
Abstract
Objective
Consumer wearables, such as the Apple Watch or Fitbit devices, have become increasingly commonplace over the past decade. The application of these devices to health care remains an area of significant yet ill-defined promise. This review aims to identify the potential role of consumer wearables for the monitoring of otolaryngology patients.
Data Sources
PubMed.
Review Methods
A PubMed search was conducted to identify the use of consumer wearables for the assessment of clinical outcomes relevant to otolaryngology. Articles were included if they described the use of wearables that were designed for continuous wear and were available for consumer purchase in the United States. Articles meeting inclusion criteria were synthesized into a final narrative review.
Conclusions
In the perioperative setting, consumer wearables could facilitate prehabilitation before major surgery and prediction of clinical outcomes. The use of consumer wearables in the inpatient setting could allow for early recognition of parameters suggestive of poor or declining health. The real-time feedback provided by these devices in the remote setting could be incorporated into behavioral interventions to promote patients’ engagement with healthy behaviors. Various concerns surrounding the privacy, ownership, and validity of wearable-derived data must be addressed before their widespread adoption in health care.
Implications for Practice
Understanding how to leverage the wealth of biometric data collected by consumer wearables to improve health outcomes will become a high-impact area of research and clinical care. Well-designed comparative studies that elucidate the value and clinical applicability of these data are needed.
Wearable technology (“wearables”) represents a broad field of biosensor-based devices worn close to the skin to unobtrusively monitor an individual’s activities. 1 Modern consumer wearables, such as the Apple Watch Series 6 or Fitbit Charge 2, interpret and transmit these data to a smartphone or centralized database, allowing individuals to track unique parameters of health and wellness over extended periods. The market for consumer wearables has experienced significant levels of expansion: per the International Data Corporation, 444.7 million wearable units were shipped in 2020, representing a year-over-year increase of 27.2%. 2 As of 2020, approximately 30% of adults in the United States endorsed using a wearable, of whom half use the device daily. 3
Though consumer wearables were widely adopted in lifestyle and fitness markets over the past decade, research into the application of wearable technology within health care has only recently accelerated. 4 The interest among clinical researchers in these devices largely arises from their ability to provide passive monitoring of biometric data, defined as data relating to characteristics that are specific to an individual: physiologic (eg, heart rate, body temperature) and behavioral (eg, daily step count, number of hours of sleep). 5 Many new-generation consumer wearables integrate multiple sources of biometric data to allow for detailed and comprehensive quantification of an individual’s health status. Consequently, health systems have begun to adopt consumer wearables as a tool to promote precision medicine. 6 Several hospital systems have partnered with wearable technology companies to develop platforms that support the interoperability of wearable-derived data with electronic health records. 7 These programs stand to potentially transform health care delivery by empowering patients’ self-management and improving universal accessibility to care.8,9 Clinicians should consider how the adoption of consumer wearables into their practices might benefit their specific patient populations. Though prior studies across various surgical fields have employed consumer wearables for prediction of postoperative outcomes,10-16 no research to date has explored the applications of these devices in otolaryngology. This review highlights the potential role of consumer wearables for patient monitoring in otolaryngology and briefly addresses the barriers and ethical considerations surrounding their adoption in health care.
Methods
An initial Google search was performed to identify all wearable devices approved by the Food and Drug Administration and/or commercially available for consumer purchase in the United States as of June 4, 2021. Key attributes of each device were documented (eg, form factor, sensors, and passively captured parameters). From this list of parameters, we identified the following as relevant to the delivery of patient care in otolaryngology: heart rate, respiratory rate, skin temperature, blood pressure, blood oxygenation levels, blood glucose levels, physical activity data (step count, energy expenditure, distance traveled, hours of active and sedentary time), and sleep data. After further discussion, we conceived the following list of theoretical parameters, which were not explicitly captured by any of the devices from the initial search but could nonetheless improve delivery of care: pain qualification, blood calcium levels, and gait/balance.
