
Abstract
Objectives
To study optimal head position after intratympanic steroid injections to enhance drug bioavailability.
Study Design
Application of virtual and in vitro models of the intratympanic anatomy.
Setting
The surgical 3-dimensional printing laboratory of a tertiary academic medical center.
Subjects and Methods
A high-resolution computerized tomographic scan of healthy temporal bone and surrounding soft tissue was segmented and reconstructed to a 3-dimensional model. The tympanic membrane was perforated in the posterior-inferior quadrant. Methylene blue–stained 10-mg/mL dexamethasone was administered to the middle ear cleft, after which a 3-dimensional rotation in space was performed to hypothesize the optimal position in relation to gravity. The same stereolithography file used for the actual model was used for a digital virtual liquid flow simulation. The optimal head position was defined as the one with the maximum vertical distance between the round window membrane and the plane of the aditus ad antrum and eustachian tube orifice.
Results
The virtual model yielded the following position of the head as optimal: 53º rotation away from the injected ear in the vertical axis (yaw), 27º rotation toward the noninjected ear in the longitudinal axis (roll), and 10º neck extension in the transverse axis (pitch).
Conclusions
Virtual imaging determined that 53º and 27º yaw and roll, respectively, away and 10º pitch were the optimal position for drug delivery after intratympanic injection to the middle ear and that an erect head position provided optimal passage of steroids from the middle ear to the inner ear.
Intratympanic injection of steroids has become a widely used route for the treatment of idiopathic sudden sensorineural hearing loss (ISSNHL) and Ménière’s disease (MD). The mechanism of action of steroids in the inner ear is unclear. In a study by Parnes et al, 1 a higher inner ear concentration of steroids was achieved via the intratympanic method as compared with oral and even intravenous routes in a guinea pig model. In recent years, the intratympanic route—in which the steroidal solution is administered to the middle ear via perforation of the tympanic membrane and left to passively diffuse through the round window membrane (RWM)—has become an alternative as a salvage therapy or when oral administration is contraindicated. 2
The steroids enter the cochlea through the RWM. 3 The laws of diffusion dictate that the diffused material is directly proportional to the time that it is left to diffuse if no steady state has been reached, thus highlighting the importance of maintaining the injected steroids in the round window (RW) niche. Three major mechanisms control the final amount of therapeutic drug that will be in contact with the RWM: loss in the eustachian tube (ET), loss in the mastoidal air cells (MACs), and transmucosal loss. 4
The RWM is not the sole entrance of active drugs to the inner ear. Passive transport can be achieved by diffusion across the annular ligament of the stapedial footplate and possibly through microfracture of the otic capsule. The discussion on inner ear drug transport can be further complicated by the fact that absorption across the RWM is not necessarily based on concentration gradients alone and is more complicated, including active transport mechanisms (ie, pinocytic vesicles) across this membrane with individual variations for membrane transport potential. However, the presence of hypotympanic air cells or air cells in the sinus tympani might also allow for drainage of the steroid away from the RWM. Additionally, mucosal webs within the RW niche can mechanically prevent any steroid from reaching the RWM. This is actually a relatively common histopathologic finding that was quoted as possibly being present in nearly 50%. 5
Several studies searched for methods to enhance the effectiveness of intratympanic steroid administration by using micro-catheters, 6 micro-wicks, 7 prolonged drug delivery through means of gel-based formulation, 8 and RW vibration to increase permeability 9 and by increasing the time that the patient is in the supine position after treatment. There is no uniform protocol among clinics, but the patient is usually instructed to remain in the supine position with the head rotated at an angle of 45° to the unaffected side and to refrain from saliva swallowing, speaking, or moving the head. Continuous oral suction is usually carried out during the procedure.
The optimal head position for reducing the loss of injected material in the ET and MACs has never been studied. The aim of this study, therefore, was to apply virtual and in vitro models to determine the optimal head position for the patient to maintain after intratympanic injection of steroids to enhance drug bioavailability.
Methods
The study was approved by the research ethics committee of the Sourasky Medical Center, Ichilov Hospital (0810-16-TLV). The optimal head position for intratympanic injections of steroids was defined by the one in which the aditus ad antrum and the ET opening are aligned on an imaginary plane parallel to the ground (perpendicular to the gravitational vector) and the RW is below this plane to its maximal vertical distance as possible ( Figure 1b ). Head positions that are not compatible with normal body and head positions were excluded.
