmission within 8.1 ± 6.7 days from discharge (postoperative days 15.9 ± 9.6). Patients with postoperative infection and wound dehiscence were most likely to be readmitted on postdischarge days 4 and 5. Both had similar median days to readmission from discharge (7 days) and median postoperative days (18 days). Last, compared to other postoperative complications, patients with fistula formation had a higher likelihood of being readmitted after postdischarge day 20 than patients with other surgical complications ( Figure 2 ).
Length of Stay, Postoperative Day, and Days to Readmission.
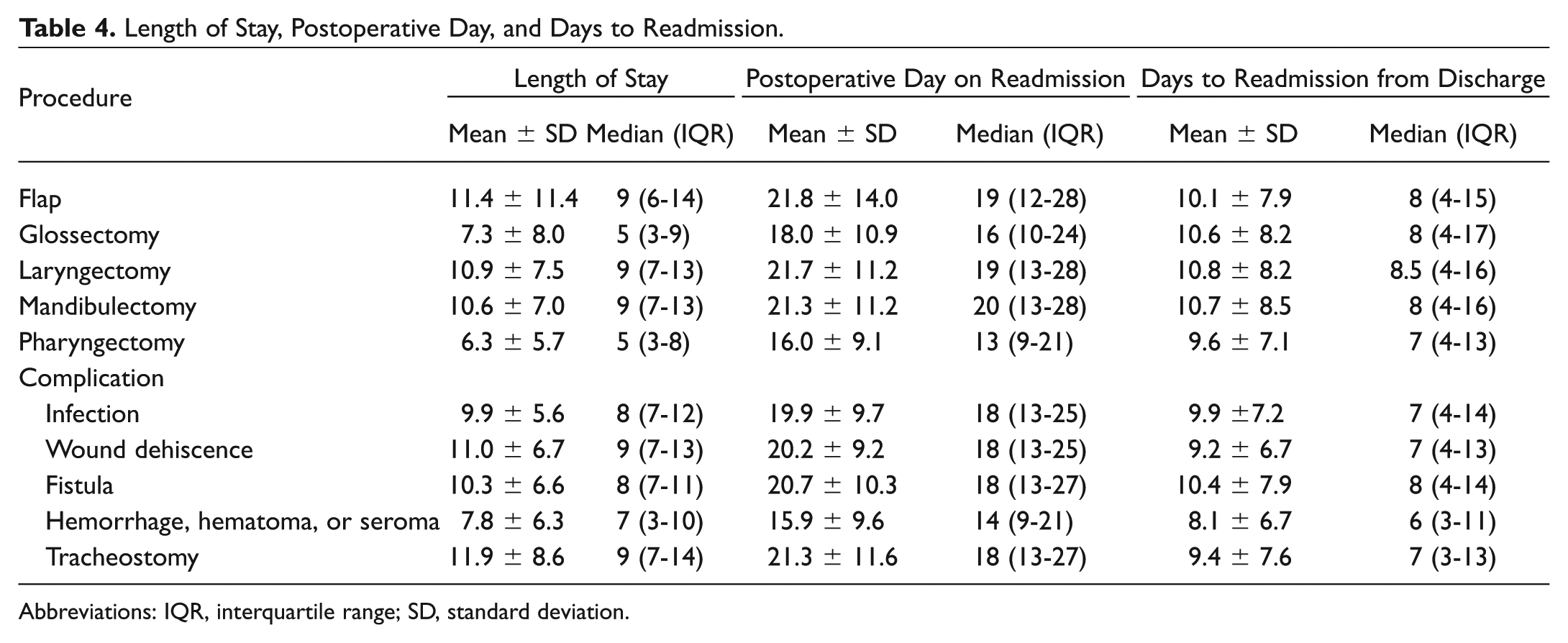
Abbreviations: IQR, interquartile range; SD, standard deviation.