A search strategy was developed combining keyword and Medical Subject Headings terms related to wearable technology or clinically relevant parameters (Supplemental Materials 1, available online). Searches were conducted in the PubMed database June 4 to 11, 2021. Manuscripts were excluded for the following reasons: article is (1) not peer reviewed or (2) in English language; (3) wearable device is not designed for continuous long-term wear; (4) wearable device does not passively capture at least 1 biometric parameter relevant to otolaryngology; (5) wearable device is designed exclusively for therapeutic purpose; (6) wearable technology has been ubiquitous in clinical care prior to the past decade (eg, Holter monitors, pedometers); or (7) wearable technology is not available for consumer purchase, including devices that are exclusively built for use in research settings. As a caveat to this final exclusion criterion, articles were included if they described the use of a research-grade device with a biosensor that is also found in a consumer wearable. The PubMed search was complemented by scanning the references of articles that met inclusion criteria. Nonhuman subject research articles were sought to supplement the discussion and form the basis of the section on barriers and ethical considerations surrounding consumer wearables. Data from articles were synthesized into a final review.
The first 2 authors independently appraised the quality of articles that serve as primary evidence of the potential applications of consumer wearables or one of the listed biometric parameters to clinical care. Randomized controlled trials were assessed with the Cochrane Risk of Bias Tool for Randomized Trials (RoB 2.0). Systematic reviews were assessed via the Risk of Bias Assessment Tool for Systematic Reviews. To our knowledge, there is no established tool for evaluating the risk of bias in observational single-cohort studies. As such, we adapted the Quality Assessment Tool for Observational Cohort and Cross-sectional Studies (National Institutes of Health) to evaluate these studies. Final decisions were reached via consensus between the first 2 authors. Tables displaying the risk of bias for each tool-specific domain and overall risk of bias for each manuscript are presented in Supplemental Materials 2 (available online). Given the paucity of literature employing consumer wearables to measure the identified parameters in perioperative care, we did not categorically exclude articles based on the strength of the methodological quality. Instead, where appropriate, we have emphasized the areas where there is limited robust evidence to conclusively support the use of wearable technology for a given purpose.
Discussion
Table 1 highlights key attributes of select consumer wearables that have been previously applied to patient monitoring. Triaxial accelerometers and optical heart rate sensors are the most common biosensors within consumer wearables. 6 Nonetheless, there remains large variability across consumer wearables regarding form factor and combination of biometric parameters captured. An in-depth discussion on the mechanism by which consumer wearables obtain and transmit biosensor data is beyond the scope of this review.
