
Abstract
Aim
to evaluate the strategy for open heart surgery after renal transplantation performed in a single institution in Japan.
Methods
we reviewed 6 open heart surgeries after renal transplantation in 5 patients, performed between January 1992 and December 2012. The patients were 3 men and 2 women with a mean age of 60 ± 11 years (range 46–68 years). They had old myocardial infarction and unstable angina, aortic and mitral stenosis, left arterial myxoma, aortic stenosis, and native valve endocarditis followed by prosthetic valve endocarditis. Operative procedures included coronary artery bypass grafting, double-valve replacement, resection of left arterial myxoma, 2 aortic valve replacements, and a double-valve replacement. Renal protection consisted of steroid cover (hydrocortisone 100–500 mg or methylprednisolone 1000 mg) and intravenous immunosuppressant infusion (cyclosporine 30–40 mg day−1 or tacrolimus 1.0 mg day−1).
Results
5 cases were uneventful and good renal graft function was maintained at discharge (serum creatinine 2.1 ± 0.5 mg dL−1). There was one operative death after emergency double-valve replacement for methicillin-resistant Staphylococcus aureus-associated prosthetic valve endocarditis. Although the endocarditis improved after valve replacement, the patient died of postoperative pneumonia on postoperative day 45.
Conclusions
careful perioperative management can allow successful open heart surgery after renal transplantation. However, severe complications, especially methicillin-resistant Staphylococcus aureus infection, may cause renal graft loss.
Keywords
Introduction
In 1975, Lamberti and colleagues 1 reported the first case of coronary artery bypass grafting (CABG) after renal transplantation. In the same year, Nakhjvan and colleagues 2 also reported CABG after renal transplantation. Since these early reports, there have been several studies on open heart surgery after renal transplantation in Western countries.3,4 In Japan, we reported the first case of CABG after renal transplantation in 1993. 5 In the same year, Ando and colleagues 6 described 2 cases of CABG after renal transplantation. As yet, there has been no analysis of open heart surgery after renal transplantation in Japan. Therefore, the purpose of this study was to evaluate our strategy for open heart surgery after renal transplantations at a single institution in Japan.
Patients and methods
Characteristics of 5 patients undergoing cardiac surgery after renal transplantation.
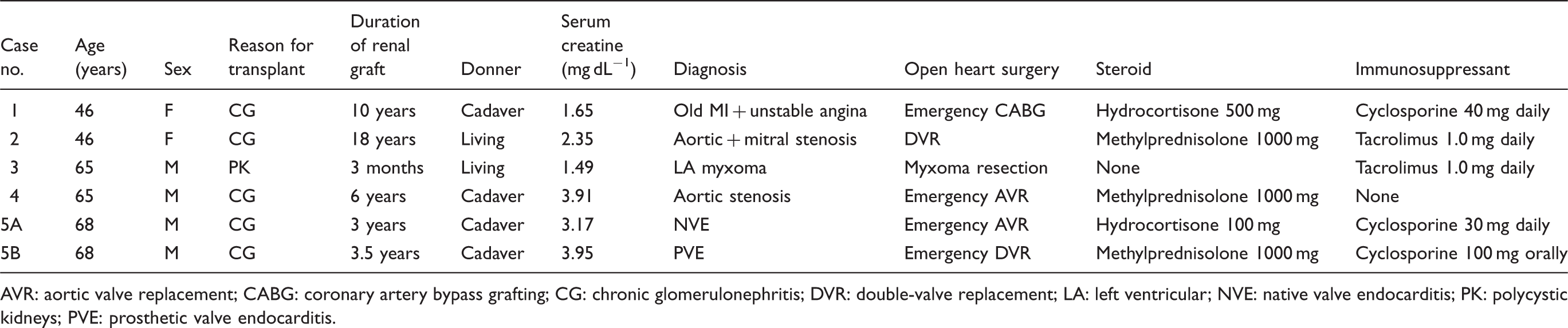
AVR: aortic valve replacement; CABG: coronary artery bypass grafting; CG: chronic glomerulonephritis; DVR: double-valve replacement; LA: left ventricular; NVE: native valve endocarditis; PK: polycystic kidneys; PVE: prosthetic valve endocarditis.
