
Abstract
Objective
To identify social determinants of health care that are associated with poorer pediatric well-differentiated thyroid cancer (WDTC) outcomes and increased stage at presentation.
Study Design
Using the SEER database (Surveillance, Epidemiology, and End Results), we retrospectively gathered data on pediatric WDTC across the United States between 1973 and 2015.
Setting
All patients between 0 and 19 years old with a diagnosis of WDTC were included.
Methods
Patient variables were analyzed for relationships to AJCC stage at presentation (American Joint Committee on Cancer), overall survival, and disease-specific survival.
Results
Among 3913 patients with pediatric thyroid cancer, 3185 were female (81.4%), 3366 had papillary thyroid cancer (85.3%), and 367 had follicular thyroid cancer (9.4%). Two- and 5-year overall and disease-specific survival approached 100%. However, when outcomes were analyzed by specific populations, male sex, non-Caucasian race, poverty, and language isolation were linked to worse overall survival. Male sex and poverty were associated with poorer disease-specific survival. Regarding overall AJCC stage at presentation, male sex and Black race were related to higher overall presenting AJCC stage. Later AJCC T stage at presentation was seen in male, Hispanic, Asian, and Black patients. There were no variables significantly related to following through with recommended surgery.
Conclusion
Pediatric WDTC continues to carry an excellent prognosis in the United States. However, when we consider specific populations, the social determinants of health care affect survival and disease burden at presentation: male sex, poverty, language isolation, and race affected survival and/or AJCC stage at presentation in pediatric WDTC.
Keywords
Thyroid cancer is the most common pediatric endocrine malignancy in the United States. 1 Certain populations have seen a steady rise in incidence by 9.6% annually for the past decade. 2 The prognosis varies widely among histopathologic types. Well-differentiated thyroid cancer (WDTC), including follicular and papillary thyroid carcinoma, has a 10-year overall survival (OS) rate nearing 100%.3-6 Undifferentiated thyroid cancer, including medullary thyroid carcinoma, is associated with significantly lower survival rates and a 10-year OS ranging from 65% to 21%.7-9 Additionally, worsened WDTC outcomes have been reported in patients who present with advanced-stage disease. 10
Irrespective of survival rates, the negative sequelae of thyroid cancer treatment can have lasting ramifications through adulthood; pediatric survivors are at increased risk of developing temperature dysregulation, chronic headaches, physical disabilities, and increased mental fatigue. 11 Furthermore, increasing treatment exposure has been linked to worsened survivor quality of life. 11
To date, there has been limited characterization on the role of health disparities in pediatric thyroid malignancies. Social determinants of health care (SDHs) are defined as “differences in the incidence, prevalence, mortality, and burden of diseases that exist among specific population groups in the United States.” 12 Several state and nationwide retrospective studies on thyroid malignancy have linked lower socioeconomic status and race to poorer survival rates and follow-up care among adults.13-15 Patients of higher socioeconomic status tend to present with lower-stage thyroid cancer. 16 In the pediatric population, lower survival rates have been indicated in males, 17 and delayed time to treatment was noted in children lacking insurance coverage or coming from low-income households.14-18 However, a more complete assessment of the relationship between SDHs and outcomes has not been studied.
The Surveillance, Epidemiology and End Results (SEER) program is a cancer population database. Funded by the National Cancer Institute of the National Institutes of Health, the SEER program “is an authoritative source of information on cancer incidence and survival in the United States. SEER currently collects and publishes cancer incidence and survival data from population-based cancer registries covering approximately 35 percent of the US population” (http://seer.cancer.gov/). SEER combines high-quality clinical, treatment, and outcomes data with that of SDHs. The sheer volume of data provided by the SEER database also permits for the detection of significant differences in population outcomes due to SDHs.
Recognizing which SDHs affect outcomes will facilitate targeted care, improving patient experience and prognosis. Herein, we present the first study to comprehensively describe health disparities in pediatric patients with WDTC on a population level. Our first objective is to identify SDHs that affect OS and disease-specific survival (DSS) in pediatric WDTC. In addition, we seek to identify SDHs that are associated with higher-stage disease at presentation.