Key Features of Consumer Wearables Previously Applied to Patient Monitoring. a
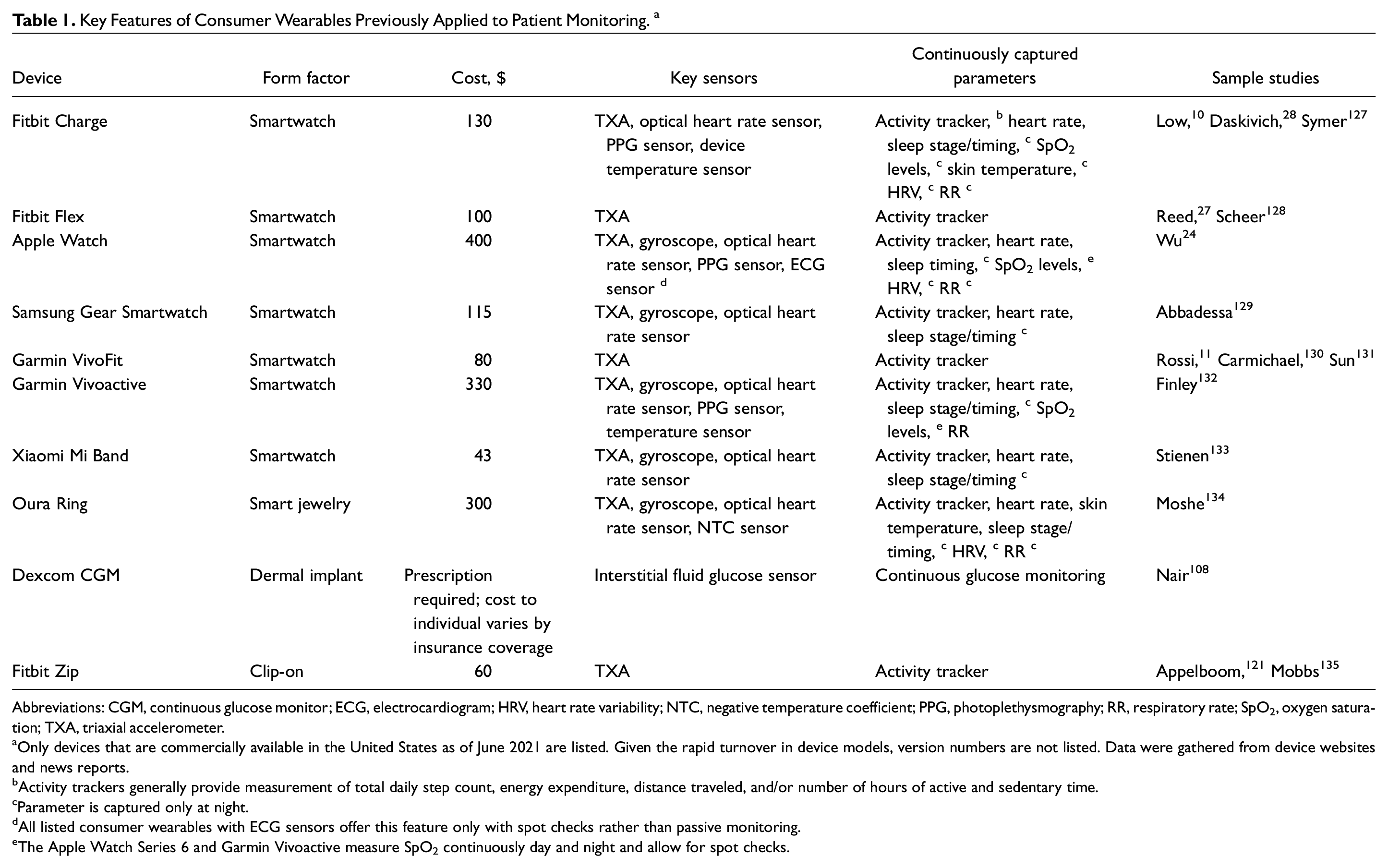
Abbreviations: CGM, continuous glucose monitor; ECG, electrocardiogram; HRV, heart rate variability; NTC, negative temperature coefficient; PPG, photoplethysmography; RR, respiratory rate; SpO2, oxygen saturation; TXA, triaxial accelerometer.
Only devices that are commercially available in the United States as of June 2021 are listed. Given the rapid turnover in device models, version numbers are not listed. Data were gathered from device websites and news reports.
Activity trackers generally provide measurement of total daily step count, energy expenditure, distance traveled, and/or number of hours of active and sedentary time.
Parameter is captured only at night.
All listed consumer wearables with ECG sensors offer this feature only with spot checks rather than passive monitoring.
The Apple Watch Series 6 and Garmin Vivoactive measure SpO2 continuously day and night and allow for spot checks.
There are numerous potential applications of consumer wearables for monitoring otolaryngology patients, such as assessment of mobilization, postoperative pain, sleep quality and timing, and ambulatory blood pressure. These devices may allow for enhanced detection of postoperative complications, such as surgical site infections, perioperative glucose abnormalities, and postoperative hypotension ( Figure 1 ). These applications are detailed in turn.
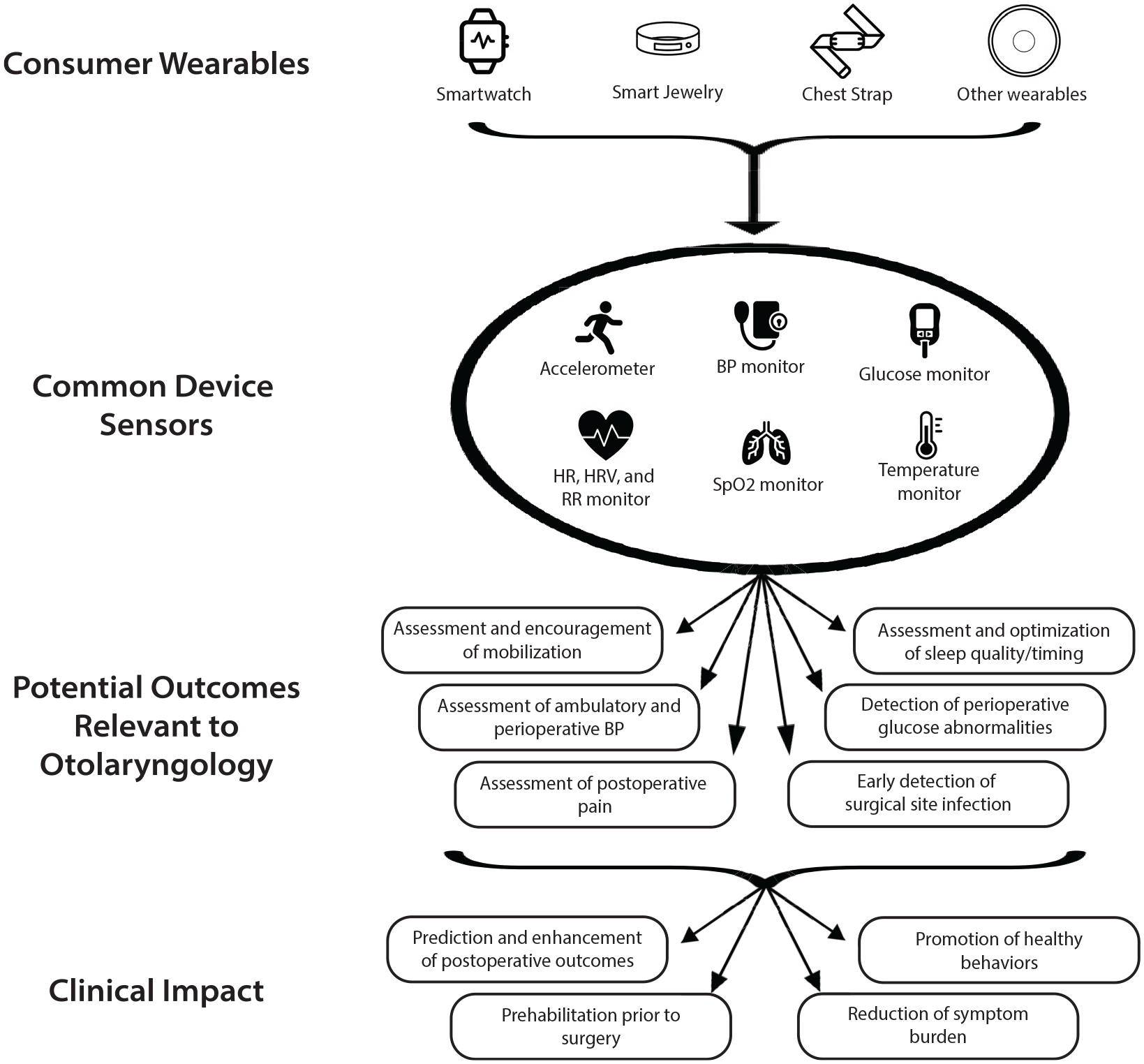
Potential applications of consumer wearables for patient monitoring in otolaryngology. BP, blood pressure; HR, heart rate; HRV, heart rate variability; RR, respiratory rate; SpO2, oxygen saturation.
Assessment and Encouragement of Mobilization
Postoperative ambulation has been suggested to reduce complications after major surgery, such as resection and free flap reconstruction of head and neck cancer (HNC). 17 As such, early postoperative mobilization remains a core principle of all ERAS guidelines (enhanced recovery after surgery). 18 Nonetheless, assessment of inpatient mobilization has traditionally relied on the imprecise recollections of the patient and hospital care team. Accurate measurement of inpatient physical activity level could allow for a better understanding of the degree to which postoperative mobilization may be considered safe and beneficial within distinct otolaryngology surgical populations. 19 Many modern consumer wearables employ triaxial accelerometers to provide an estimate of select parameters of physical activity, such as step count, calorie expenditure, and distance traveled.20,21 Emerging research across various surgical populations has identified that these parameters may predict the risk of readmission,10-12,22,23 hospital length of stay,13,24-28 postoperative complications,11,12,14 and patient-reported outcome measures15,16,29-33 (Supplemental Table S1, available online), though the strength of evidence supporting these findings is mixed. Inpatient monitoring via consumer wearables potentially permits indirect assessment of factors contributing to diminished mobilization, such as postoperative pain, thereby prompting tailored interventions. 34
