
Abstract
Objective
The aim of this systematic review is to compare the surgical outcomes of supraclavicular artery island flap (SCAIF) and free tissue transfer (FTT) in head and neck reconstruction.
Data Sources
PubMed, Web of Science, and EMBASE databases.
Review Methods
Independent screening and data extraction were performed by 2 authors. Only studies that directly compared SCAIF and FTT were included. Data were pooled with random-effects meta-analysis to determine the standardized mean differences (SMDs), risk differences, and 95% confidence intervals (CIs). Heterogeneity was assessed using the I2 statistics. The Methodological Index for Non-Randomized Studies tool was used to evaluate extent of bias in studies.
Results
The initial query yielded 661 results, of which 4 comparative studies remained for final analysis. The pooled sample sizes for the SCAIF and FTT cohorts were 100 and 84, respectively. SCAIF was associated with reduction of operative time by a large effect size (SMD, 1.65; 95% confidence interval, 0.78-2.52). The harvested flap areas and perioperative complications, including rates of total flap loss, partial flap necrosis, and recipient/donor site dehiscences, were comparable between the 2 procedures with low to high heterogeneity among studies.
Conclusion
SCAIF requires less operative time and has comparable short-term perioperative results to FTT. The findings of this study support the viability of SCAIF as an alternative to FTT and provide evidence for its inclusion in the reconstructive armamentarium of major head and neck ablation and trauma.
Keywords
Free tissue transfer (FTT) continues to be the primary workhorse in complex, soft tissue reconstruction of the head and neck. In particular, radial forearm free flap (RFFF) and anterolateral thigh flap (ALT) have emerged as standard flaps in the armamentarium of the reconstructive surgeon.1,2 Yet, in the medical climate of optimizing cost-effectiveness and quality improvement, regional pedicled flaps are attractive reconstructive alternatives for postablative and posttraumatic defects. The pectoralis major has been used as a popular option for regional tissue reconstruction, but its thickness and restricted reach have conferred some limitations. 3
The supraclavicular artery island flap (SCAIF), with its proximity, thin skin paddle, and versatility, has emerged as a dependable source of reconstruction,4-10 with multiple recent studies documenting the anatomic reliability of this flap.9,11-15 Pallua and colleagues 11 popularized SCAIF in the 1990s for cervical mentosternum reconstruction. Subsequently, multiple studies highlighted the use of this flap related to parotidectomy, auriculectomy, laryngectomy, partial laryngopharyngectomy, the establishment of digestive tract continuity, and massive head and neck defects secondary to necrotizing fasciitis.9,12-23
The anatomical parameter of this flap, including its thickness and pliability, is similar to RFFF, 8 with the added benefit of providing better color match. In certain cases, using SCAIF supersedes the use of FTT because of coexisting patient conditions deemed high risk, such as old age, advanced tumors, poor nutrition, and multiple comorbidities. 9 Given the increasing popularity of SCAIF, assessment of its candidacy as an alternative flap to FTT is required and comparative analyses between them are necessary in defects amenable to both types of repair.
Hence, the objective of this systematic review is to compare the surgical outcomes of SCAIF and FTT in head and neck reconstruction. To our knowledge, this is the first systematic review and aggregate quantitative analysis examining this topic.
Materials and Methods
The primary study question, framed in the PICO (Population, Intervention, Comparison, and Outcome) format, was the following: in patients who underwent head and neck reconstruction, how do the surgical outcomes of SCAIF compare to FTT? The framework of this review was consistent with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) reporting standards.
We performed a systematic review by searching PubMed, Web of Science, and EMBASE databases. The inquiry was performed with the keywords supraclavicular and flap. This search was limited to English-only articles; conference abstracts, book chapters, and textbooks were excluded. Only studies that directly compare SCAIF and FTT with relevant outcomes were included. For studies with overlapping patient cohorts, we included only the study with the largest sample size or, if the sample sizes were equal, the highest reporting quality (lowest risk of bias).