Materials and Methods
The SEER database was queried for cases of WDTC from 1973 to 2015. This data set is a direct sample of the pediatric WDTC population, as all data are equally available (and all were used in this study). Given that the database does not include patient-protected health information and is accessible to the public, this study was exempt from approval by the Mayo Clinic institutional review board. Patients <20 years old were identified with ICD-O-3 site code for the thyroid gland (C73.9) and histologic codes for papillary thyroid carcinoma (8050, 8260, 8340-8344, 8350, 8450-8460) and follicular thyroid carcinoma (8290, 8330-8335; International Classification of Disease for Oncology, Third Edition). SEER*Stat 8.3.6 software (National Cancer Institute) was used to collect data on patient demographics, tumor characteristics, survival, and socioeconomic variables per county. We selected for primary tumors and eliminated secondary ones due to confounding variables. The demographics sex, race, and marital status were self-assigned by the patient or caregiver. Socioeconomic variables were percentage county without a high school diploma (less than high school graduate), percentage county language isolation, percentage county below poverty line, and county urban population. The county characteristic of language isolation is defined as the percentage of households within the county without an English-speaking individual of at least 14 years old, as calculated from the US census data. Poverty in the SEER database is defined per the US poverty federal guidelines. Each variable was modeled as a continuum.
Variables with too many levels were redefined and collapsed into fewer levels, as done in previous SEER analyses. 19 Mean and standard deviation were used to summarize descriptive statistics and continuous features. Percentage and frequency count were utilized for summaries of categorical features.
Disparities in Survival
