
Abstract
The coronavirus 2019 pandemic has increased the use of powered air-purifying respirator (PAPR) devices, which produce appreciable noise levels during filtration. Our objective was to determine if active PAPR usage significantly impairs auditory communication in health care providers. We additionally sought to assess what volume of speech presentation was required for adequate communication with providers wearing a PAPR. In subjects with normal hearing at baseline, audiometric data demonstrated a 93% (95% CI, 86%-99%) decrease in word recognition scores during active PAPR usage. Presentation at 85 to 90 dB was needed to obtain word recognition scores similar to baseline in subjects with normal hearing without a PAPR. Pure tone averages also significantly decreased with PAPR usage, by 54 dB (95% CI, 46-62). Active PAPR usage has a substantial impact on auditory perception when utilized by health care providers. The potential longer-term effect of these devices on providers with regular active usage is of interest for future study.
Keywords
The coronavirus 2019 pandemic has led to an appreciable increase in the frequency, duration, and immediacy of personal protective equipment worn by health care providers. One form of protection recommended by the Centers for Disease Control and Prevention for clinicians who cannot wear traditional N95 respirator masks is the powered air-purifying respirator (PAPR) device, which propels air through filters into a fitted hood. 1 This filtration produces ambient noise, which may have a sound output of 74 dB within the respirator hood. 2 To place this into context, normal speaking volume is approximately 50 to 60 dB,3,4 a washing machine 70 dB, 3 and a motorcycle 95 dB, within this logarithmic scale. 3 In effect, PAPR usage exposes the wearer to noise slightly louder than a vacuum cleaner 5 during active filtration.
With these noise exposure levels in mind, as well as recent increases in PAPR usage amid the worldwide pandemic, it is important to determine if these devices contribute to barriers in communication during clinical interactions. We thus sought to query the null hypothesis that PAPR noise generation does not impede auditory communication during active provider usage. Our objective was therefore to determine if the use of a PAPR device significantly alters word recognition scores (WRSs) and pure tone hearing thresholds when worn by a health care provider. We additionally sought to assess what volume of speech presentation is required for adequate communication with a provider wearing a PAPR.
Methods
This study was designed to include adult English-speaking health care workers at least 18 years of age. Subjects had normal hearing and otologic histories. Exclusion criteria included previously diagnosed sensorineural or conductive hearing loss, hearing amplification device need, or prior otologic surgery. Audiometric status was confirmed via formal pure tone threshold and word recognition testing at the outset. All subjects participated voluntarily in this study, which met criteria to proceed as determined by the Mass General Brigham Institutional Review Board.
Sound field testing was performed in a sound-proof room utilized for standard audiometric testing in a tertiary care clinic. The difference in WRS in the better-performing ear was the primary outcome. WRSs were assessed as the percentage of correctly identified words according to standard prerecorded speech audiometry. 6 WRSs were measured without the PAPR (baseline) at a presentation level of 55 dB and comparatively with active PAPR usage at 55, 80, 85, and 90 dB. During these assessments, 92% word recognition was considered adequate for successful communication. 7 Pure tone threshold measurements were obtained at baseline and with active PAPR usage at 250, 500, 1000, 2000, 4000, and 8000 Hz. Pure tone averages (PTAs) were calculated according to previously described methods. 8 Pure tone results also focused on the better-hearing ear. The ILC Dover HP Sentinel S-2001 with CBRN hood PAPR was used throughout testing. Data were appropriate for parametric analysis based on assessments of skew and kurtosis 9 and were analyzed with Stata 15.0 (StataCorp).
Results
Data from 5 subjects demonstrated a WRS ≥92% during baseline testing and pure tone thresholds of 0 to 15 dB without the PAPR (baseline). With active PAPR usage, however, there was a statistically significant decrease in WRS; when sound was presented at 55 dB, the WRS decreased by 93% (95% CI, 86%-99%; Table 1 , Figures 1 and 2 ; Appendix, available online). No subject could correctly identify >3 words in a 25-word list (12%) when presented at a volume considered typical for communication (55 dB). Presentation at 85 to 90 dB was needed to obtain WRSs similar to baseline in the better-hearing ear. PTAs were also significantly decreased with active PAPR usage, worsening by a mean 54 dB (95% CI, 46-62 dB).
Differences in Word Recognition Score and Pure Tone Average With and Without Active PAPR Usage.

Abbreviation: PAPR, powered air-purifying respirator.
Scores are reported as mean ± SE (95% CI).
