
Abstract
Background
Palpation is the most important means of locating lung tumors and resecting them with sufficient margins. This study aimed to predict the palpability of pulmonary lesions using high-resolution computed tomography.
Methods
Eighty-six pulmonary lesions were palpated in fresh resected lung specimens from July 2013 to March 2014. The following parameters were compared between 10 impalpable and 76 palpable lesions: maximum tumor size in pulmonary and bone window level settings, consolidation tumor size in pulmonary window level setting, and pleural-tumor distance. In 54 adenocarcinomas, the lepidic component and fibrosis foci rates were compared between the two groups.
Results
Tumor size in bone window level setting and the consolidation tumor size were significantly smaller in the impalpable group (both p < 0.001), and an operational cutoff of 5 mm was identified by receiver-operating characteristic analysis (sensitivity/specificity was 90.0%/94.7% and 90.0%/86.9%, respectively). Pulmonary lesions were impalpable with 87.5% probability when the tumor size in bone window level setting was ≤5 mm and the pleural-tumor distance was ≥ 5 mm, and with 85.7% probability when the consolidation tumor size was ≤5 mm and the pleural-tumor distance was ≥ 5 mm. Lepidic component and fibrosis foci rates of impalpable/palpable lesions were 96.0%/52.8% and 4.0%/24.7%, respectively (both p < 0.001).
Conclusions
Tumor size in bone window level setting or a consolidation tumor size ≤5 mm and pleural-tumor distance ≥ 5 mm are simple criteria that are potentially useful indicators for preoperative marking to locate small-sized lepidic-predominant adenocarcinomas with few fibrotic foci.
Keywords
Introduction
Surgical treatment of small pulmonary lesions with ground-glass opacity (GGO) has increased due to recent remarkable developments in high-resolution computed tomography (HRCT). Segmentectomy and wedge resection offer a favorable prognosis following resection of small pulmonary tumors.1,2 However, these lesions are difficult to locate by palpation intraoperatively; thus the thoracic surgeon may be unsure whether the mass has been resected with sufficient margins. 3 Accordingly, numerous preoperative labeling techniques have been investigated.4–8 However, these techniques carry several risks, and appropriate criteria have not been established. Intraoperative palpability relies on the tumor size and pleural-tumor distance (PTD), and several studies have examined the accuracy of palpability during video-assisted thoracoscopic surgery (VATS), based on these parameters.9–12 VATS was converted to a thoracotomy for impalpable tumors, but none of the studies indicated whether the pulmonary lesion was palpable during thoracotomy or in the fresh resected specimen. Thus the factors affecting the prediction of palpability are still unclear. Palpation of fresh resected lung specimens is of a higher quality than palpation during VATS or thoracotomy; therefore, a pulmonary lesion that is impalpable in a resected fresh specimen is an indication for preoperative marking. This study aimed to predict the palpability of pulmonary lesions by comparing impalpable and palpable lesions using HRCT. Moreover, the histopathological characteristics associated with the palpability of the lesions were analyzed.
Patients and methods
This study was approved by the institutional review board of Kanagawa Cancer Center (IRB# 33, 04/09/2014), and followed the tenets of the Declaration of Helsinki. All patients provided written informed consent. Of 256 pulmonary lesions that were resected from July 2013 to March 2014 in our institution, 86 measuring ≤50 mm in diameter, which were palpated in fresh resected lung specimens, were evaluated. None of the cases were marked preoperatively. The tumor size at each window level on HRCT and the PTD were compared between 10 impalpable lesions and 76 palpable lesions.
The patients underwent lobectomy or segmentectomy by a posterolateral thoracotomy through an approximately 15-cm skin incision. A wedge resection was performed using complete VATS with 3 ports inserted through one 3–5-cm and two 1–1.5-cm incisions. The pulmonary lesion in the fresh lung specimen was palpated with both hands by at least one pathologist and one thoracic surgeon wearing plastic gloves within 30–60 min of resection. Pulmonary lesions were considered palpable when the tumor was detected by more than two examiners and was consistent with preoperative HRCT findings (tumor location and size). Lesions not meeting these criteria were considered impalpable.
Chest computed tomography (CT) was performed using an X-Vigor/Real CT scanner or an Aquillion CT scanner (Toshiba Medical Systems, Tochigi, Japan). Tumor size was determined by HRCT at a 1- to 2-mm section thickness by measuring the maximum axial tumor size in a pulmonary window level setting (TSPW; level 600 HU; width 1600 HU). The consolidation tumor size in a pulmonary window level setting (TScon), and the tumor size in a mediastinal window level setting (TSMW; level 40 HU; width 400 HU) and in a bone window level setting (TSBW; level 600 HU; width 2000 HU) were also measured. Consolidation was defined as an area of increased opacification that completely obscured the underlying vascular structure. PTD was the distance between the pulmonary lesion and the nearest visceral pleural surface. Measurements of each parameter are shown in Figure 1.
