
Abstract
Objective
To compare survival among patients with head and neck cancer before and after implementing a weekly multidisciplinary clinic and case conference.
Methods
A retrospective cohort study with chart review was conducted of 3081 patients (1431 preimplementation, 1650 postimplementation) diagnosed with stage I-IVB tumors in the oral cavity, oropharynx, hypopharynx, nasopharynx, or larynx. Pre- and postimplementation differences in overall and disease-specific survival 1, 2, and 3 years after diagnosis were assessed with unadjusted Kaplan-Meier curves and multivariable Cox proportional hazard regression models adjusted for demographic characteristics, comorbidity burden, smoking status, tumor site and stage, p16 status for oropharyngeal squamous cell cancer, and initial treatment modality.
Results
Patients less commonly presented with oropharyngeal squamous cell cancer and advanced tumors (III-IVB) and received primary treatment with surgery alone or with adjuvant therapy preimplementation than postimplementation. Overall survival at 3 years was 77.1% and 79.9% (P = .07) and disease-specific survival was 84.9% and 87.5% (P = .05) among pre- and postimplementation patients, respectively. At 3 years, preimplementation patients had slightly poorer overall (hazard ratio, 1.20; 95% CI, 1.02-1.40) and disease-specific (hazard ratio, 1.26; 95% CI, 1.03-1.54) adjusted survival than postimplementation patients. In unadjusted and adjusted analyses, survival improvements were more pronounced among patients with advanced disease.
Discussion
A multidisciplinary clinic and case conference were associated with improved outcomes among patients with head and neck cancer, especially those with advanced tumors.
Implications for Practice
All patients with head and neck cancer should receive multidisciplinary team management, especially those with advanced tumors.
National Comprehensive Cancer Network (NCCN) guidelines strongly recommend that a team of multidisciplinary health care providers with specialized expertise provide initial evaluation and treatment planning for patients with head and neck cancer (HNC). 1 Involved disciplines include head and neck surgery, radiation oncology, medical oncology, nursing, speech and language pathology, physical therapy, nutrition, and social work. 2 Tailored treatment planning and care coordination are particularly important for HNC due to its complexity, multimodal treatment, and generally older patient population, which is more likely to have comorbidities and less social support. 3
Multidisciplinary HNC tumor boards meeting virtually or in person are designed to improve patient management and outcomes by reviewing new and recurrent cancers and providing recommendations for evaluation and management. Improvement in patient management is often assessed by the interval between diagnosis and treatment initiation,4,5 an independent predictor of survival, 6 and altered staging or treatment plans.7,8 Only a limited number of studies investigating the effectiveness of this multidisciplinary approach have reported survival outcomes, with conflicting findings.2,4,9-11
Kaiser Permanente Northern California (KPNC) is an integrated health care delivery organization with 21 medical centers and >250 affiliated clinics, currently serving 4.4 million enrolled members. Until mid-2013, patients diagnosed with HNC were generally managed at local medical centers. They may or may not have been reviewed at a general tumor board or referred to 1 of 3 regional HNC-specific tertiary care hubs at the discretion of their primary otolaryngologists. In June 2013, KPNC consolidated care for patients with new and recurrent HNC, establishing a universal referral process from all local medical centers to a weekly multidisciplinary clinic (MDC) at the 3 hubs. Each patient is evaluated by appropriate specialists, including fellowship-trained head and neck surgeons, radiation oncologists, medical oncologists, speech and language pathologists, dieticians, and social workers. After MDC evaluations, providers from all HNC hubs convene virtually to present and discuss all referred patients, joined by other providers with expertise in HNC, including neuroradiology, nuclear medicine, and pathology. Six or more fellowship-trained surgeons and multiple additional physicians from other specialties also attend each weekly virtual case conference, where approximately 25 patients are prospectively reviewed. For all patients, participating physicians review imaging studies and pathology, confirm staging, and approve or modify treatment plans proposed by presenting hub surgeons. Clinical guidelines for pretreatment evaluation, staging, and treatment were developed to ensure quality of care consistent with NCCN recommendations.
The purpose of this study was to compare overall survival (OS) and disease-specific survival (DSS) among patients diagnosed with HNC pre- and postimplementation of the MDC and case conference. We hypothesized that incorporating a multidisciplinary care approach would be associated with improved patient outcomes.
Methods
Study Design and Setting
Our retrospective cohort study compared characteristics and outcomes of KPNC patients diagnosed and initially treated for primary mucosal HNC before and after MDC and case conference implementation across all medical centers. Four-year inclusion periods pre- and postimplementation were defined respectively as January 1, 2009, to December 31, 2012, and June 6, 2013, to June 5, 2017. Patients diagnosed with HNC in the first 6 months before implementation were excluded to avoid management overlap between cohorts. All patients were followed from HNC diagnosis for 3 years or until death, whichever occurred earlier.
Study Population
Eligible patients with histologically confirmed primary squamous cell carcinoma of the oral cavity, oropharynx, hypopharynx, nasopharynx, or larynx were identified with data from the KPNC Cancer Registry, which has captured all cancers diagnosed or treated across all KPNC facilities since 1988 following national SEER program standards (Surveillance, Epidemiology, and End Results). Patients were excluded if they (1) were diagnosed with an occult, stage 0, or stage IVC tumor; (2) died before treatment initiation; (3) received treatment outside KPNC; (4) discontinued health plan membership before treatment initiation; (5) had previous radiation to the head and neck; (6) declined treatment; or (7) received palliative care with no curative treatment ( Figure 1 ).