Steroid cover during the operations consisted of hydrocortisone 100–500 mg or methylprednisolone 1000 mg, if necessary. Continuous intravenous immunosuppressant infusion was also performed with cyclosporine or tacrolimus. Regarding the intravenous dose of cyclosporine during open heart surgery, we previously reported that 30–40 mg per day (1/3rd of the preoperative oral dose) is enough for open heart surgery after renal transplantation, based on the intraoperative concentrations. 5 Regarding the intravenous dose of tacrolimus during open heart surgery, we administrated 1.0 mg per day (1/5–1/2 of the oral dosage) based on a previous report. 7
Results
Five operative procedures were uneventful and the patients were discharged after 37 ± 15 days (range 9–49 days). The changes in serum creatinine levels after open heart surgery are shown in Figure 1. Renal function at discharge was satisfactory without increased serum creatinine levels (2.4 ± 1.1 to 2.1 ± 0.5 mg dL−1). There was one operative death (17%) after emergency DVR for MRSA-associated PVE (case 5B in Table 1). This patient initially underwent emergency aortic valve replacement for native valve endocarditis caused by Klebsiella pneumoniae infection, and was discharged (case 5A in Table 1), but 6 months later, he developed MRSA-associated PVE and was treated with vancomycin. Since his MRSA infection had spread to the mitral valve, he underwent emergency DVR by the Manouguian's method. Because of the administration of vancomycin, his preoperative renal function deteriorated (serum creatinine 3.95 mg dL−1) so that intraoperative and postoperative hemodialysis was required. Although DVR ultimately treated his PVE, he died of pneumonia on postoperative day 45.
Changes in renal function (serum creatinine) after open heart surgery.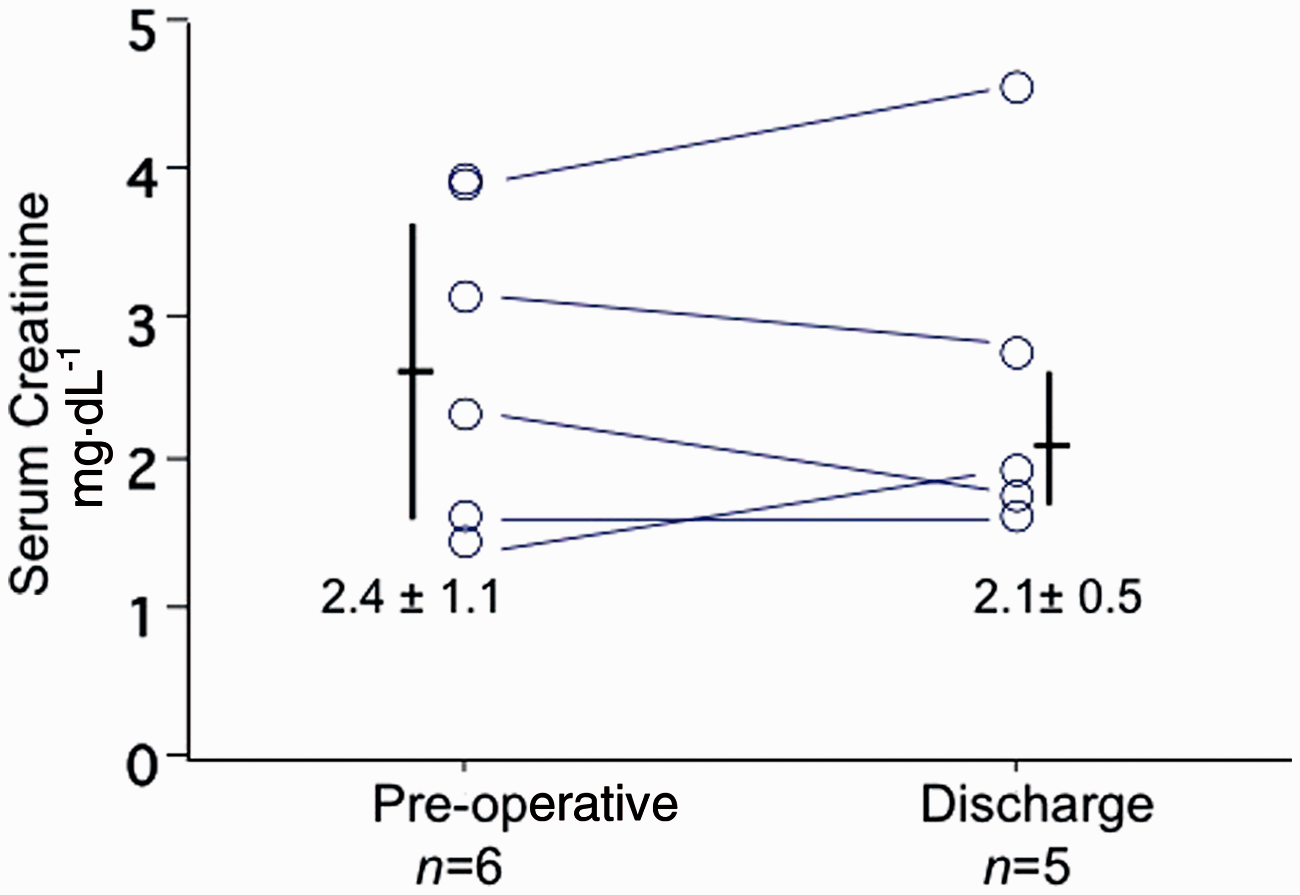
Discussion
Open heart surgery after renal transplantation in Japan.