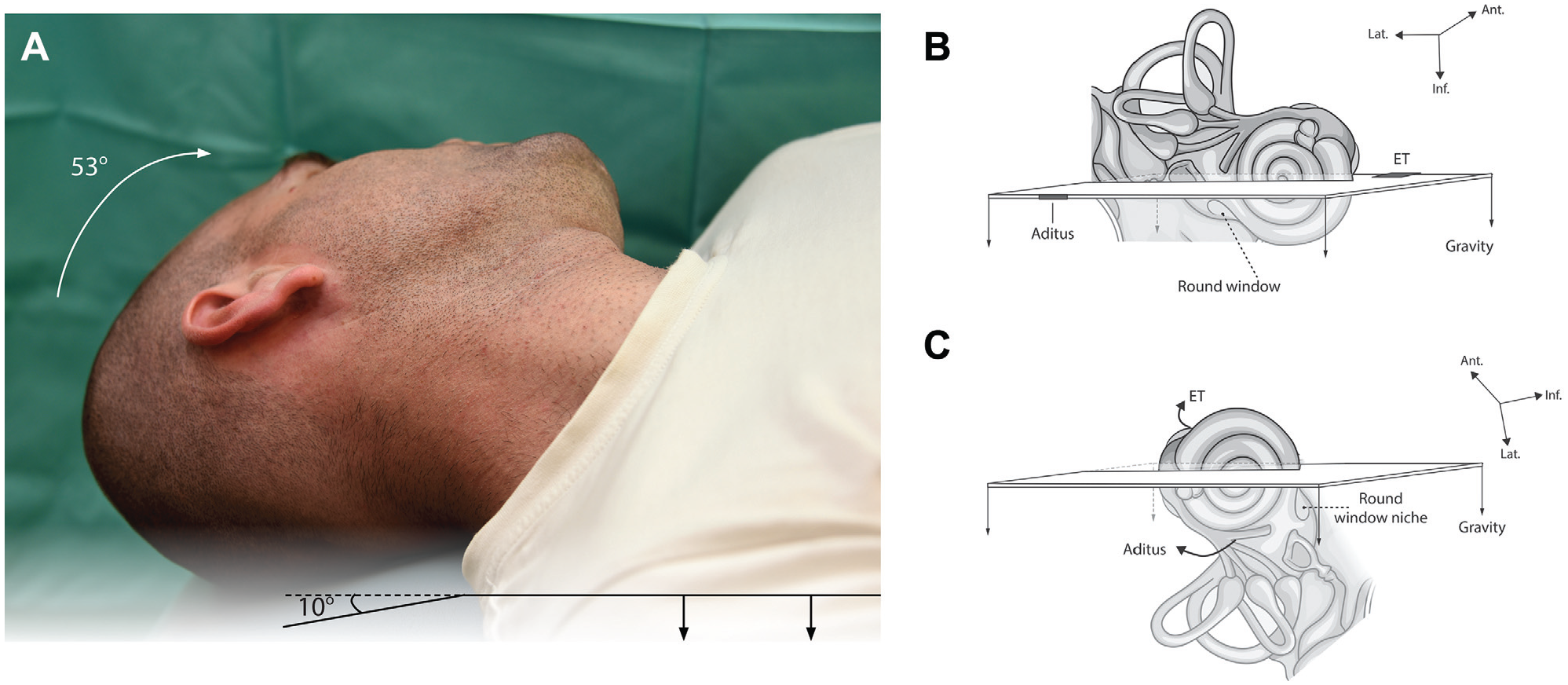
(A) Optimal orientation for intratympanic injections in terms of anatomic relationship among the eustachian tube (ET), aditus ad antrum, and round window. Depicted head position is after 53° rotation. A scheme representing the otic capsule in (B) standing position and (C) its optimal orientation.
The 3-Dimensional Model
A high-resolution computed tomography scan (section thickness, 0.9 mm) of the left temporal bone and surrounding soft tissue of an 85-year-old healthy woman was segmented and reconstructed to a 3-dimensional (3D) ear model with Mimics segmentation software (Materialise, Louvain, Belgium). The locations of the RW, aditus ad antrum, and proximal end of the ET were marked on the scan ( Figure 2 ). The 3D model was then designed as a stand-alone piece for fluid testing with 3-Matic CAD software (Materialise). It was printed on a 1:1.5 scale with stereolithography technology (Formlabs, Somerville, Massachusetts) by 100-μm layers of Clear Resin 1 L. A model framework thickness of 2 mm was used to ensure a watertight seal of the middle ear cleft (MEC) contour. Transparency assisted in visual evaluation of the dispersion of fluid ( Figure 3 ).