No restriction to indications for SCAIF was placed. Only outcomes described by 3 or more studies were included in the analysis. Two investigators independently performed the screening and data abstraction (D.C.S. and A.T.). The technique of SCAIF harvest has been previously described by multiple studies.8,10,11,17,24-29 The methodological quality of the studies was assessed based on the Methodological Index for Non-Randomized Studies (MINORS) criteria. 30 Any overlying discrepancies between the findings of the first 2 authors were resolved through a mutual discussion with the senior author of this study (E.A.G.).
Data were pooled with random-effects meta-analysis to determine the standardized mean differences (SMDs), risk differences (RDs), and 95% confidence intervals (CIs). Statistical analysis was performed using meta-analysis software 31 to pool outcomes across studies (when 3 or more studies reported a common outcome) for reconstruction performed using SCAIF vs FTT. Pooled mean and standard deviation (SD) for continuous variables were estimated and weighted based on study sample sizes. For continuous outcomes (eg, operative time, flap area), effect size is reported as the SMD, calculated as the mean difference in outcomes for the 2 treatment groups, divided by the standard deviation within the groups. The SMD is comparable to Cohen’s effect size and can be interpreted as trivial if less than 0.20, small if 0.20 to 0.49, moderate if 0.50 to 0.79, and large if 0.80 or higher. 32 For dichotomous outcomes (eg, total flap loss, partial necrosis), effect size is reported as the (absolute) risk difference between groups. All data were pooled using a random-effects model, which does not assume a common effect size across studies and results in wider 95% CIs compared to a fixed-effects approach. The random-effects model was graphically displayed in the form of a forest plot. The model calculated the effect sizes between SCAIF and FTT cohorts of individual studies and pooled the final outcome. The diamond in the forest plot represented the pooled effect size and CI associated with it. Heterogeneity was assessed using the I2 statistics, with values of 25%, 50%, and 75% corresponding to low, moderate, and high heterogeneity, respectively. 33 Significance was assessed with a threshold P value of .05.
Results
The search resulted in 661 studies, of which 4 studies remained for final analysis ( Figure 1 ). The characteristics of the studies and demographic variables are summarized in Table 1 . All of the studies were retrospective or case series with chart reviews. The sample sizes ranged from 12 to 45 for the SCAIF cohort and 15 to 28 for the FTT cohort, resulting in a pooled total of 100 and 84 patients, respectively. The indications for reconstruction varied across studies. Two studies evaluated reconstruction after oral cavity and/or oropharyngeal resections.6,7 Kozin and colleagues 5 investigated repair of cutaneous defects and defects related to total laryngectomy, parotidectomy, and temporal bone resections. Various posttraumatic and postablative defects were examined by Granzow and colleagues. 4 The mean age was between 55.6 to 68.9 and 58.8 to 64.0 for SCAIF and FTT groups, respectively. One study 4 reported mean body mass index (BMI; 24.12 vs 26.38, P = .26, for SCAIF and FTT, respectively). Preoperative radiation ranged from 8% to 48.9% for the SCAIF cohort and 0% to 42.3 for the FTT group. Preoperative chemotherapy was administered in 8% to 33.3% of patients in the SCAIF group and 0% to 25% in patients who underwent FTT. The follow-up timelines varied from 6.0 to 22.8 months. One study 5 did not report length of follow-up.