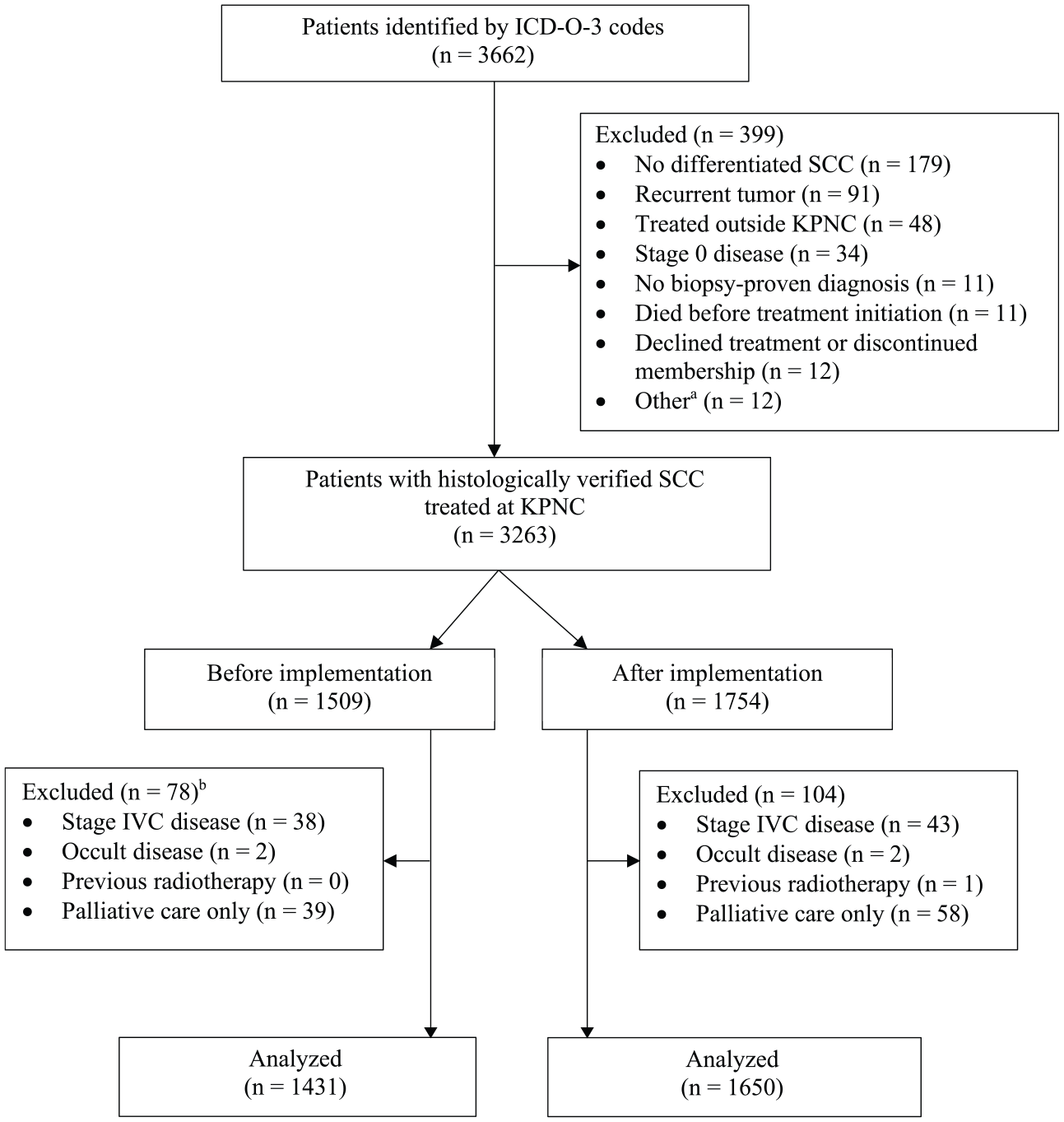
Participant flow diagram. ICD-O-3, International Classification of Diseases for Oncology, Third Edition; KPNC, Kaiser Permanente Northern California; SCC, squamous cell cancer.
Data Sources and Elements
Patient-level data were obtained from the cancer registry, clinical and administrative databases, and medical chart and pathology review. KPNC Cancer Registry data included age at diagnosis, sex, race/ethnicity, tumor anatomic site, stage per American Joint Committee on Cancer (AJCC; seventh edition), and histology. Data from clinical databases included smoking status at diagnosis; preexisting comorbidities, identified by clinical diagnosis and procedure codes linked to inpatient and outpatient encounters in the 12 months before diagnosis; and use of speech-language pathology services and imaging studies.
For patients with oropharyngeal squamous cell carcinoma (OSCC), immunohistochemistry data on p16 expression were obtained from pathology reports. In addition, because oropharyngeal tumors were not routinely tested for p16 before MDC implementation, we conducted immunohistochemistry analysis of p16 expression on 251 patients with previously untested tissue specimens from adequate and available formalin-fixed paraffin tumor blocks. p16 status was identified for 95% of all patients with OSCC. To minimize intra- and interobserver variability in analysis of p16 expression, a designated pathologist (Y.W.) assisted in interpreting all stained slides.
Data on primary and adjuvant treatment, including dates, modality, and type, were obtained primarily from standardized chart review. Three clinicians (C.M., N.T.N., J.A.) completed chart reviews with a standardized protocol after reviewing the same 100 charts to ensure consistent data collection. Chart reviews verified diagnoses, tumor site, and primary treatment modality and confirmed staging. Patients managed nonsurgically were staged with AJCC clinical designation based on radiographic and clinical findings. Patients treated surgically were staged with the pathologic AJCC designation within each tumor site. Other data elements obtained from chart review included performance of neck dissection and number of lymph nodes removed from the treated sides, 12 receipt and modality of salvage therapy, and date and cause of death when applicable.
The independent variable of interest was HNC diagnosis pre- or post-MDC implementation. Primary outcomes were OS and DSS 1, 2, and 3 years after diagnosis. Covariates included factors known or posited to influence OS or DSS and available from existing data sources: age at diagnosis, sex, race/ethnicity, smoking status, Charlson comorbidity index, tumor site, stage, p16 status for OSCC, and primary and adjuvant treatment modality.