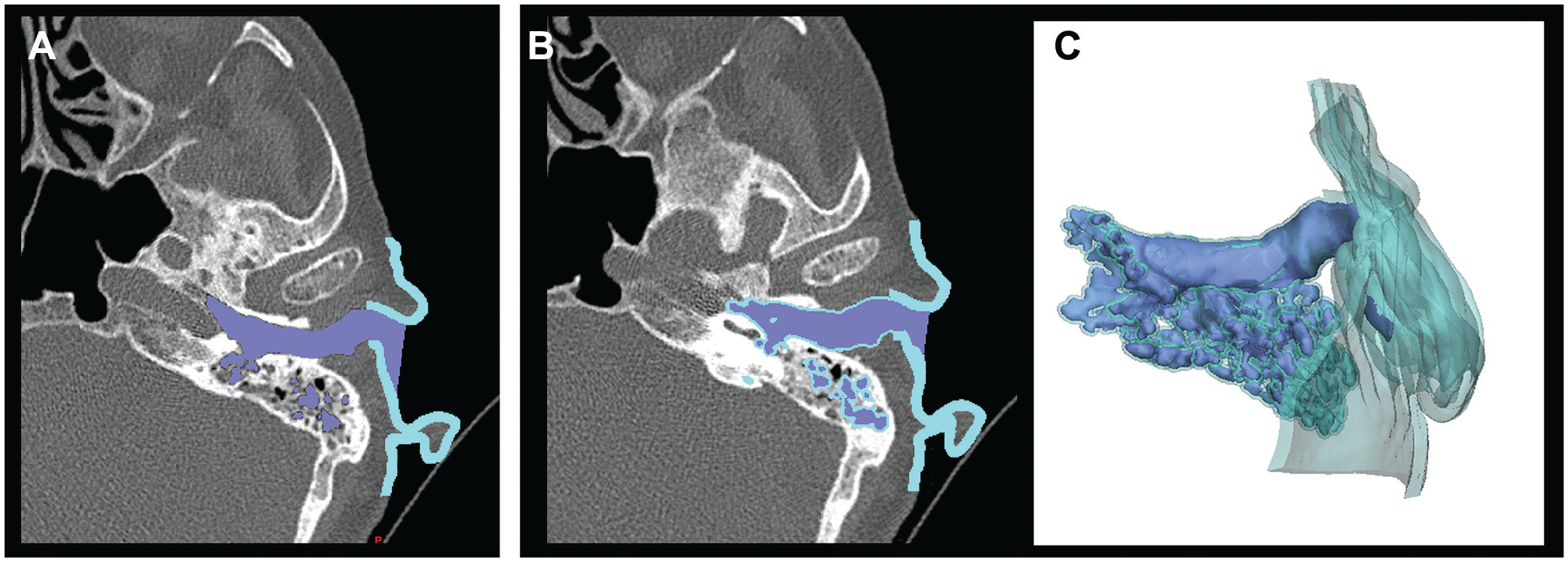
The actual model design. Light blue, skin; mauve, injected methylene blue; turquoise green, auricle. (A) Model segmentation. (B) Two-millimeter offset of the middle ear cleft defined the cavity for investigation. (C) The ready-to-print model.