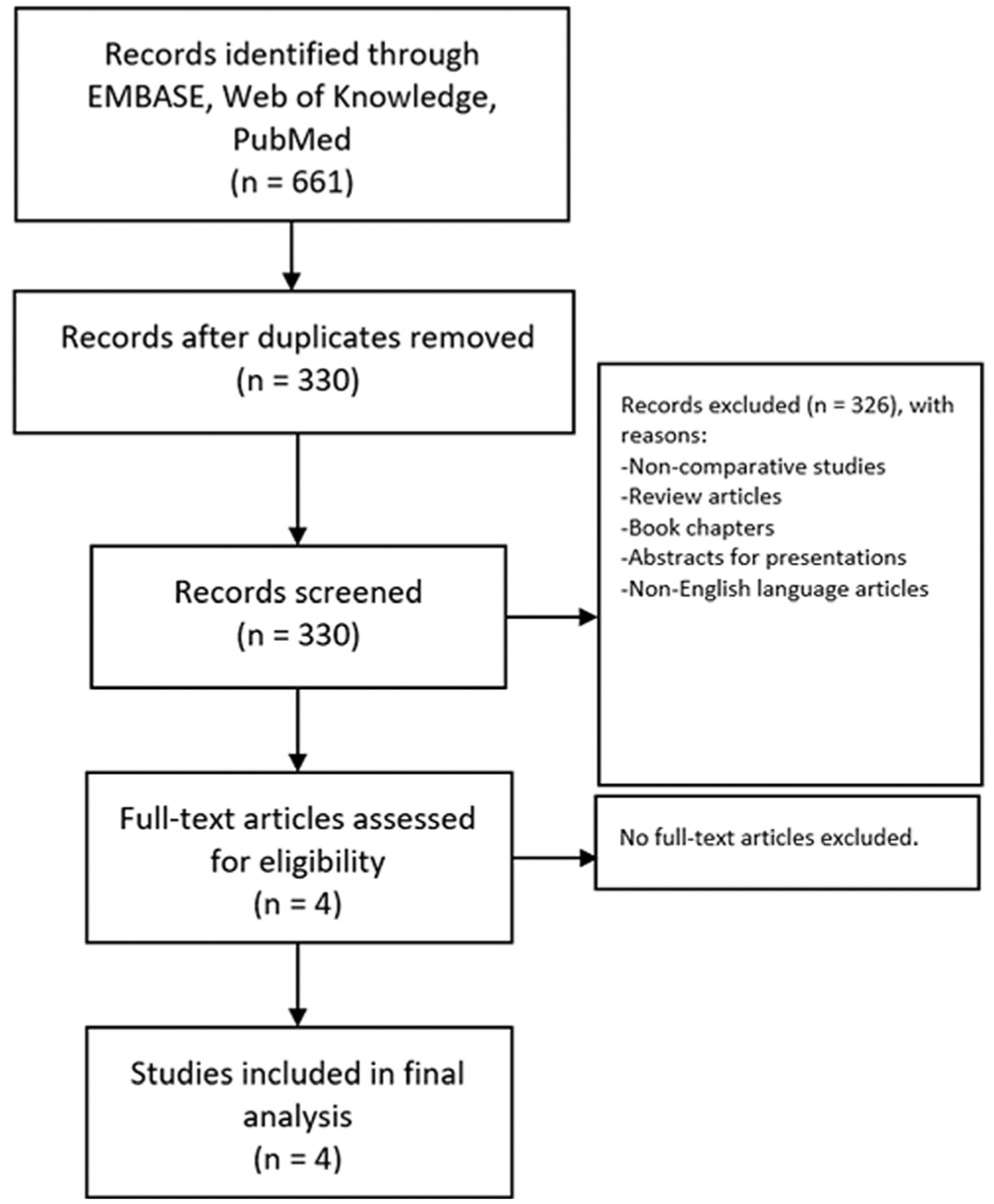
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Study Characteristics and Demographic Variables of SCAIF vs FTT Cohorts.