To assess the impact of MDC on care processes, we measured the mean time in days from initial referral for specialist evaluation to treatment initiation and the proportion of patients receiving speech and language pathology consultations. To assess the impact of imaging advances over time, we examined the use of all imaging and the use of PET and PET/CT scans (positron emission tomography/computed tomography) for initial diagnosis and surveillance. We also assessed rates of migration from clinical to pathologic staging.
Statistical Analysis
We compared the distribution of covariates between patients diagnosed pre- and postimplementation, assessing the statistical significance of differences with t tests or Wilcoxon tests for continuous variables and Pearson chi-square or Fisher exact tests for categorical variables. We used the Kaplan-Meier method to estimate OS and DSS probabilities 1, 2, and 3 years after diagnosis for each group, evaluating differences in survival probabilities with the log-rank test. We used the same method to estimate OS and DSS probabilities separately for patients with early-stage (I/II) and advanced-stage (III/IV) tumors.
To examine associations of MDC implementation with OS and DSS, hazard ratios (HRs) and 95% CIs were estimated with univariable and multivariable Cox regression analysis. Treatment covariates were modeled as time-dependent variables to account for varying intervals between diagnosis and treatment. Follow-up began on the HNC diagnosis date and continued until death or the end of the specified year intervals, whichever occurred earlier. Primary analyses included all patients, with multivariable regression models adjusted for age, sex, race/ethnicity, Charlson comorbidity index, smoking status, major tumor site, stage, p16 status, and primary and adjuvant treatment modality. Similar secondary analyses were performed to examine whether associations differed by major tumor site and by stage (early vs advanced). All statistical tests were 2-sided, with a significance level of 5%. Analyses were conducted with SAS version 9.4 (SAS Institute Inc).
The KPNC Institutional Review Board approved the study, granting a waiver of informed consent.
Results
After exclusions, the study population comprised 3081 patients diagnosed with HNC: 1431 pre- and 1650 post-MDC implementation ( Figure 1 ). Patients in both groups were similar at diagnosis in age, sex, race/ethnicity, comorbidity burden, smoking status, and, among patients with OSCC, p16 status ( Table 1 ). However, tumor site, stage, and treatment modality distributions differed across groups. Oral cavity cancer was more commonly diagnosed and OSCC less commonly diagnosed before than after MDC implementation. Patients in the preimplementation group had less advanced tumors, were less likely to receive surgery alone as primary treatment, and were more likely to receive adjuvant therapy as compared with patients in the postimplementation group. Median time to treatment from diagnosis was unchanged at 32 days preimplementation and 33 days postimplementation. After implementation, the proportion of patients receiving speech and language pathology consultations increased from 28.6% to 48.8% (P < .001).
Characteristics of Patients Before and After MDC Implementation. a
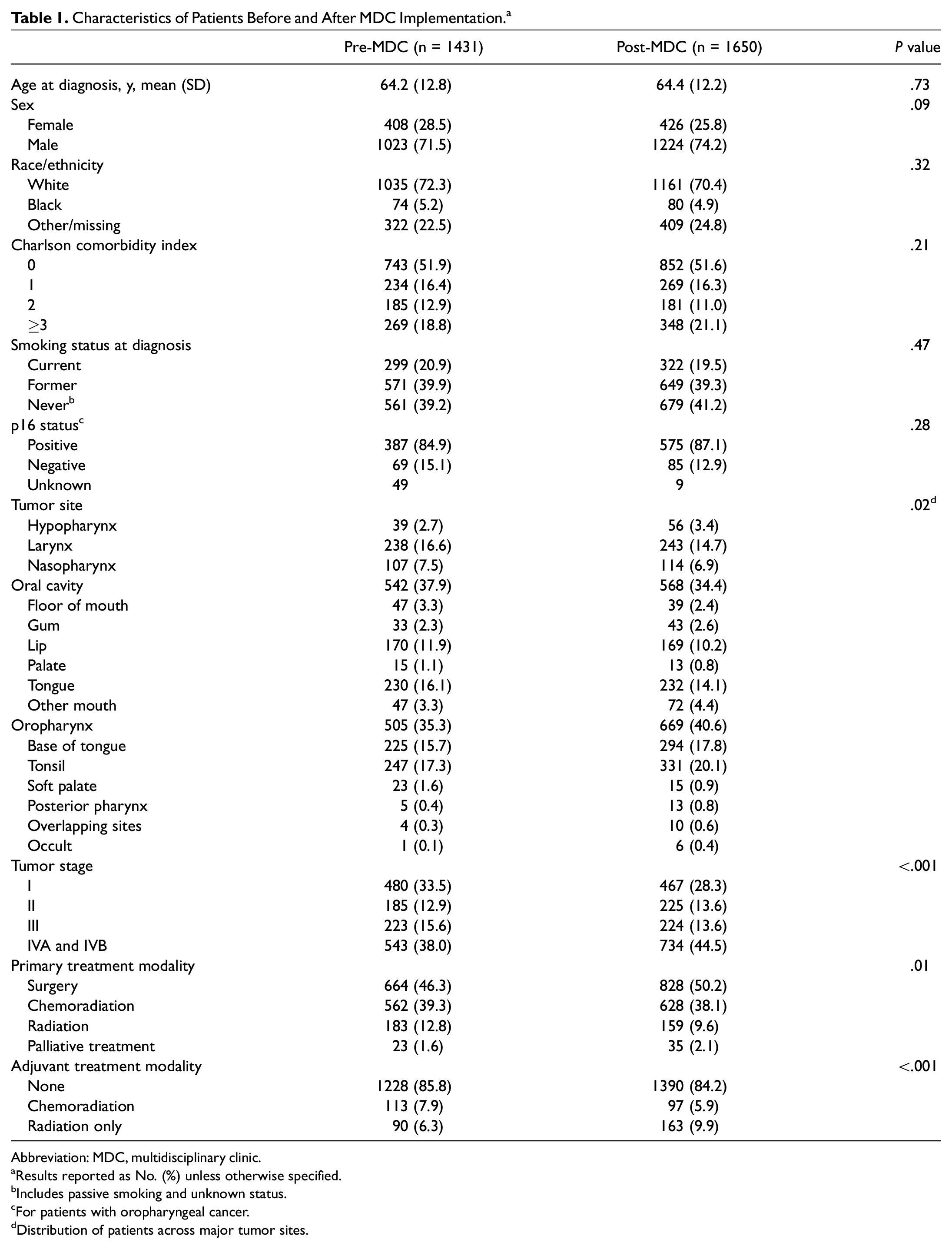
Abbreviation: MDC, multidisciplinary clinic.