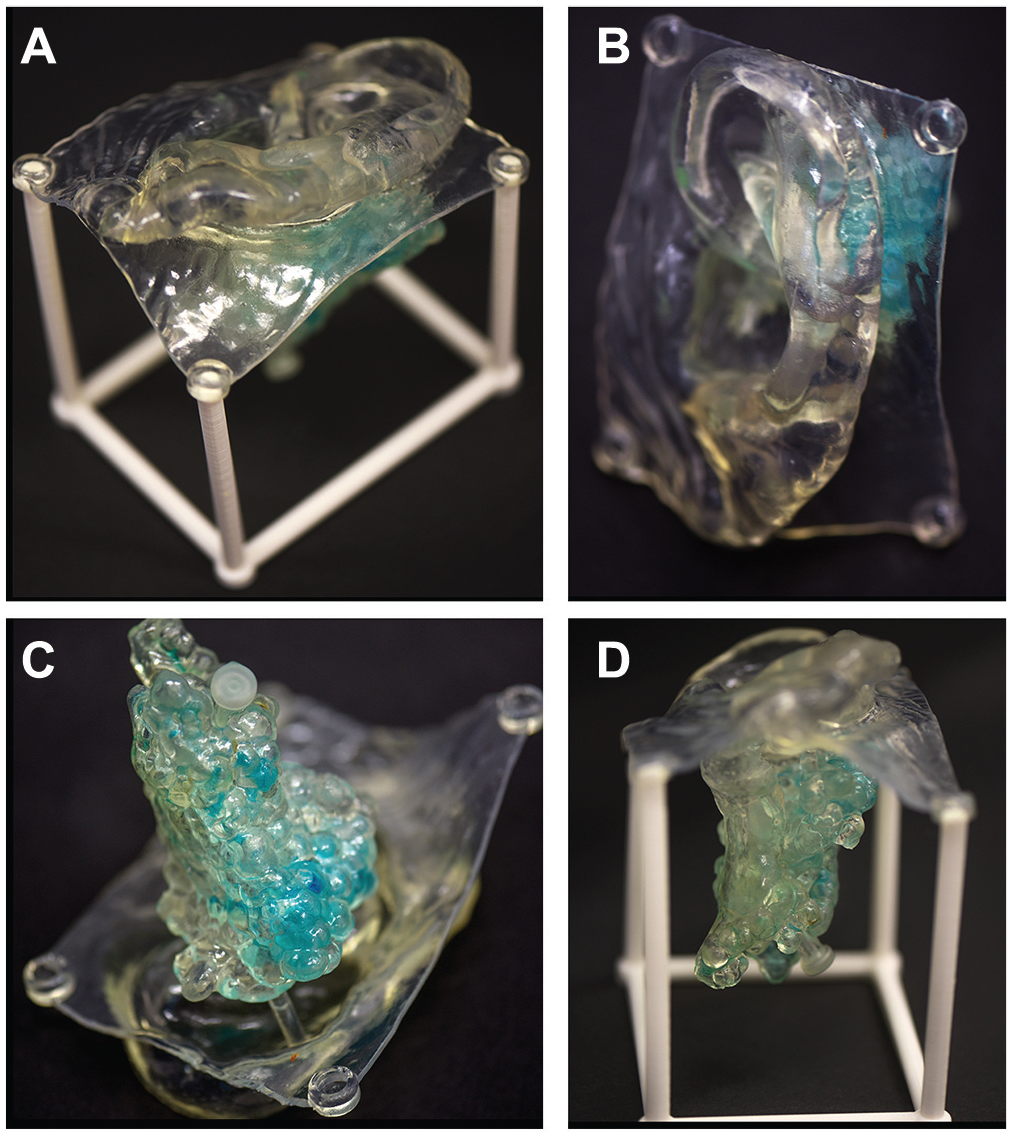
The final actual model. (A) Inferior-lateral view. The auricle and the chassis are visualized. (B) Lateral view. (C) Medial view. The mastoidal air cell system and the pluggable draining aperture are visualized. (D) Inferior view showing the mastoidal air cell system.
The tympanic membrane was perforated in the posterior-inferior quadrant, and 0.8 mm and 1.0 mm of methylene blue–stained 10-mg/mL dexamethasone were administered to the MEC by means of a 1.5-mL syringe connected to a 22G disposable spinal needle. After fluid administration, a 3D rotation of the model in space was performed to define the optimal position in relation to gravity. The fluid was drained from the printed MEC through a preprinted pluggable draining aperture in the mastoid tip ( Figure 3C ).
The Virtual Model
The same stereolithographic file used for the actual model was used for a digital virtual liquid flow simulation with Maya Autodesk Bifrost simulation software (Autodesk, Inc, San Rafael, California). After physical liquid parameters (ie, viscosity, specific gravity, volume, and flow pressure) were uploaded to the software, flow simulation was performed digitally in a wide range of ear orientations in relation to gravity. Final visual evaluation of the fluid dispersion was made according to the locations of the RW, aditus ad antrum, and proximal end of the ET ( Figure 4 ). The printed model and the digital simulation were meticulously compared to ensure a reliable virtual reality.