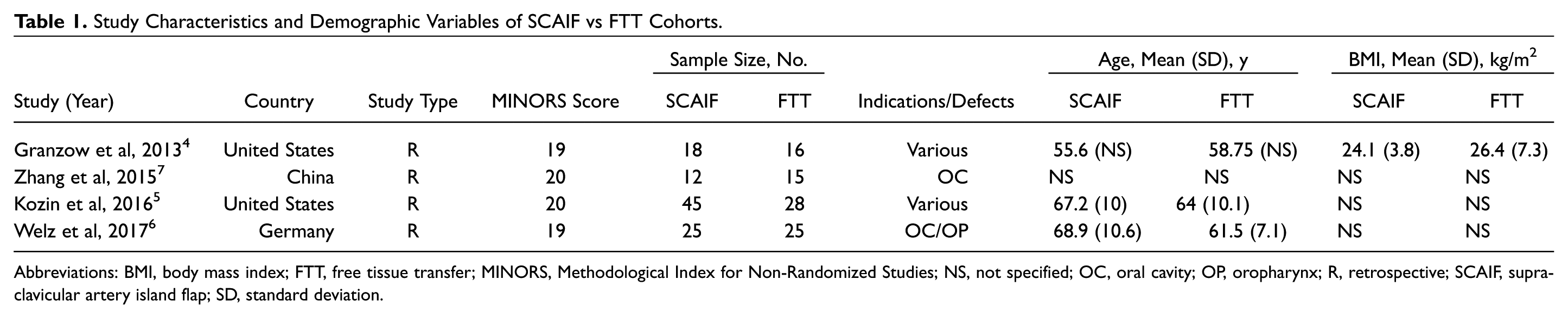
Abbreviations: BMI, body mass index; FTT, free tissue transfer; MINORS, Methodological Index for Non-Randomized Studies; NS, not specified; OC, oral cavity; OP, oropharynx; R, retrospective; SCAIF, supraclavicular artery island flap; SD, standard deviation.
The quality of each study was evaluated with the MINORS criteria ( Table 2 ). The MINORS scores ranged from 19 to 20 (mean, 19.5), with 24 as the perfect score (eg, lowest risk of bias) for comparative, observational studies. 30 All studies were deficient in power calculations and blinded evaluation of outcomes. Granzow and colleagues 4 observed a higher diabetes rate in their FTT cohort while Welz and colleagues 6 found that their SCAIF cohort was older. These baseline variabilities may act as confounders during comparative analyses. All studies were observational but did involve planned data collection.
Methodological Quality of Included Studies by MINORS Criteria.
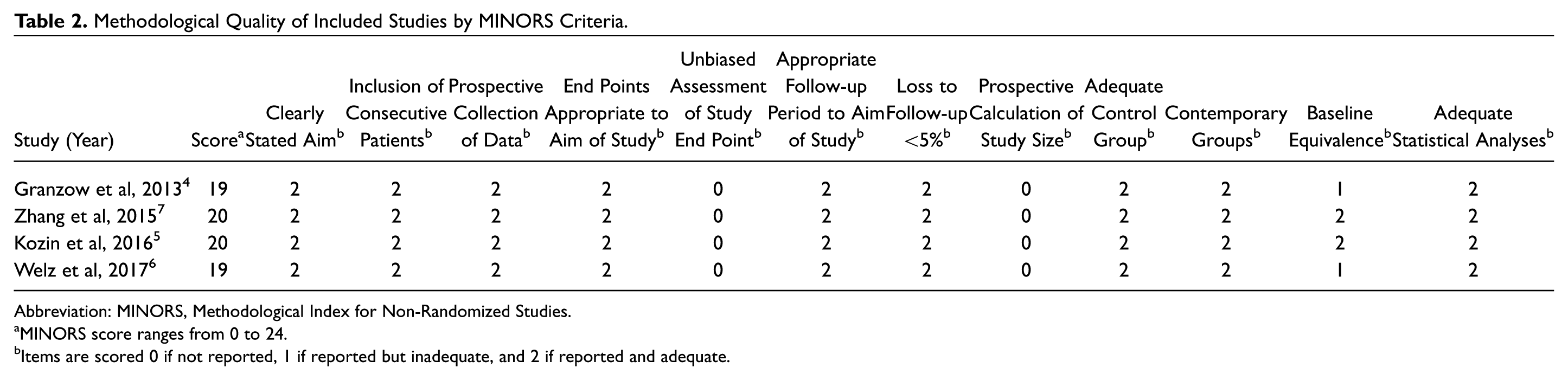
Abbreviation: MINORS, Methodological Index for Non-Randomized Studies.
MINORS score ranges from 0 to 24.
Items are scored 0 if not reported, 1 if reported but inadequate, and 2 if reported and adequate.