Results reported as No. (%) unless otherwise specified.
Includes passive smoking and unknown status.
For patients with oropharyngeal cancer.
Distribution of patients across major tumor sites.
After MDC implementation, PET or PET/CT scan use before treatment initiation decreased among all patients, except those with advanced disease receiving primary surgical treatment ( Table 2 ), and imaging by any modality increased before treatment initiation, particularly among patients with early-stage disease receiving surgery as primary treatment ( Table 3 ). Use of pathologic staging after clinical staging increased from 46 (3.2%) patients preimplementation to 123 (7.8%) postimplementation (P < .001) due to the increased use of surgery, but the proportion of patients whose tumors were downstaged, upstaged, and remained at the same stage were equivalent over time.
PET or PET-CT Scan Use Before Treatment Initiation Pre- and Post-MDC Implementation. a
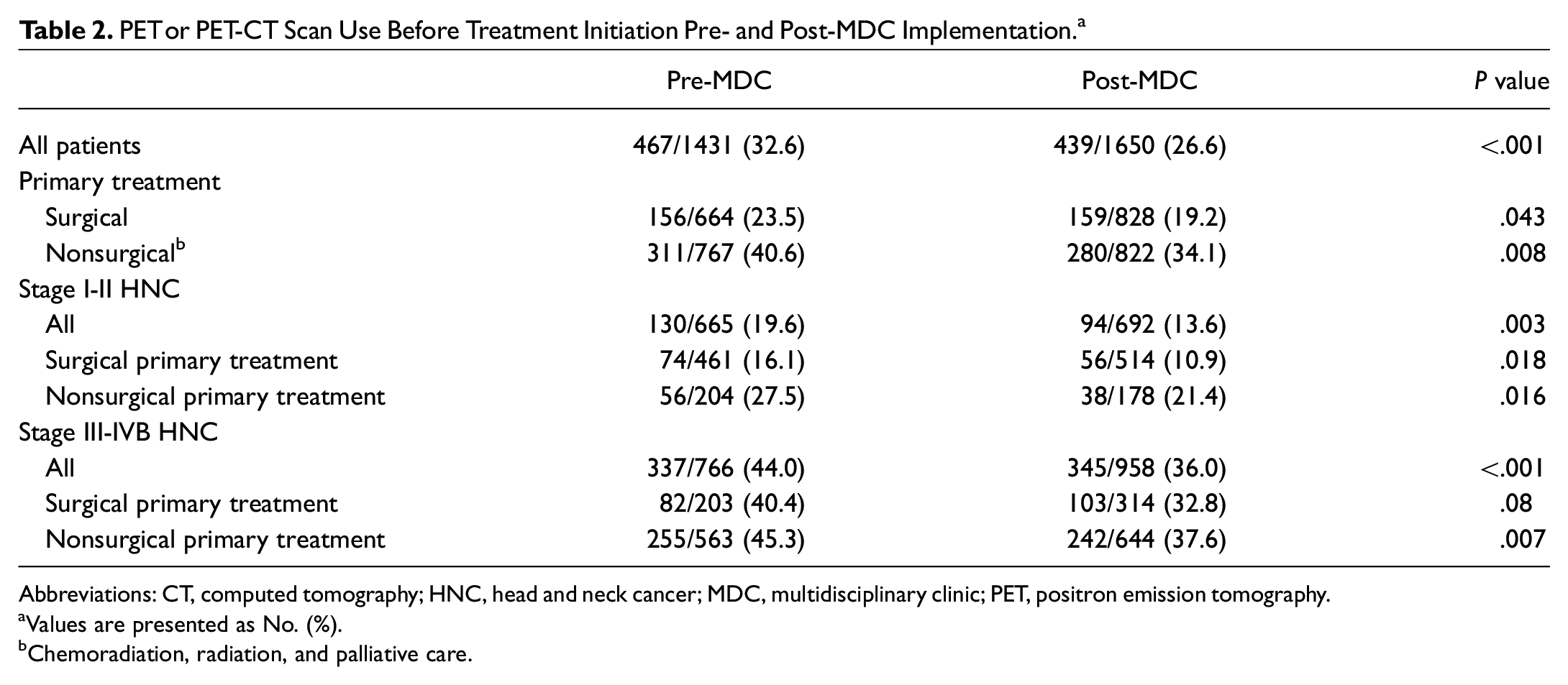
Abbreviations: CT, computed tomography; HNC, head and neck cancer; MDC, multidisciplinary clinic; PET, positron emission tomography.
Values are presented as No. (%).
Chemoradiation, radiation, and palliative care.