Though prior research on consumer wearables in the inpatient postoperative setting remains limited, extensive literature over the past decade has evaluated the application of these devices in the outpatient setting, often as components of structured behavioral change programs.35,36 These interventions tend to evaluate whether real-time biofeedback provided by consumer wearables, whether alone or in combination with other behavioral incentives, promotes increased physical activity and decreased sedentary behavior. Within the field of otolaryngology, poor preoperative functional performance has been associated with a significantly higher rate of unplanned 30-day readmissions after HNC surgery. 37 Behavioral interventions incorporating consumer wearables could optimize preoperative mobilization as a means of prehabilitation. Of note, there is conflicting evidence surrounding the efficacy of prehabilitation: though several studies across various surgical fields suggest that prehabilitation may shorten hospital length of stay38,39 and reduce the risk of postoperative complications,40,41 others report that prehabilitation does not improve postoperative outcomes.42-47 Though there has been some focus on prehabilitation to reduce swallowing dysfunction among patients with HNC, 48 to our knowledge, no published literature has evaluated the effect of exercise prehabilitation on postoperative outcomes in this population. 49 Assessment of baseline preoperative physical activity level could also allow for the development of tailored activity goals in the immediate and extended postoperative setting. 50 This could be particularly beneficial for patients with HNC, as exercise is a known alleviating factor for cancer-related fatigue, which often lasts for months to years after curative treatment.51,52 The success of these interventions rests on their ability to incentivize sustained patient engagement with prescribed behaviors, a notoriously difficult feat. 53 Nonetheless, the use of consumer wearables for assessment and promotion of physical activity among otolaryngology patients remains a clear avenue for future research.37,54
Assessment of Postoperative Pain
Postoperative pain is a common phenomenon after major surgery that has been suggested to increase the risk for pulmonary complications and the development of chronic pain.17,55,56 Though pain management is a core component of ERAS protocols, what constitutes appropriate perioperative pain management and how this is best assessed remains a topic of debate and public scrutiny.57-59 Overprescribing of narcotics in the perioperative setting has been implicated as contributing to the nation’s opioid epidemic. Opioids were responsible for nearly 70,000 overdose deaths in 2020 alone. 60 Otolaryngologists and other surgeons face the challenge of adequately treating acute pain needs while recognizing their role in preventing broader deleterious health trends.
