
Abstract
The branching pattern of pulmonary veins exhibits many variations. Here we describe 2 patients with lung malignancies who were found to have pulmonary vein anomalies. We performed video-assisted thoracoscopic lobectomies based on preoperative simulations by 3-dimensional computed tomography. Using 3-dimensional computed tomography, a surgeon can easily construct digital images of the patient’s pulmonary vessels within a few minutes. Simulation using 3-dimensional computed tomography imaging is useful for further understanding of the surgical anatomy.
Keywords
Introduction
Video-assisted thoracic surgery (VATS) for anatomical lung resection requires precise knowledge of the pulmonary vessels and bronchi because of the narrow operative field and reduced tactile sensations. Preoperative simulations of the surgical anatomy are of considerable value because anatomic anomalies of pulmonary vessels can cause serious intraoperative problems such as bleeding.1,2 Preoperatively, we have used a high-quality three-dimensional computed tomography (3D-CT) image analysis system (Synapse Vincent, Fuji Film Co., Ltd., Tokyo, Japan) for constructing virtual-reality 3D pulmonary anatomy since 2011. 3 Here we report 2 cases of anomalous pulmonary vein anatomy in which we performed VATS lobectomy based on preoperative simulations by 3D-CT.
Case 1
An 83-year-old woman had an abnormal shadow in the right lung on a routine medical check-up. An enhanced CT scan demonstrated a 1.9-cm nodule in the right lower lobe and the superior segment of the right lower lobe vein (V6) ostium, separate from the inferior pulmonary vein and each other (Figure 1A). The 3D-CT image clearly showed that the V6 directly drained into the left atrium just below the superior pulmonary vein (Figure 1B). Initially, we performed thoracoscopic partial resection and intraoperative rapid diagnosis indicated adenocarcinoma. Subsequently, we performed a VATS right lower lobectomy with lymph node dissection through 4 access ports. The V6 independently drained into the left atrium (Figure 1C). Figure 1D shows a schema of this anomalous V6. This independent V6 and the inferior pulmonary vein were therefore carefully ligated with a surgical stapler. The postoperative course was uneventful and the pathological diagnosis was stage IA lung adenocarcinoma.