All Imaging Use Before Treatment Initiation Pre- and Post-MDC Implementation. a
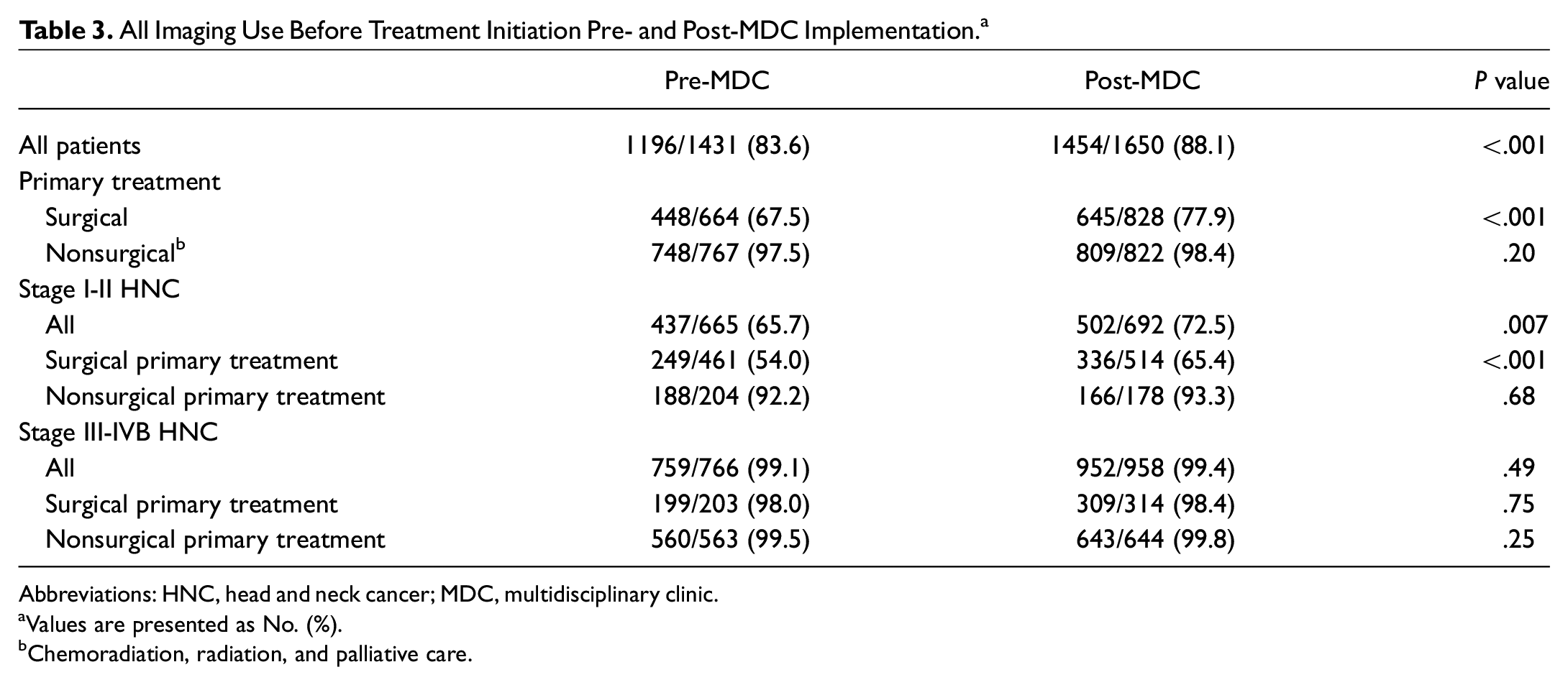
Abbreviations: HNC, head and neck cancer; MDC, multidisciplinary clinic.
Values are presented as No. (%).
Chemoradiation, radiation, and palliative care.
Based on the Kaplan-Meier method, OS and DSS were similar in both groups for the first 2 years and then lower among patients diagnosed with HNC preimplementation ( Figures 2 and 3 ). Three years after diagnosis, OS was 77.1% and 79.9% (P = .07) and DSS 84.9% and 87.5% (P = .05) among pre- and postimplementation patients, respectively. Three years after diagnosis, among patients with early-stage cancers, OS was 84.1% and 84.5% (P = .83) and DSS 93.5% and 94.4% (P = .53) pre- and postimplementation. Among patients with advanced-stage cancers, comparable estimates at 3 years were 71.0% and 76.5% (P = .014) for OS and 77.5% and 82.5% (P = .014) for DSS.
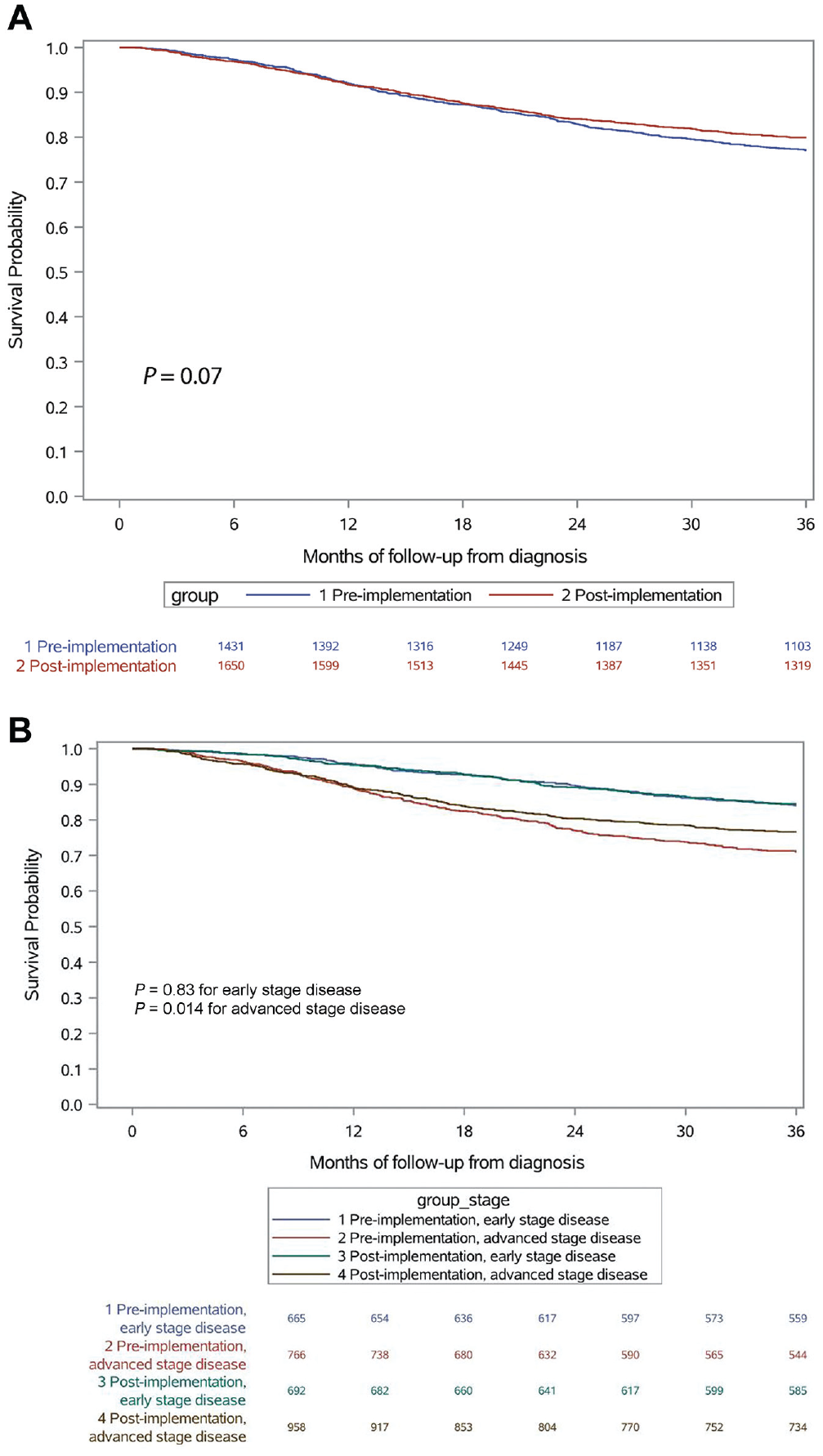
Overall survival before and after multidisciplinary clinic implementation.
