
Abstract
Objective
To determine whether liposomal bupivacaine (Exparel) is safe and effective in the management of posttonsillectomy pain among adult patients.
Study Design
A prospective single-blind randomized controlled trial.
Setting
An academic quaternary care center (Mayo Clinic, Rochester, Minnesota).
Subjects and Methods
From May 2015 to December 2016, 39 patients were randomized to receive oral pain medication and 8 mL of injected liposomal bupivacaine or oral pain medication alone for treatment of their posttonsillectomy pain. Visual analog scale pain intensity scores, oral pain medication usage, liquid oral intake, and complications were recorded for 2 weeks after the procedure.
Results
Thirty-nine patients were randomized, with 17 patients in the liposomal bupivacaine group and 22 in the control group. Fifteen patients in the liposomal bupivacaine group and 18 patients in the control group completed the study. Pain intensity score on postoperative day 1 (P = .043) proved to be the only statistically significant result, with no difference noted in pain scores on postoperative days 2 to 14. There was no difference in pain medication usage, liquid oral intake, postoperative hemorrhage, or adverse events between groups.
Conclusions
The injection of liposomal bupivacaine in the posttonsillectomy wound bed demonstrates improved pain intensity scores for the first 24 hours after surgery with no adverse complications noted in comparison with patients who did not receive the injection. Given the limited pain reduction and increased cost, use of liposomal bupivacaine in adult tonsillectomy patients appears to have minimal indication for use.
Tonsillectomy remains one of the most common surgical procedures performed in the United States. In 2006, >700,000 tonsillectomies, adenotonsillectomies, and adenoidectomies were performed in ambulatory and inpatient centers across the United States. 1 Given the frequency of this procedure, many studies have been performed in an effort to evaluate and optimize the procedure’s indications and subsequent effects on patients.
Pain is one of the most significant side effects for which patients will often inquire in the clinical setting. In an attempt to reduce this burden, many researchers have been driven to investigate methods for the reduction of pain after tonsillectomy. Studies have been performed on a variety of medications and surgical techniques, such as intravenous and local steroids, topical agents, and injection of local anesthetics.2-4 The pursuit for reduced pain, specifically the medications directed at treating this pain, has become even more important after the increased scrutiny of narcotic medications for children following the Food and Drug Administration (FDA) black box warning of codeine in 2009. 5
Lipsomal bupivacaine (Exparel) was approved by the FDA in 2011 for administration into a surgical site to produce postsurgical anesthesia. The liposomal drug delivery system releases the bupivacaine at a slower rate, with plasma concentrations present up to 96 hours after injection. 6 The drug’s half-life is 24 to 34 hours, as opposed to approximately 2.7 hours with plain bupivacaine, and it has been shown to provide measurable pain relief up to 72 hours after injection. 7 In an effort to reduce pain and oral pain medication usage, specifically narcotic pain medication, liposomal bupivacaine could be a positive adjunct in the treatment of patients undergoing tonsillectomy. Hence, our study hypothesis is as follows: if patients who have undergone bilateral tonsillectomy are injected intraoperatively with liposomal bupivacaine, then their pain intensity scores and oral pain medication usage will be reduced. In addition, liquid oral intake will be greater in comparison with that of patients who have not received the injection.
Methods
This study was executed at the Mayo Clinic (Rochester, Minnesota) from May 2015 to December 2016. The study was approved by the Mayo Clinic Institutional Review Board. The study is a parallel-group design with an allocation ratio of 1:1 and is a single-blind randomized controlled trial. This trial was registered and posted on Clinicaltrials.gov (NCT02444533). There was no industry sponsorship or involvement with the study. With consideration to our primary endpoints, a sample size determination was performed. A sample size of 14 in each group would have 80% power to detect a difference in means of 2.00 (the difference between the standard treatment group mean, µ1, of 8.00 and the injected treatment group mean, µ2, of 6.00), assuming that the common standard deviation is 1.800 with a 2-group t test and a 2-sided significance level of .050. The goal sample size was a total of 30 patients, 15 in each arm.8,9
