
Abstract
Objective
The aim of this study was to evaluate the hearing outcome of cochlear implantation in patients deafened by Ménière’s disease.
Study Design
Retrospective single-institution study.
Setting
Tertiary medical center.
Methods
Our institutional database of 1400 patients with cochlear implants was reviewed to identify cases with deafness due to Ménière’s disease. Twenty-nine patients were identified: 24 with unilateral and 5 with sequential bilateral cochlear implants. Pre- and postoperative speech recognition scores and medical data were extracted from the medical record and analyzed.
Results
Overall the mean difference between pre- and postoperative speech recognition after >1 year was 56% (95% CI, 47.08%-64.92%). The mean preoperative monosyllabic word score was 9.5%, and the mean postoperative scores at 1 month, 3 months, 6 months, 1 year, and >1 year were 37.1%, 46.1%, 54.1%, 59.1%, and 66.8%, respectively. Cochlear implantation resulted in improved word scores in all patients regardless of prior medical or surgical treatment (endolymphatic sac, labyrinthectomy). The mean postoperative hearing improvement in patients aged <70 and ≥70 years was 65.26% (95% CI, 54.79%-75.73%) and 40.00% (95% CI, 27.22%-52.77%). Postoperative word scores in patients with bilateral cochlear implants were not significantly different between the first and second implanted ears or between the monoaural and binaural testing conditions.
Conclusion
Cochlear implant in patients deafened by Ménière’s disease significantly improves word recognition scores regardless of whether medical or surgical treatment is used prior to implantation. The potential improvement in word recognition scores decreases after age 70 years.
The symptoms of Ménière’s disease include episodic vertigo, fluctuating progressive sensorineural hearing loss, tinnitus, and aural fullness. 1 Prevalence in the United States is approximately 190 in 100,000, with a female predominance. 2 The age of onset ranges from the fourth to the seventh decade of life and increases with age. 2 Reported incidence of bilateral Ménière’s disease has ranged between 12% and 50% of cases.3-5 The proportion of patients with Ménière’s disease whose symptoms progress to bilateral or severe to profound hearing loss secondary to the underlying natural history is relatively low. 6 Approximately 1% to 6% of these patients 4 progress to severe to profound hearing loss, and about 1% go completely deaf. 7 Cochlear implantation is currently the only treatment available for hearing restoration in the affected ear in cases of profound hearing loss.
Previous studies of speech perception in Ménière’s disease have indicated improvements in word or sentence testing scores.8,9 Most studies comparing speech perception between patients with Ménière’s disease and patients with cochlear implants (CIs) but without Ménière’s diesase6,10-14 have reported hearing improvement outcomes similar to the general CI population. Only McRackan et al 13 cited poorer outcomes. Other studies have examined the effect of surgical Ménière’s treatments on CI outcomes, such as endolymphatic sac surgery and labyrinthectomy.10,13 Neither of these surgical treatments had a detrimental effect on the audiologic outcomes of CIs for patients with Ménière’s disease who had intractable vertigo and medical treatment failure.
Few studies have examined the influence of age at implantation on outcome in Ménière’s disease. Mukherjee et al stated that age did not influence CI hearing outcomes in such patients. 15 This one finding contrasts with other studies that examined the effect of age at implantation in the general adult CI population. Blamey et al reported that age at implantation negatively influenced the outcomes of patients aged ≥70 years in the general population. 16 Roberts et al 17 found a similar decrease in word recognition improvement in patients >65 years old. Wong et al noted that elderly patients could benefit from CIs and argued that age should not be a factor limiting CI surgery. 18
Herein we retrospectively examined speech perception outcomes in patients with Ménière’s disease who received CIs at Massachusetts Eye and Ear. We stratified these patients by surgical versus nonsurgical Ménière’s treatment and by age at implantation to study the influence of surgery and age on monosyllabic word scores. We also analyzed the effects of bilateral CIs and duration of hearing loss on CI performance.
Methods
Patients
Patients were selected from an institutional data repository of those who received CIs at the Massachusetts Eye and Ear between 1984 and 2016. This repository was constructed by one of the authors (A.K.) in 2015 and 2016 by reviewing the medical records of all patients with implants since the start of cochlear implantation at this institution. The repository has 23 variables that document the medical and surgical history of each patient. Variables include primary hearing loss etiology, inner ear anatomy, prior ear surgery, and implant surgery approach and complications. Medical data from all cases of hearing loss due to Ménière’s disease were extracted, and these were matched with audiologic testing data from the audiology clinical database.