Operative Time
A random effects meta-analysis for operative time is shown as a forest plot in Figure 2 . Pooled, weighted mean (SD) operative times for SCAIF and FTT cohorts were 368.68 (105.4) minutes and 462.1 (113.9) minutes, respectively, with a large effect size in favor of SCAIF (diamond; SMD, –1.65; 95% CI, –2.52 to −0.78). High heterogeneity was noted (I2 = 82%).
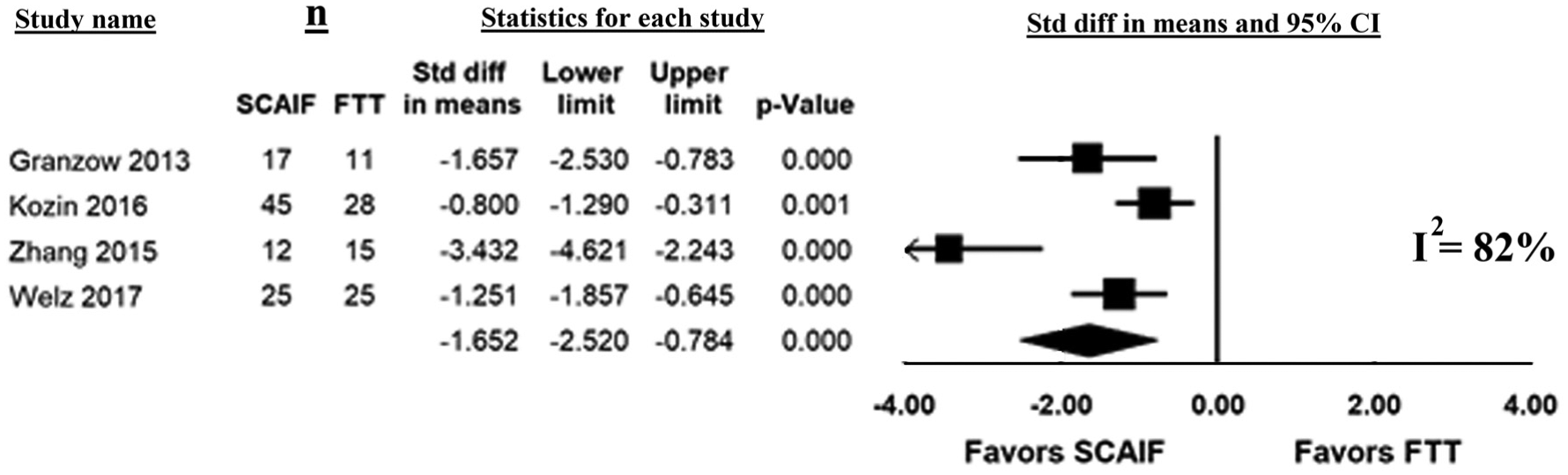
Forest plot demonstrating random-effects meta-analysis for operative time. Diamond indicates pooled SMD. CI, confidence interval; FTT, free tissue transfer; SCAIF, supraclavicular artery island flap; SMD, standardized mean difference.
Two studies performed cost analysis and found SCAIF to be significantly cheaper (P < .001) compared to FTT.5,6 Kozin and colleagues 5 demonstrated that total hospital charges for SCAIF were 32% lower overall than FTT. Welz and colleagues 6 found a cost increase of 1.7 times in their RFFF group compared to their SCAIF cohort.
Flap Characteristics
Three studies reported outcomes on harvested flap areas. Flap area was analyzed through a random-effects model, and the result is shown in Figure 3A . Pooled, weighted mean (SD) flap areas were 74.7 (32.6) cm2 and 86.2 (79.4) cm2 for SCAIF and FTT groups, respectively. FTT potentially allowed larger flap areas to be harvested; however, the CI was not able to rule out a moderate effect size in favor of SCAIF (diamond; SMD, –0.304; 95% CI, –1.30 to 0.70). Again, large heterogeneity was observed among the included studies (I2 = 88%).
