
Abstract
Objective
to evaluate the role of surgery (anterior thoracotomy versus video-assisted thoracoscopy) in avoidance of stroke by obliteration of the left atrial appendage in patients with chronic nonrheumatic atrial fibrillation.
Methods
in a prospective study, 58 patients (35 men and 23 women, aged 62±13.2 years) with chronic nonrheumatic atrial fibrillation were divided into 2 groups: group A was 29 patients who underwent an anterior thoracotomy, and group B was 29 patients who had video-assisted thoracoscopic obliteration of the left atrial appendage. All patients were followed up for at least 2 years.
Results
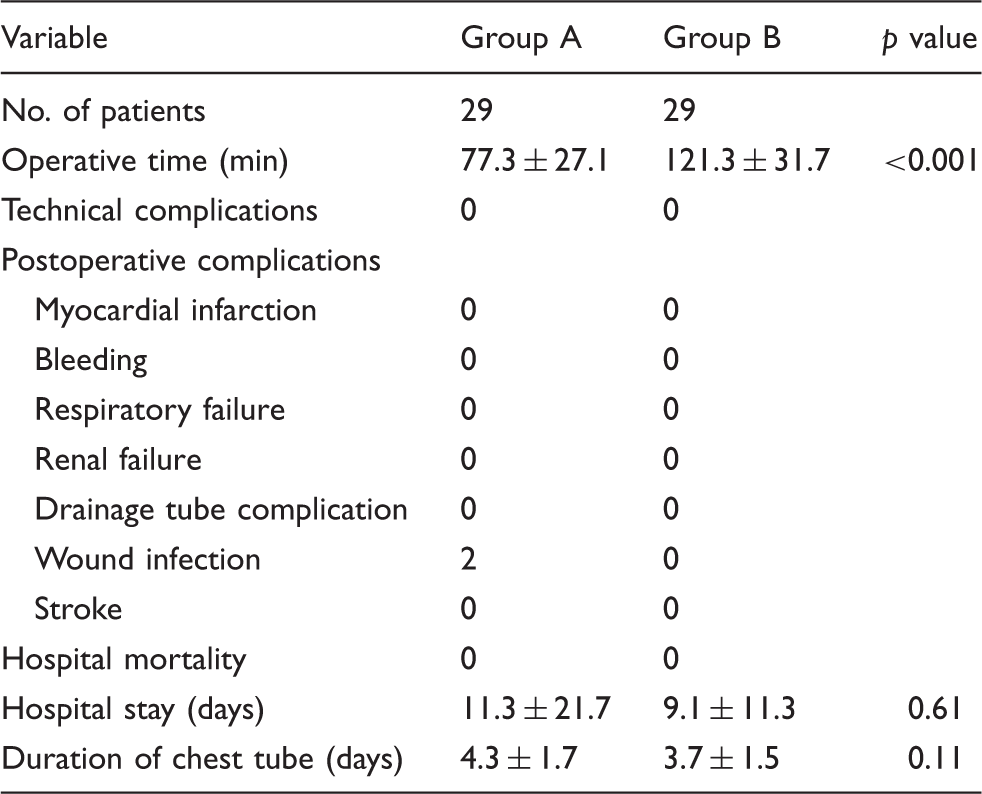
the 2 groups were well matched for age, sex, and comorbidities. No stroke was observed in either group. Operative time was significantly longer in group B. There was no intraoperative or postoperative complication, except for 2 cases of superficial wound infection in group A.
Conclusions
in chronic atrial fibrillation, prophylactic left atrial appendage exclusion is suggested to prevent occurrence of stroke, which can be achieved by a surgical or thoracoscopic approach, but a video-assisted thoracoscopic approach is effective, less invasive, and avoids the complications of a surgical approach.
Introduction
Stroke is the third leading cause of mortality and a leading cause of disability in the world today. 1 Brain ischemia is multifactorial; it may result from carotid artery occlusion, plaque embolization, or aortic atheromatous debris. A major cause is cardiac emboli, most commonly occurring in patients with atrial fibrillation (AF) which is the most common sustained cardiac arrhythmia. This association is assuming increased importance as AF markedly increases with the aging population. 2 Moreover, cardioembolic strokes are associated with the worst long-term prognosis. The left atrial appendage (LAA) has prompted considerable study as a cause of cardioembolic stroke. Goldsmith and colleagues 3 identified endocardial changes in the LAA muscular wall, and echocardiographic studies have long documented spontaneous echo contrast or “smoke” that indicates intracavitary blood stasis. Blackshear and Odel 4 reviewed 23 studies that included patients with rheumatic and nonrheumatic AF: in nonrheumatic AF, 91% of left atrial thrombi were isolated to or originated from the LAA. The multiple problems with anticoagulant therapy have led to a search for alternative approaches for stroke prevention in AF. These approaches are predicated on the fact that in nonvalvular AF, the embolus originates from the LAA in roughly 90% of cases. 4 This has led to a strategy of mechanically obliterating the LAA through an endovascular approach, a surgical approach, or a video-assisted thoracoscopic approach, and excluding it from the systemic circulation.