Twenty-nine recipients of CIs with hearing loss attributed to Ménière’s disease were included: 24 unilateral and 5 bilateral. Patients were all adults postlingually deafened who met the American Academy of Otolaryngology–Head and Neck Surgery diagnostic criteria for Ménière’s disease. 1 Patients had either bilateral end-stage Ménière’s disease or unilateral Ménière’s disease with contralateral hearing loss of different etiology. Patients deafened by Ménière’s disease in 1 ear but who received cochlear implantation in the contralateral ear were excluded. CI surgery for all patients was based on a postauricular mastoidectomy and posterior tympanotomy approach and scala tympani insertion. Electrode insertion was via cochleostomy anterior and inferior to the round window membrane. No intraoperative complications were reported.
Data Extracted
Repository data extracted for retrospective analysis included demographic statistics (ie, age and sex) and clinical information: side of implant insertion, type of implant, age at implantation, duration of hearing loss, unilateral or bilateral Ménière’s disease, Ménière’s treatment (medical vs surgical) and type of surgery (endolymphatic sac surgery or labyrinthectomy), device type, and time of implant activation. Monosyllabic word scores—consonant-nucleus-consonant (CNC) or the Northwestern University Auditory Test No. 6—before and after cochlear implantation were extracted from the audiology database.19,20 Word scores were completed close to 1, 3, and 6 months after CI activation, as well as 1 and >1 year. The highest monosyllabic word scores at >1-year postoperative follow-up were used to evaluate the effect of age at implantation across all patients and between those <70 and ≥70 years old.
Statistical Analysis
Quantitative variables were summarized as mean and standard deviation and categorical variables as frequencies. Quantitative variables were analyzed with independent t tests and categorical variables with chi-square test and Fisher’s exact test. The paired 2-tailed Student’s t test was used to compare preoperative, postoperative, and all follow-up monosyllabic word scores (1, 3, and 6 months; 1 and >1 year). Analysis of variance and Bonferroni post hoc test were used to determine differences among monosyllabic word scores based on the surgery conducted. The associations between monosyllabic word scores and age at implantation were examined through correlation coefficients. One- and 2-tailed P values <.05 indicated significant difference. All statistical analyses were performed with JMP version 13 for Windows (SAS Institute Inc).
Ethical Concerns