OS and DSS were summarized with the Kaplan-Meier method. Relationships between predictors of OS and DSS were analyzed via univariate and multivariable Cox models. The assumption of linearity was checked via splines of predictors in fits, while the assumption of proportionality was checked through Schoenfeld residuals. A P value <.05 was used for statistical significance. All statistical analyses were performed in R version 3.4.2 (R Foundation for Statistical Computing).
Hazard ratios (HRs) were used to analyze the effects of sex on mortality. This was calculated per the following steps:
Hazard was defined as probability of an event (death) at a specific time:

HR was then calculated by comparing one population’s hazard with another’s. However, when probability of death at a certain time point is small (as in this study), the HR is approximately the ratio of the event incidences:

Disparities by Stage at Presentation
The relationships of tumor burden at presentation to socioeconomic status and patient demographics were assessed through T, N, M, and overall AJCC staging (American Joint Committee on Cancer). N and M stages were categorized binomially: a value of 1 was assigned if there was any nodal (N) or distant (M) metastasis and 0 if there was none. Overall AJCC stage and T stage were analyzed via ordinal logistic regression or binomial logistic regression when multiple categories or binary stages were present, respectively. Univariate modeling across each predictor precluded multivariable modeling in all cases.
Disparities in Following Through on a Recommendation for Surgery
Our group also queried the relationship between disparities and whether a recommended procedure was received. Patients were included in this analysis only if surgery was recommended.
Results
Baseline Patient and County Characteristics
In the SEER database, 3733 cases of pediatric thyroid cancer were identified between 1973 and 2015. Baseline county, socioeconomic, and patient data are recorded in Tables 1 and 2 .
Patient Characteristics. a
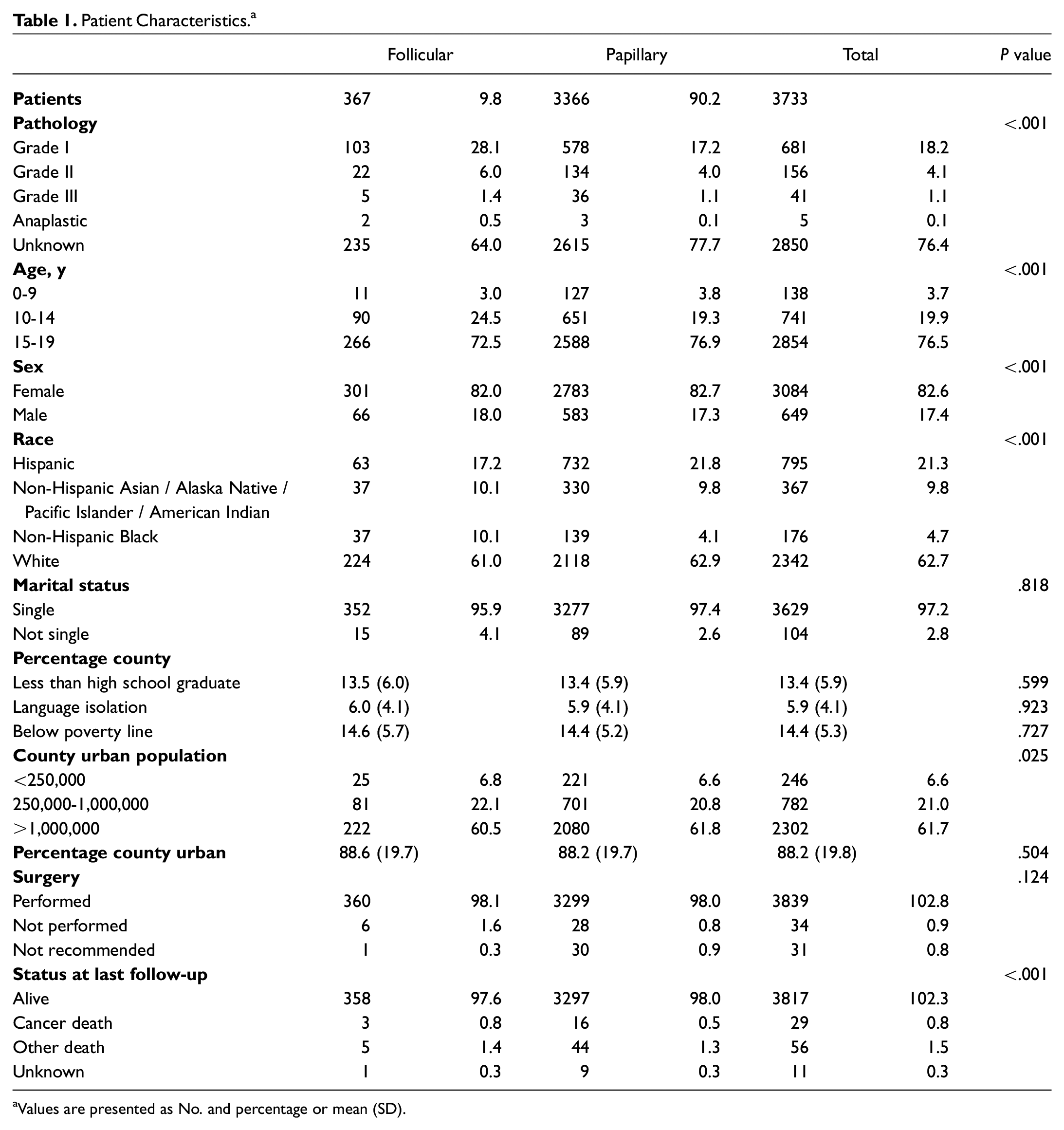
Values are presented as No. and percentage or mean (SD).
Patient Cancer Stage. a
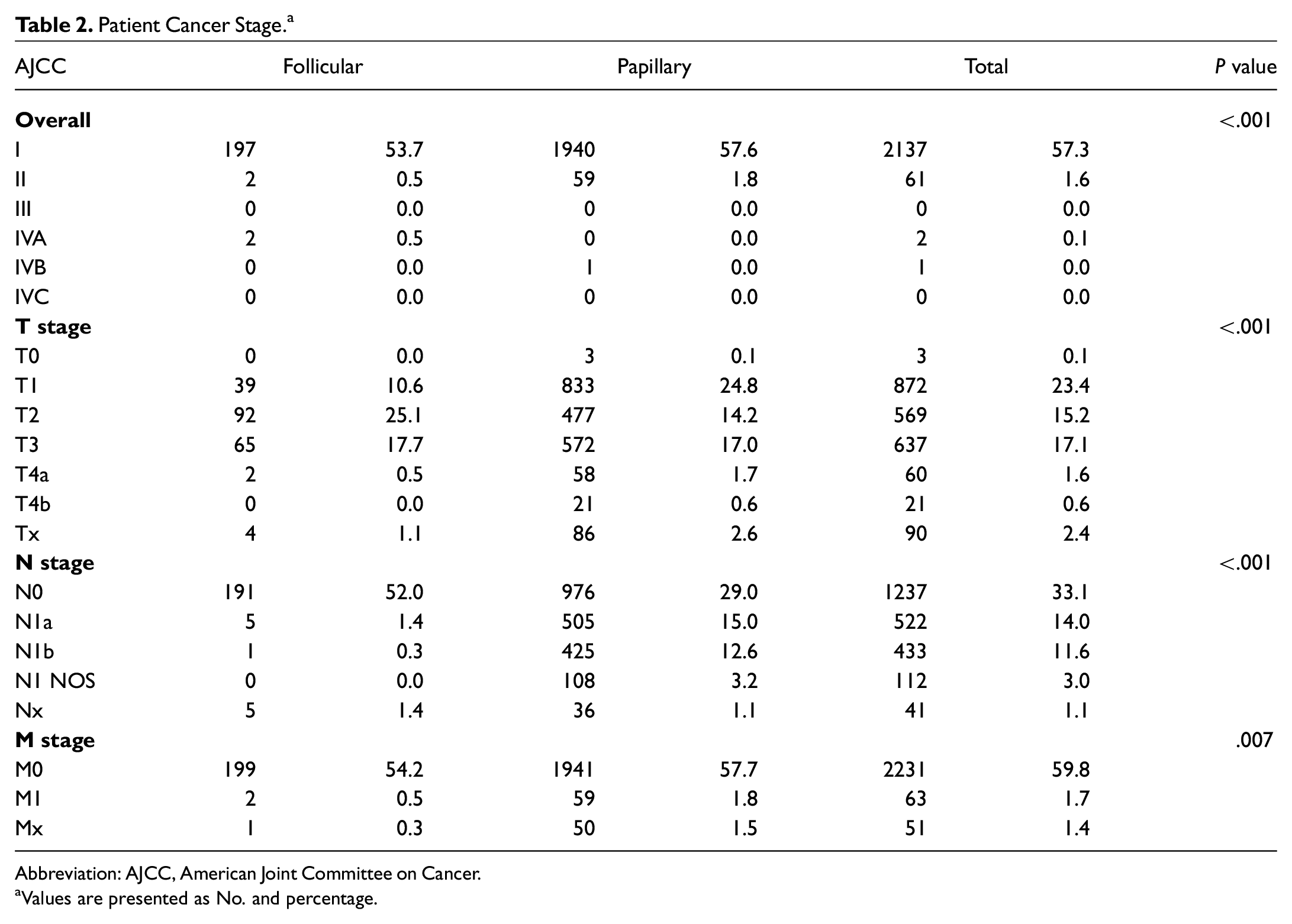
Abbreviation: AJCC, American Joint Committee on Cancer.