Pain is a complex biopsychosocial phenomenon unique to the individual, yet assessment of pain is traditionally restricted to unidimensional metrics, such as the Numeric Pain Rating Scale. However, these measures are subject to various cognitive biases and cannot be reliably captured in certain noncommunicative patient populations. 61 The Joint Commission recognizes the limitations in metrics such as the Numeric Pain Rating Scale and encourages development of comprehensive assessments that incorporate the impact of pain on physical function. 62 Given the known association between pain and delayed mobilization after major surgery, it is tempting to look to step count as measured by consumer wearables as a proxy indicator of postoperative pain levels. 34 However, the degree to which accelerometry data correlate with reported pain scores remains disputed. 61 Thus, while accelerometry may provide some insight, these data alone are likely insufficient to characterize postoperative pain levels.
Alternatively, since pain is known to induce a sympathetic autonomic response, it may be possible to assess postoperative pain by assessing and trending physiologic markers that are continuously captured by many consumer wearables. 63 Specifically, increased pain has been associated with changes to resting heart rate and heart rate variability (HRV), a widely used metric of autonomic nervous system function. 64 Select consumer wearables with optical heart rate sensors deliver an approximation of heart rate and HRV by using reflective photoplethysmography, a technique in which changes in blood volume are measured by the amount of light reflected off illuminated skin.65,66 Other devices report a direct estimate of HRV via single-lead electrocardiogram.6,64 By continuously trending these parameters of autonomic function, consumer wearables could establish a patient’s preoperative baseline values and theoretically allow for better delineation of the timing and intensity of postoperative pain episodes.
Nonetheless, biometrics such as heart rate or HRV may be influenced by any source of sympathetic stimulation, such as inflammation, emotional stress, or physical activity. 67 Consequently, their specificity in identifying or quantifying postoperative pain remains low, especially in the outpatient setting. 68 The ability of artificial intelligence to predict subjective levels of pain from composite algorithms incorporating electrocardiogram data, skin temperature, accelerometry data, and/or galvanic skin response appears promising,69-72 though the generalizability of these findings is questionable due to the use of simulated pain in healthy volunteers. These findings require validation in real-world assessments among patients with actual pain. 73 Thus, while the inclusion of objective biometric parameters to complement the evaluation of postoperative pain remains an area of significant interest, there exists no widely available tool to support clinicians to this end.