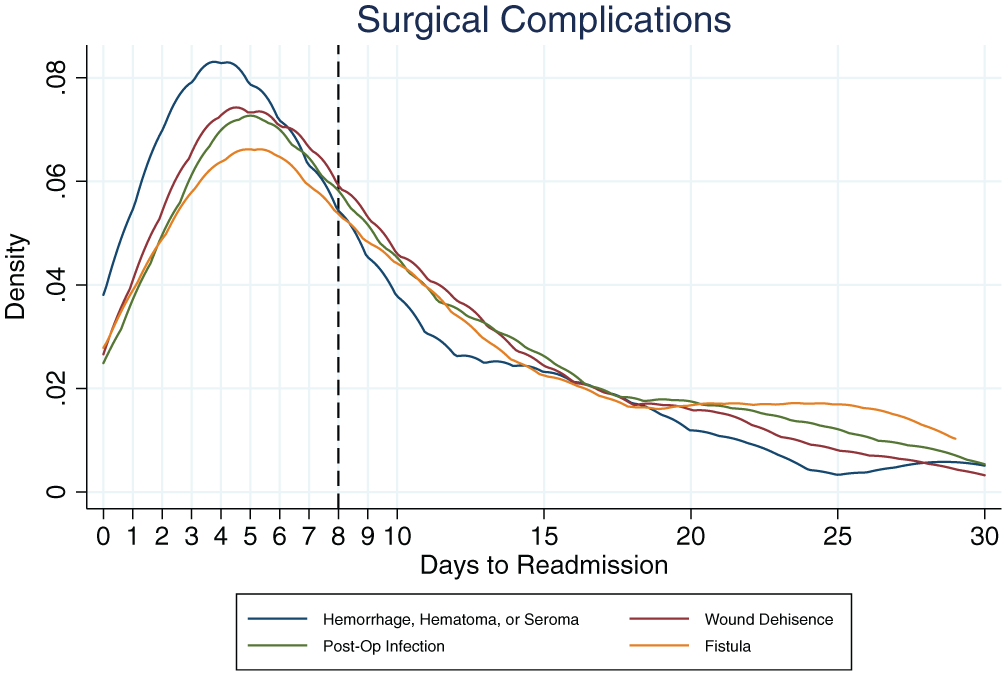
Kernel density estimates, surgical complications.
With respect to medical complications, patients readmitted for an acute cardiac event (median, 7; IQR, 3-13) or pneumonia (median, 6.5; IQR, 3,13) were likely to present earlier than all other medical complications. Patients with acute renal failure were most likely to present on postdischarge day 5 or 6 (median, 9; IQR, 4-17) but also had the highest frequency of readmission among patients readmitted after postdischarge day 20 ( Figure 3 ).
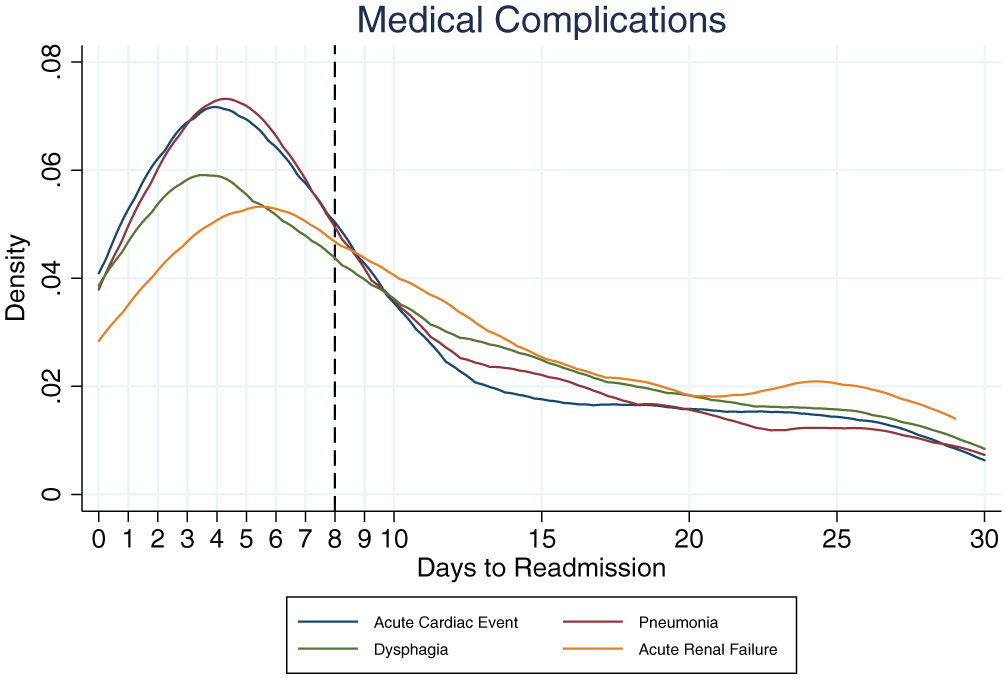
Kernel density estimates, medical complications.