The present study was approved by the Human Studies Committee of the Massachusetts Eye and Ear (protocol 2019P000777; principal investigator, S.D.R.).
Results
Patient Characteristics
We identified 29 patients (16 female) with hearing loss attributed to Ménière’s disease ( Table 1 ). Seventy-nine percent (23/29) had bilateral Ménière’s disease and 21% (6/29) unilateral. A total of 34 ears were implanted. All 6 unilateral cases received a unilateral CI in the Ménière’s ear. Of 23 bilateral cases, 18 and 5 received unilateral and sequential bilateral CIs, respectively.
Patient Characteristics. a
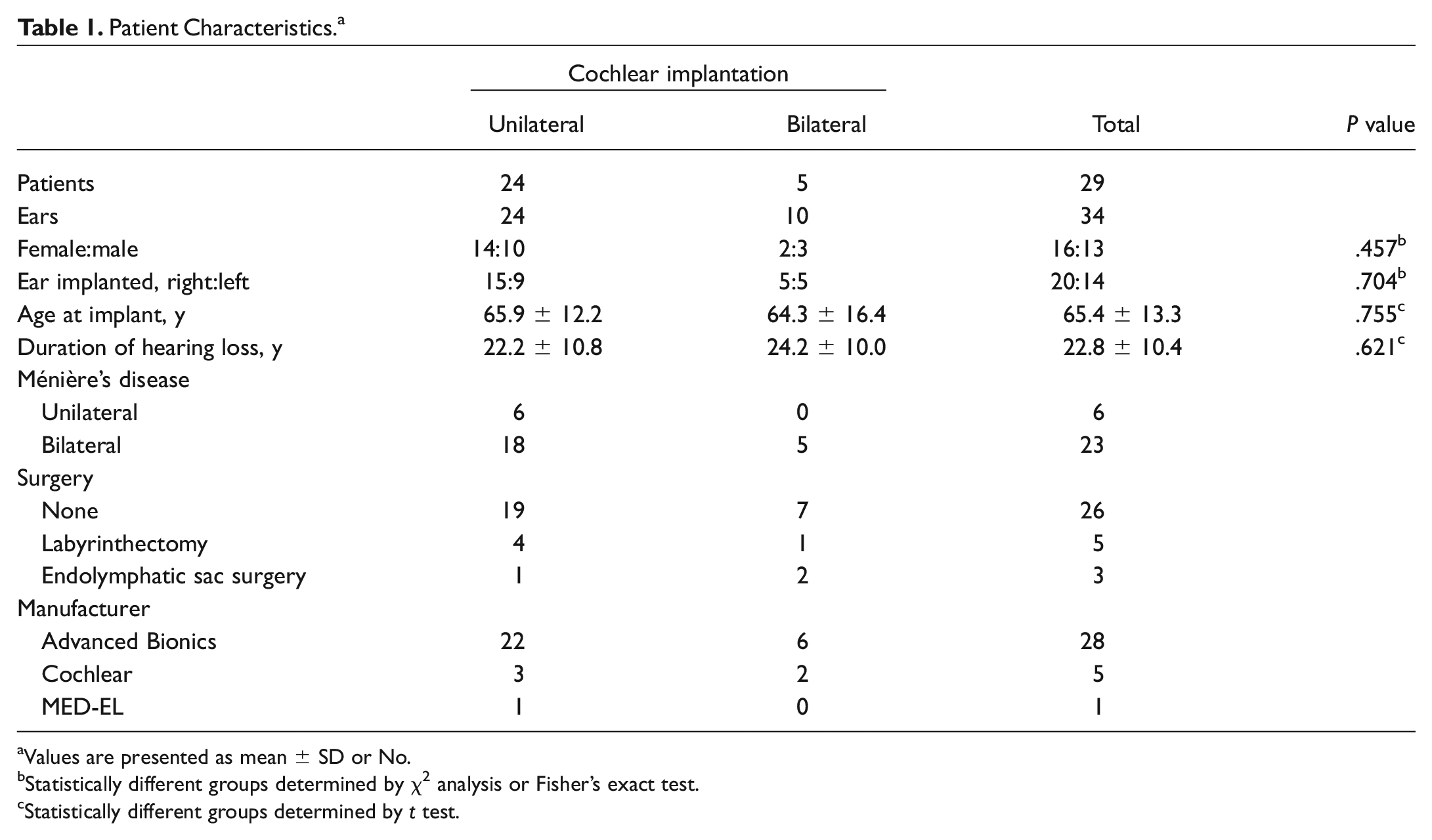
Values are presented as mean ± SD or No.
Statistically different groups determined by χ2 analysis or Fisher’s exact test.
Statistically different groups determined by t test.
The mean age at implantation was 65.4 ± 13.3 years, and the mean duration of hearing loss was 22.8 ± 10.4 years. Of 34 ears, 8 had undergone labyrinthectomy (n = 5) or endolymphatic sac surgery (n = 3) prior to cochlear implantation ( Table 1 ). The majority of the ears (28/34) were implanted with Advanced Bionics electrodes (n = 19, HiFocus/1J; n = 7, Helix; n = 2, Mid-Scala). Five ears were implanted with Cochlear Corporation electrodes (n = 2, Contour; n = 2, Contour Advanced; n = 1, Nucleus 512), and 1 ear was implanted with a MED-EL device (Synchrony Standard). Mean pure tone average prior to cochlear implantation was 95.9 ± 17.8 dB. Mean postoperative hearing follow-up was 5.7 years. No significant differences were observed between cases of unilateral and bilateral CI for sex, side of implant, age at implantation, and duration of hearing loss.
Monosyllabic Word Scores After Cochlear Implantation
The overall mean difference between pre- and postoperative speech recognition after >1 year was 56% (95% confidence interval, 47.08%-64.92%). Mean monosyllabic word scores preoperatively, 1 month, 3 months, 6 months, 1 year, and >1 year were 9.5%, 37.1%, 46.1%, 54.1%, 59.1%, and 66.8% respectively ( Figure 1 ). Postoperative >1-year word recognition was significantly higher than that preoperatively (P < .0001). Postoperative monosyllabic word scores were, on average, higher than preoperative scores (1 month vs preoperative, P < .0001) and improved significantly over time (3 months vs 1 month [P = .0003], 6 vs 3 months [P = .0018], and >1 vs 1 year [P = .0199]). Hearing loss duration was not correlated with >1-year postoperative monosyllabic score (r = −0.1667, P = .4158). The mean postoperative hearing improvement in patients aged <70 and ≥70 years were 65.26% (54.79%-75.73%) and 40.00% (27.22%-52.77%), respectively.