Assessment of Sleep Quality and Timing
Sleep is a vital function of life that is closely tied to physical health and quality of life. 74 Hospitalized patients are frequently subject to a variety of sleep disturbances, such as environmental noise and routine overnight measurement of vital signs. Sleep disturbances are especially common among patients with HNC, resulting in an elevated risk for postoperative delirium.75,76 Furthermore, the stress from poor sleep when coupled with surgical stress may prolong postoperative recovery. 77 Though measurement of sleep parameters in all hospitalized patients by polysomnography would be cost inefficient, infeasible, and poorly tolerated, sleep quality is rarely assessed even by subjective metrics. 78 Consumer wearables present a novel method by which sleep quality and timing may be unobtrusively assessed in the perioperative setting. Many modern consumer wearables incorporate data from triaxial accelerometers and optical heart rate sensors into proprietary integrative algorithms to provide estimates of various sleep parameters, including total sleep time, wake after sleep onset, and sleep efficiency. 79 Though prior literature has suggested that consumer wearables tend to overestimate total sleep time and sleep efficiency as compared with polysomnography, recent studies on new-generation devices that incorporate multisensor data have demonstrated high validity that rivals many research-grade devices.80,81 As such, consumer wearables remain a viable option for the assessment of perioperative sleep quality and could allow for tailored interventions in the inpatient setting to promote sleep hygiene. 82
Wearable-derived data on sleep quality and timing could be similarly used in the outpatient setting, especially in select populations that are known to suffer from poor sleep, such as patients with obstructive sleep apnea-hypopnea syndrome (OSAHS) or chronic rhinosinusitis. 83 Identification of parameters suggestive of persistent poor sleep quality or increased cardiovascular risk could theoretically persuade patients to adhere to recommended treatment plans.84,85 Importantly, real-time feedback delivered by consumer wearables must be coupled with patient education and may require additional behavioral incentives to promote patient engagement. Broadly, there is a significant need for prospective research evaluating behavioral interventions incorporating consumer wearables to promote patients’ adoption of healthy sleep habits. 86
There is ongoing research into the ability of consumer wearables to detect clinically relevant OSAHS parameters, such as sleep stage timing and number of nightly apneic episodes.87-89 Though the application of artificial intelligence deep learning algorithms incorporating wearable-generated data appears promising, this is a growing area of research for which the evidence base remains limited. Modern consumer wearables remain limited in their ability to assess these parameters and should not yet be considered substitutes for gold standard polysomnography.90,91
Assessment of Ambulatory Blood Pressure
Primary hypertension is seen in nearly half of adults in the United States and contributes to an elevated risk of stroke, myocardial infarction, and mortality, especially in the perioperative setting.92-95 Select cuff-based wristwatches, such as the Omron HeartGuide, provide an intermittent reading of ambulatory blood pressure. 96 Other consumer wearables, such as the Biobeat wrist monitor, continuously track blood pressure via reflective photoplethysmography.97,98 These devices have not been studied in the preoperative setting, where they could facilitate prehabilitation or prediction of clinical outcomes before major surgery. By trending patients’ blood pressure in the days to weeks prior to surgery, otolaryngologists and anesthesiologists may obtain a better impression of their baselines, potentially reducing the rate of same-day surgery cancellations due to uncontrolled hypertension. 99 Alternatively, given the known association between OSAHS and incident hypertension, ambulatory blood pressure readings gathered from consumer wearables could be integrated into metrics of clinical success after sleep surgery. 100 Finally, continuous blood pressure monitoring could be incorporated as part of a larger behavioral intervention to influence patients’ adherence to continuous positive airway pressure therapy, which has been demonstrated to mitigate the risk of hypertension in patients with OSAHS. 101
Enhanced Detection of Postoperative Complications
Consumer wearables could serve to complement data collection among patients in the hospital general ward. Through their advantage of continuous passive observation, these devices may trend data that are otherwise captured at only select intervals, thereby allowing for early recognition of markers suggestive of postoperative complications. Prior literature has suggested that continuous inpatient monitoring with wearable devices, when coupled with automated alerts in the setting of clinical deterioration, may result in improved patient outcomes.102,103
Postoperative surgical site infection is a common complication that significantly influences morbidity and mortality among patients with HNC. 104 Infection status in hospitalized patients on the general ward is traditionally assessed via intermittent physical examination and monitoring of vital signs. Yet, physiologic parameters suggestive of a postoperative infection may develop in only the interval between vital sign checks, resulting in a delay to treatment. 102 A randomized controlled trial by Downey et al found that a nonconsumer wearable patch with continuous vital sign monitoring allowed for earlier administration of antibiotics after evidence of sepsis and lower 30-day readmission rates. 105 However, no studies to date have specifically applied consumer wearables for identification of infection in the postoperative setting. Therefore, the ability of consumer wearables to detect derangements in physiologic parameters suggestive of postoperative infection or sepsis is an area of potentially high-impact future research.