Values are presented as No. and percentage.
Overall and Disease-Specific Survival
Two- and 5-year OS was 99.6% and 99.0% while DSS was 99.8% and 99.6%, respectively ( Figure 1a ). There were 78 deaths.
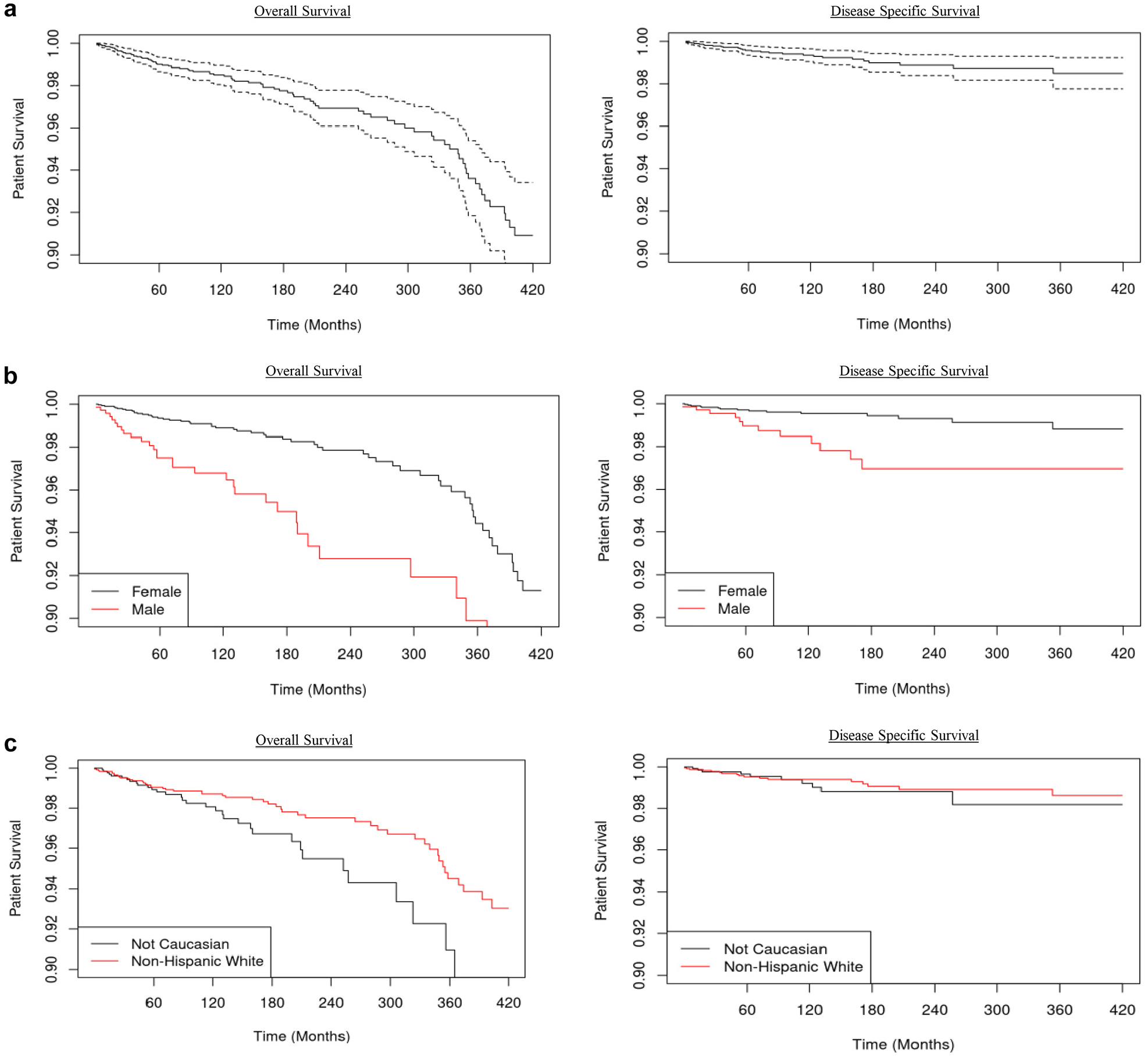
Kaplan-Meier plots of overall and disease-specific survival. (a) The solid line represents the survival curve while the dashed lines are 95% CIs: (b) by sex (P < .10) and (c) by race (P < .10).