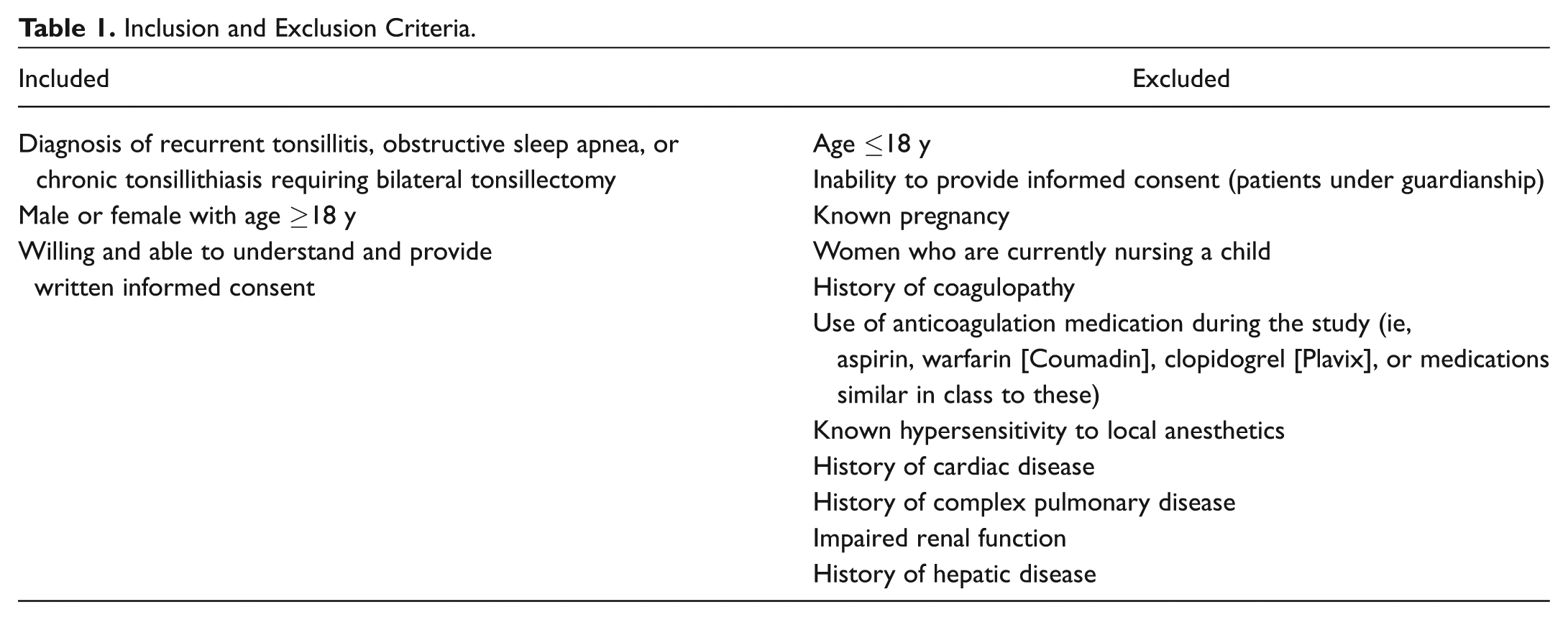
Participant inclusion and exclusion criteria are outlined in Table 1 . Participants who had additional procedures at the time of tonsillectomy (adenoidectomy, turbinoplasty, etc) were excluded from the study. Randomization was performed prior to participant enrollment. A computer-generated random sequence program was utilized. 10 Fifty packets of participant forms were assembled and numbered, with half recorded as controls and half as treatment. The computer-generated randomizer was used to obtain a random sequence for packet distribution according to the number on the packet as participants were allocated. The first author identified the participants to be enrolled, discussed the study with those identified, and assigned participants per the computer-generated randomization to the treatment groups.
Inclusion and Exclusion Criteria.
Participants were blinded to their treatment, but surgeons performing the procedure and study authors were not blinded to the participant’s treatment arm.
Interventions
Standardized tonsillectomy was performed for each patient for uniformity of technique and adjunctive medications. Participants were given general anesthesia, and each was given a 10-mg intravenous dose of dexamethasone in the operating room prior to the start of the procedure. No perioperative antibiotics were used. Bilateral subcapsular tonsillectomy was performed with the monopolar electrocautery set at 18 W. After the tonsillectomy, 8 mL of the liposomal bupivacaine (266 mg/20 mL, 4 mL on each side) was injected into participants in the treatment group. Injections were placed in the anterior pillar, posterior pillar, and tonsillar fossae. No injections were performed in the control arm.
Participants were instructed on their postoperative medication treatment regimen. Each patient was given a prescription for liquid oxycodone (5 mg/5 mL), with instructions to take 5 to 10 mL up to every 3 hours as needed for pain. In addition, participants were instructed to use acetaminophen (1000 mg orally every 6 hours) and ibuprofen (800 mg orally every 6 hours) as needed for pain, supplied in liquid or pill form based on patient preference. No additional prescription or over-the-counter medications were allowed for pain management. Note that the frequency of oxycodone prescribed is off-label, with the package insert directing usage every 4 to 6 hours. In addition, medications were not provided to the patients, but all patients used each medicine recommended by the study authors for their pain control as confirmed by their pain medication usage charting.
Primary Outcome Measures
Pain Intensity Scores
Pain intensity scores were recorded with a standard visual analog scale (VAS; 0-10 cm). On the far left of the scale, 0 was labeled “no pain,” and on the far right, 10 was labeled “worst possible.” Scores were recorded 4 times per day at set times: 08:00, 12:00, 16:00, and 20:00 hours. Scores were recorded on a provided form for 1 to 14 days, with day 1 being the day of surgery. For each day, the mean was calculated and used for statistical analysis.
Analgesic Use
For each pain medication used (oxycodone, acetaminophen, and ibuprofen), participants were asked to record the time, date, and dosage for each medication. Participants were provided with a medication administration diary. Total medication amount in milligrams was recorded for each day. Data were collected for days 1 to 14.
Liquid Oral Intake
Participants were asked to record their liquid oral intake with a form that provided guidance on the number of ounces that typical beverages and cups contain. Each time the patients consumed a liquid beverage, no matter the type, they were asked to record the amount in milliliters or ounces. Participants were asked to record these data for days 1 to 7. Total amounts consumed per day were tabulated and converted to milliliters for statistical analysis.