Perioperative hyperglycemia represents a significant predictor of surgical complications, medical complications, and surgical site infections among patients with HNC undergoing microvascular reconstruction. 106 Inpatient blood glucose monitoring is typically performed by taking a finger-prick blood sample at select intervals, though this allows for significant gaps during which glucose levels are not assessed. Moreover, these methods are invasive and inconvenient, especially for patients who require blood glucose monitoring several times daily. 4 Though continuous glucose monitors (CGMs) such as the Dexcom G6 have been widely adopted in the ambulatory setting, the potential application of these devices within the inpatient setting has not been well explored.107,108 In a recent study, Davis et al identified via pooled analysis that CGM technology may serve as a reliable tool for use among noncritically ill hospitalized patients.109,110 Thus, the ability to transmit interstitial glucose levels from a patient’s CGM to the surgical team could allow for improved inpatient blood glucose management and optimization during postoperative recovery.
Postoperative hypotension is frequently seen among surgical patients and has been associated with increased risk of myocardial injury, acute kidney injury, and mortality.111,112 Current data suggest that postoperative hypotension after major surgery is frequently undetected in the general care ward. 111 Therefore, continuous inpatient monitoring by consumer wearables coupled with automated alerts to the care team could permit early detection and intervention in the setting of critically low or elevated blood pressure readings.
Barriers and Ethical Considerations Surrounding Adoption of Consumer Wearables in Health Care
There remain various limitations and ethical considerations that must be addressed before the widespread integration of consumer wearables in clinical care. Notably, there are many concerns regarding the privacy and ownership of wearable-generated health data. Biometric data collected by consumer wearables currently fall in a gray area within the bounds of the Health Insurance Portability and Accountability Act (HIPAA). 113 Wearable-derived data that are shared with health care organizations or integrated into electronic health records must be protected and stored in a HIPAA-compliant manner. As such, many wearable tech companies are building HIPAA-compliant platforms, such as Google Fit and Apple HealthKit, which support the interoperability of wearable-derived data with electronic health records. 7 As these partnerships develop, wearable tech companies and health systems must ensure that the transfer of data across platforms remains secure against the risk of leakage and tampering.114,115 Data that are solely gathered for consumer use do not fall under the purview of HIPAA. Consequently, many wearable tech companies have historically required users to give up their right to privacy over wearable-generated health data, allowing these companies to potentially take advantage of these data for commercial use or targeted advertising.9,116 There is a pressing need for the development of a legal infrastructure that delineates the rights and responsibilities of these companies regarding patient-generated health data. 117
The use of wearable-derived health data by insurance companies is another area of concern. Many health and life insurance companies are increasingly offering their customers discounts on consumer wearables or their insurance premiums if certain activity targets are met. While this could be viewed as a move to promote healthy behaviors and reduce future payouts, it is certainly possible that insurers could use data suggestive of poor health or lifestyle habits to penalize customers with risk-adjusted higher premiums or even coverage denials, as this is not currently covered under the Affordable Care Act clause on preexisting conditions. 118 Insurance companies will undoubtedly play an increasing role over the next decade in promoting the accessibility and affordability of consumer wearables. As such, conversations among key stakeholders are necessary to ensure appropriate oversight on how insurance companies may use consumers’ wearable-derived data.