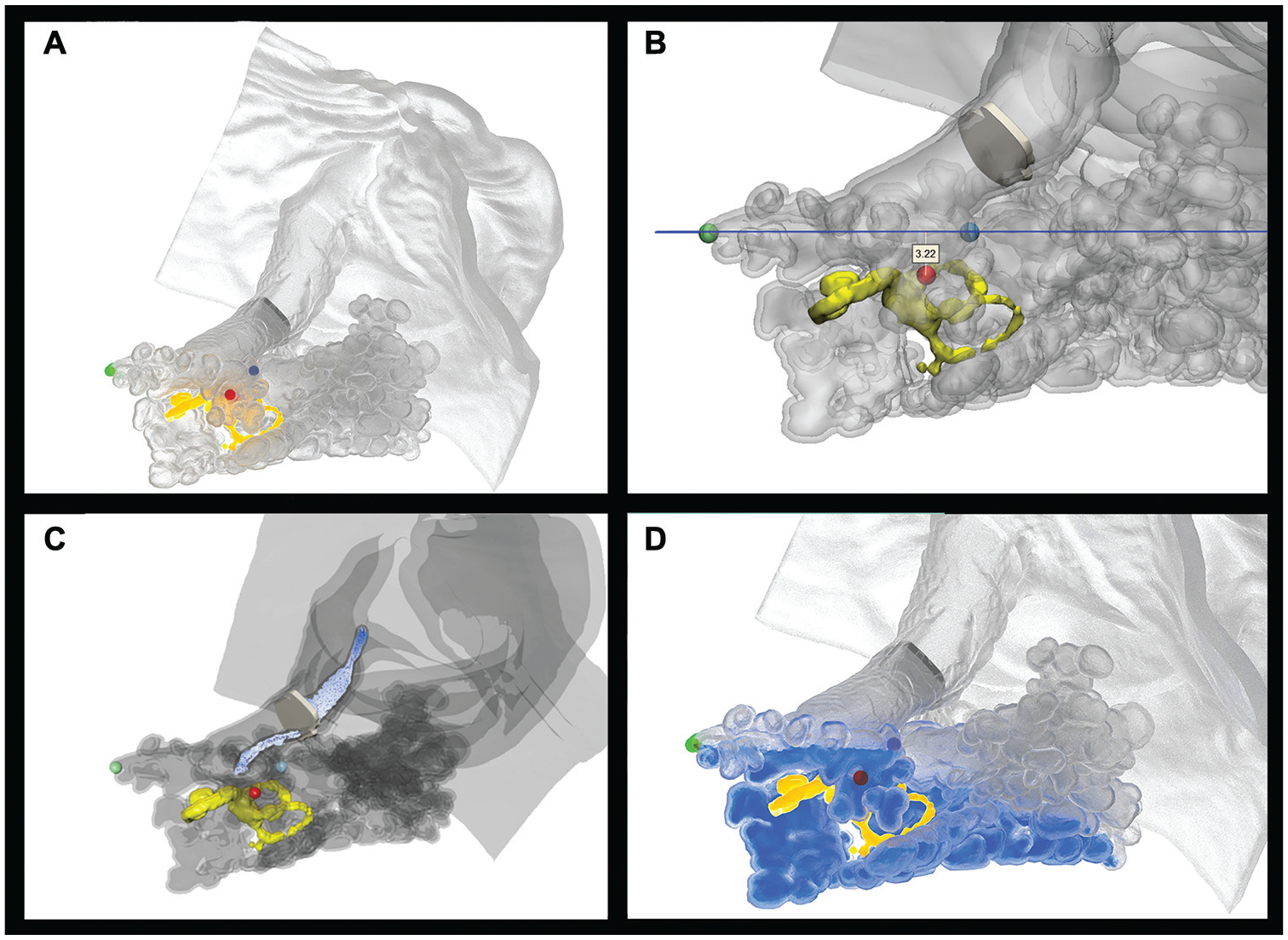
Eustachian tube orifice, aditus ad antrum, and round window (green, blue, and red, respectively). (A) Before injection. (B) Maximal vertical distance between the round window and the orifice plane of the aditus ad antrum and eustachian tube, parallel to the ground. (C) Intratympanic and (D) 0.7-mL injection simulation.