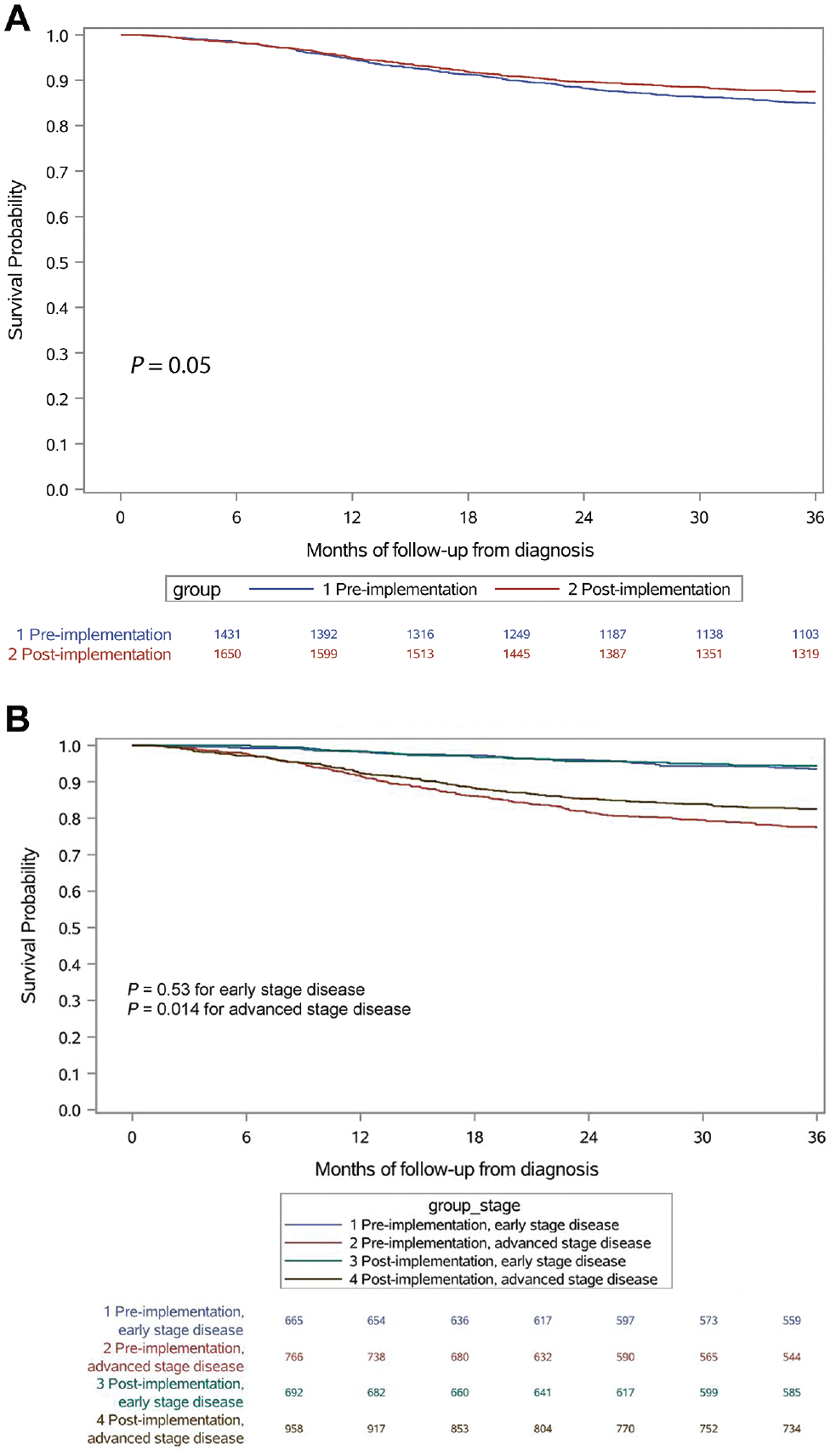
Disease-specific survival before and after multidisciplinary clinic implementation.