Secondary Outcome Measures
Safety and Adverse Events
Participant safety measures were recorded for 6 weeks after the participant’s tonsillectomy. Primary measures included the following: rates of posttonsillectomy bleeding, admission to the hospital for any reason, serious vital sign alternations surrounding the injection of the liposomal bupivacaine, and rates of allergic reaction to the liposomal bupivacaine. Posttonsillectomy bleeding was defined as any blood from the oral cavity after the procedure that prompted the patient to contact a care provider for advice or evaluation. The electronic medical record, direct reporting from the participant at the 6-week postoperative visit, and phone calls to the participants were used to identify adverse events. All patients were contacted 6 weeks after their procedure to ensure accuracy of adverse event reporting.
Statistical Methodology
Descriptive statistics are reported as mean and SD for continuous variables and number and percentage for categorical variables. Between-group comparisons for outcomes and demographic statistics were made with t tests or Wilcoxon rank-sum tests for continuous variables and chi-square tests for categorical variables. Statistical significance was defined as a P < .05. All analyses were performed in R (version 3.2.0; Vienna, Austria).
Results
Forty-seven patients were eligible to participate per the inclusion criteria. Eight patients declined to participate, which resulted in 39 being enrolled in the study ( Figure 1 ). Of the 39 patients who were randomized, 17 were in the liposomal bupivacaine group and 22 in the control group. The completion rate of the study was 85%, with 33 of 39 patients fulling completing the required documentation. The demographics of both groups are outlined in Table 2 . Sex differences were not statistically different for the entire sample (23 women vs 10 men, P = .137), but in the control group there were 15 women versus 3 men (P = .004) and in the liposomal bupivacaine group there were 8 women versus 7 men (P = .79). Body mass index (BMI) proved to be statistically different between groups, with the control group’s mean BMI at 24.2 and the liposomal bupivacaine group’s at 30.6 (P = .004). Two patients in the liposomal bupivacaine group and 4 patients in the control group did not complete the required forms and were eliminated from the pain score, pain mediation usage, and liquid oral intake analysis. These 6 patients were followed and their data analyzed for safety and complications.
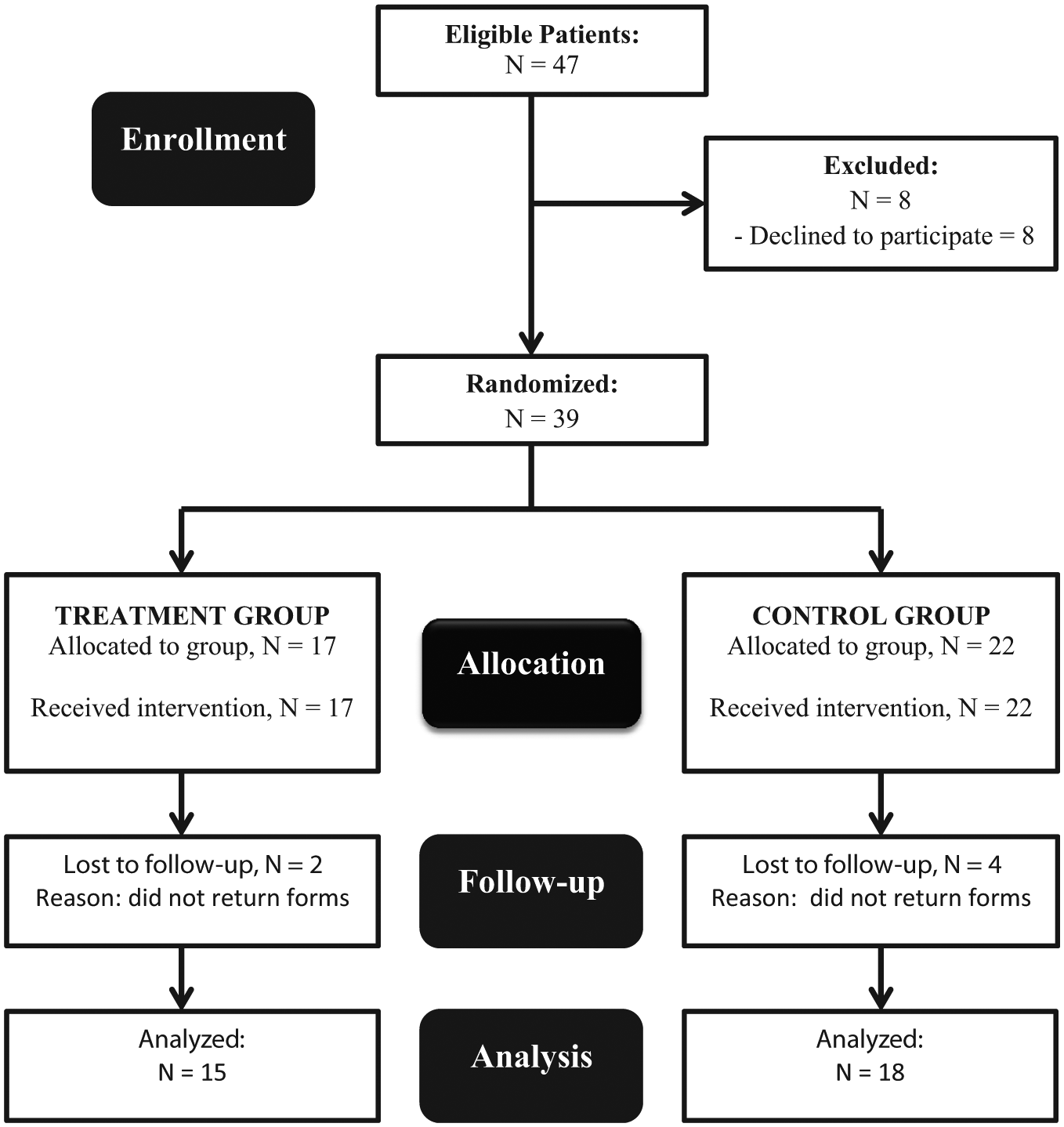
Trial flow diagram according to CONSORT 2010 recommendations.