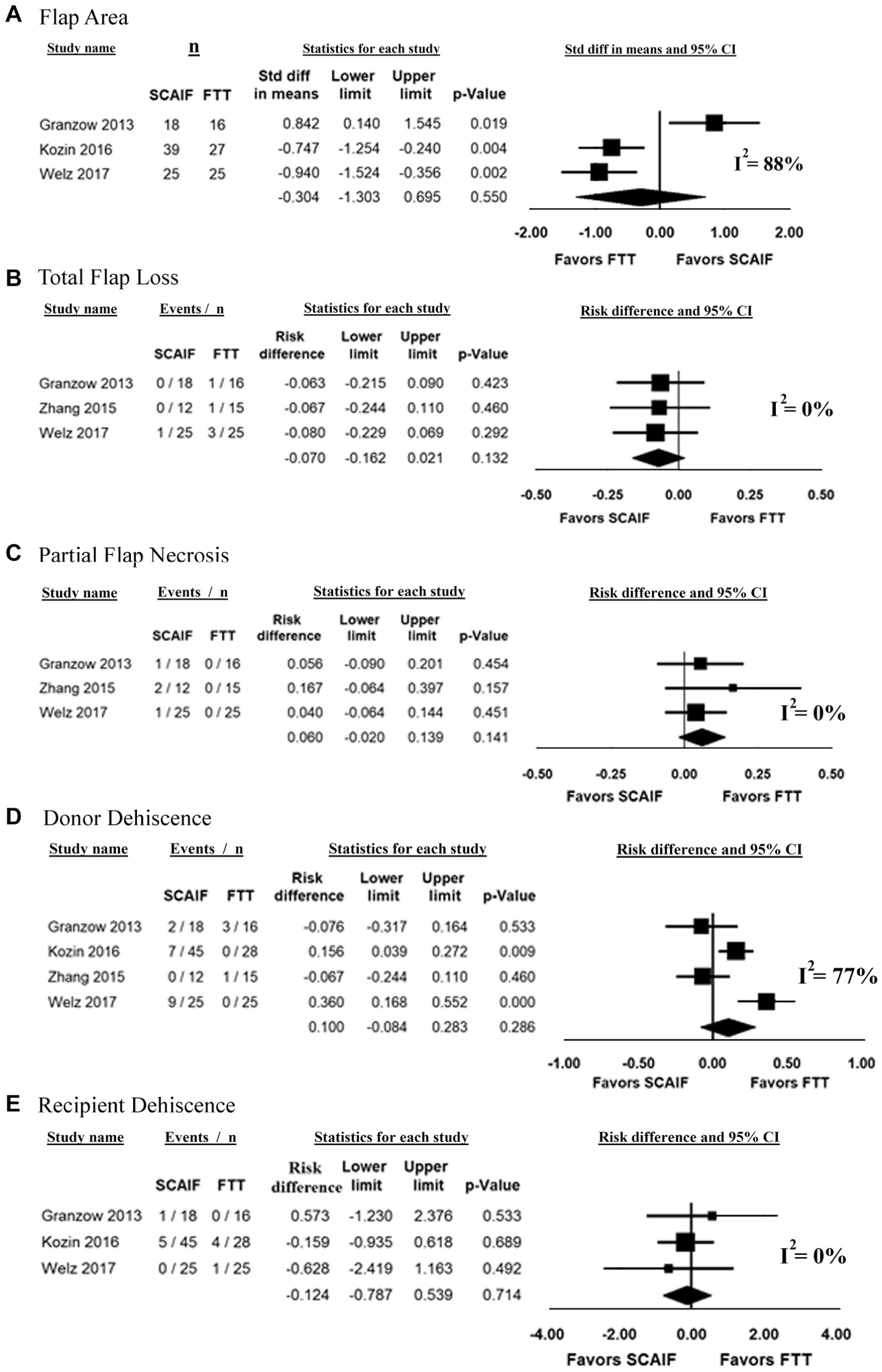
Forest plots demonstrating random-effects meta-analyses for (A) flap area, (B) total flap loss, (C) partial flap necrosis, (D) donor site dehiscence, and (E) recipient site dehiscence. Diamond indicates pooled SMD or RD. CI, confidence interval; FTT, free tissue transfer; RD, risk difference; SCAIF, supraclavicular artery island flap; SMD, standardized mean difference.