Many clinicians and patients may be skeptical of using wearable-derived data in health care since few consumer wearables have been cleared as medical devices through the Food and Drug Administration’s 510(k) program. 119 The accuracy of data collected from consumer wearables is subject to several factors, such as device model, device nonuse, environmental factors, and motion artifact.67,120 Device accuracy is additionally limited by decreased ambulation speed and stride length, which are often seen in the postoperative setting.121,122 Prior research has suggested that reflective photoplethysmography may express variable degrees of accuracy when applied to individuals with darker skin tones.123,124 This remains disputed 67 but, if true, carries major implications for the equitable and meaningful use of these devices in diverse populations. Validation of consumer wearables for the detection of clinically relevant end points requires the design of prospective studies in target populations and settings in which device accuracy is likely to remain high. For example, measurement of physiologic parameters reflective of sympathetic stimulation (eg, heart rate, HRV, respiratory rate) should occur only at rest, as these values are highly variable with physical activity.67,125 Even if consumer wearables are validated for monitoring select populations, health care providers should not rely exclusively on wearable-derived data to guide decision making. Given the potential for misdiagnosis due to unreliable data or false alarms, the responsibilities of clinicians in responding to wearable-derived data need to be delineated. 4
Furthermore, some patients may find the devices to be uncomfortable or perceive the process of continuous remote monitoring as intrusive. 126 Patients may consider remote monitoring to be a burden if they are tasked with interpreting and making decisions that they feel should be done by their health care team. 9 Conversely, a care team may not be equipped to handle this potential deluge of data. Learning to interpret heterogeneously collected metrics and apply findings to clinical care, particularly in the absence of established best practices, may require considerable time, effort, and additional training. 7
Finally, remote monitoring with consumer wearables requires broadband connectivity, technology literacy, and, in many cases, a compatible smartphone device. This may explain a lower rate of consumer wearable use among elderly, socioeconomically disadvantaged, and less educated populations. 3 Underrepresentation of certain populations in training data and validation study cohorts would limit the generalizability of research findings. Clinicians and patients should employ shared decision making to thoroughly discuss the risks, benefits, and specific concerns surrounding consumer wearables for patient monitoring. 123 As each of these devices carries a cost ranging from $43 to $400, health systems or insurance companies should consider providing consumer wearables directly to patients at no cost. Doing otherwise risks promoting health disparities, as only patients with the means to provide their own wearables would receive the potential benefits. However, for these larger entities to justify offsetting the costs to patients, there must be sufficient evidence substantiating the benefits of incorporating these devices in clinical care. We recommend that future studies conduct cost-effectiveness analyses to estimate the long-term expenses and returns of uniformly providing consumer wearables to specific patient populations.
Implications for Practice
Consumer wearables may significantly transform health care delivery as tools to promote precision medicine. Limited literature from other surgical fields supports the ability of wearable-derived data to predict postoperative outcomes and promote the adoption of healthy behaviors. Nonetheless, research on the role of consumer wearables for monitoring otolaryngology patients is lacking. Interventions employing consumer wearables to assess and encourage physical activity and sleep in the perioperative period represent an actionable and high-impact area of research. Otolaryngologists’ understanding of the potential role and limitations of consumer wearables could allow for well-designed prospective studies that validate the utility of these devices in our field.
Supplemental Material
sj-docx-1-oto-10.1177_01945998211061681 – Supplemental material for Consumer Wearables for Patient Monitoring in Otolaryngology: A State of the Art Review
Supplemental material, sj-docx-1-oto-10.1177_01945998211061681 for Consumer Wearables for Patient Monitoring in Otolaryngology: A State of the Art Review by Shaan N. Somani, Katherine M. Yu, Alexander G. Chiu, Kevin J. Sykes and Jennifer A. Villwock in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-2-oto-10.1177_01945998211061681 – Supplemental material for Consumer Wearables for Patient Monitoring in Otolaryngology: A State of the Art Review
Supplemental material, sj-docx-2-oto-10.1177_01945998211061681 for Consumer Wearables for Patient Monitoring in Otolaryngology: A State of the Art Review by Shaan N. Somani, Katherine M. Yu, Alexander G. Chiu, Kevin J. Sykes and Jennifer A. Villwock in Otolaryngology–Head and Neck Surgery
Supplemental Material
sj-docx-3-oto-10.1177_01945998211061681 – Supplemental material for Consumer Wearables for Patient Monitoring in Otolaryngology: A State of the Art Review
Supplemental material, sj-docx-3-oto-10.1177_01945998211061681 for Consumer Wearables for Patient Monitoring in Otolaryngology: A State of the Art Review by Shaan N. Somani, Katherine M. Yu, Alexander G. Chiu, Kevin J. Sykes and Jennifer A. Villwock in Otolaryngology–Head and Neck Surgery
Footnotes
Acknowledgements
We thank Jacob White for his assistance in designing search queries and conducting the initial literature search.
Authorship Contributions
Disclosures
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.