Demographic Data for Participants. a
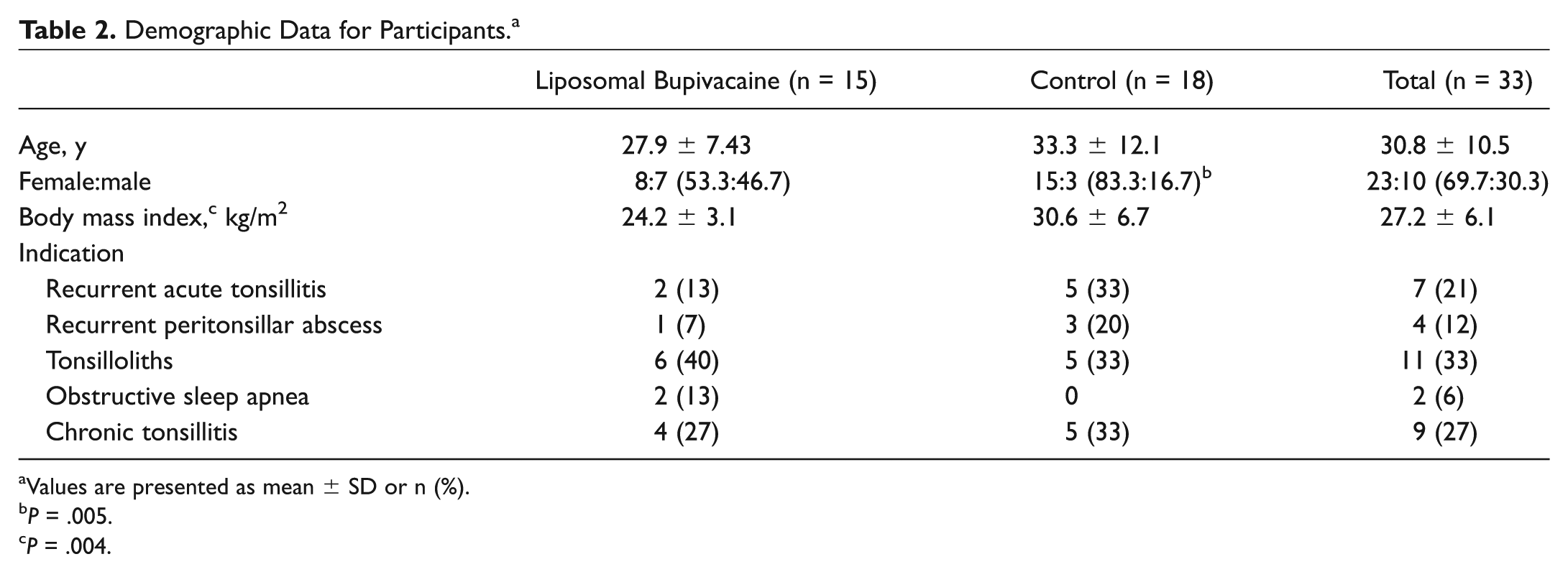
Values are presented as mean ± SD or n (%).
P = .005.
P = .004.
Pain Intensity Scores
Pain >intensity scores were recorded from postoperative days (PODs) 1 to 14, with day 1 being the day of surgery. Data from 15 patients who received the liposomal bupivacaine and 18 control patients were analyzed. Mean pain intensity scores are outlined in Figure 2 . On POD 1, there was a statistically significant difference in pain intensity scores between the groups, with the mean pain intensity score on POD 1 being 3.07 for the liposomal bupivacaine group and 4.90 for the control group (unpaired t test, P = .043). Of note, on POD 1, there were fewer pain score data points recorded secondary to the variability of operating room start times, but the number of scores recorded between the groups in total were not significantly different (41 scores for the liposomal bupivacaine group and 43 for the control group). There was no statistical difference in days 2 to 14 for pain intensity scores. For days 2 to 5, based on the length of action for liposomal bupivacaine, the P values were .294 for day 2, .626 for day 3, .792 for day 4, and .453 for POD day 5.