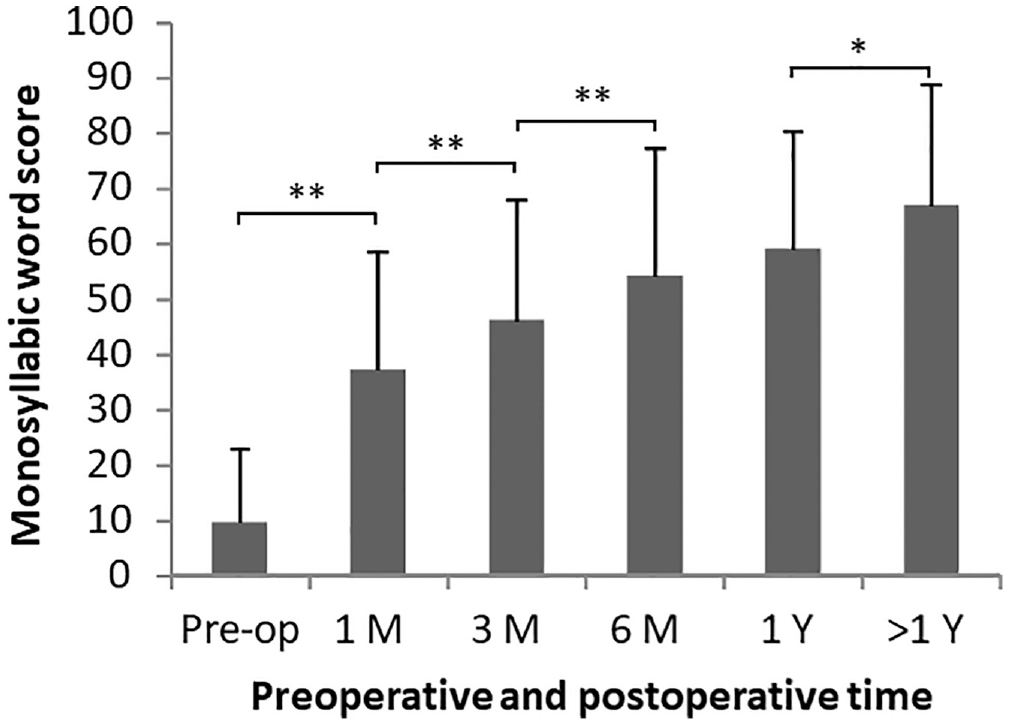
Mean ± SD monosyllabic word scores tested preoperatively and postoperatively at 1, 3, and 6 months as well as 1 and >1 year. *P < .05. **P < .01.
Monosyllabic Word Scores and Prior Ménière’s Surgery
Patients with Ménière’s disease were classified into 3 groups based on type of surgery undertaken: no surgery, endolymphatic sac surgery, and labyrinthectomy. The individual and mean word scores for each group are shown in Figure 2 . A comparison of monosyllabic word scores for each type of surgical intervention across all test periods (preoperatively and postoperatively at 1, 3, and 6 months as well as 1 and >1 year) indicated no significant differences except at 1 year (P = .0088). The post hoc Bonferroni test also indicated a significant difference between the no-surgery and endolymphatic sac surgery groups (P = .0143). The finding is weak, however, and likely due to chance considering that (1) no significant difference was observed in mean monosyllabic word scores between the no-surgery and endolymphatic sac surgery groups after >1 year and (2) each surgery group had a small number of patients. CIs improved monosyllabic word scores in all 3 groups. No significant differences were observed in mean monosyllabic word scores between patients who did and did not have prior Ménière’s surgery.