Case described in this report. †Renal graft loss due to methicillin-resistant Staphylococcus aureus. AR: aortic regurgitation; AVR: aortic valve replacement; CABG: coronary artery bypass grafting; CG: chronic glomerulonephritis; DAA: dissecting aortic aneurysm; DVR: double-valve replacement; IgA: immunoglobulin A; IV: intravenous; LA: left atrial; NVE: native valve endocarditis; PCI: percutaneous coronary intervention; PH: pulmonary hypertension; PK: polycystic kidneys; PO: per os; POD: postoperative day; PVE: prosthetic valve endocarditis; MI: myocardial infarction; MR: mitral regurgitation; MS: mitral stenosis; MRSA: methicillin-resistant Staphylococcus aureus; RT: renal transplantation; SLE: systemic lupus erythematosus; TAA: thoracic aortic aneurysm; TEVAR: thoracic endovascular aortic repair.
The number of open heart surgery after renal transplantation in Japan is small (only 6 in our institute and 26 in total in Japan). In contrast, Zhang and colleagues 4 recently reported the operative results of open heart surgery after renal transplantation in 57 patients in Washington Hospital Center, USA. The population of renal transplantation patients in Japan is much smaller than that of Western countries. In 2010, 16,899 renal transplantations were performed using cadaver donors in 10,622 (63%) patients and living donors in 6277 (37%) in the USA (2010 database of United Network for Organ Sharing, http://www.unos.org). In the same period in Japan, only 1476 renal transplantations were performed using cadaver donors in 186 (13%) patients and living donors in 1276 (86%; 2010 database of Japan Organ Transplant Network, http://www.jotnw.or.jp). Therefore, the renal transplantation population in Japan is 1/10th of that in the USA, and the renal transplantation population receiving cadaver donors in Japan is only 1/50th of that in the USA.
Prevention of postoperative infection is very important after open heart surgery in renal transplantation patients. Zhang and colleagues 4 reported that 8 (14%) renal grafts were lost and 10 (18%) postoperative infections occurred. Establishing the minimum effective dose of immunosuppressant infusion is the key to the success of open heart surgery after renal transplantation. In 1970, cyclosporine was extracted from a Norwegian fungus (Tolypocladium inflatum Gams), and is now the most widely used immunosuppressant. Cyclosporine is more frequently administered intravenously than orally (6:3 in Table 2), presumably because of its poor oral absorbability. Regarding the intravenous dose of cyclosporine during open heart surgery, Eide and colleagues 22 used half of the preoperative oral dose, whereas we used 1/3rd of the preoperative oral dose, based on our previous report, 5 and the results were satisfactory. In 1984, tacrolimus was isolated from the Japanese fungus Streptomyces tsukubaensis, and it is now also widely used as an immunosuppressant. Tacrolimus was first used for open heart surgery in 1998. 7 Tacrolimus was administrated intravenously and orally in an equal number of patients (Table 2). We used an intravenous dose of tacrolimus based on a previous report. 7 Japanese cardiovascular surgeons were not familiar with the use of these intravenous immunosuppressant infusions before heart transplantation started in Japan in 1999. 23 This might be another reason why the number of open heart operations after renal transplantation in Japan is so small.
In conclusion, we think that careful perioperative management can allow successful open heart surgery after renal transplantation. However, severe complications, especially MRSA infection, may cause renal graft loss.
Footnotes
Acknowledgements
We thank Yuki Imamura, RN and Ryoko Yagi (Fujiwara), RN (Transplant Coordinator, Japan Organ Transplant Network) for their assistance.
Presented at the 20th Annual Meeting of Asian Society for Cardiovascular & Thoracic Surgery, Indonesia, March 2012.
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared