
Abstract
Coronary pseudoaneurysms following implantation of drug-eluting stents, although rare, are not unknown. Nearly all such cases have been reported in patients with sirolimus or paclitaxel polymer-based stents. We describe a case of coronary pseudoaneurysm developing with a non-polymer-based drug-eluting stent in a 50-year-old man who was successfully managed by coronary artery bypass grafting.
Introduction
The development of coronary artery pseudoaneurysm following placement of a drug-eluting stent (DES) has been mostly found with sirolimus or paclitaxel polymer-based stents. We report an unusual case of coronary pseudoaneurysm developing after placement of a non-polymer-based DES.
Case Report
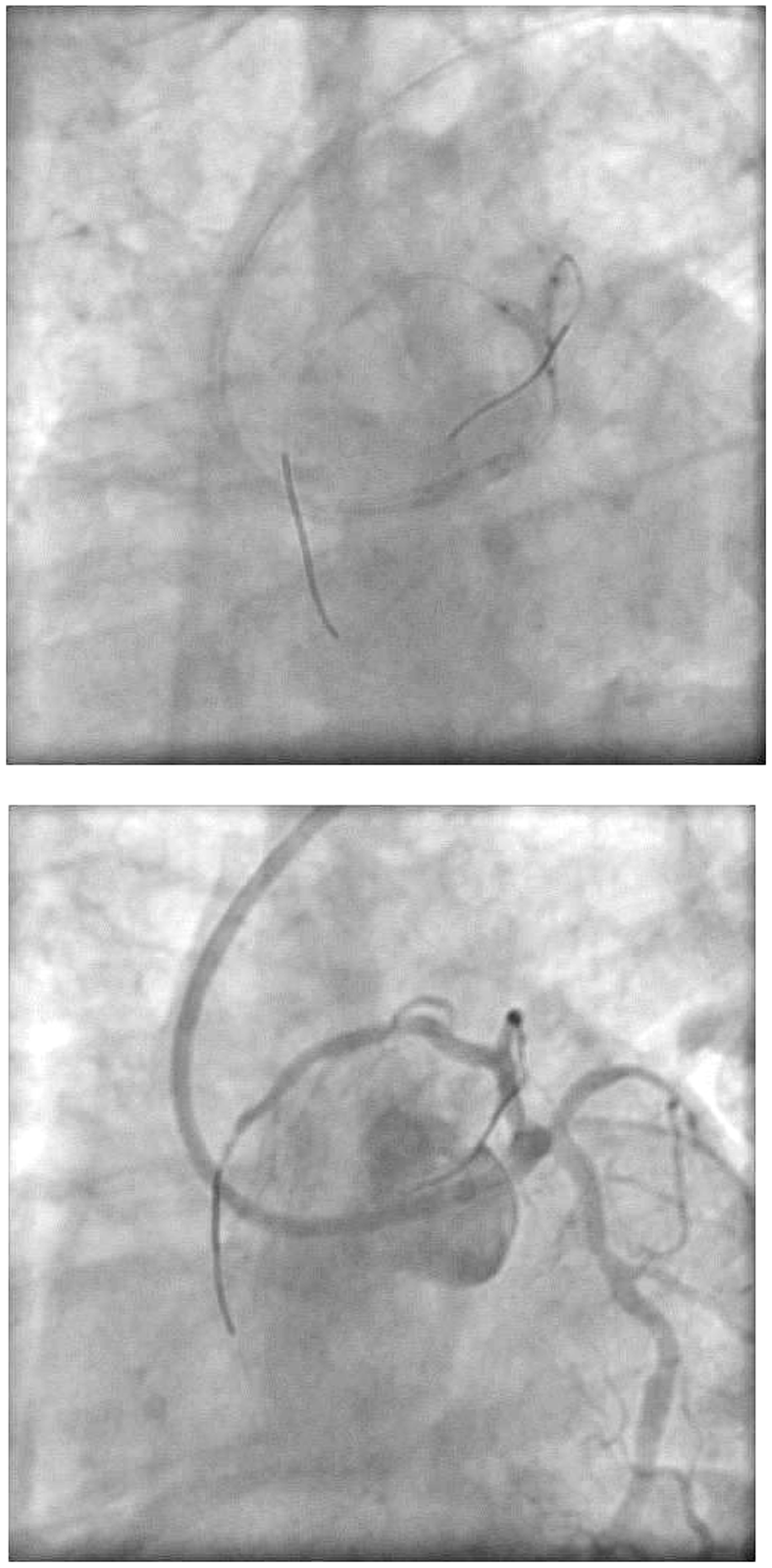
A 50-year-old man with hypertension, diabetes, and recent-onset angina underwent coronary angiography that revealed severe disease in the proximal left anterior descending coronary artery (LAD), severe ostial disease in the first diagonal branch (D1), and severe ostial disease in the major obtuse marginal vessel (Figure 1A). The right coronary artery was normal. During angioplasty of the LAD and D1, both vessels were wired with 0.014 Cougar wires (Medtronic, Inc.) and pre-dilated using 2 × 12-mm and 1.5 × 10-mm Sprinter balloons (Medtronic, Inc.), respectively. A Yukon 3 × 18-mm stent (2.0% sirolimus-eluting non-polymer-based on-site coated stent; Translumina, Germany) was implanted in the LAD (Figure 1B). The D1 lesion was rewired, and provisional