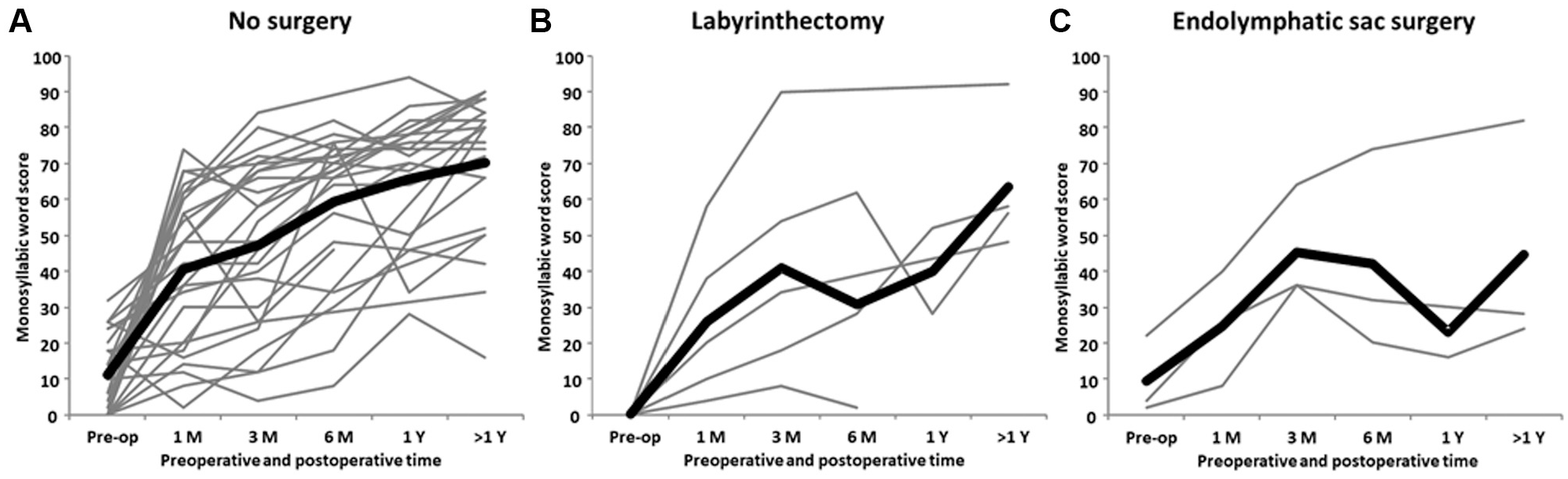
Monosyllabic word scores for 3 treatment groups. Gray and bold lines are individual and mean scores preoperatively and postoperatively at 1, 3, and 6 months as well as 1 and >1 year.
Monosyllabic Word Scores and Age at Implantation
Age at implantation for all patients was negatively correlated with mean postoperative monosyllabic word score >1 year after implantation (r = −0.6185, P = .0003, n = 30). Patients were divided into 2 age groups: <70 years (n = 21) and ≥70 years (n = 13). Thirty-eight percent (13/34) of our Ménière’s CI group was ≥70 years old. Four patients did not have follow-up data beyond 1 year after implantation. Of these 4 patients, 2 were <70 years old at implantation and 2 were ≥70 years. Pre- and postoperative monosyllabic word scores stratified by age are shown in Figures 3 and 4 . The negative correlation between age of implantation and monosyllabic word score is stronger in patients aged ≥70 years (r = −0.7335, P = .0102, n = 11) than in patients aged <70 years (r = −0.2495, P = .3030, n = 19).
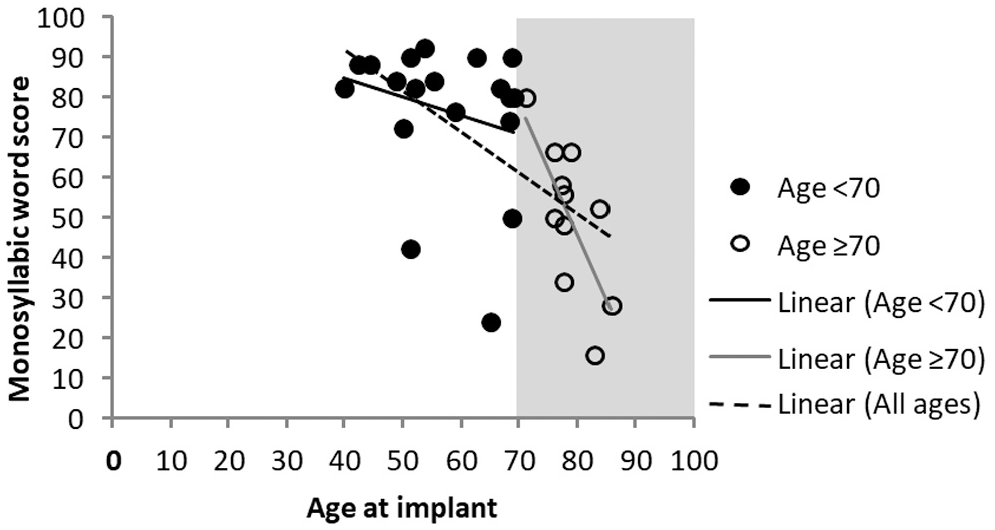
Postoperative monosyllabic word scores after 1 year are presented by age at implantation. Separate linear regression lines are shown for patients aged <70 years (r = −0.2495, P = .3030) and ≥70 years (r = −0.7335, P = .0102) and of all ages (r = −0.6185, P = .0003).