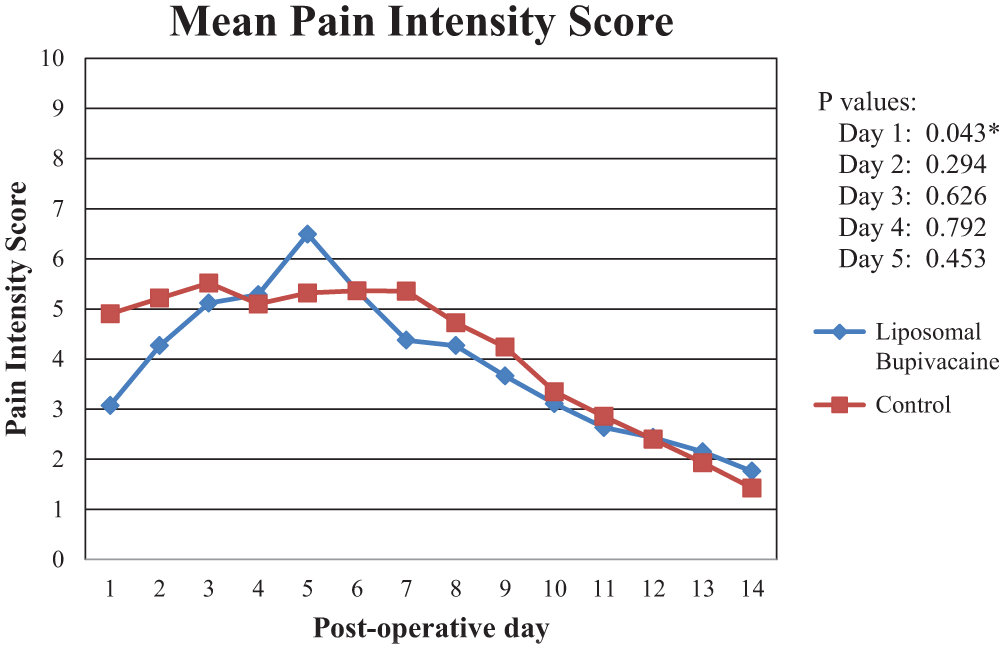
Mean pain intensity scores based on patient raw data. P values for days 2 to 14 did not reach statistical difference. *P < .05.
Pain Medication Usage
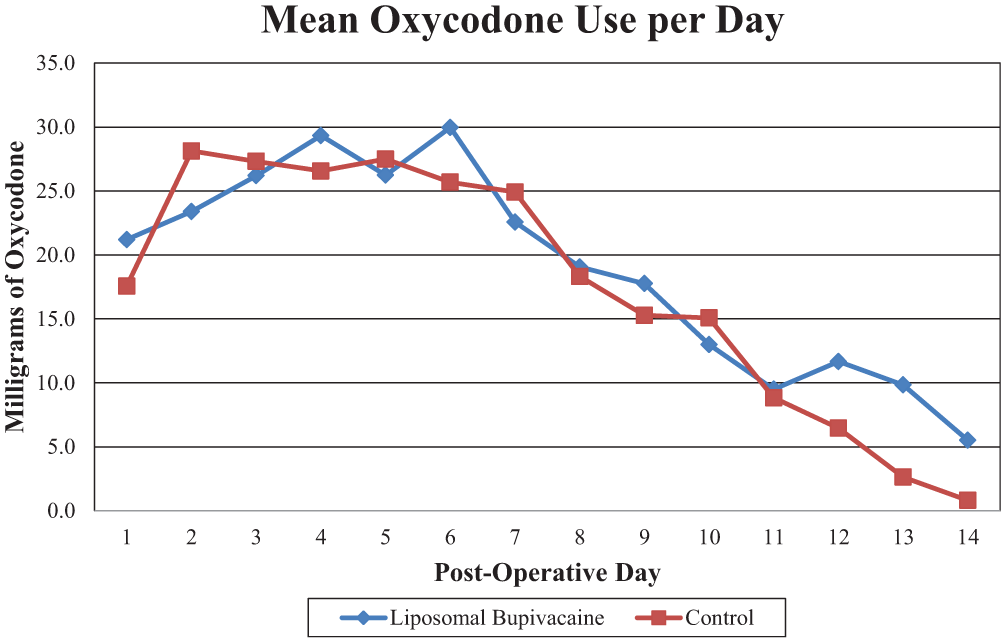
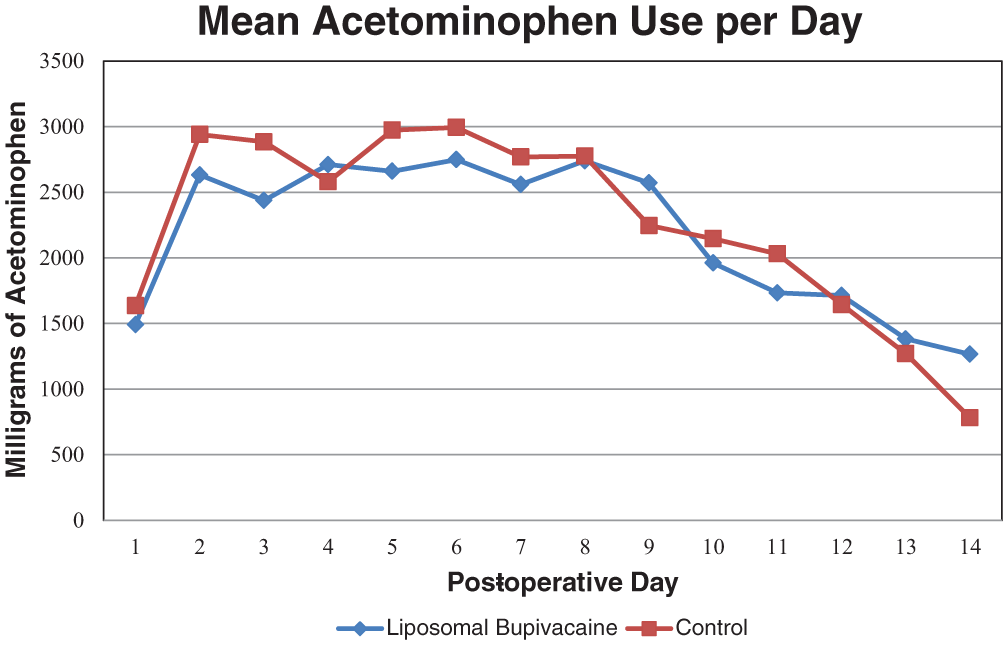
Oxycodone, acetaminophen, and ibuprofen usage was analyzed for postoperative days 1 to 14. No patients reported use of pain medications outside the study medications. There was no difference in the amount of pain medication (in milligrams per 24 hours) for any of the pain medications that the patients were directed to take. Figures 3 to 5 outline the amount of medication used for oxycodone, acetaminophen, and ibuprofen, respectively. P values for postoperative day 1 were as follows: .449 for oxycodone, .696 for acetaminophen, and .167 for ibuprofen. For PODs 1 to 14, there were no statistically significant P values for pain medication usage, for any of the medications used.