Discussion
In this large retrospective review of 30-day unplanned readmissions following head and neck surgery, we analyzed readmissions among patients with mucosal tumors of the aerodigestive tract as they represent a high-risk population compared to patients with other types of head and neck cancer such as cutaneous, endocrine, or salivary gland tumors. 20
This study demonstrates that HNC patients are at high risk of readmission and that the risk of readmission may differ within this population depending on the cancer site and surgical intervention. The overall rate of 13.8% readmission is similar to those reported in prior studies.5,8,12,15 Our reported rate is higher than those reported of general otolaryngology patients, which includes a higher volume of ambulatory procedures (eg, sinus surgery, voice disorders, facial plastics, and otology).8,9 This difference reflects the relatively high morbidity of HNC and its treatment and underscores the need to evaluate and approach patient safety and quality improvement projects pertaining to HNC populations differently compared to other otolaryngology populations.
Having a laryngectomy and having cancer of the larynx were found to increase odds of readmission within the HNC population. Other studies suggest similar findings and likely represent the fact that laryngectomy patients are at greater risk of readmission compared to other HNC patients.10,14,16 While the most common codes for readmission following laryngectomy were fistula formation and tracheostomy complications, clinically fistulas represent the same underlying process as surgical site infections and wound dehiscence seen in the other surgical patients. Thus, while the coding is different, the reasons for readmission represent more of the same overall problem affecting HNC patients—wound dehiscence and surgical site infection. Quality improvement measures targeted at these most common causes of readmission are likely to reduce 30-day readmission and improve patient care.
Our results suggest that patients who undergo laryngectomy should be more carefully monitored for wound dehiscence and infection and that interventions targeted at wound healing and infection control are likely to decrease readmission. These measures may include optimization of postoperative nutrition and controlling for comorbidities that affect wound healing such as diabetes mellitus and hypothyroidism.21-23 Protocols involving evaluation and treatment with a dedicated inpatient wound care team may facilitate improvements in wound care throughout the trajectory of the patient’s postoperative course.
Like laryngectomy, flap procedures also conferred risk of readmission and were readmitted for similar reasons. Therefore, it is likely that these patients would also likely benefit from the abovementioned interventions. However, given the constraints of the study, we were not able to make reliable inferences on the extent of the ablative and reconstructive portions of the surgery using codes as a surrogate. It was unclear if surgical site infections and dehiscence were from the ablative site or the donor sites. Studies with clinical and surgical data would be needed to further understand the exact reasons for readmission.
Fluid and electrolyte disorders, uncomplicated diabetes, congestive heart failure, depression, metastatic cancer, and lymphoma on admission were found to significantly increase odds of readmission. Prior studies have reported similar risk factors.7,8 These comorbidities may help providers identify patients who are at high risk of readmission and who may need to be more closely monitored. Incorporation of multidisciplinary teams that include nutritionist, speech-language pathologist, social workers, mental health providers, respiratory therapist, and medical intensivist may help to control for these comorbidities and reduce readmissions. Some centers have recognized this need and have created specialized head and neck units within their hospital with health care teams that are familiar with the unique needs of head and neck surgical patients. They include nurses and respiratory therapist trained in management of tracheostomies as well as nurse practitioners and case managers familiar with the home health care needs. Interventions using multidisciplinary teams familiar with HNC populations may improve transition of care and reduce readmissions.24,25
Presence of any one of these comorbidities can also help providers identify at-risk patients at the time the need for surgery is identified. Preoperative clinics can provide valuable patient education and help optimize medical comorbidities prior to surgery. Furthermore, at-risk patients may be assigned a case manager or patient navigator who can closely monitor patients throughout the trajectory of their care and as they transition from the preoperative setting to the postoperative setting and back to clinic.6,26,27
The KDE elucidated different trends in days between discharge and readmission by the type of complication. While the results show that most patients are readmitted within the first 10 days after discharge, the frequency at which these patients are readmitted varies. In particular, patients with hemorrhages presented earlier compared to other postoperative complications, and those with fistula tracts were more likely to present later than those with other surgical complications. On further analysis, it was found that patients who were readmitted due to a hemorrhage, hematoma, or seroma had a shorter hospital stay compared to those who were readmitted for other complications (7.8 [7.0-8.6] days, 10.6 [10.2-11.1] days; P < .000). Patients with glossectomy or oropharyngeal cancer were most commonly readmitted for hemorrhage, hematoma, or seroma. Thus, outpatient follow-up within 1 to 2 weeks from discharge would be appropriate and may identify patients at risk for such complications. Providers may also consider discharge to acute care facilities (or skilled nursing facilities) where patients may continue to benefit from close observation that would otherwise be associated with high inpatient costs and resources.