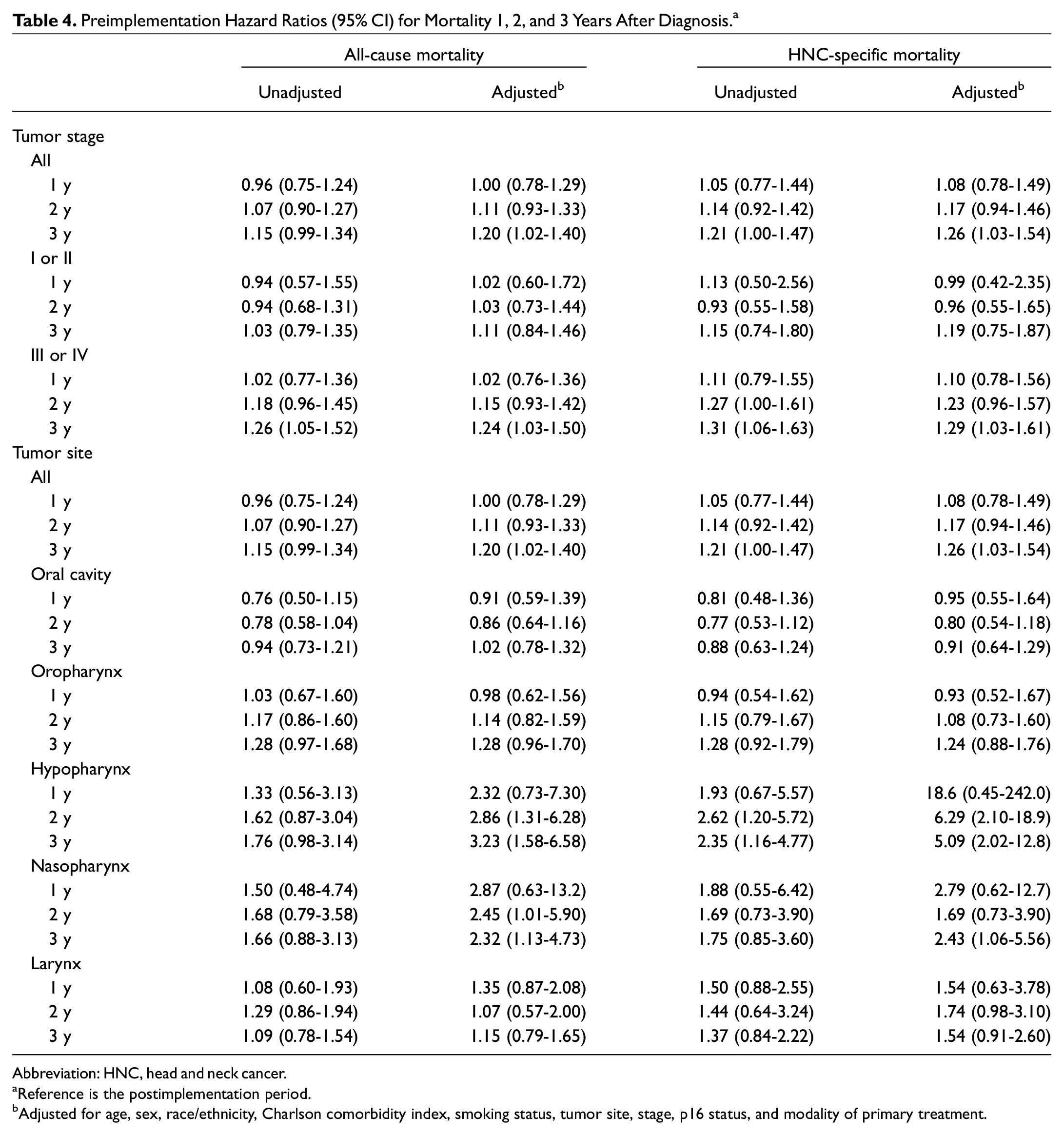
In multivariable regression analyses, no meaningful differences between pre- and postimplementation patients in OS and DSS were observed 1 or 2 years after diagnosis. However, 3 years after diagnosis, preimplementation patients had poorer OS (HR, 1.20; 95% CI, 1.02-1.40) and DSS (HR, 1.26; 95% CI, 1.03-1.54) than postimplementation patients. These associations were more pronounced for patients with advanced disease (Table 4). Although tumor site–specific associations appeared most pronounced for patients with nasopharyngeal and hypopharyngeal cancer, the relatively small number of patients in those groups affected the precision of estimates (Table 4).
Preimplementation Hazard Ratios (95% CI) for Mortality 1, 2, and 3 Years After Diagnosis. a
Abbreviation: HNC, head and neck cancer.
Reference is the postimplementation period.
Adjusted for age, sex, race/ethnicity, Charlson comorbidity index, smoking status, tumor site, stage, p16 status, and modality of primary treatment.
Subsequent regression models included treatment-related factors that might explain observed survival differences. When compared with patients diagnosed postimplementation, those diagnosed preimplementation were less likely to receive primary neck dissection as part of definitive surgical treatment (19.7% vs 26.9%, P < .001) and to have ≥18 lymph nodes resected (36.6% vs 63.4%, P < .001) and more likely to receive a noncisplatin regimen as part of definitive chemoradiation treatment (19.6% vs 13.1%, P < .01). After primary neck dissection was included in regression models, associations of pre- versus postimplementation with OS and DSS at 3 years remained largely unchanged. However, they moved slightly toward the null and became less statistically significant after separately adjusting for <18 or ≥18 resected lymph nodes (OS: HR, 1.17; 95% CI, 1.00-1.37; DSS: HR, 1.24; 95% CI, 1.01-1.51) and bolus cisplatin, weekly cisplatin, or noncisplatin chemotherapy (OS: HR, 1.17; 95% CI, 1.00-1.36; DSS: HR, 1.21; 95% CI, 0.99-1.48). Simultaneous adjustment for the number of resected lymph nodes and chemotherapy type also attenuated associations of pre- versus postimplementation with OS (HR, 1.15; 95% CI, 0.98-1.35) and DSS (HR, 1.20; 95% CI, 0.98-1.46).