Mean acetaminophen usage per day (milligrams per 24 hours). P values for days 1 to 14 did not reach statistical significance (P > .05).
Mean oxycodone usage per day (milligrams per 24 hours). P values for days 1 to 14 did not reach statistical significance (P > .05).
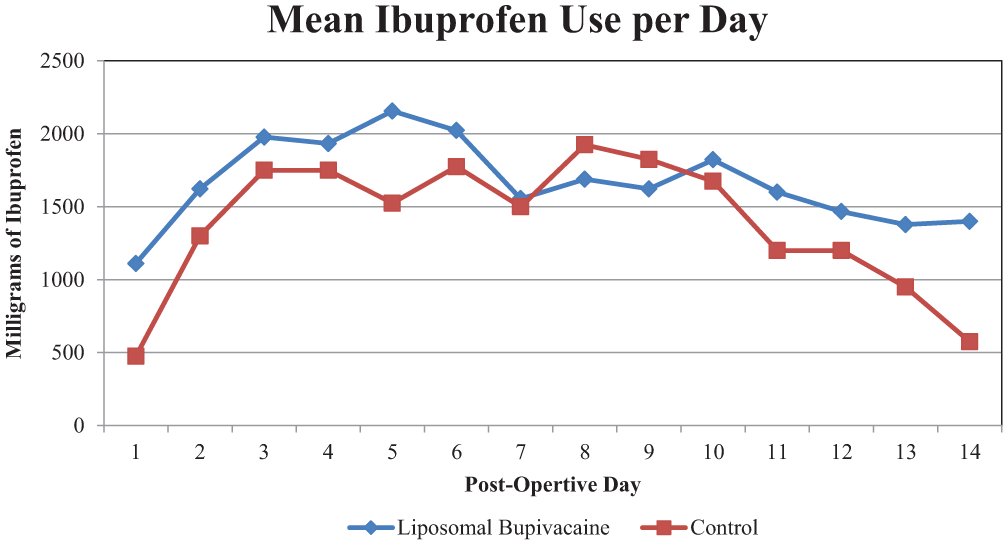
Mean ibuprofen usage per day (milligrams per 24 hours). P values for days 1 to 14 did not reach statistical significance (P > .05).
Liquid Oral Intake
Figure 6 depicts liquid oral intake in milliliters per 24 hours for PODs 1 to 7 for the liposomal bupivacaine and control groups. Total liquid oral intake did not differ between the groups, with the liposomal bupivacaine arm taking 13,715 mL (SD, 7551 mL) and the control arm taking 12,492 mL (SD, 4271 mL; P ≥ .99).
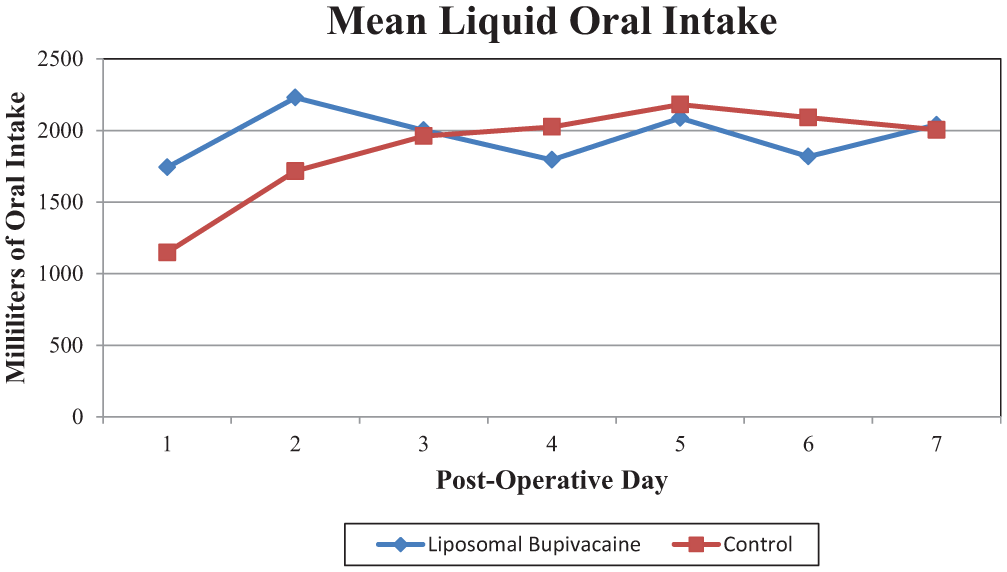
Mean liquid oral intake (milliliters per 24 hours). P values for days 1 to 7 did not reach statistical significance (P > .05).