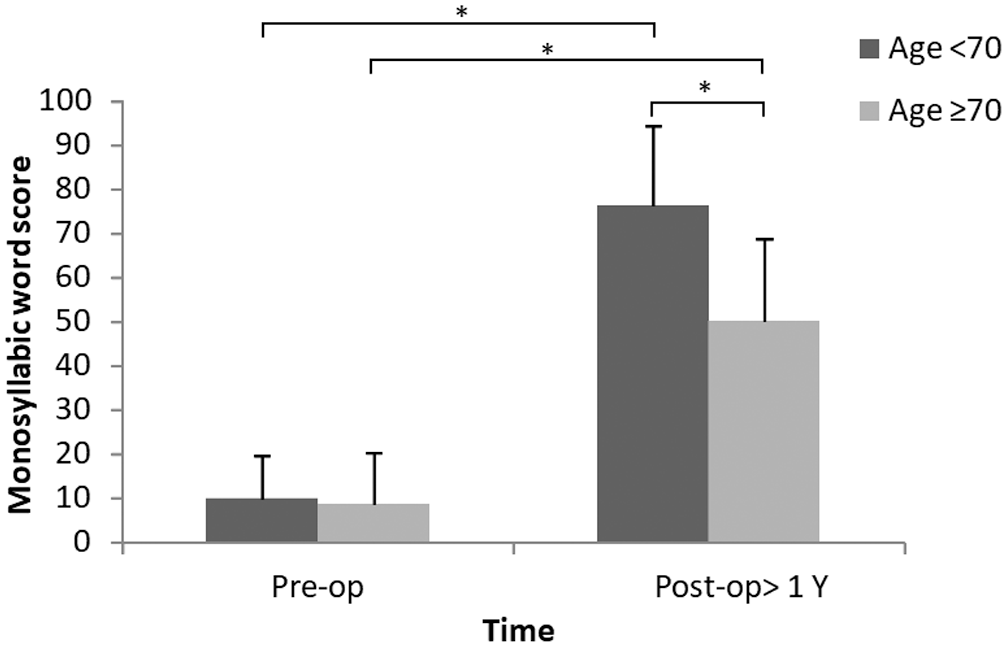
Mean ± SD monosyllabic word scores in patients with Ménière’s disease grouped by age. *P < .01.
No significant differences were observed in mean preoperative word scores between the age groups (P = .7533). Mean word scores increased in both groups after cochlear implantation (age <70 years, P < .0001; ≥70 years, P < .0001). However, postoperative monosyllabic word scores were higher among younger CI users (<70 years) than older ones (≥70 years): 76.32% ± 18.19% versus 50.36% ± 18.48% (P = .0013; Figure 4 ). CI benefits declined steeply as a function of age after 70 years. The duration of hearing loss was not significantly different between the age groups: <70 years (20.23 ± 8.86 years) versus ≥70 years (28.89 ± 11.82 years; P = .0721). Although the duration of hearing loss between the age groups did not reach statistical significance, the mean difference was almost 9 years, which could be clinically significant in some cases.
Bilateral Cochlear Implants
Five patients in this study received sequential bilateral CIs: 2 patients <70 years old and 3 patients ≥70 years. The mean interval between the first and second implantation was 1.71 years. No significant difference was observed in the preoperative mean monosyllabic word scores tested in quiet between the first implanted ear (CI1, 7.2% ± 11.4%) and the second (CI2, 10.8% ± 11.4%; P = .63). There was no significant difference in the postoperative mean monosyllabic word scores at >1 year among CI1 (75.6% ± 18.9%), CI2 (65% ± 28.9%), and binaural performance (CI1 + CI2, 84% ± 12.8% [P = .47]; Figure 5 ). However, postoperative monosyllabic word scores were significantly higher than preoperative scores in CI1 ears (P = .0005) or CI2 ears (P = .0275).