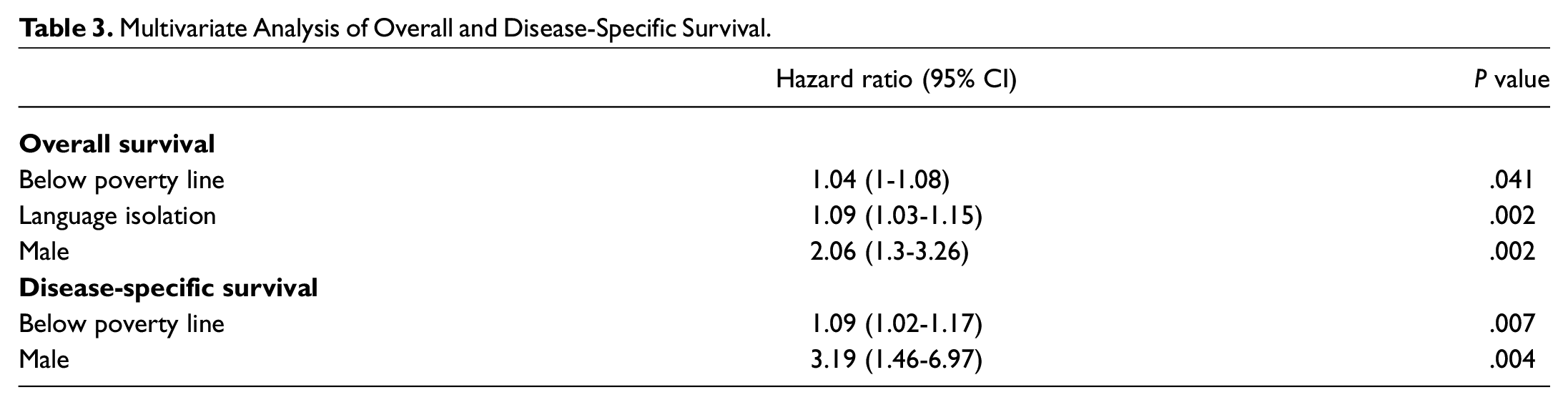
Following multivariate analysis, mean percentage of a county below the poverty line (HR, 1.04; 95% CI, 1-1.08; P = .041), mean percentage of a county language isolated (HR, 1.09; 95% CI, 1.03-1.15; P = .002), and male sex (HR, 2.06; 95% CI, 1.3-3.26; P = .002; Figure 1b ) were linked to worsened OS. Only male sex (HR, 3.19; 95% CI, 1.46-6.97; P = .004) and mean percentage county poverty (HR, 1.09; 95% CI, 1.02-1.17; P = .007) were associated with poorer DSS ( Table 3 ). The HR for males was 2.06; the incidence of death in males was slightly larger than twice that in females ( Table 4 ). Race ( Figure 1c ) and county education (high school) were not statistically associated with decreased OS or DSS following multivariable analysis. However, in terms of overall mortality risk per 100 person-years, non-Caucasian race had an HR of 1.72 (95% CI, 1.13-2.62; P = .011; Table 5 ). When event occurrence is rare, as in this study, we often look at the number of events (NOE) per 100 person-years. NOE is calculated as the number of deaths per cumulative patient time elapsed. For example, if 1 patient died after 10 years and another after 5 years, the NOE would be 2/15, or 0.133 deaths per year. Then, multiplying the numerator and the denominator by 100 would give 13.3 NOE per 100 person-years (reported as 13.3).
Multivariate Analysis of Overall and Disease-Specific Survival.
Multivariable Analysis for Incidence of Death Following Diagnosis of Well-Differentiated Thyroid Cancer.