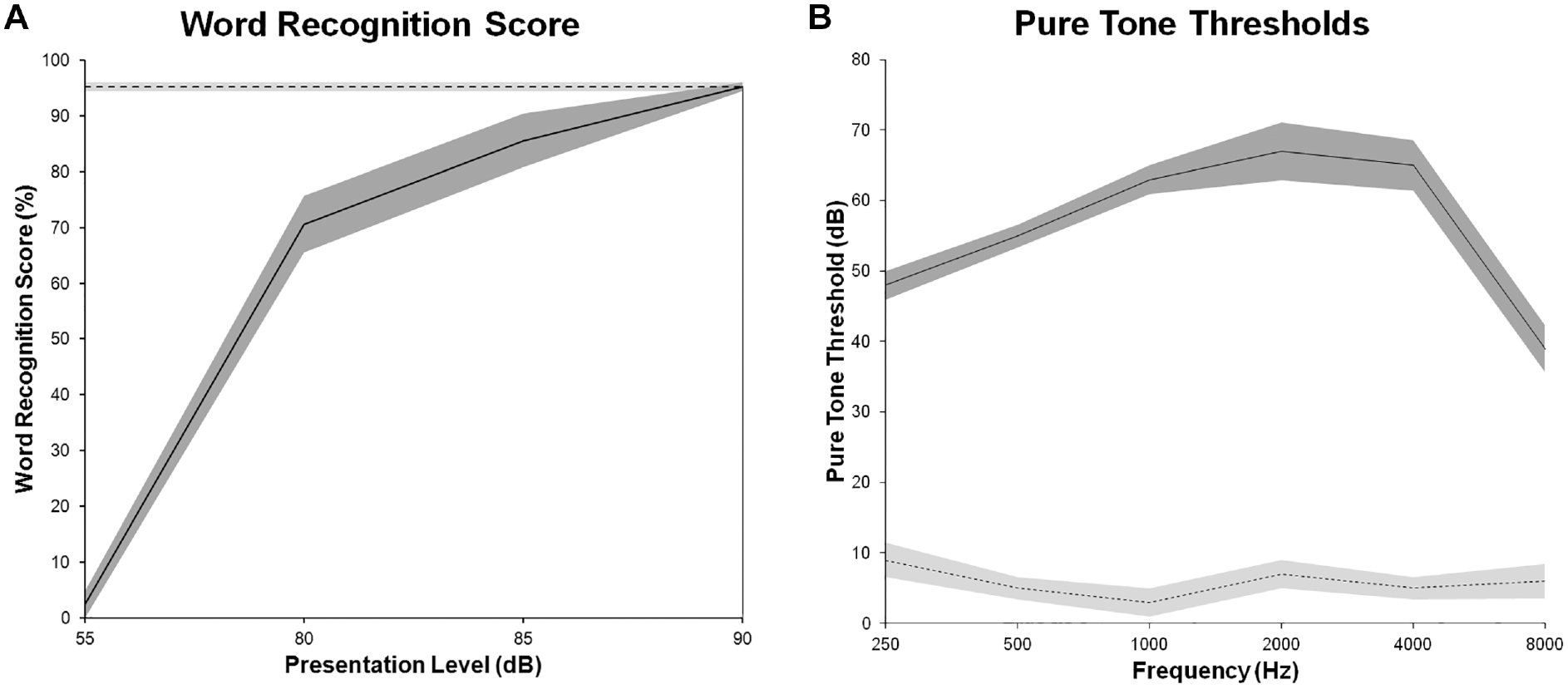
(A) Word recognition scores and (B) pure tone thresholds with and without active PAPR usage. Solid line, with PAPR. Dashed line, without PAPR. Shaded region, standard error. PAPR, powered air-purifying respirator.