Harvested flap area was larger for FTT in 2 studies.5,6 In contrast, a larger harvest area for SCAIF was reported by Granzow and colleagues 4 (164.6 cm2 vs 110.8 cm2, P = .02).
Perioperative Outcomes
SCAIF potentially decreased total flap loss, but the effect size was small (7% RD, number needed to treat of 14) and did not reach statistical significance ( Figure 3B ). FTT may have decreased partial flap necrosis, but the effect size was small (6% RD, number needed to treat of 17) and not statistically significant ( Figure 3C ). There was no difference in outcomes for SCAIF vs FTT with regard to donor site dehiscence and recipient site dehiscence ( Figure 3D , E ). However, differences may have been missed because of low statistical power.
Several postoperative parameters were reported by individual studies but not included in the meta-analysis secondary to lack of uniform reporting. Granzow and colleagues 4 noted 2 instances of salivary leak in their FTT cohort, an esophageal leak in both groups, and esophageal stenosis in 1 patient in their SCAIF cohort. Donor site infection was reported by Kozin and colleagues 5 (2 and 4 patients in the SCAIF and FTT groups, nonsignificant difference, respectively). Recipient site infection was noted by 2 studies4,5 and found to be comparable. Welz and colleagues 6 found higher incidence of fistula after oral cavity reconstruction in their SCAIF group compared to their FTT cohort (12% vs 4%, P < .05, respectively). In that study, a higher rate of minor complications was noted in the SCAIF group, while a higher rate of major complications was noted in the FTT cohort. Last, hematoma was reported by 2 studies.4,5 No incidence of hematoma occurred in the SCAIF cohort, but both studies found no significant difference between the 2 groups.4,5
Discussion
FTT has risen to be the standard workhorse in complex head and neck reconstruction. Yet, it remains necessary to inquire on methods and techniques that can serve as alternatives to existing interventions if contraindications exist. It is important to investigate if the approach can offer equivalent outcomes, especially with regard to potential complications, expenditure of health care resources, quality of life, and the ability to complete the goals of surgical care. 34 In the pursuit of maximizing cost-effectiveness and conforming to patient comorbidities, SCAIF has emerged as a potential alternative to FTT in various indications for soft tissue reconstruction. SCAIF is robust, thin, and malleable like RFFF and can be harvested without microvascular expertise.4-10 Often, the literature surrounding novel interventions is encumbered by low power secondary to limited sample size. A systematic review and meta-analysis have the potential to overcome these drawbacks.
In our meta-analysis, we found that SCAIF reduces overall operative time by a large and highly significant effect size. This was likely attributed to the preclusion of microvascular anastomosis. This finding is consistent with other studies, where the majority of flap harvest was demonstrated to be less than 1 hour.8,9,35,36 This may have extensive implications in decreasing perioperative morbidity37,38 and reducing overall cost of care. 39 In FTT, a 2-team approach is often performed to promote time efficiency, albeit at the disadvantage of incurring additional costs. Despite this, the operative times of SCAIF remain superior for similar indications of reconstruction.
These savings were highlighted in cost analyses performed by 2 studies.5,6 Kozin and colleagues 5 found that hospital-wide charges for SCAIF were 16%, 46%, and 25% lower than FTT for cases of total laryngectomy, parotid/temporal bone resection, and cutaneous defects, respectively. The cost reduction was an amalgamation of a variety of factors, including decreased operative times, less intensive postoperative monitoring, and limited stay in intensive care units. In addition, by incorporating the costs of personnel, operative procedure, and intensive care unit stay, Welz and colleagues 6 demonstrated a statistically significant reduction of costs in favor of SCAIF.