Results
The MEC volume of the actual model measured 9.6 mL. The actual model scale was printed in a 1:1.5 scale, and the standardized 1:1 MEC volume was calculated to be 2.8 mL. This result was overestimated by the virtual model (3.2 mL). The difference between the calculated and measured volumes is the result of the technical difficulty of extracting all the supportive material volume (used as airspace filler during printing) from the MEC after 3D printing, mainly from the MAC system.
The printed model provided a watertight sealing of the MEC and enabled a wide positional range in space after intratympanic fluid administration. By freehand rotation of the model, the optimal model positioning was achieved when the model was rotated from the natural (supine) position 60° around the vertical axis (yaw) away from the injected ear and 30° around the longitudinal axis (roll) toward the shoulder of the noninjected ear. No rotation around the z-axis (pitch) was needed. Validation of the measurements by the virtual model yielded slight differences of the optimal model positioning (
Vertical axis (yaw): 53° rotation away from the injected ear
Longitudinal axis (roll): 27° rotation toward the noninjected ear
Transverse axis (pitch): 10° neck extension
The angular safety of the optimal position was defined by the degree of freedom to which the subject can rotate in each plane while keeping the RW below the aditus ad antrum and the ET. It was measured by the virtual model and found to be 12°, 9°, and 4° in the vertical, longitudinal, and transverse axes, respectively.
This virtual model–based optimal position localizes the aditus ad antrum and the ET orifice in the horizontal plane, as well as the RW 3.22 mm below it ( Figure 5 ). The maximal effective intratympanic volume needed for optimal diffusion through the RW was 1.2 mL. An erect position (in which the Frankfort horizontal plane is perpendicular to the axis of gravity) was predicted from our virtual model as another effective option in which the aditus ad antrum, the ET orifice, and the tympanic membrane injection site were all well above the RW (ie, a vertical distance up to 2.0 mm).
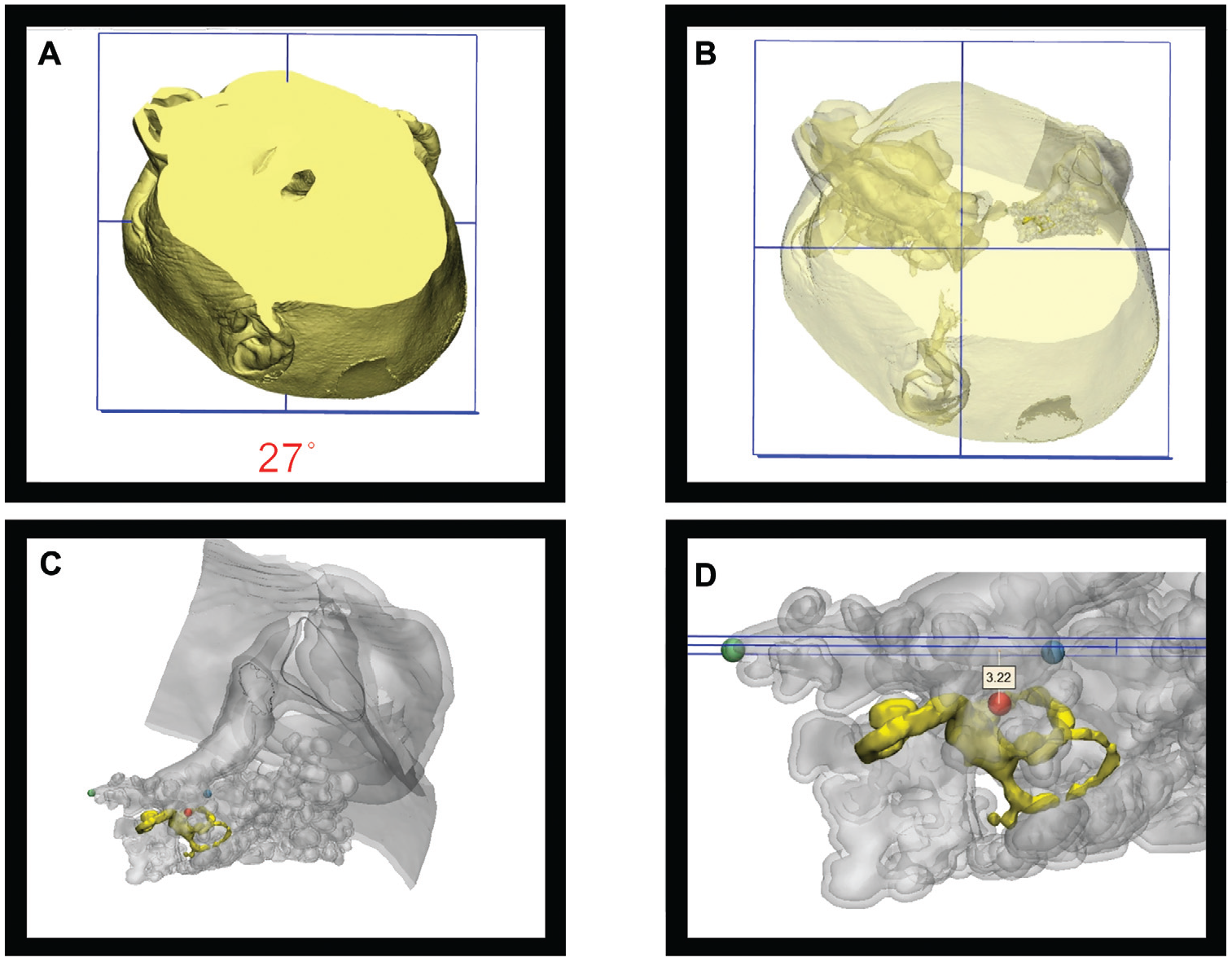
(A) Optimal head positioning for round window maximal hydrostatic pressure. (B) Same alignment with visualization of middle ear components. (C) Magnification of the virtual model in the optimal head positioning. (D) The membranous labyrinth related to the aditus ad antrum, eustachian tube orifice, round window.
Discussion
ISSNHL and MD are debilitating diseases for some patients, affecting many of the fundamental aspects that determine their quality of life. The increasing frequency of the use of intratympanic steroids for both conditions has made the optimal delivery of steroids to the inner ear a critical issue. Data on intratympanic injection of steroids have shown that high concentrations of steroids reach the inner ear by means of this technique. 10