Case 1. (A) Enhanced computed tomography image showing the superior segment of the right lower lobe vein (V6) ostium separate from the inferior pulmonary vein (IPV; white arrow). (B) Virtual 3-dimensional computed tomography image showing that the V6 directly draining into the left atrium. (C) Intraoperative image demonstrating that the V6 drained independently into the left atrium. (D) Schema of this anomalous V6.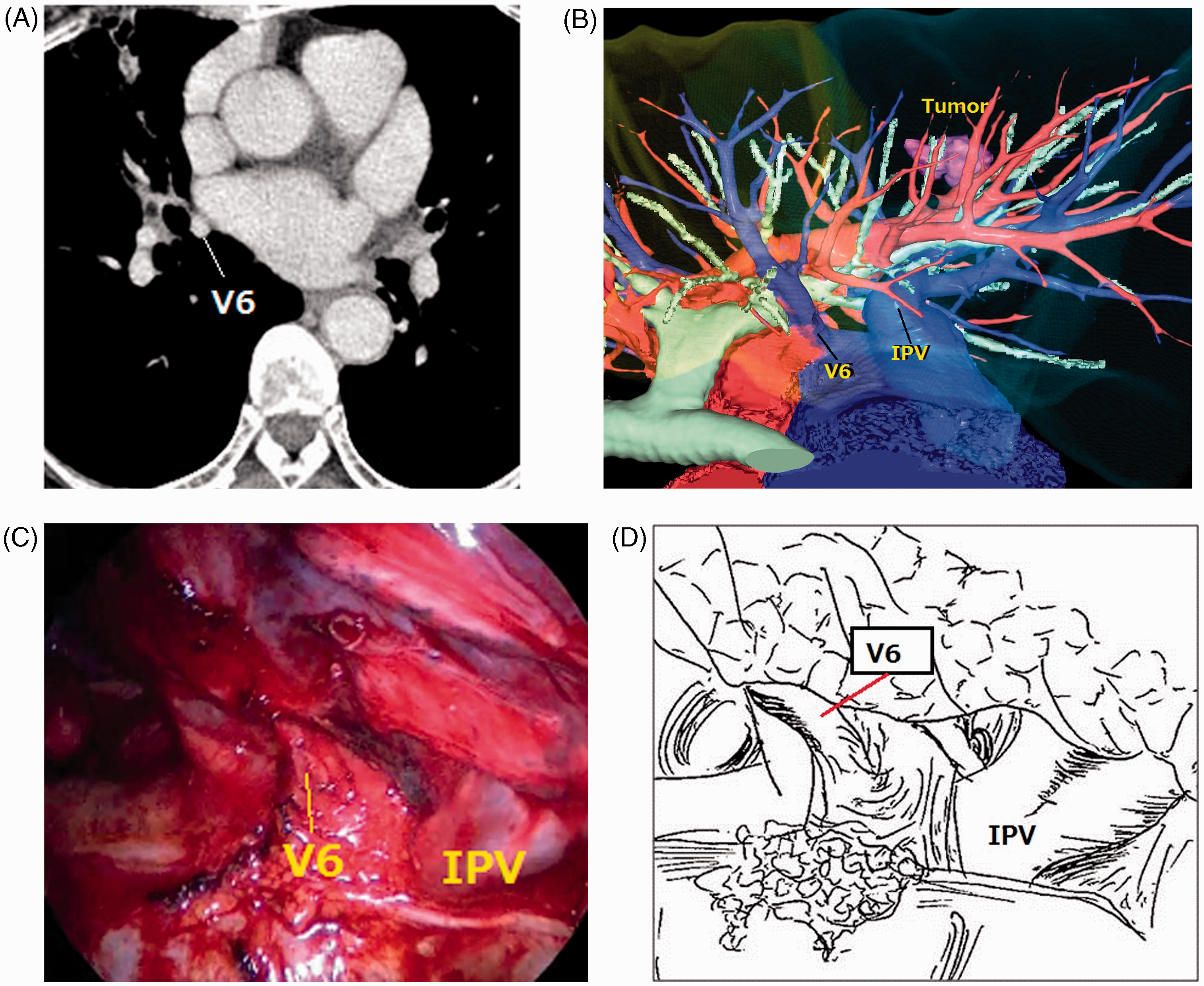
Case 2
A 70-year-old woman was referred to our institution with an abnormality in the right lung field on a chest radiograph. An enhanced CT scan showed a lesion measuring 1.5 cm × 1.4 cm in the right S2 area and a right upper lobe vein posterior to the bronchus intermedius (Figure 2A). A review of the patient’s 3D-CT image clearly showed that the right upper lobe vein was directly connected to the inferior pulmonary vein (Figure 2B). VATS right upper lobectomy with lymph node dissection was performed through 4 access ports. We separated the abnormal right upper lobe vein from the bronchus intermedius and surrounding lung tissue (Figure 2C). Figure 2D shows a schema of the anomalous right upper lobe vein. After the abnormal vein was divided between double ligatures, the posterior aspect of the major fissure was carefully divided. The patient’s postoperative course was uneventful, and the histological diagnosis was a metastatic lung tumor from breast cancer treated 10 years previously.
Case 2. (A) Enhanced computed tomography image showing a right upper lobe vein (RULV) posterior to the bronchus intermedius (white arrow). (B) Three-dimensional computed tomography image showing the right upper lobe vein directly connected to the inferior pulmonary vein (IVP) positioned posterior to the bronchus intermedius. (C) Intraoperative findings showing the anomalous right upper lobe vein corresponding to the 3-dimensional computed tomography image. (D) Schema of the anomalous right upper lobe vein.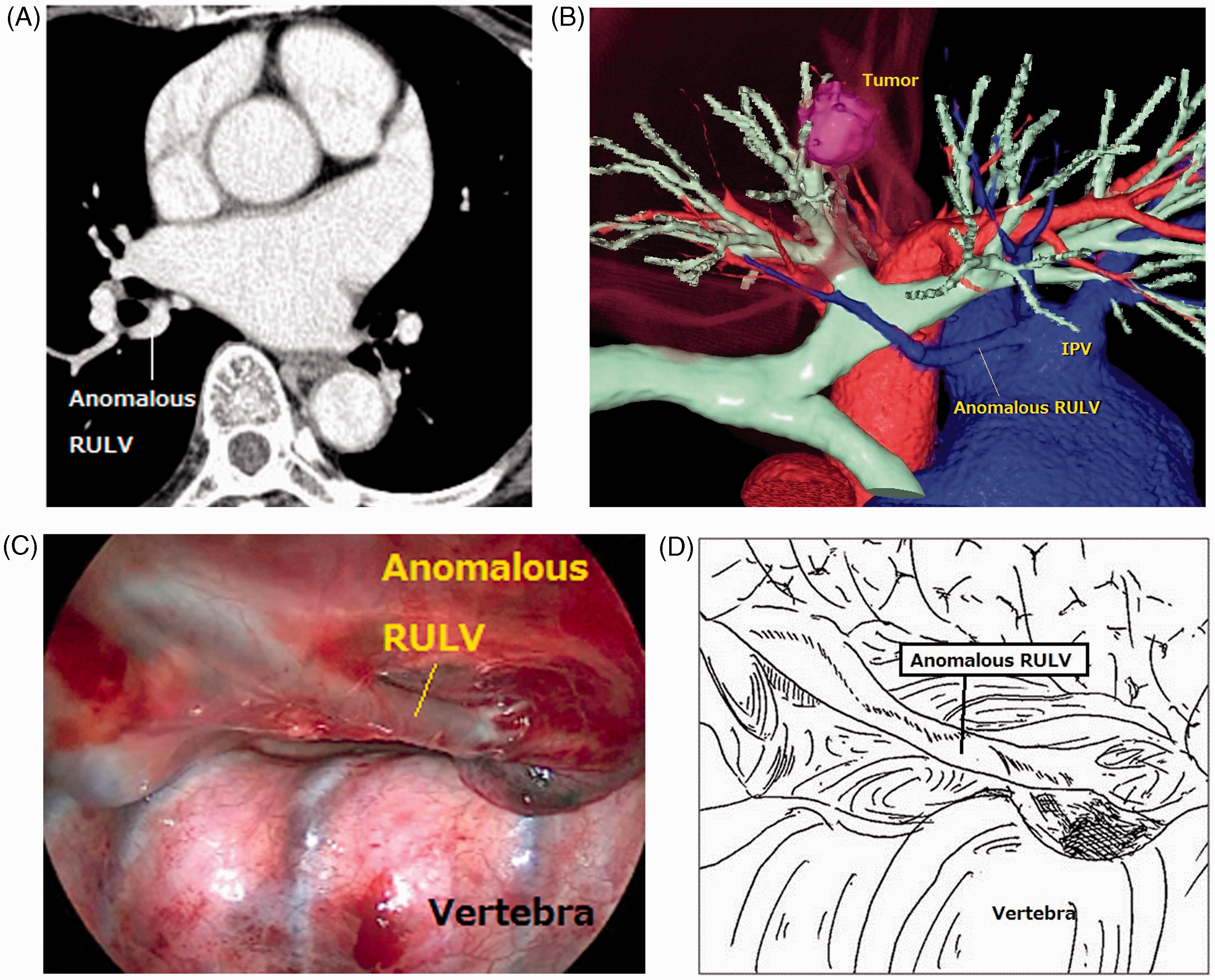
Discussion