stenting of D1 using a bare metal stent (Driver, 2.5 × 12 mm) was followed by final kissing balloon dilatation (3 × 12 mm at 8 atm in the LAD; 2.5 × 10 mm at 6 atm in D1) with good angiographic results (Figure 2). The major obtuse marginal was stented with another Yukon stent (2.5 × 12 mm). The patient was discharged 48 h later on routine medications including aspirin 300 mg and clopidogrel 75 mg daily.
(A). Native disease in the left anterior descending coronary artery (inverted white arrow) and first diagonal (arrowhead); there is severe disease in both vessels (left anterior oblique caudal view). (B) Stent in the left anterior descending (LAD) coronary artery (left) and the first diagonal (D1; right), left anterior oblique caudal view. Kissing balloon dilation of the left anterior descending coronary artery and first diagonal (top), and the final angiographic result (bottom).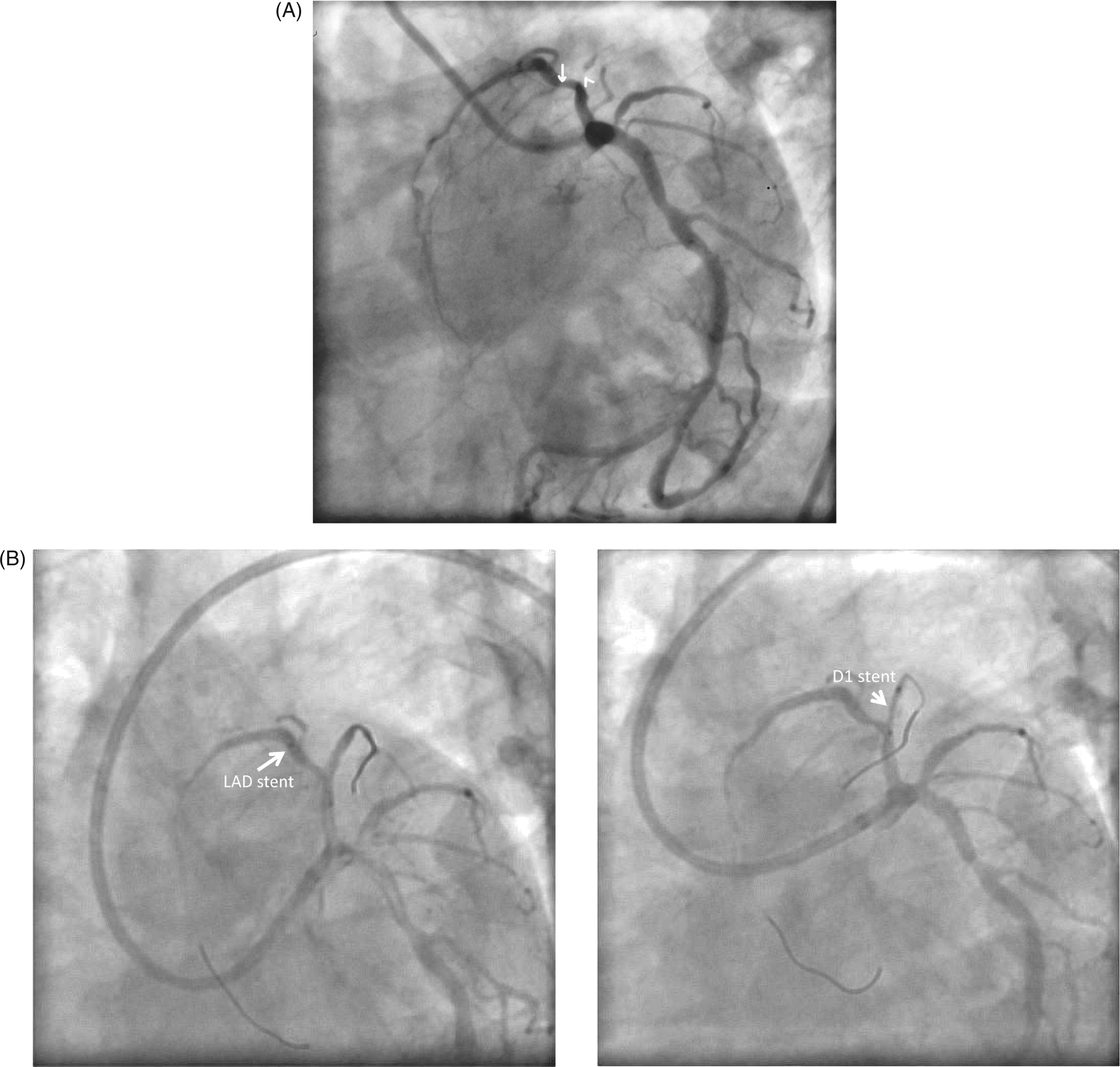
After remaining well for 8 weeks, the patient had a recurrence of angina. He denied any history of fever, and blood chemistry, cell counts, and cardiac biomarkers were normal. Repeat coronary angiography revealed severe in-segment restenosis in both the LAD and D1, with aneurysm formation in the proximal LAD (Figure 3). The stent in the major obtuse marginal was patent. Coronary artery bypass grafting was advised. Intraoperatively, a 2 × 2.5-cm pseudoaneurysm was found in the proximal LAD, which was closed at the distal end with encircling polypropylene sutures, and