Patients and methods
Patient selection
From January 2008 through January 2010, 58 patients (35 men and 23 women, aged 62 ± 13.2 years) were included in this prospective study at King Fahd Hospital. After institutional ethics review committee approval, all patients with chronic AF were identified from routine clinical practice, with at least one risk factor for stroke according to CHA2DS2-VASc score (left ventricular systolic dysfunction, hypertension, age ≥ 75 years, diabetes mellitus, prior embolic episode, vascular disease, age 65–74, female sex) and either an absolute contraindication to oral anticoagulation or documentation of prior LAA thrombosis despite adequate oral anticoagulation. Transesophageal echocardiography (TEE) was performed within 24 h, showing no atrial clot and negative coronary screening. Informed consent was obtained before surgery. The patients were subdivided into 2 groups: group A was 29 patients who underwent an anterior thoracotomy for obliteration of the LAA, and group B was 29 patients who underwent video-assisted thoracoscopic obliteration of the LAA.
Operative techniques
All patients were hemodynamically stable when brought to the operating room. General anesthesia was used in all cases. Anesthetic time was calculated as time from induction until extubation. A single prophylactic dose of antibiotic was given at the start of surgery.
Anterior thoracotomy for obliteration of LAA
Each patient was anesthetized and intubated with a single-lumen endotracheal tube. TEE preoperatively confirmed the absence of LAA thrombus at the time of surgery (Figure 1(a)). Operative exposure was achieved by a small anterior thoracotomy in the 4th or 5th intercostal space. An inframammary skin incision (6–8 cm long) allowed division of the pectoralis muscle to expose the chosen intercostal space. The intercostal space was opened over the superior margin of the rib, entering the pleural cavity. A retractor was placed and the pericardium was visualized. Careful attention was paid to the phrenic nerve. The pericardium was incised anterior to the phrenic nerve with a scalpel or scissors. As a first step, the epicardial base of the LAA was carefully mobilized, avoiding tissue bunching, to increase the distance between the LAA and the circumflex artery. A Derra clamp was placed at the base of the LAA with attention to the circumflex artery. Two 90-cm 2/0 nonabsorbable Mersilene ligatures were knotted sequentially at the base of the LAA, approximately 5 mm apart. The clamp was moved stepwise during this procedure. The ligatures were controlled for bleeding or dehiscence. Obliteration was confirmed by intraoperative TEE (Figure 1(b)). A single thoracostomy tube (28 F or 32 F) was placed in the pleural cavity and connected to underwater seal drainage. The incision was closed in layers.
(a) Preoperative transesophageal echocardiography visualization of an open left atrial appendage without clot (arrow). and (b) Postoperative transesophageal echocardiography showing obliteration of the left atrial appendage (arrow).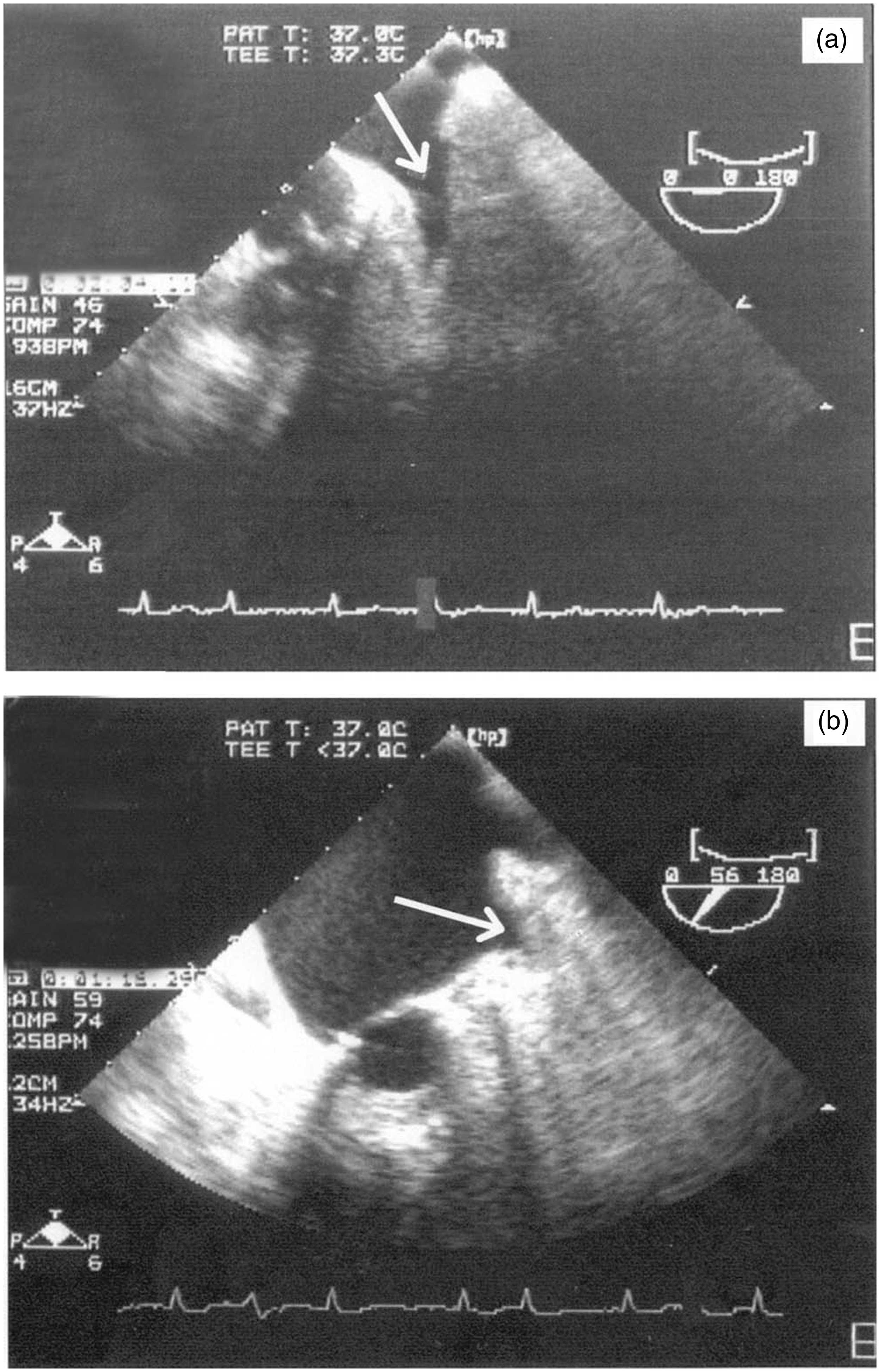
