
Abstract
Objectives
To examine clinical profile and outcomes of elderly patients (65-90 years) undergoing head and neck surgeries in the United States.
Study Design
A retrospective cross-sectional analysis.
Setting
The Nationwide Readmissions Database, 2010 to 2015.
Subjects and Methods
Adult (≥18 years) patients who underwent head and neck surgeries. Analysis included χ2 test and logistic analysis.
Results
A total of 113,602 and 32,580 patients <65 and ≥65 years old, respectively, were included. Patients ≥65 years old were more likely to have multiple comorbidities (62.8% vs 32.6%, P < .001) and to present with head and neck cancer (19.8% vs 11.4%, P < .001). The most common comorbidity was diabetes (21.0%). The most common cancer types by site were mouth (29.12%), thyroid (28.08%), and nonmelanoma skin cancer (13.22%). The percentage of geriatric patients who underwent head and neck surgeries increased from 21.8% in 2010 to 25.0% in 2015 (P < .001). A total of 5450 (16.85%) patients developed postoperative complications, and the most common complications were pulmonary related (10.55%), bleeding (6.96%), acute renal failure (6.01%), and infection (3.97%). Blood transfusion was required in 3.53% of the patients. Readmission prevalence was 0.32%, and mortality risk was twice as likely (odds ratio, 2.05; 95% confidence interval, 1.77-2.38; P < .001). Independent risk factors of mortality were older age, multiple comorbidities, type of surgery, blood transfusion, and tracheostomy (P < .05, each).
Conclusion
Elderly patients currently represent 25% of patients admitted for head and neck surgery. This population should be provided with a different level of care due to a higher risk of complications and mortality.
The population landscape of medicine is constantly evolving. By 2030, almost 20% of patients will be elderly, age 65 years and older. 1 This has significantly increased from 9% in 1960. 1 Worldwide, life expectancy is over 70 years and is expected to rise to 77 years in 2045 to 2050. 2 In addition, the elderly population consumes relatively more health care resources than patients <65 years old. 1 Treatment of this group can often be a challenge due to comorbidities, polypharmacy, social issues, and disabilities. 3 Consequently, as the demographics of the population shift, an emphasis should be placed on elderly patients.
From this change in the population demographics, it is expected that head and neck surgeons will increasingly care for elderly patients. Disease presentation in the ambulatory setting and treatment strategies will continually change as the population of patients undergoing head and neck surgeries is composed of more elderly patients. To date, there remains a relative paucity of data regarding treatment outcomes among elderly patients undergoing head and neck surgeries. Furthermore, treatment algorithms are often adapted from younger patients as the elderly do not constitute a large portion of clinical trial participants. 4 Some strides have been made to improve understanding of this cohort, including establishment of the American Society of Geriatric Otolaryngology in 2007. 5
The objective of the current study was to examine the presentation and treatment outcomes of elderly patients who underwent head and neck surgery. In this analysis, we examined clinical and demographic risk factors associated with postoperative complications and mortality in this elderly population.
Methods
This study is a retrospective cross-sectional analysis using the Nationwide Readmissions Database (NRD) for the years 2010 to 2014. 6 The NRD is a part of the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality. 6 The NRD is a unique and powerful database designed to support various types of analyses of national readmission rates for all payers and the uninsured. 6 The database includes discharge data from 27 geographically dispersed states, accounting for 57.8% of the total US resident population and 56.6% of all US hospitalizations. 6 In addition, the database allows for weighted analysis that has been used in this project to provide a better estimation of national outcomes. 6 The NRD tracks patients across the sampled hospitals within a calendar year for any readmission. 6 This database addresses a large gap in health care data—the lack of nationally representative information on hospital readmissions for all ages. 6 The NRD consists of publicly available deidentified data that do not meet the criteria of human subject research and do not meet the criteria of review by the University of Iowa Institutional Review Board.
The main objectives of the study are to examine the presentation and outcomes of patients ≥65 years old who underwent head and neck surgeries. Patients <65 years old who underwent comparable procedures were considered a reference group. The study population included adult patients (≥18 years) who underwent head and neck surgeries as a primary admission procedure (see Appendix A in the online version of the article) classified by site of surgery into thyroid, parathyroid, ear, nose/paranasal sinuses, mouth/tonsil, salivary gland/ducts, pharynx/larynx, and maxillofacial bone/mandible. The extracted sample was then surveyed based on the age of the patients at admission and classified into 2 broad categories: <65 (controls) vs ≥65 years old (cases). Patients who were 65 years and older were further classified into 65 to <70, 70 to <80, and 80 to 90. The latter classification was used when examining the elderly population separately. Patients older than 90 years were not included as their sample size is <10 patients and the data-using agreement prohibited reporting on a very small sample size. All admissions were checked for completeness of data. Admissions with missing values for the study parameters were excluded.
Outcomes of interest included (1) postoperative complications as previously described, 7 (2) risk of requiring blood transfusion (not reported, reported), (3) risk of requiring tracheostomy (not reported, reported), (4) risk of readmission within 30 days postoperatively, (5) inpatient mortality risk within 30 days postoperatively, (6) total length of hospital stay (LOS) in days, and (7) cost of health services provided during the admission—the database includes hospital charges associated with each admission as well as cost-to-charge ratio determined for each hospital that allows conversion of charges values to cost values; all cost values were adjusted for inflation rate to reflect 2018 US dollar value using Bureau of Labor Statistics inflation calculator.6,8
The independent factors that were assessed for their association with age included (1) sex: male, female; (2) modified Charlson comorbidity index score (CCIS), classified into 0, 1, and ≥29; (3) diagnosis of a head and neck cancer and the site of cancer, if present; (4) history of radiotherapy; (5) history of chemotherapy; (6) burn as the indication for admission; (7) trauma as an indication for admission; (8) site of the primary procedure based on the International Classification of Diseases, Ninth Revision (ICD-9) codes (see Appendix A in the online version of the article); (9) neck dissection: performed, not performed; (10) hospital volume, defined as the number of head and neck surgeries performed in each hospital per year, classified by applying quartile classification with rounding to the nearest 10 to avoid introducing bias, with the classification including low-volume hospitals (<25th percentile: 1-30 surgeries/year), intermediate-volume hospitals (25th to <75th percentiles: 31-140 surgeries/year), and high-volume hospitals (≥75th percentile: ≥141 surgeries/year); and (11) location and type of hospital as coded in the database into metropolitan nonteaching, metropolitan teaching, and nonmetropolitan. 6
Statistical analysis used weighted data to reflect national estimates. The records’ weights are available in the NRD and calculated based on the stratification variables that were used in the sampling methodology. 6 Cross-tabulation and χ2 test were used to examine the association between each of the independent factors and the outcomes of interest. Variables that demonstrated a significant association with the outcomes were considered possible confounders and were included in multivariate logistic regression models. Odds ratio (OR) and 95% confidence interval (CI) were calculated from multivariate logistic regression models. Multivariate linear regression models were used to compare means of LOS and cost of health services while controlling for confounders. Significance level was set as α = .05. All data analyses were performed using SAS 9.4 for Windows (SAS Institute, Cary, North Carolina).
Results
A total of 113,602 patients <65 years old and 32,580 patients ≥65 years old were included ( Table 1 ). There was a significant increase in patients ≥65 years old undergoing head and neck surgeries from 21.8% in 2010 to 25.0% in 2015 (P < .001). Comorbidities were prevalent in patients ≥65 years old (75.45% had at least 1 comorbidity); the most common comorbidities were diabetes (23.2%), chronic pulmonary diseases (16.64%), renal diseases (8.05%), and congestive heart failure (6.53%) ( Figure 1 ). Compared to patients <65 years old, older patients were more likely to be admitted for oncological surgery (19.79% vs 11.40%, P < .001); the most common malignancies were oral cavity (29.12%), thyroid (28.08%), and nonmelanoma skin cancers (13.22%). Patients 65 years or older were less likely to be admitted due to trauma than younger patients (9.45% vs 20.32%, P < .001). The most common performed procedures by site in patients ≥65 years old were thyroid (28.21%), pharynx/larynx (14.00%), parathyroid (12.13%), nasal cavity/paranasal sinuses (11.85%), and mouth/tonsil (11.61%). In addition, elderly patients were more likely to undergo concomitant neck dissection (8.70% vs 2.98%, P < .001).
Descriptive Statistics of the Study Population, National Readmission Database, 2010 to 2015.
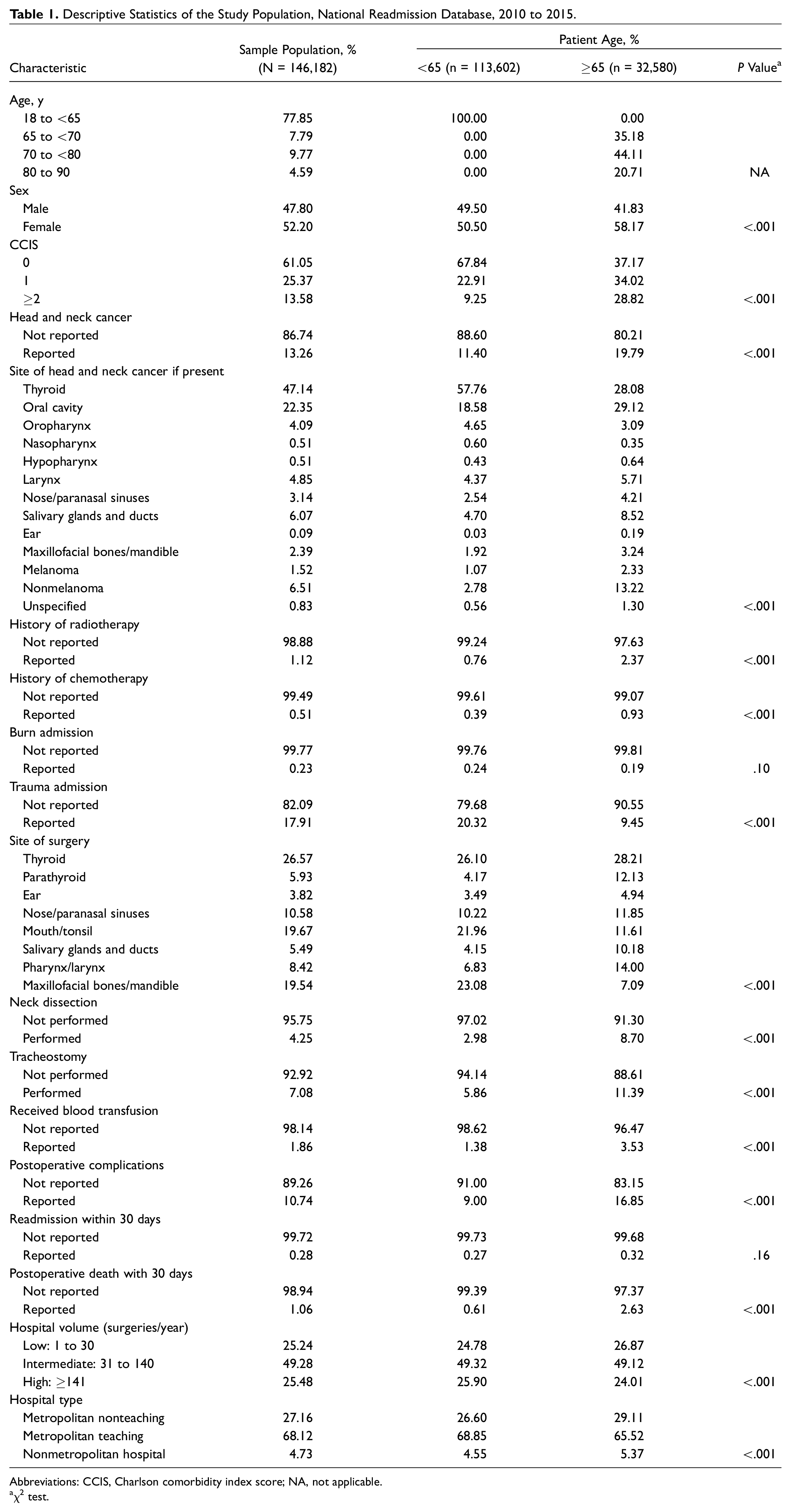
Abbreviations: CCIS, Charlson comorbidity index score; NA, not applicable.
χ2 test.
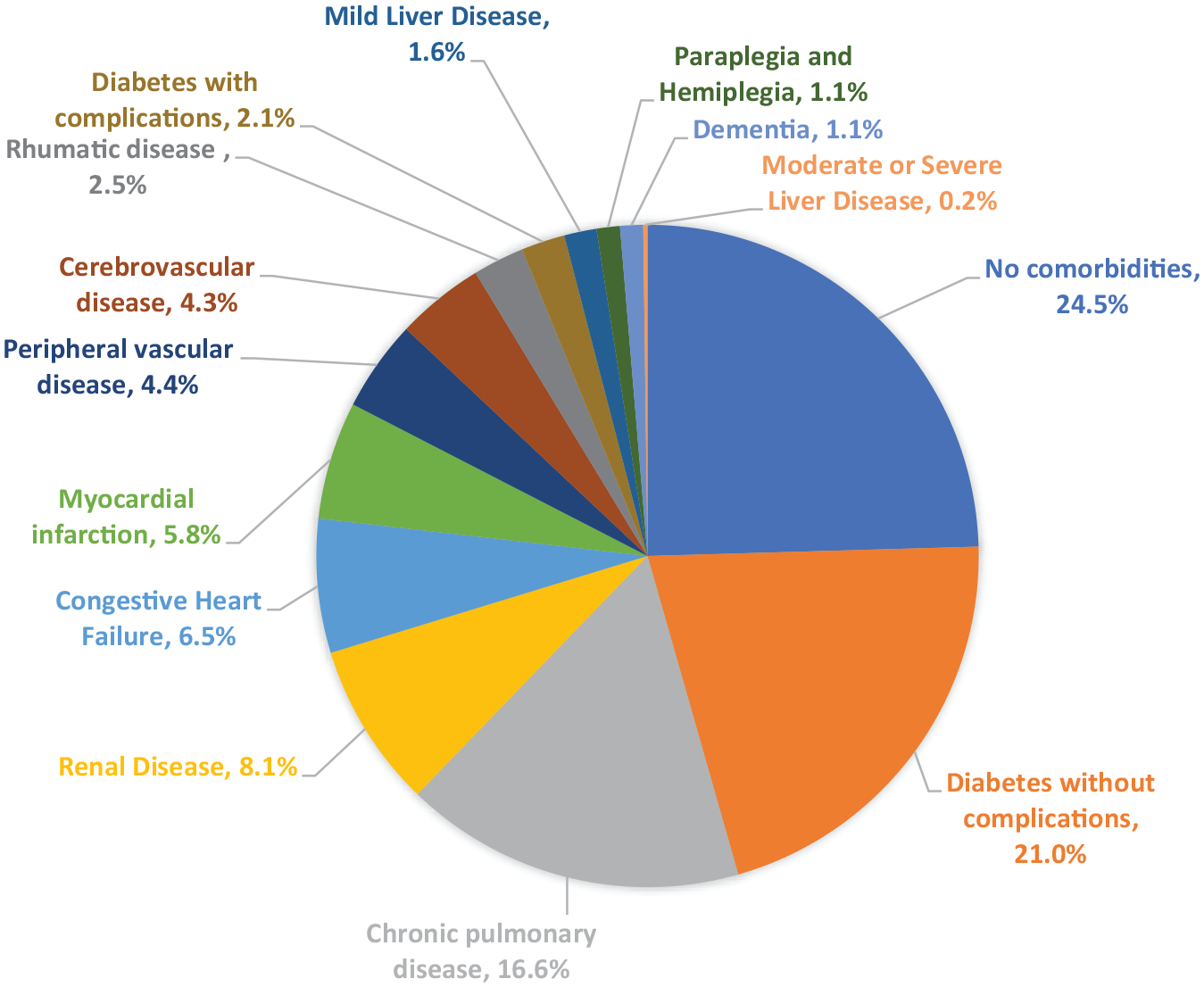
Distribution of comorbidities in patients ≥65 years old who underwent head and neck surgeries.
Postoperative complications in the adjusted analysis were significantly higher in elderly patients (OR, 1.49; 95% CI, 1.41-1.58; P < .001) ( Table 2 ). The most common complications were pulmonaryrelated (10.55%), bleeding (6.96%), acute renal failure (6.01%), infection (3.97%), and cardiovascular complications (1.34%) ( Figure 2 ). Elderly patients were also more likely to require blood transfusion (OR, 1.59; 95% CI, 1.43-1.75; P < .001) and tracheostomy (OR, 1.13; 95% CI, 1.03-1.25: P = .009). Postoperative mortality risk within 30 days was twice as likely in patients ≥65 years old (OR, 2.05; 95% CI, 1.77-2.38; P < .001). Overall, among patients ≥65 years old, the older they were in age, the higher the risk of postoperative complications, blood transfusion, tracheostomy, and mortality ( Figure 3 ). There was no significant difference in length of hospital stay and readmission risk when comparing patients aged ≥65 to <65 years. The cost associated with the health care provided was significantly higher for patients <65 years old, but the difference is not financially meaningful in terms of cost of health services (<$1000).
Risk of Selected Postoperative Outcomes for Patients Aged >65 Years vs ≥65 Years.
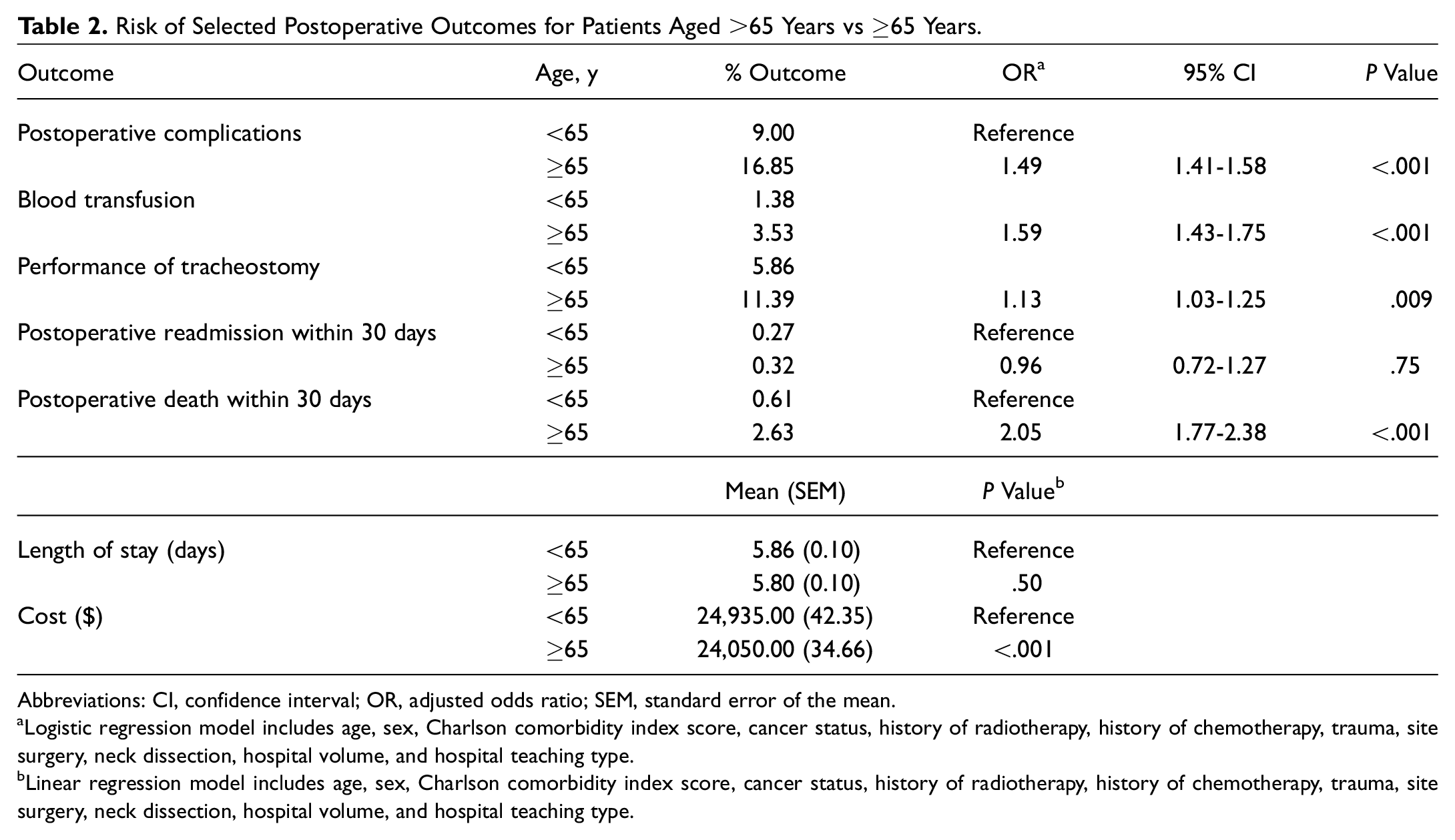
Abbreviations: CI, confidence interval; OR, adjusted odds ratio; SEM, standard error of the mean.
Logistic regression model includes age, sex, Charlson comorbidity index score, cancer status, history of radiotherapy, history of chemotherapy, trauma, site surgery, neck dissection, hospital volume, and hospital teaching type.
Linear regression model includes age, sex, Charlson comorbidity index score, cancer status, history of radiotherapy, history of chemotherapy, trauma, site surgery, neck dissection, hospital volume, and hospital teaching type.
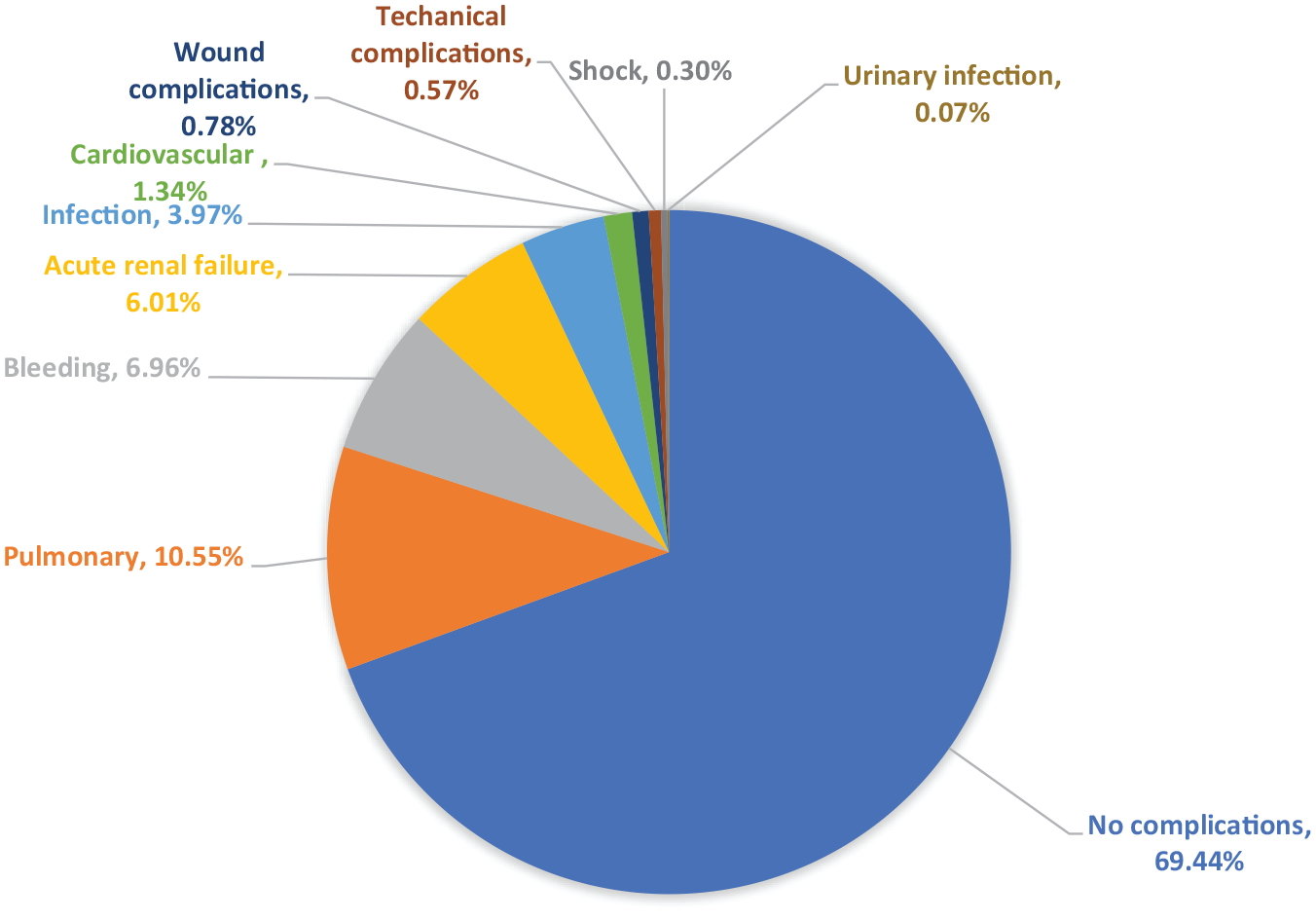
Distribution of postoperative complications in patients ≥65 years old who underwent head and neck surgeries.