Adverse Effects and Complications
No patients experienced an allergic reaction to the injected liposomal bupivacaine. There were no intraoperative or anesthetic complications in either group. One patient in the liposomal bupivacaine group presented to the emergency room on POD 6 for pain control, and 2 patients in the control group presented on PODs 5 and 6 as well. There was 1 admission in the control group for pain control but no admissions to the hospital for pain control or swallowing dysfunction in the liposomal bupivacaine group. One patient in the liposomal bupivacaine group developed subcutaneous emphysema of the neck on POD 2 secondary to cough and a likely violation of the buccal pharyngeal fascia during the tonsillectomy. The patient was admitted, and the subcutaneous emphysema resolved over the course of the next 24 hours without further complication.
There were no primary posttonsillectomy hemorrhages within the first 24 hours after surgery. Of the 39 patients enrolled in the study, 6 (15%) had secondary posttonsillectomy hemorrhage (>24 hours after surgery). Of these 6 cases of hemorrhage, 3 (8%) were considered major and required intervention in the operating room, and 3 (8%) were considered minor and observed. Table 3 describes the rates of complications and posttonsillectomy hemorrhage between the liposomal bupivacaine and control groups. In regard to hemorrhage rates between groups, the liposomal bupivacaine group had 4 of 17 (24%) patients who had major or minor hemorrhage, and the control group had 2 of 22 (9%; P = .229). The mean onset of bleeding after tonsillectomy was 7.5 days in the liposomal bupivacaine group and 8 days in the control group.
Complications. a
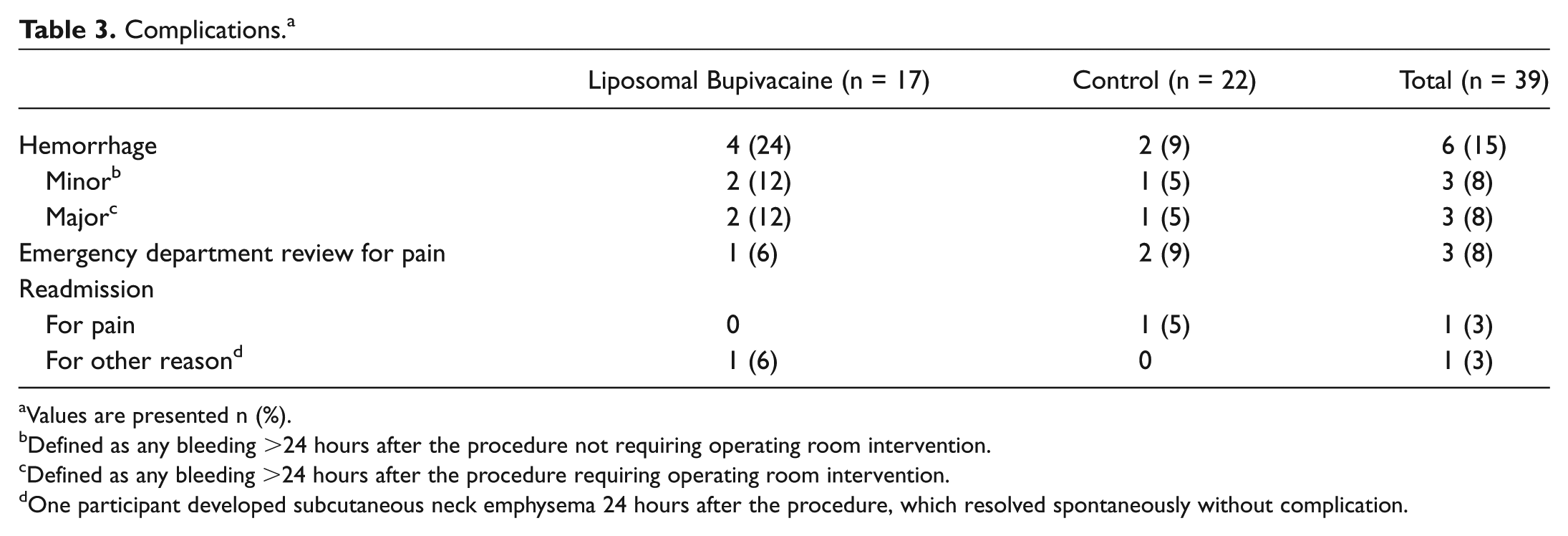
Values are presented n (%).
Defined as any bleeding >24 hours after the procedure not requiring operating room intervention.
Defined as any bleeding >24 hours after the procedure requiring operating room intervention.
One participant developed subcutaneous neck emphysema 24 hours after the procedure, which resolved spontaneously without complication.
Discussion
This study is the first to examine the role of liposomal bupivacaine, in a randomized controlled fashion, on primary outcomes such as pain, medication usage, and liquid oral intake among adult patients undergoing tonsillectomy. Given differences in past research regarding plain bupivacaine, we thought it necessary to answer the question of whether liposomal bupivacaine is beneficial in this setting, by first looking to see if it was better than no treatment at all. The only parameter that was statistically different (P < .05) was the first 24 hours after the procedure, where pain intensity scores fared better than those of the control group (P = .043). No other parameter (ie, oxycodone, acetaminophen, ibuprofen use, or liquid oral intake) a showed statistically significant difference during the study.