We also found no significant difference in harvested flap area between the 2 groups; although FTT may allow for greater flap dimensions, our analysis was not able to rule out a moderate effect size in favor of SCAIF. Harvested FTT dimensions tend be larger in the included studies,5-7 and several investigators have defined the limits of SCAIF harvest. Kokot and colleagues, 8 for example, demonstrated that a flap length greater than 22 cm was significantly associated with flap necrosis. Other studies have demonstrated survival in flap lengths up to 41 cm or within 5 cm of the last audible Doppler signal after flap elevation. 10 Nonetheless, the result of our random-effects model suggests that both types of flaps have the capacity to repair similar caliber defects.
Our study also demonstrates comparable short-term perioperative outcomes for SCAIF compared to FTT. There was no significant difference with regard to total flap loss, partial flap necrosis, donor site dehiscence, and recipient site dehiscence. There was a propensity for SCAIF to have decreased total flap loss, but the effect size was small and did not reach statistical significance. Similarly, there was a predilection for FTT to have decreased partial flap necrosis, but the effect size was small and not significant. After the resurgence of the SCAIF flap, initial reports of complications revolved around distal flap necrosis, which was secondary to the investigational nature of the flap’s appropriate dimensions.8,10 This was further exemplified by the included studies, where 3 studies found partial flap necrosis to occur in SCAIF and none in FTT,4,6,7 with some cases requiring partial necronectomies. 6 In cervicofacial defects, the extent of skin paddle rotation may lead to obstruction of the vascular pedicle. Furthermore, tunneling of flap underneath a bridge of skin or deep to mandible for reconstruction of oral cavity or oropharyngeal defects may cause additional vascular compromise. 8 In contrast, 2 of the included studies found that total flap losses were more frequent in FTT, with both demonstrating absence of complete flap loss events in SCAIF.4,7 This is expected due to the nature of perfusion for FTT, which result in an all or none thrombotic event that can lead to complete flap failure. Although our analysis found no difference, sufficiently powered, larger comparative studies may be needed to further explore the perioperative advantages and disadvantages of SCAIF vs FTT.
There are several limitations to this review. The individual studies that comprised this meta-analysis were not randomized in design and were observational in nature. Each study was therefore susceptible to selection bias and was dependent upon the accuracy of medical documentation. In addition, operative time measurements were not standardized or fully described in studies. Although indications for reconstruction were relatively uniform between the 2 cohorts within 3 studies,5-7 1 study had greater variability with regard to the types of defect reconstructed. 4 Relative to each other, these 4 studies had distinct indications for reconstruction, which may explain the extended degree of heterogeneity observed among certain surgical outcomes. Different ablative and traumatic etiologies can result in varying defects and may affect choice and the dimensional parameters of the harvested flaps, dampening confidence in the homogeneity of our pooled data. Given the limited amount of study in this systematic review, no stratification was performed by indication or type of defect. We included all types of indications for reconstruction, and there was no attempt to reclassify these indications for our statistical analysis.
Given the elevated heterogeneity parameter, the random-effects model was appropriately used in this setting; the model provided wider CIs and gave additional weight to smaller studies. In addition, the increased heterogeneity was partially mitigated by the encouraging quality of the involved studies.
In summary, this is the first meta-analysis that pooled comparative outcomes between SCAIF and FTT. We found that SCAIF significantly reduces operative time by a large margin compared to FTT and that short-term perioperative outcomes are comparable between the 2 types of reconstructive options. Both procedures should be viewed as reasonable for defects within the reach of the SCAIF pedicle. Surgeons have different levels of comfort with various flaps, and the decision for when to use which should not be dictated solely by the potential cost savings of SCAIF relative to FTT. This systematic review reinforces the idea that SCAIF is a safe option for thin soft tissue reconstruction and should be included in reconstructive decision making after major head and neck ablation or trauma. In addition, the findings of this study may provide a basis for clinical counseling and a framework for future studies. In particular, studies with large cohorts, randomized in design, in the setting of uniform indications, will be necessary.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.
This article was presented at the 2018 AAO-HNSF Annual Meeting and OTO Experience; October 7-10, 2018; Atlanta, Georgia.