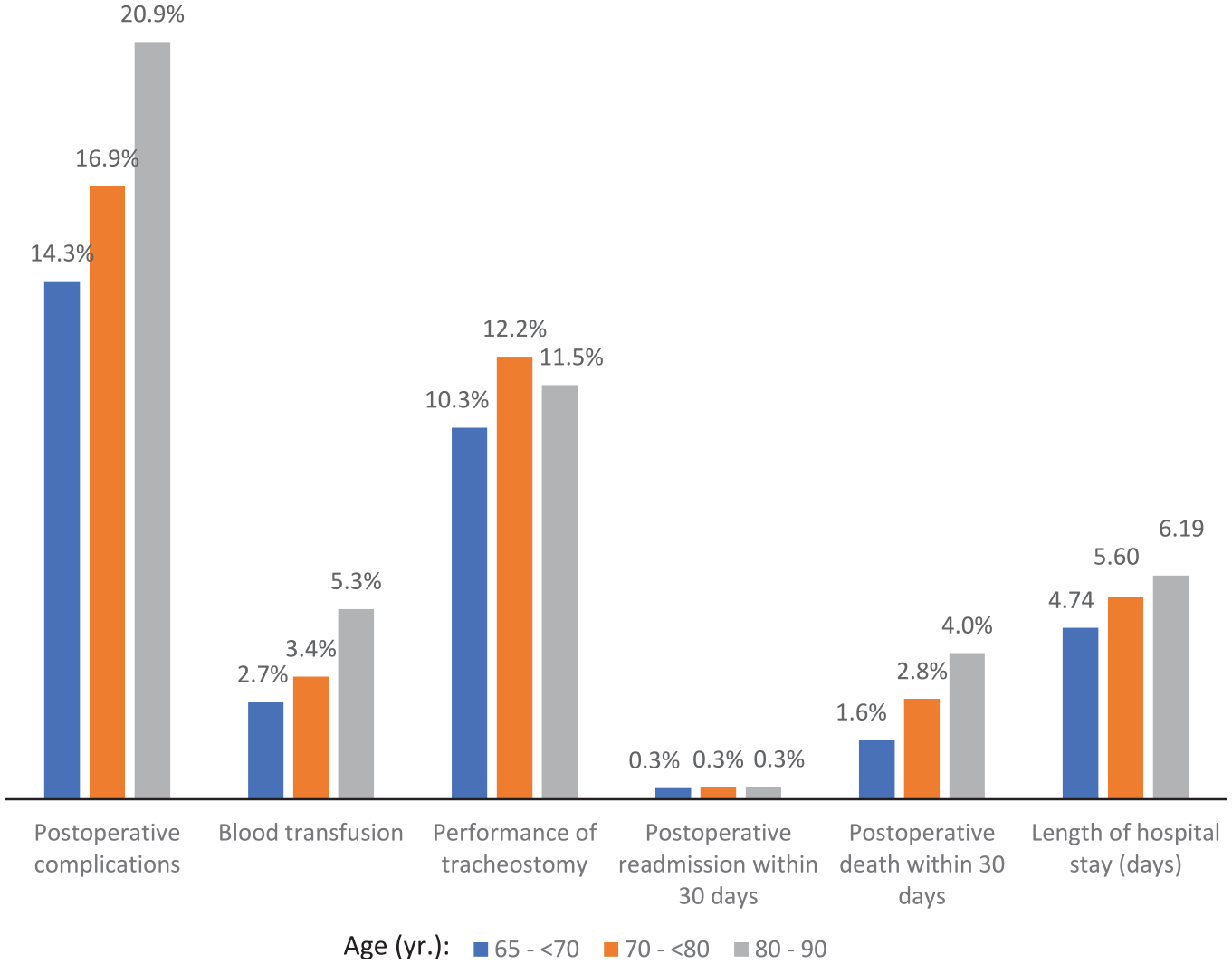
Outcomes in patients ≥65 years old who underwent head and neck surgeries.
Postoperative mortality risk in the adjusted analysis for patients ≥65 years old was associated with older age, male sex, and multiple comorbidities (P < .05 each) ( Table 3 ). Surgeries of thyroid and salivary duct had the lowest risk of mortality compared to other site surgeries (P < .05). In addition, patients ≥65 years old who had oncological surgery had a lower mortality risk than their counterparts who had nononcological surgeries (OR, 0.14; 95% CI, 0.10-0.21; P < .001). Tracheostomy and blood transfusion during hospital admission were associated with increased risk of inpatient mortality (P < .001 each).