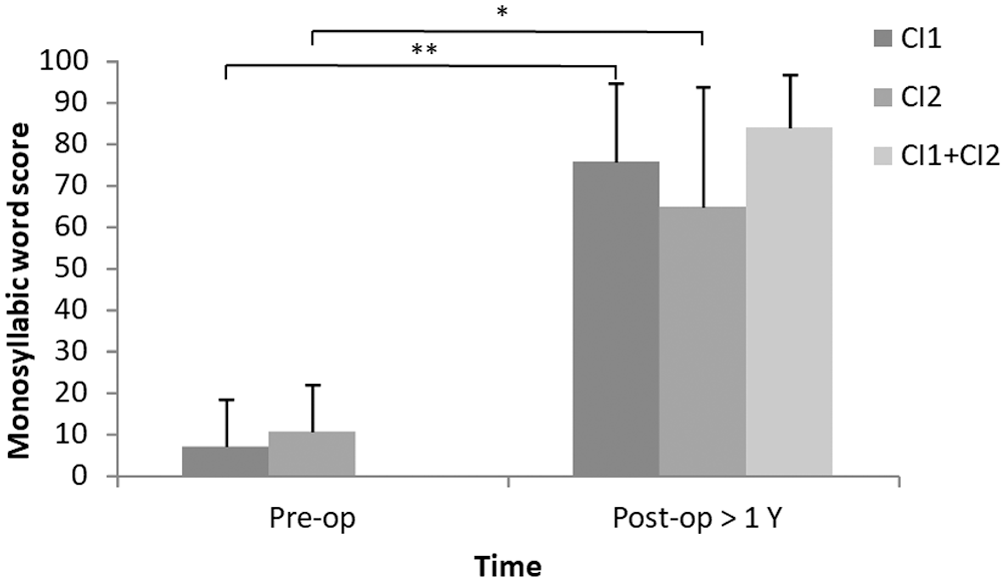
Bilateral cochlear implantation in patients with bilateral Ménière’s disease. Mean ± SD monosyllabic word scores for first cochlear implant alone (CI1), the second cochlear implant alone (CI2), and bilateral CIs (CI1 + CI2). *P < .05. **P < .01.
Technological Evolution
The data for this study were accumulated over 20 years (1996-2016), during which a number of technological advancements were made in CI design. To consider whether these technological changes accounted for differences in hearing outcome, we compared mean hearing improvement in patients who received their CIs from 1996 to 2005 and those undergoing implantation from 2006 to 2016. More than 80% of observations were from implantation from 2006 to 2016. There was no significant difference in hearing outcomes between the 2 decades (P = .8106). The overall mean postoperative hearing improvement of the 2 cohorts was 53.6% (95% confidence interval, 27%-80.19%) and 56.48% (46.26%-66.69%) for 1996 to 2005 and 2006 to 2016, respectively. We further compared the decade effect of implantation between those patients aged <70 and ≥70 years and found no significant difference.
Discussion
In the present study, we retrospectively investigated the association among surgery interventions, age at implantation, duration of hearing loss, and speech recognition following CI surgery in patients with Ménière’s disease. Consistent with previous studies, CIs improved monosyllabic word scores regardless of whether patients had received medical treatment, endolymphatic sac surgery, or labyrinthectomy prior to implantation. The word recognition improvement decreased for patients who underwent implantation at ≥70 years of age. This finding is similar to the age effects reported in the general CI population14,15,21 but not in previous studies of patients with Ménière’s disease and CIs.15,22 No significant differences were noted in postoperative outcomes of sequential bilateral cochlear implantation between the monoaural word scores of both ears or between the monaural and binaural word scores.
Previous studies of CIs in patients with Ménière’s disease have reported superior, 10 equal,6,11,12,14 or worse 13 outcomes as compared with the general CI population. Lustig et al indicated that preoperative and 6-month and 1-year postoperative monosyllabic word scores were 26%, 52%, and 60%, respectively, in patients receiving CIs. 10 Masood et al also noted that CNC scores kept improving at 6 months (55.9%), 1 year (56.5%), and 2 years (58.9%) postimplantation as compared with preimplantation (9.0%; P < .001). 23 Average pre- and postoperative monosyllabic word scores in our study were similar to these results. Mean pre- and postoperative monosyllabic word scores at 1, 3, and 6 months and 1 and >1 year were 9.5%, 37.1%, 46.1%, 54.1%, 59.1%, and 66.8%, respectively. When compared with the preoperative status, the increase in postoperative word score indicated significantly improved hearing (P < .05) that persisted >1 year postimplantation.