Preoperative identification of anomalous pulmonary vessels is thought to be important for avoiding injury to vessels and for further understanding of pulmonary anatomy.1–5 Therefore, preoperative simulation of the surgical anatomy using imaging modalities is desirable. There are various advantages of this 3D-CT software that is based on volume-rendering techniques. First, a surgeon without expert knowledge concerning synthetic imaging can quickly construct each patient’s 3D images. After the digital images from enhanced CT are transferred to the 3D system by compact disk read-only memory, the system displays 3D images automatically within a few minutes. The software also allows us to freely rotate the objects and to change their dimensions. Intraoperative visualization guidance of the target vessels and bronchi and their relationship to one another should help surgeons perform lung resections with fewer complications, and be prepared for complicated operations such as multi-segmentectomies. Furthermore, unlike the currently available 3D-CT software programs, this system can obtain 3D images of the pulmonary artery and the veins separately, compared to only one image obtained from a conventional CT scan. Therefore, it can reduce the radiation exposure dose.
As demonstrated by the 2 cases presented here, this 3D-CT imaging technique is useful for identifying anomalous pulmonary vein connections. In case 2, it might have been difficult to identify the anomalous vein using conventional CT. Asai and colleagues 6 reported that the frequency of the right upper lobe vein being positioned posterior to the bronchus intermedius, as in case 2, is 5.7%. Cronin and colleagues 7 reported that 2.5% of patients had an accessory pulmonary vein at the superior segment of the right lower lobe, similar to case 1. We consider preoperative simulations using 3D-CT to be useful for the safe performance of VATS lobectomy and for further understanding of the surgical anatomy. Further advances in 3D-CT imaging technology should lead to significant developments not only in VATS and thoracotomy, but also in robotic surgeries and surgical education systems.
Footnotes
Acknowledgement
The authors are indebted to the medical editors of the Department of International Medical Communications of Tokyo Medical University for their editorial review of the English manuscript.