Discussion
MDC implementation was associated with improved OS and DSS among HNC patients 3 years after diagnosis. Improvements were more pronounced among patients with advanced disease and those with nasopharyngeal and hypopharyngeal tumors. Observed improvements were related to ≥18 resected nodes and receipt of cisplatin versus noncisplatin chemotherapy, which occurred more frequently after implementation. After implementation, time from diagnosis to treatment initiation was unchanged, speech pathology consultations occurred more frequently, and PET and PET-CT scan use decreased.
A potential explanation for our findings is improved staging and treatment planning arising from the multidisciplinary care approach. Other reports note the effect of direct multidisciplinary collaboration on diagnostic and staging accuracy and treatment planning in patients with complex tumors.4,7 Decreased PET and PET-CT scan use after MDC implementation was consistent with workup recommendations, based on NCCN guidelines, developed to ensure appropriate imaging for referred patients. Pretreatment PET or PET-CT scans were recommended only for patients with stage III and IV tumors. MDC discussions also commonly supported avoiding treatment delay by proceeding on the basis of available imaging, such as a negative chest CT finding, rather than awaiting a PET or PET-CT scan.
A recent meta-analysis of cohort studies concluded that multidisciplinary team management in HNC care is associated with improved survival. 13 However, it included just 5 studies, 3 of which assessed the impact of multidisciplinary team management only in oral cavity tumors.11,14,15 Even less is known about its impact across multiple tumor sites. Liu et al found that a multidisciplinary tumor board was associated with improved 5-year OS and DSS for patients with oral cavity, oropharyngeal, laryngeal/hypopharyngeal, and nasopharyngeal tumors. 2 Friedland et al reported better 5-year survival (unspecified as OS or DSS) for patients with stage IV tumors in these locations, as well as nasal cavity/sinus and salivary gland tumors, and increased use of multimodal treatment. 9 In contrast, Patil et al found no effect on 2- or 5-year overall mortality among patients with oral cavity, oropharyngeal, nasopharyngeal/nasal cavity, and hypopharyngeal tumors. 4
Two previous reports noted that multidisciplinary team management had a greater impact on survival among patients with advanced HNC.9,14 Among nearly 17,000 patients with oral cavity cancer, OS benefits over 6 years by tumor stage were observed only for those with stage IV disease. 14 Similarly, among 726 patients with HNC in multiple sites, survival benefits were observed over 12 years for those with stage IV cancer; however, the analysis was inadequately powered to detect survival benefits of multidisciplinary team management among patients with stage I-III cancer. 9 Nevertheless, in the previously cited meta-analysis, a separate analysis of these reports found a trend toward the effectiveness of multidisciplinary management on survival among patients with stage IV disease that did not reach statistical significance. 13 Our findings expand on the evidence by confirming the differential effect of multidisciplinary team management on patients with more advanced disease and by defining advanced disease as including stage III cancer.
Reducing the time from diagnosis to treatment is a frequent goal of multidisciplinary team management in many types of cancer, 16 and time to treatment initiation is an independent predictor of survival in HNC.17,18 Median time from diagnosis to surgery in 2006 to 2014, the most recent interval for which data are reported, was 33 days (interquartile range, 21-49), up from 19 days in 1998.17,18 Time from diagnosis to treatment initiation of 61 to 90 days versus <30 days was associated with a 13% increase in mortality risk, with 67 days as the optimal threshold.6,18 A single study noted that treatment initiation >30 days after diagnosis was associated with better disease-specific and disease-free survival as compared with initiation <30 days after diagnosis. 19 We found that the interval between diagnosis and treatment initiation did not change after implementation, which may be due to our health care organization’s integrated nature.
The use of speech and language pathology consultations increased after implementation. Nearly half of all patients evaluated in the MDC received a consultation, as opposed to 2% in a national sample of Medicare patients with HNC. 20 Involving speech and language pathologists is important to optimizing speech and swallowing functions and improving quality of life among patients with HNC. 20 Patients in our study diagnosed after MDC implementation likely experienced similar benefits, but we did not directly assess these outcomes.
Strengths and Limitations
Study strengths were the use of Cox regression analyses adjusted for multiple covariates. Diagnosis, treatment, and disease status data were obtained from comprehensive chart reviews, minimizing the risk of data misclassification inherent in retrospective analyses. Our study is the first to assess the associations of MDC implementation with survival outcomes by HNC tumor site. However, despite our comparatively large study population, limited sample sizes and observed number of deaths for individual tumor sites affected our ability to assess site-specific variations in associations with survival. We also identified resection of ≥18 lymph nodes and delivery of cisplatin chemotherapy as accounting in part for observed differences in outcomes.
Other limitations were our inability to obtain complete radiation therapy data for patients who received it at contracted sites outside our organization. We were thus unable to assess the association with survival outcomes of radiation-related factors, such as shifts in care from general to head and neck–specialized radiation oncologists and use of conventional 3-dimensional conformal radiation therapy vs organ-sparing intensity-modulated radiation therapy or volumetric modulated arc therapy. Improvements in HNC treatment over time may have affected survival, regardless of MDC implementation. Organizational logistics precluded creating a contemporaneous control group. The increased proportion of patients receiving speech and language pathology consultations after implementation may have been a result of more patients presenting with advanced disease. Finally, our study took place in an integrated health care delivery system, and the findings may not generalize to other settings.
Conclusions
Among 3081 patients diagnosed with HNC at multiple tumor sites, MDC and case conference implementation was associated with improved outcomes, particularly for advanced-stage tumors, that were related to more consistent use of guideline-directed surgical and nonsurgical treatment. We found evidence of differential impact across tumor sites, but this finding may have been observed by chance and warrants confirmation in larger populations with contemporaneous control groups. The findings offer further evidence that MDC is most beneficial for patients with advanced disease, affirming the value of resource- and time-intensive multidisciplinary team management to improved survival.
Footnotes
Acknowledgements
We thank Jennifer Green for providing editorial assistance, Margaret Warton for support with initial data acquisition to facilitate chart review, and Daniel Fernandez and Kiranjit Grewal for retrieving and processing archived tumor blocks for p16 immunohistochemistry analysis.