The pathophysiology of Ménière’s disease supports similar benefit from cochlear implantation as for the general population. Nadol and Thornton examined the temporal bone of a patient with unilateral Ménière’s disease and found no significant difference in number of hair cells or spiral ganglion cells in the Ménière’s ear versus the contralateral non-Ménière’s ear. 24 Therefore, such patients who undergo cochlear implantation should expect hearing outcomes similar to those of patients without Ménière’s disease.8,10
Intratympanic gentamicin and surgery, including endolymphatic sac surgery and labyrinthectomy, are ablative methods for managing intractable vertigo. 3 Numerous previous studies have evaluated the hearing outcomes following simultaneous labyrinthectomy and cochlear implantation in patients with Ménière’s disease.25-27 Speech recognition results indicated improved outcomes in the implanted ear. In addition, sequential cochlear implantation has been performed following labyrinthectomy in a small number of cases with favorable outcomes. 28
McRackan et al reported that patients with Ménière’s disease who underwent surgical or ablative procedures for their vestibular symptoms had significant improvements in their hearing outcomes following cochlear implantation when compared with those who did not (CNC score, P = .014). 13 Mukherjee et al observed that CIs in cases of Ménière’s disease could yield favorable hearing outcomes in patients who did not undergo labyrinthectomies, patients who underwent simultaneous labyrinthectomy and cochlear implantation, and patients who underwent sequential labyrinthectomy and cochlear implantation. 15 Generally, patients receive great hearing benefits following cochlear implantation, with or without labyrinthectomy. 15 Previous interventions, including treatment with gentamicin, endolymphatic sac surgery, and intratympanic steroids, did not influence hearing outcomes. No single previous treatment (intratympanic steroids, endolymphatic surgery, or labyrinthectomy) influenced audiologic outcomes following cochlear implantation. 22 Our findings also revealed no difference between the no-surgery and surgery groups, although the number of surgical patients was limited. Ménière’s surgery should not be a contraindication for cochlear implantation.
Few studies have reported that age at implantation does not affect hearing outcomes.15,22 Similar to our findings, most cite decreasing CI benefit with age after 70 years.14,15,21 Roberts et al noted that CI recipients aged ≥80 years (postlingually deafened) had lower speech perception scores than other adult CI recipients. 17 We found that patients aged ≥70 years with Ménière’s disease had lower monosyllabic word scores than patients <70 years after cochlear implantation. In addition, the hearing benefits of CIs declined steeply as a function of age after 70 years. Despite the lower speech perception abilities in the older CI group, improvements in monosyllabic word scores were still noted in the present study. The findings suggest that similar quality-of-life benefits for younger and older adult CI groups may result from individual improvements in auditory communication rather than the absolute mean outcomes between groups. 17 Berardino et al stated that CIs were offered to older patients (>65 years) in 36% of cases. 22 In our study, 38% (13/34) of the patients who had received CIs were >70 years old.
Even though a minority of all patients with Ménière’s disease develop bilateral disease, more patients with the bilateral form receive CIs. Berardino et al reported that Ménière’s disease was unilateral in 22% of the CI ears and bilateral in 78%. 22 In our study, 79% of patients had bilateral disease. All underwent implantation sequentially. Holden et al stated that sequential bilateral cochlear implantation in a bilateral case of Ménière’s disease improved the patient’s ability to understand speech in noise and localize sound. 29 Our study evaluated speech scores in quiet and found that postoperative scores were not significantly different among the first implanted ears, among the second implanted ears, and under binaural testing conditions.
As a retrospective review, the present study had several limitations. Only monosyllabic word scores in quiet were available to evaluate hearing outcomes after cochlear implantation. The ability to understand speech in noise was not done as part of the standard clinical evaluation in our institution and therefore was not available to be analyzed. In addition, sound localization capacity under bilateral cochlear implantation was not tested. Furthermore, pre- and postoperative vertigo, tinnitus, and quality of life were not recorded clearly, and the study sample size was small because cases of bilateral severe to profound sensorineural hearing loss due to Ménière’s disease are rare. Despite the small sample, we found a significant trend of postoperative performance in our patients. Due to the retrospective study design, we could not control the heterogeneity of the cases vis-á-vis prior therapies, surgical technical factors, types of speech testing, and device technology.
Conclusion
Our study confirms that word recognition scores improve after cochlear implantation for deafness caused by Ménière’s disease regardless of whether patients received medical or surgical Ménière’s treatment prior to cochlear implantation. Although elderly patients are likely to have poorer speech perception than younger adult recipients, they still demonstrate significant hearing gains following CI surgery. Improvement in word recognition scores declines steeply as a function of age at implantation after 70 years.
Footnotes
This article was presented at the 2020 AAO-HNSF Virtual Annual Meeting & OTO Experience; September 13−October 25, 2020; Boston, Massachusetts.