Risk of Postoperative Mortality within 30 Days in Patients ≥65 Years Old Who Underwent Head and Neck Surgeries in Relation to Clinical and Demographic Factors.
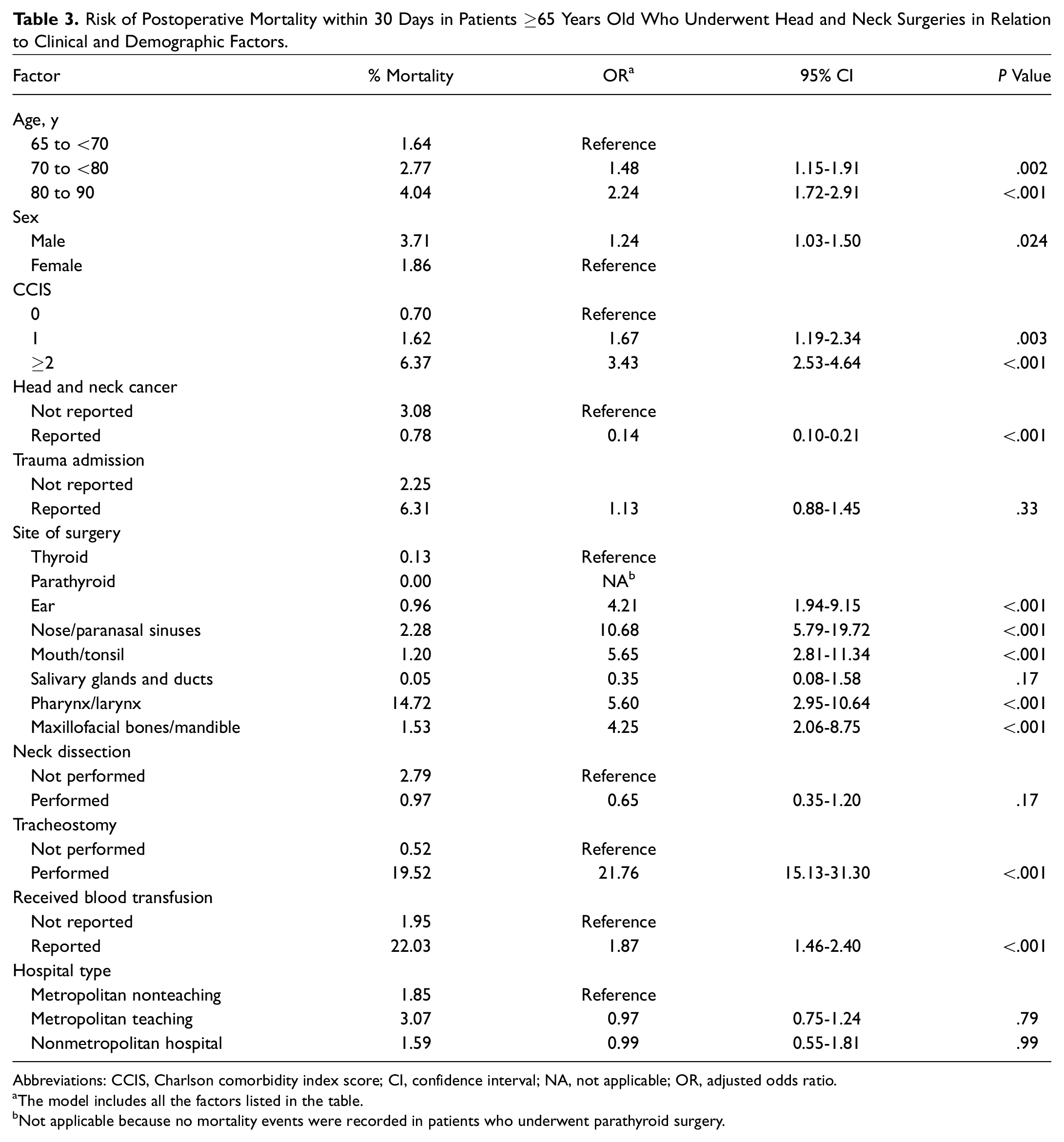
Abbreviations: CCIS, Charlson comorbidity index score; CI, confidence interval; NA, not applicable; OR, adjusted odds ratio.
The model includes all the factors listed in the table.
Not applicable because no mortality events were recorded in patients who underwent parathyroid surgery.
Discussion
By the year 2030, almost 20% of the population is estimated to be composed of people aged 65 years and older. 1 Worldwide, life expectancy is expected to increase to 78 years in 2095 to 2100. 2 Consequently, the treatment patterns of otolaryngologists are significantly influenced by this growing population, and the economic impact is profound. In 2000, 35% of inpatient hospital visits were due to patients 65 and older. The present study is one of the largest in head and neck surgery literature to assess for postoperative risk factors and short-term mortality at a population level among elderly patients. We found that postoperative complications and 30-day operative mortality were increased in the elderly population compared to patients <65 years old. Increasing comorbidity score, the need for a blood transfusion, and the performance of a tracheotomy were predictive of increased mortality.