the proximal end was closed from inside the aorta using a pericardial patch. The left internal mammary artery was used to bypass the LAD, and a saphenous vein graft was used for D1. The patient remained well 15 months later.
Severe stent restenosis of both the left anterior descending coronary artery and first diagonal, with an aneurysm in the stented portion of the left anterior descending coronary artery.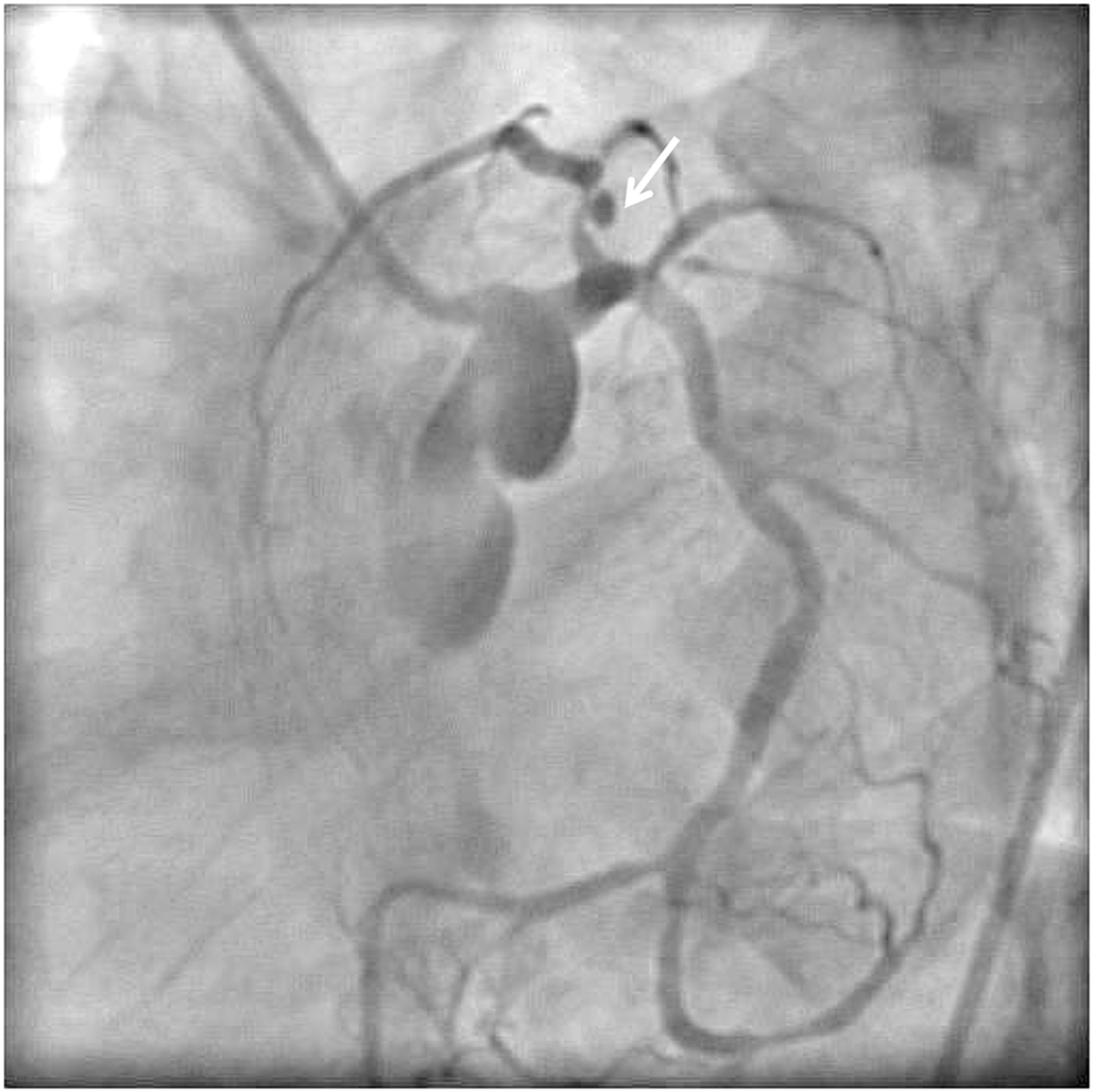
Discussion
Development of a coronary artery aneurysm after a percutaneous coronary intervention is rare, occurring in 0.3% to 6.0% of cases. Most such aneurysms are actually pseudoaneurysms. 1 – 3 Causative factors include residual nonhealing dissections, arterial barotrauma secondary to high-pressure balloon inflation, use of oversized balloons or stents, and use of debulking measures such as atherectomy and laser angioplasty. 3,4 Although known to reduce restenosis by inhibiting neointimal proliferation, DES are associated with the formation of coronary aneurysms more frequently than bare metal stents. Inflammation secondary to a hypersensitivity reaction to the metal, the polymer, or the drug, is the postulated mechanism, but multiple factors may be responsible. The polymer carrier is especially known to induce an inflammatory response leading to incomplete endothelialization, tissue damage, poor wound healing, and intra-intimal hemorrhage in animal studies. 5 Understandably, most cases of coronary aneurysm following DES placement have been with sirolimus or paclitaxel polymer-based stents.
Our patient had undergone stenting with a sirolimus-eluting non-polymer-based stent. To the best of our knowledge, development of a coronary pseudoaneurysm with a non-polymer-based DES has not been previously reported. This adds to the existing evidence that factors beyond the polymer may play a role in aneurysm development after DES placement. These include delayed re-endothelialization and healing secondary to the antiproliferative action of the eluted drug, cell necrosis or apoptosis due to an antimetabolite effect of the drug, or acquired late stent malapposition. 6 – 8 The fact that the Yukon stent implanted in the major obtuse marginal was patent supports the hypothesis that other factors might be at play. Since bifurcation stenting was performed in the LAD/D1 system and followed by a mandatory final kissing balloon dilatation, the resultant final high-pressure dilatation with consequent vessel microtrauma and/or micro-dissection (not apparent angiographically) may also have led to the pseudoaneurysm development. Management of such cases is challenging and needs to be individualized in the absence of any clear-cut guidelines. Options include placement of stent grafts, coronary coils, or coronary artery bypass grafting. We opted for coronary artery bypass in view of the LAD/D1 bifurcation disease and the possibility of jailing the large D1 by placement of a stent graft.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.