Overall and Disease-Specific Deaths per 100 Person-Years.

Based on Schoenfeld residuals, decade-specific all-cause and cancer-specific mortality between sexes and races was compared (Supplemental Data, available online). The data suggest no significant decrease in the effects of SDHs on survival over time:
Sex: overall mortality .250
Sex: cancer-specific mortality .090
White race: overall mortality .100
White race: cancer-specific mortality .550
AJCC Staging at Presentation
Following multivariate analysis, male sex (odds ratio [OR], 1.87; 95% CI, 1.15-2.96; P = .009) and non-Hispanic Black race (OR, 2.61; 95% CI, 1.22-5.12; P = .008) were related to higher presenting AJCC stage ( Table 6 ). Patients who were male (OR, 1.43; 95% CI, 1.17-1.74; P < .001), Hispanic (OR, 1.74; 95% CI, 1.46-2.09; P < .001), non-Hispanic Asian (OR, 1.36; 95% CI, 1.04-1.79; P = .026), and non-Hispanic Black (OR, 1.88; 95% CI, 1.32-2.66; P < .001) had increased odds of presenting at later AJCC T stage. There were no patient or demographic variables associated with increased AJCC N or M stage at presentation.
Multivariate Analysis of AJCC Stage at Presentation.
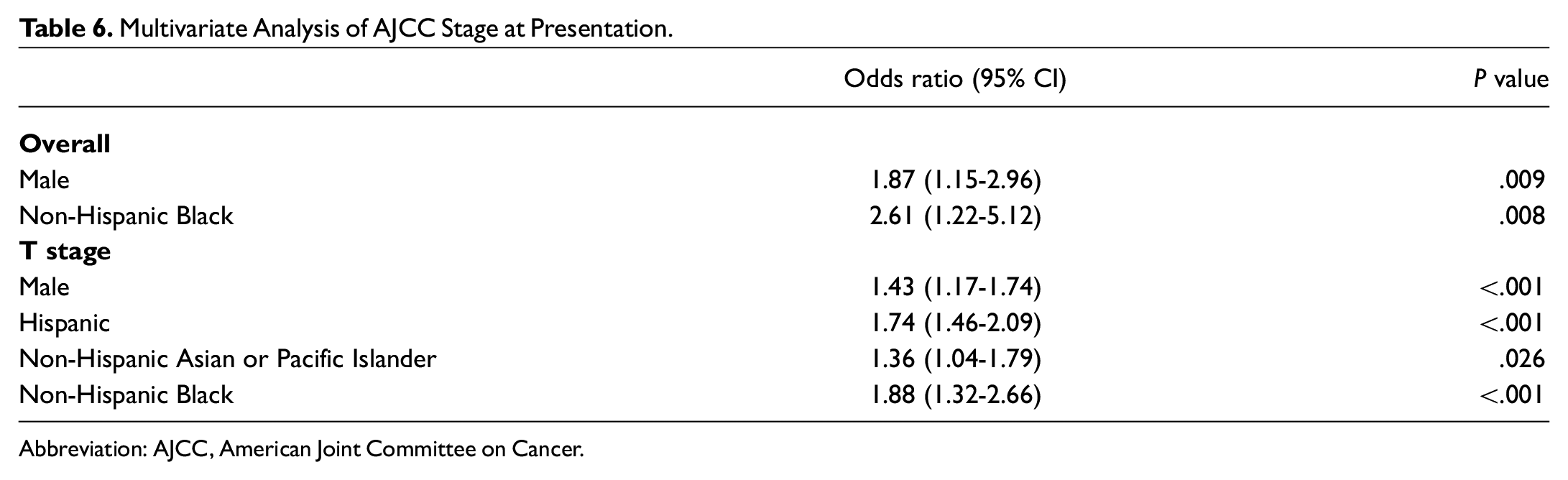
Abbreviation: AJCC, American Joint Committee on Cancer.