Video-assisted thoracoscopic obliteration of LAA
Each patient was anesthetized and intubated with a double-lumen endotracheal tube. TEE confirmed the absence of LAA thrombus at the time of surgery (Figure 1(a)). Patients were positioned, prepared, and draped as for a left lateral thoracotomy. Three to 5 thoracoscopic incisions were made to introduce the video-assisted thoracoscopic instruments. Using the double-lumen endotracheal tube, the volume of the left lung was reduced. The pericardium was opened with scissors anterior to the phrenic nerve. The LAA tip was grasped with a nontraumatic clamp, and an Endoloop snare was fixed as a tie to the appendiceal tip. A second Endoloop was introduced over the first tie and manipulated with the assistance of instruments to the appendiceal base where it was cinched to occlude the appendage. Occlusion was documented by TEE as the abrupt appearance of dense stationary high-contrast echoes (Figure 1(b)). At the conclusion of the procedure, the pericardium was left open. A single thoracostomy tube (28 F or 32 F) was placed in the pleural cavity and connected to underwater seal drainage.
All patient were extubated and transferred to the recovery room for a few hours of observation, and returned to the ward on the same day. The chest tube was removed when the amount of daily drainage was less than 100 mL. Postoperative analgesia was provided in all cases, and the patients were discharged from the hospital on aspirin only.
Data analysis
All data including preoperative demographic details were recorded, and the outcomes of both groups were compared. The primary outcome variable was the incidence of postoperative cerebrovascular events, defined as focal neurological dysfunction of vascular etiology including transient ischemic attack, defined as a fully reversible neurological ischemic event lasting < 24 h, and stroke, defined as a neurological ischemic event with persistent signs of neurological dysfunction. Secondary outcome variables included intraoperative and postoperative complications, operative time (the interval between first port incision or surgical skin incision and completion of wound closure), intraoperative technical complications, intraoperative or postoperative bleeding, postoperative myocardial infarction (according to electrocardiographic criteria and serum troponin I level), respiratory failure requiring mechanical support (prolonged intubation >48 h, reintubation, or noninvasive positive-pressure ventilation), renal failure requiring dialysis, drainage tube-related complications (pneumothorax) and duration of chest tube drainage postoperatively, wound infections, length of hospital stay which was calculated from the day of the surgical procedure until discharge or hospital death, and perioperative mortality rate which was defined as the percentage of patients who died of all causes within 30 days of surgery. Follow-up for at least 2 years was obtained for all patients after discharge from the hospital, by telephone interview at 6-month intervals, and questions regarding neurologic symptoms.