From 2010 to 2015, we found a significant increase in patients ≥65 undergoing head and neck surgery. Patients ≥65 were more likely to undergo surgery for head and neck cancer and less likely to undergo surgery for trauma compared to patients <65 years old. Even though most diagnoses of head and neck cancer occur during the fifth and sixth decades of life, 10 a significant burden of head and neck cancer occurs in older individuals. Previous studies have shown that elderly patients are less likely to receive guideline-recommended treatment.4,11 The combination of nonstandard treatment and less data regarding treatment outcomes of elderly head and neck surgery patients can lead to suboptimal treatment. These findings necessitate further prospective studies to better understand this growing population of aging patients.
Tracheotomy is one of the most commonly performed procedures by otolaryngologists. A review of 1130 tracheotomy patients demonstrated a low mortality rate (<1%) and low rate of major complications (<5%) with the procedure itself. 12 Shah et al, 13 in an analysis of 113,653 tracheotomy patients, found that age was one of the greatest risk factors for in-hospital mortality. In agreement, we found that performance of a tracheotomy in elderly patients was a strong predictor of 30-day operative mortality. It is impossible to say whether the tracheotomy directly contributed to the increased mortality, but the more likely reason for increased mortality is related to the underlying illness that led to the performance of a tracheotomy. Tracheotomy is often performed in critically ill patients with life-threatening illnesses and significant underlying comorbidities. Physicians can use this important prognostic information to help counsel patients and families about mortality risk after a tracheotomy in patients aged ≥65 years.
The benefits vs risks of blood transfusions must be carefully weighed in the postoperative period. In the current study, patients over ≥65 years were more likely to require a blood transfusion postoperatively, and the risk of 30-day operative mortality was strongly associated with patients who received a blood transfusion. Although the statistical model controlled for comorbidity index, it is likely there is a residual impact of comorbidity status on the risk of transfusion. The NRD does not provide data as to whether the blood transfusion was required due to worsened chronic anemia, hematologic disorder, or perioperative blood loss. It is known that anemia, along with other hematologic disorders, increases with age. 14 Our results are in agreement with prior studies that have shown blood transfusions are associated with an increased 30-day operative mortality in noncardiac surgery patients.15,16 An analysis of 48,720 patients undergoing noncardiac surgery showed that older patients were more likely to require a blood transfusion. 15 In a retrospective analysis of hip fracture patients 60 years and older who underwent operative repair, Carson et al 17 found no benefit of transfusion in patients with a hemoglobin over 8.0.
Postoperative complications and 30-day operative mortality were higher in patients ≥65 years old undergoing head and neck surgery compared to patients <65 years old. The most common complications included pulmonary-related illnesses, bleeding, and acute renal failure. Similarly, in gastrointestinal surgery patients ≥75 years old, pulmonary complications can be up to 5.1 times higher and urologic compilations can be up to 6.8 times higher. 18 While there is much heterogeneity among individuals ≥65 years, this population tends to have more comorbidities and disabilities, which makes optimal management increasingly complex. We found that patients with ≥2 CCIS had an increased 30-day operative mortality compared to patients with less comorbidities. The most common comorbid conditions included diabetes, chronic obstructive pulmonary disease, and renal disease. As the proportion of older patients undergoing head and neck surgery increases, understanding what factors may increase complications and mortality is paramount. This information provides important data to help counsel older patients with concomitant comorbid illnesses regarding the increased morbidity and mortality in the postoperative period.
The current study has multiple limitations inherent to an administrative database. The cross-sectional design prevents establishing causality. The NRD uses ICD-9 codes in reporting disease and outcomes that lack relevant clinical details. The present study provides data on short-term mortality (30 day), but results cannot be extrapolated to long-term mortality. All patients in the current study underwent surgery, and the study does not include patients who underwent nonsurgical treatment for their respective ailment. Nevertheless, this study provides a national perspective of large sample size that could guide future studies examining the observed association at the population level.
Conclusions
This large population-level retrospective analysis analyzes presentations and outcomes of elderly patients who underwent head and neck surgery. Elderly patients are increasingly undergoing head and neck surgery. Tracheotomy, postoperative blood transfusion, and increasing comorbidities were associated with increased 30-day operative mortality. Older patients undergoing head and neck surgery were more likely to have head and neck cancer compared to younger patients and may be less able to adapt to the added stress of any postsurgical complication. These results highlight the need for providing different level of care and interventions to prevent postoperative complications.
Supplemental Material
Appendix_A – Supplemental material for Presentation and Outcomes of Elderly Patients Undergoing Head and Neck Surgeries: A National Perspective
Supplemental material, Appendix_A for Presentation and Outcomes of Elderly Patients Undergoing Head and Neck Surgeries: A National Perspective by Zaid Al-Qurayshi, Christopher Blake Sullivan, Adam Schwalje, Jarrett Walsh, Rodrigo Bayon, Ralph Tufano and Emad Kandil in Otolaryngology–Head and Neck Surgery
Footnotes
The study was selected for a podium presentation at the 123rd annual meeting of the American Academy of Otolaryngology–Head & Neck Surgery; September 14, 2019; New Orleans, Louisiana.
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.