Surgery If Recommended
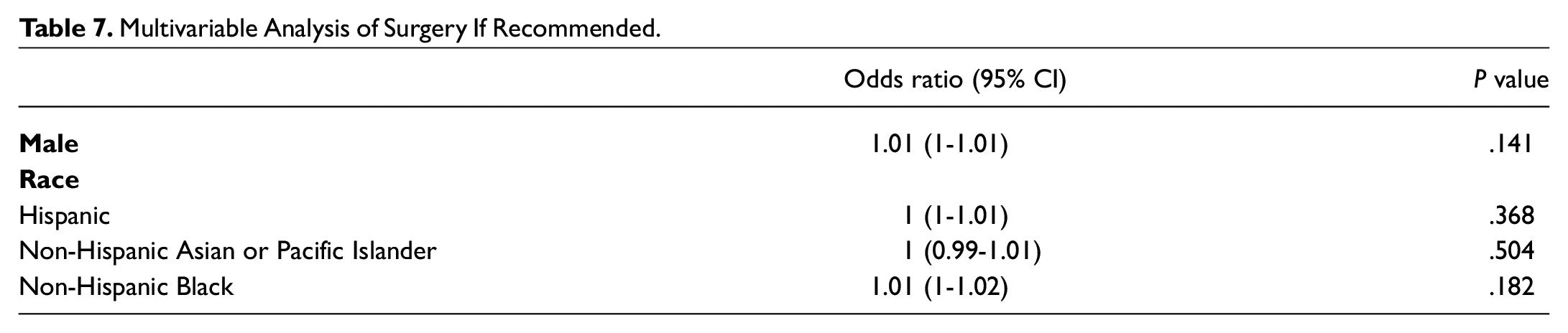
Following multivariate analysis, there were no variables significantly related to declining or proceeding with recommended surgery ( Table 7 ).
Multivariable Analysis of Surgery If Recommended.
Discussion
To our knowledge, this is the first study to comprehensively characterize SDHs in pediatric patients with WDTC. While the observed statistical effect sizes in this article are small, their implications are much larger, as the entire populations of these patients are examined.
SDHs and Survival
Our study revealed that children with WDTC have an excellent prognosis, nearing 100% 10-year OS and DSS, similar to adult rates.8,9 Despite the low mortality, certain SDHs still significantly affected survival. This is indicative of a well-powered study, capable of detecting disparities that affect the larger population.
We found that children living in poor or language-isolated counties had reduced OS, which has not been reported in pediatric WDTC. To investigate a potential cause of this finding, we hypothesized an association with higher disease stage at presentation, which was refuted. However, Garner et al noted that time from diagnosis to commencing treatment was delayed in poorer populations. 18 Taken together, these findings support the need for improved health care access among children in these vulnerable groups. Including social work early and often may help dispel financial barriers to treatment. Additionally, ensuring cultural diversity among medical staff might further physician relatability and patient concordance. 20
Although OS of WDTC was affected by poverty and language isolation, DSS was unchanged. This finding would suggest that these SDHs have a more global impact on children with WDTC. For example, a delay in time to treatment, as mentioned earlier, may lead to prolonged treatment course or increased therapy burden requirements. This may result in secondary ailments that reduce life span by causes that are otherwise not specified.
Our finding that male sex was associated with decreased OS and DSS in pediatric thyroid cancer is consistent with previous literature. 17 It has been hypothesized that tumor biology and pharmacogenetics contribute to worsened survival in males.17,21,22 Additionally, delayed presentation in male children, leading to higher overall AJCC and T stage at presentation, may result in poorer survival rates. We agree with Williams and Spector that there is a need for further molecular-level and epigenetic research on the apparent survival discrepancy between sexes in pediatric thyroid malignancy.17,23-26
Numerous studies have cited the effects of race and county education level on cancer survival rates.27-32 Although non-Caucasian race had increased overall mortality risk per person-year ( Table 5 ), this did not carry over to disease-specific outcomes, where a statistically significant association was not seen. Following multivariable analysis, our study did not find a statistical relationship between mortality or county education and OS and DSS. The covariates of race and county education level may require a more lethal disease to become statistically significant prognostic factors in survival outcomes.
Finally, although we hypothesized that discrepancies in survival between sexes and races have been dissipating over time, we did not find this to be statistically significant (figures in Supplemental Data, available online).
SDH and Disease Burden at Presentation
Our results indicate greater overall AJCC presentation in non-Hispanic Black patients. Additionally, later AJCC T stage was associated with Hispanic, non-Hispanic Black, and Asian children. Several studies have linked SDHs to more advanced thyroid cancer stage at presentation in adults.16,33 To our knowledge, this study is the first to examine the relationship between SDHs and stage at presentation in pediatric thyroid malignancy.
Increased disease burden at presentation may be due to distrust in the health care system among minority groups, leading to delayed medical presentation.34-36 As reported by Arnett et al, 37 significant medical mistrust among African Americans warrants additional consideration in certain minority groups to improve outcomes and time to medical intervention. Provider implicit bias may also play a role in diminishing initial concerns of patients from minority groups, further delaying treatment.38,39 Finally, access to specialty care, as is required in the treatment of pediatric thyroid cancer, has been poorer among minority races. 40 This has led to delayed and worsened disease burden at medical presentation among minority groups.41,42
Although not unique to malignancy diagnosis, the aforementioned data emphasize racial influences on patient care and outcomes. This might be remedied by enhancing self-awareness to racial biases and increasing intervention efforts among vulnerable minority groups. Treatment of WDTC also requires collaboration among medical specialists (including but not limited to surgeons, endocrinologists, oncologists, radiologists, and geneticists). While SDHs are thought to impede a family’s ability to successfully navigate interdisciplinary care,43,44 implementation of well-coordinated multidisciplinary teams may abate the negative health care effects of SDHs on “at risk” communities.43,45,46 For this reason, children with WDTC may be best served by a dedicated team consisting of pediatric specialists from various relevant medical fields.