Liposomal bupivacaine was approved by the FDA in 2011 for administration into the surgical site to produce postsurgical anesthesia. Liposomal bupivacaine has been shown to reduce pain and opiate use in a variety of surgical procedures. Orthopedic surgery, general surgery, and thoracic surgery, as well as other specialties, have employed this medication in a variety of studies in an effort to reduce the amount of opioid medications that patients are given and to provide longer postsurgical anesthesia.11-14
These studies and others suggest that liposomal bupivacaine may be an important adjunct to postsurgical pain with the goals of improved pain, a longer duration of pain control, and reduced dependence on and use of opioid analgesics. A more thorough review of these studies was completed via a Cochrane review published in 2016 by Hamilton et al. 15 The conclusion of this review, which included 9 studies that met strict criteria (1377 participants), showed that although the studies did demonstrate reduced pain as compared with placebo, there was no appreciable difference in comparison with standard bupivacaine in the treatment of postsurgical pain.
No study has examined the effectiveness or safety of liposomal bupivacaine among adult patients undergoing tonsillectomy. Regarding bupivacaine as an injectable medication, multiple studies showed benefit while others did not. Recent studies, such as those by Erdogan et al in 2014 and Kaspoglu et al in 2013, demonstrated statistically significant reductions in pain scores among adult tonsillectomy patients treated with bupivacaine in comparison with placebo.16,17 Alternatively, in 1993 Schoem et al executed a prospective randomized double-blind study with plain bupivacaine after adult tonsillectomy, looking at pain intensity scores, medication usage, and oral intake. 18 Their study showed no significant difference between the group receiving the bupivacaine injection and the group receiving a saline injection, and this has been seen in others’ studies as well.19,20 In the pediatric population, a meta-analysis published by Sun et al indicated a statistically significant difference in pain intensity scores up to 48 hours and a decreased use of postoperative analgesic medication usage in multiple studies examining bupivacaine administration in this subgroup of patients who had undergone tonsillectomy. 21
Note that while we did see a statistically significant difference between pain intensity scores on POD 1, a clinically significant difference between groups on POD 1 is unlikely to have occurred. The mean POD 1 pain intensity score was 3.07 In our treatment group and 4.90 in our control arm, for a difference of 1.83 points. Kelly demonstrated that to obtain a reduction in pain that the patient noted was “a lot better,” pain scores needed to differ by at least 2.5 points on the VAS. 22 Others noted that a difference of at least 1.8 points on the VAS is needed to see any clinically significant difference.23,24 It is also important to recognize that differences in sex and BMI between the groups may reduce the reliability of the results. Although our randomization of participants created a near-equal distribution between groups, unless a large cohort of patients is obtained, similarities between weight and sex become difficult to equalize and may add to concerns of confounding factors leading to the results reported.
In regard to complications and adverse effects, our study demonstrates that liposomal bupivacaine appears to be a safe medication to use in this setting. In our study, no patients reported difficulties with swallowing or were readmitted secondary to swallowing dysfunction. The overall hemorrhage rate was 15% (6 of 39). Lack of clarity and a variety of definitions are present in the literature regarding posttonsillectomy hemorrhage. In some studies, hemorrhage is defined only if the patient is admitted to the hospital for treatment, while in others even blood-tinged sputum is recorded.25,26 Rates for posttonsillectomy hemorrhage also vary, with smaller studies often reporting rates >15%.27,28 Larger studies recorded posttonsillectomy hemorrhage rates between 2% and 4.2%.26,29 Given our small sample size, it becomes difficult to make any statistical generalizations regarding the rate of hemorrhage. When hemorrhage rates were evaluated between groups, there was no difference seen, but again an increased sample size would contribute to definitive determinations.
Limitations of the study included our ability to blind the surgeon/researcher to the study drug. In this case, the opacity of the liposomal bupivacaine liquid made any attempts at blinding difficult. In an ideal situation, 1 surgeon would have performed all the procedures, with the ability to be blinded to the treatment given; in addition, the use of plain liposomes could have been used as a placebo agent, although this material was not available for use at our institution. Saline injection as a controlling factor could be considered a limitation, although there is no consensus in the literature regarding the necessity of this step. Sample size was also a limiting factor, and ideally, a multi-institutional study assessing hundreds of patients receiving liposomal bupivacaine after tonsillectomy would be performed to solidify our conclusions.
Conclusions
This study is the first to assess the role of liposomal bupivacaine for adult patients who have undergone tonsillectomy. We demonstrated a slight but statistically significant difference in pain intensity scores in the first 24 hours after surgery in comparison with patients who did not receive the injection. Pain medication usage and liquid oral intake did not differ between the groups. We did not see any adverse effects or increased complication rates among patients who received the drug that were statically significant, although an elevated hemorrhage rate in both groups should be noted. Given the relatively short length of action and small decrease in pain intensity scores, utilization of the drug for postoperative adult tonsillectomy patients may not be advantageous.
Author Contributions
Disclosures
Footnotes
Acknowledgements
We thank statistician Tina M. Gunderson, MS, for partial assistance with statistical analysis.
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2016 AAO-HNSF Annual Meeting & OTO EXPO; September 18-21, 2016; San Diego, California.