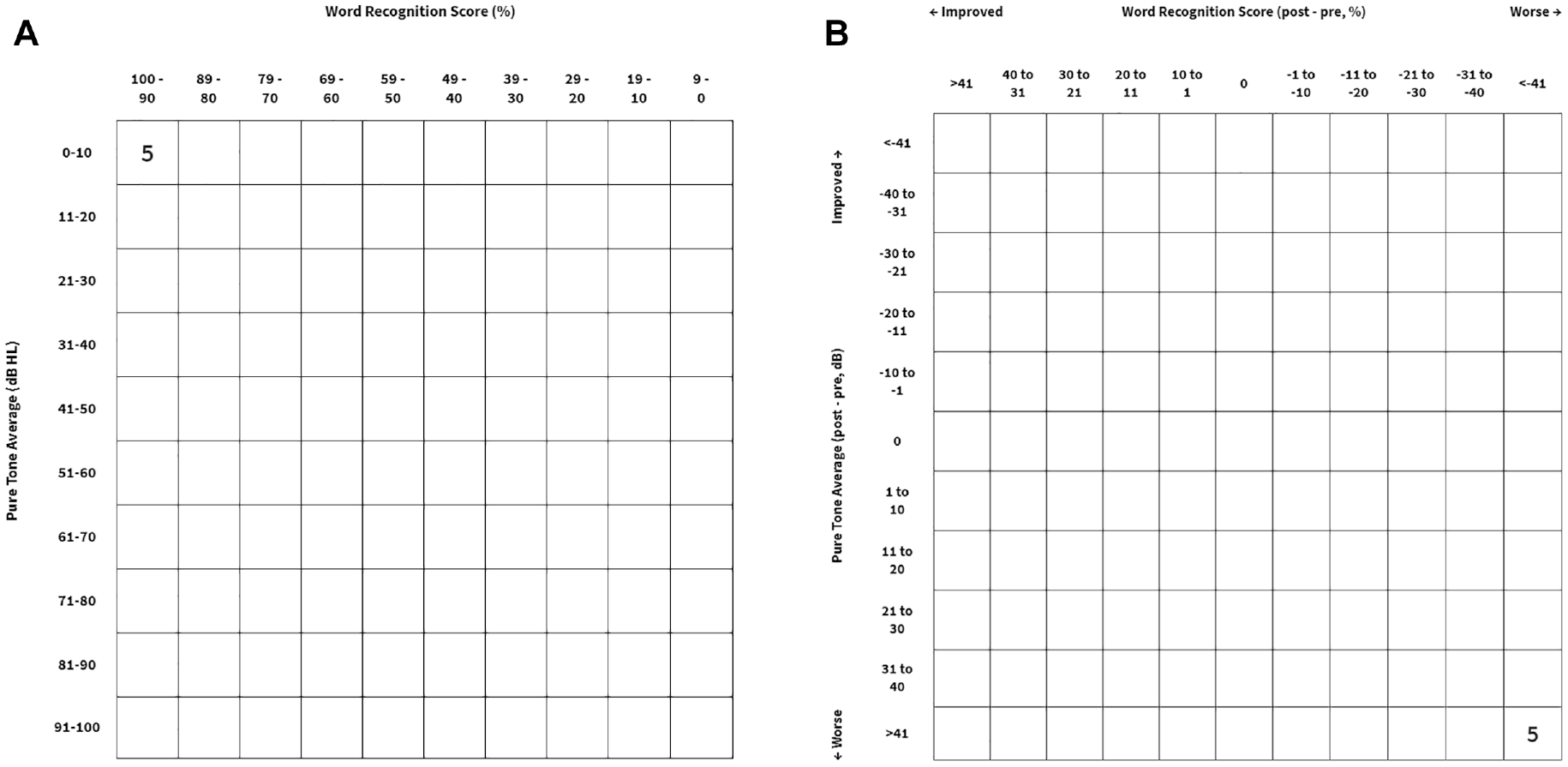
Scattergram (A) without and (B) with active powered air-purifying respirator usage.
Discussion
These data suggest that active PAPR usage amid the pandemic creates a substantial barrier for hearing thresholds and communication. For words presented at 55 dB when the device is worn, WRS declined by an average of 93%, and PTA worsened by 54 dB. Among audiologists and otolaryngologists, such measurements inherently raise concern for communication ability. The volume of speech required for normal WRS was approximately 30 dB louder than typical speaking volume, comparable to a motorcycle or lawnmower. 2
In acute health care settings such as emergency departments, operating rooms, and intensive care units, where unhindered communication is vital, it may be difficult for providers to maintain speech volumes at this level. It could also introduce concerns related to patient privacy, vocal strain/overuse, and the potential for noise-induced problems. 3 In addition, during active usage in the hospital, overall effects may be worsened amid concurrent background noise. The potential otolaryngological impact of PAPR usage is thus a compelling area for future study.
Prolonged exposure to noise when the PAPR is worn for entire work shifts may also be a consideration. The Centers for Disease Control and Prevention cautions that auditory damage can occur after 2 hours of exposure to sounds between 80 and 85 dB. 3 The National Institute for Occupational Safety and Health recommends that occupational noise exposure not exceed 85 dB over an 8-hour time-weighted average. 10 The World Health Organization and US Environmental Protection Agency describe a lower limit, recommending that environmental noise not exceed 75 dB over 8 hours in an attempt to prevent noise-induced hearing loss. 3 Studying the impact of prolonged PAPR usage (74 dB) on hearing may thus be a worthy future endeavor.
Conclusion
Active PAPR usage has a significant impact on auditory perception when utilized by health care providers. The potential longer-term impact of these devices on providers with regular usage is of interest for future study.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211058350 – Supplemental material for Impact of Powered Air-Purifying Respirator Devices on Word Recognition in Health Care Providers
Supplemental material, sj-docx-1-oto-10.1177_01945998211058350 for Impact of Powered Air-Purifying Respirator Devices on Word Recognition in Health Care Providers by Emily J. Moldoff, Miranda K. Eubank, Anne Y. Feng, C. Eduardo Corrales and Jennifer J. Shin in Otolaryngology–Head and Neck Surgery
Footnotes
Author Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.