Male sex was associated with higher overall AJCC and T stage thyroid cancer at initial presentation. Male sex has been associated with more aggressive disease at presentation, defined as testing positive for specific genetic mutations, such as BRAF V600E, which carry poorer prognoses. 47 However, to our knowledge, worsened disease stage at presentation has yet to be reported in pediatric thyroid malignancy. Harvard Men’s Health Watch 48 indicated that women visit their physicians approximately 3 times more often than men. Female children and adolescents are also more affected by societal pressures of expected body mass index and physical appearance. 49 The anxiety among female children to meet these expectations is self-induced and from their peer groups. 50 With evidence of greater societal pressures on female physique and aesthetic appearance,51-54 it is possible that female children and their guardians are more sensitive to physical changes. This may lead to the earlier discovery of thyroid pathology or reporting of thyroid dysfunction sequelae. Finally, several studies on elementary school-aged children have cited a greater increase in somatic and pain complaints with age in girls than in boys.55-62 Although pubertal hormonal changes likely elicit gender differences in how pain is experienced and perceived, societal expectations for boys may delay help-seeking behavior.41,63,64 It has been noted that boys are less willing to talk about their disease and accept their diagnoses. 41 Future studies are needed to directly support the hypothesis that rearing boys with an emphasis on resilience may lead to embarrassment or denial of an ailment, thereby delaying diagnosis.
Following Through on Recommended Surgical Intervention
This study did not find predictors affecting patient follow-through on recommended surgery, a finding seen in other diseases.19,65-67 At our institution, race/ethnicity is not associated with increased costs of surgical otolaryngology care. 68
Limitations
The SEER database provides AJCC staging and not the American Thyroid Association’s Pediatric Risk Classification, the latter being more appropriate for this study. Per AJCC and the age group analyzed, the highest stage possible in this population was stage II. Additionally, disease stage at presentation was used as a surrogate for time to presentation, as the database records the former only. Finally, SEER does not provide insight into the patient’s perspective, and exact reasoning for refusing surgery when recommended could not be elicited. We hypothesize that it may be due to the distrust in health care providers by the relevant minority groups, a relationship that has been appreciated in medicine and medical research.69-71
There is a statistical rule of thumb to have 10 events for each degree of freedom; for example, with 96 total deaths, one could confidently assess OS by comparing and controlling for 9 variables. We acknowledge that in the case of cause-specific death, there are not enough patients for a full multivariable model, which is why variable selection was done. Overall, it is important to recall that power is related to making a type II error or concluding that a variable is not statistically significant when it is supposed to be. Given that there were variables that showed statistically significant differences in survival, even in the case of a small event number, it can be assumed that the variables in question would have an even lower P value in the case of a higher event count.
Conclusion
Pediatric WDTC continues to carry an excellent prognosis in the United States. However, several SDHs remain associated with worsened outcomes and increased disease burden at initial presentation. OS was decreased in males, those below the poverty line, or those with language isolation. DSS was decreased in males and in children below the poverty line. Race and county education level were not statistically associated with worsened prognosis. However, race did affect the total time that a patient was at risk, as seen by the increased event rate per person-year. Regarding disease burden at presentation, higher AJCC stage was seen in males and non-Hispanic Black patients, and AJCC T stage increase was associated with males and children of Hispanic, non-Hispanic Black, or Asian race. Awareness of SDHs is imperative to the early diagnosis and prognosis of pediatric thyroid cancer in vulnerable populations. With increasing awareness of implicit bias and SDHs, future studies could focus on what interventions have been effective at eliminating the effects of SDHs and where limited resources should be allocated.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211032901 – Supplemental material for Effects of Social Determinants of Health Care on Pediatric Thyroid Cancer Outcomes in the United States
Supplemental material, sj-docx-1-oto-10.1177_01945998211032901 for Effects of Social Determinants of Health Care on Pediatric Thyroid Cancer Outcomes in the United States by Nelson R. Gruszczynski, Christopher M. Low, Garret Choby, Kara D. Meister, Byron H. Smith and Karthik Balakrishnan in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.