After the injection of steroids to the middle ear, the patients are instructed to lie in a supine position with the aims of minimizing the loss of fluid to the ET and to the antrum and concentrating the fluid at the RW niche. The patients are usually required to remain in the supine position for around 30 minutes, although it was suggested that a shorter period may suffice. 11 This position is uncomfortable for the patients. It also prolongs their treatment time and lengthens the time that they occupy the examination chair in the clinic.
Advances in 3D and computerized models in recent years have led to the simulation of several otologic conditions.12-14 Due to the lack of direct access to the middle ear after a therapeutic injection, such a model can add valuable information regarding the treatment of ISSNHL and MD through intratympanic injections of steroids.
In this study, we simulated the middle ear after the injection of fluids to hypothesize the optimal position in which a minimal amount of fluid will be lost and a maximum amount will be delivered to the inner ear. The results showed that this position is reached when the head is rotated 60° away from the injected ear around the vertical axis and 30° around the longitudinal axis toward the side of the noninjected ear. The model also revealed that an erect position is an effective option. That finding is important, since it can shorten the time that patients are required to lie supine, thereby increasing their satisfaction, reducing their discomfort, and shortening the time that they occupy the examination chair in the clinic.
The main limitation of this study is the use of a model rather than an in vivo investigation, since it is impossible to similarly measure the optimal position on patients. The advancements in 3D models, however, enable very accurate reproduction of the real-life situation, which has important implications regarding patients’ treatment. Another limitation derives from the fact that this study is based on a single temporal bone scan and anatomic variations were not taken into consideration. This study, however, describes a novel technique to consider in future work. The clinical benefit is yet to be proved.
To the best of our knowledge, this is the first study to demonstrate and measure the exact position that would achieve the optimal delivery of steroidal treatment by means of intratympanic injections. This information may be used by physicians to enhance the efficacy of treatment given to patients with ISSNHL or MD, improve their comfort, and shorten the time that they occupy the examination chair. Improved clinical outcome for this advocated temporal bone position still awaits results of controlled studies.
Conclusions
The optimal position for intratympanic delivery of steroids to the middle ear based on the findings of virtual and in vitro models is described. In addition, an erect head position was found to be sufficient for optimal passage of steroids from the middle ear to the inner ear.
Author Contributions
Disclosures
Footnotes
No sponsorships or competing interests have been disclosed for this article.