This study has several limitations. First, patients who died 30 days within surgery were excluded, so no relationship between readmission and risk of mortality can be inferred. Second, due to the granularity of patient-level information in the database used, we were unable to control for tumor stage in our analysis, although we were able to use metastatic cancer as a surrogate for tumor burden in the multivariate analysis. Third, it is possible that patients had been readmitted to an outside facility, causing us to underestimate the rate of readmission. In addition, analysis was largely based on ICD-9 code. In this regard, coding can be at the discretion of billers and coders whose objective is coding for hospital reimbursement for Diagnoses Related Group (DRG). Last, given the retrospective nature of this study and constraints of this database, we were not able to differentiate between primary vs salvage surgery following radiation/chemoradiation. The implications of prior radiation and its effect on postoperative wound healing and fistula formation are well described in the literature.23,28,29 Future studies investigating readmission in HNC patients should attempt to address this issue and how it affects the trajectory of patient care from a patient safety and quality improvement perspective.
Implications for Practice
In effort to reduce 30-day readmissions, there is a growing need to balance quality of care and efficiency within financial and administrative constraints. It is important for health care administers and providers to identify at-risk populations and tailor interventions targeted at these populations and the common causes of readmission. In this at-risk population of HNC patients, limited resources and funding should be allocated toward measures that reduce surgical site infections and wound dehiscence as well as controlling for comorbidities that confer risk of readmission. Utilization of multidisciplinary care teams, dedicated head and neck inpatient units, and patient navigators may help in improving patient care throughout the trajectory of their care and ultimately reduce readmissions.
Conclusions
This study looked at readmissions among HNC patients who underwent surgery across multiple head and neck surgery centers across the country. Overall, 13.8% of patients with mucosal tumors of the aerodigestive tract are readmitted within 30 days. Patients with cancer of the hypopharynx (21.6%) or larynx (17.4%) and those who underwent a flap procedure (16.9%) or laryngectomy (16.5%) are readmitted at higher rates. Comorbidities such as electrolyte imbalances, diabetes, depression, metastatic cancer, and congestive heart failure are predictive of readmission. Last, the postoperative complications upon readmission vary by the type of cancer and the procedure type. The data from this study can be used by hospital administrators, quality improvement officers, and surgeons for comparative benchmarks on readmissions and to develop targeted interventions to reduce 30-day readmission rates.
Author Contributions
Disclosures
Supplementary Material
Supplementary Material, Supplemental_Table_S1 – Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission
Supplementary Material, Supplemental_Table_S1 for Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission by Michael K. Ghiam, MD, Alexander Langerman, MD, MSH, Zoukaa Sargi, MD, MPH and Sarah Rohde, MD in Otolaryngology–Head and Neck Surgery
Supplementary Material
Supplementary Material, Supplemental_Table_S2 – Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission
Supplementary Material, Supplemental_Table_S2 for Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission by Michael K. Ghiam, MD, Alexander Langerman, MD, MSH, Zoukaa Sargi, MD, MPH and Sarah Rohde, MD in Otolaryngology–Head and Neck Surgery
Supplementary Material
Supplementary Material, Supplemental_Table_S3 – Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission
Supplementary Material, Supplemental_Table_S3 for Head and Neck Cancer Patients: Rates, Reasons, and Risk Factors for 30-Day Unplanned Readmission by Michael K. Ghiam, MD, Alexander Langerman, MD, MSH, Zoukaa Sargi, MD, MPH and Sarah Rohde, MD in Otolaryngology–Head and Neck Surgery
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2017 AAO-HNSF Annual Meeting and OTO Experience; September 10-13, 2017; Chicago, Illinois.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.