Statistical analysis
The data of both groups were calculated (mean ± standard deviation) and compared using paired t tests. Differences were considered significant at p < 0.05. All analyses were performed with the Statistical Package of Social Sciences (SPSS) version 13.0 software for Windows (SPSS, Inc., Chicago, IL, USA).
Results
Intraoperative and postoperative results in patients who had open surgical (group A) or video-assisted left atrial appendage obliteration (group B).
Discussion
In patients with nonrheumatic AF, the LAA is the origin of at least 90% of all left atrial thrombi, and the resulting systemic emboli cause approximately 25% of all strokes.4–6 The stroke rate in patients with AF older than 75 years of age approximates 8% per year with one clinical risk factor, and has been estimated as 12% per year at any age in clinical trial populations with history of prior thromboembolic disease.7,8 Three-year stroke rates in elderly nursing home patients not anticoagulated are in excess of 50%. 9 Anticoagulation reduces embolic stroke in AF, but is often withheld due to contraindications, inconvenience, inability to monitor anticoagulation levels, or the perception of excessive risk of bleeding. Even when anticoagulation is prescribed, therapeutic levels are frequently not well-maintained.10,11
The surgical approaches for treatment of AF include the Cox maze procedure and catheter-based ablation with pulmonary vein isolation. The Cox maze procedure has been limited because of its length, technical difficulty, and prolonged cardiopulmonary bypass times. Recently, catheter-based ablation and pulmonary vein isolation have gained popularity because it is a technically simple and less invasive procedure that can be performed on a beating heart without cardiopulmonary bypass, but it has variable rates of success among centers, often requires repeat procedures, and is associated with serious, although infrequent, complications. In addition, it does not deal with the LAA, the source of embolic thrombi in at least 90% of patients with AF. Concomitant AF treatment with surgical ablation was not carried out in either method of approach in our patients because the ablation device was not available in our department.
In 1955, Belcher and Somerville 12 discussed the potential to decrease systemic embolization by LAA ligation, and since that time, the procedure has been performed both concurrently with open cardiac surgical procedures, and as an independent procedure via open surgery, thoracoscopy, and more recently via endoluminal techniques which have many disadvantages such as placement of an intracardiac foreign body and utilization of immediate post-procedure antithrombotic therapy. 13 Many studies recorded a persistent risk of cardioembolic phenomenon associated with incomplete exclusion or an appendage remnant >1 cm.14–16 In our center, we have not yet seen this phenomenon, using either the open surgical or video-assisted thoracoscopic technique. Some other experienced centers advocate using a stapler along with buttressing material to further reduce this risk. 17 Video-assisted thoracoscopic obliteration of the LAA has many technical and therapeutic advantages; it is less traumatic and cosmetically better than an anterior thoracotomy.
This series showed no occurrence of stroke during 2 years of follow-up. Similar results were recorded in a study by Nagpal and colleagues. 13 Operative time was substantially longer in the thoracoscopy group, a finding that was anticipated given the added time necessary for placement of a double-lumen endotracheal tube and the thoracoscopic procedures. There was no intraoperative technical complication or postoperative tube-related complication in either group. Also, there was no perioperative mortality in these patients. Similar results have been recorded in many series of LAA ligation or exclusion.4,18–20 Two patients who had an anterior thoracotomy had a superficial wound infection.
It was concluded that the LAA is a lethal source of emboli in AF patients. In chronic AF, prophylactic LAA exclusion is suggested as a method to prevent the occurrence of stroke. The LAA obliteration can be achieved through either a surgical or thoracoscopic approach, but the video-assisted thoracoscopy approach is effective, less invasive, and avoids the complications of the surgical approach.
Presented at: The 61st International Congress of The European Society for Cardiovascular and Endovascular Surgery, Dubrovnik, Croatia, April 25–28, 2012; The 8th Congress of Update in Cardiology and Cardiovascular Surgery, Antalya, Turkey, March 1–4, 2012; The 58th annual meeting of The Indian Association of Cardiovascular and Thoracic Surgeons and 1st joint workshop with The European Association for Cardiothoracic Surgery, Kolkata, India, February 8–12, 2012; and The Annual Scientific Meeting of International Society for Minimally Invasive Cardiothoracic Surgery, Los Angeles, USA, May 30–June 2, 2012.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.