(A, B, C) Case 1 was a palpable invasive adenocarcinoma and (D, E, F) case 2 was an impalpable adenocarcinoma in situ. The pleural-tumor distances (PTD) measured in pulmonary window level setting, tumor consolidation diameters in pulmonary window level setting (TScon), and tumor sizes in pulmonary window level setting (TSPW) are shown in A and D, respectively. Tumor sizes in bone window level setting (TSBW) are shown in B and E, and tumor sizes measured in mediastinal window level setting (TSMW) are shown in C and F.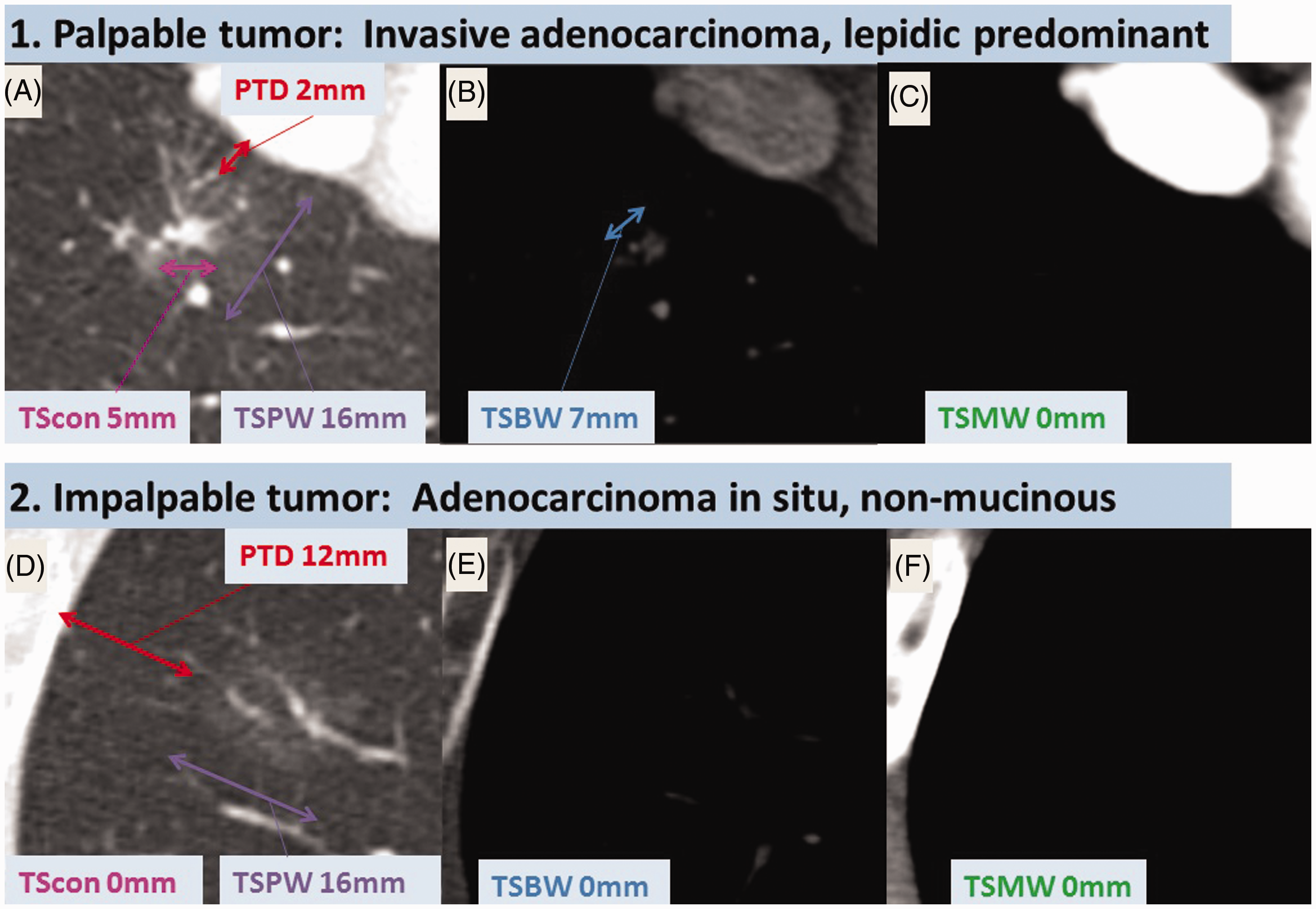
All histopathological examinations of the resected lung specimens were performed by pathologists, and the findings were compared between impalpable lesions and palpable lesions. Pulmonary adenocarcinomas were classified based on the predominant subtype as defined by the 2011 international classification, 13 and subtyped semiquantitatively using assessment of each component in 5% increments. The lepidic component rate of the adenocarcinomas was compared between impalpable lesions and palpable lesions. Hematoxylin and eosin and elastica-van Gieson staining was performed on adenocarcinoma sections to differentiate collapsed foci from fibrotic foci. The proportion of these foci to the whole tumor area (collapsed foci rate and fibrosis foci rate) at maximal tumor size on tissue sections was compared between impalpable lesions and palpable lesions.
Continuous variables were analyzed using Student’s t test and categorical variables using Fisher’s exact test. Statistical significance was defined as p < 0.05. Receiver-operating characteristic analysis was used to evaluate the sensitivity and specificity of detecting an impalpable pulmonary lesion by HRCT on each window level setting.
Results
Patient demographics and history, tumor size, and pleural-tumor distance in impalpable and palpable lesions.
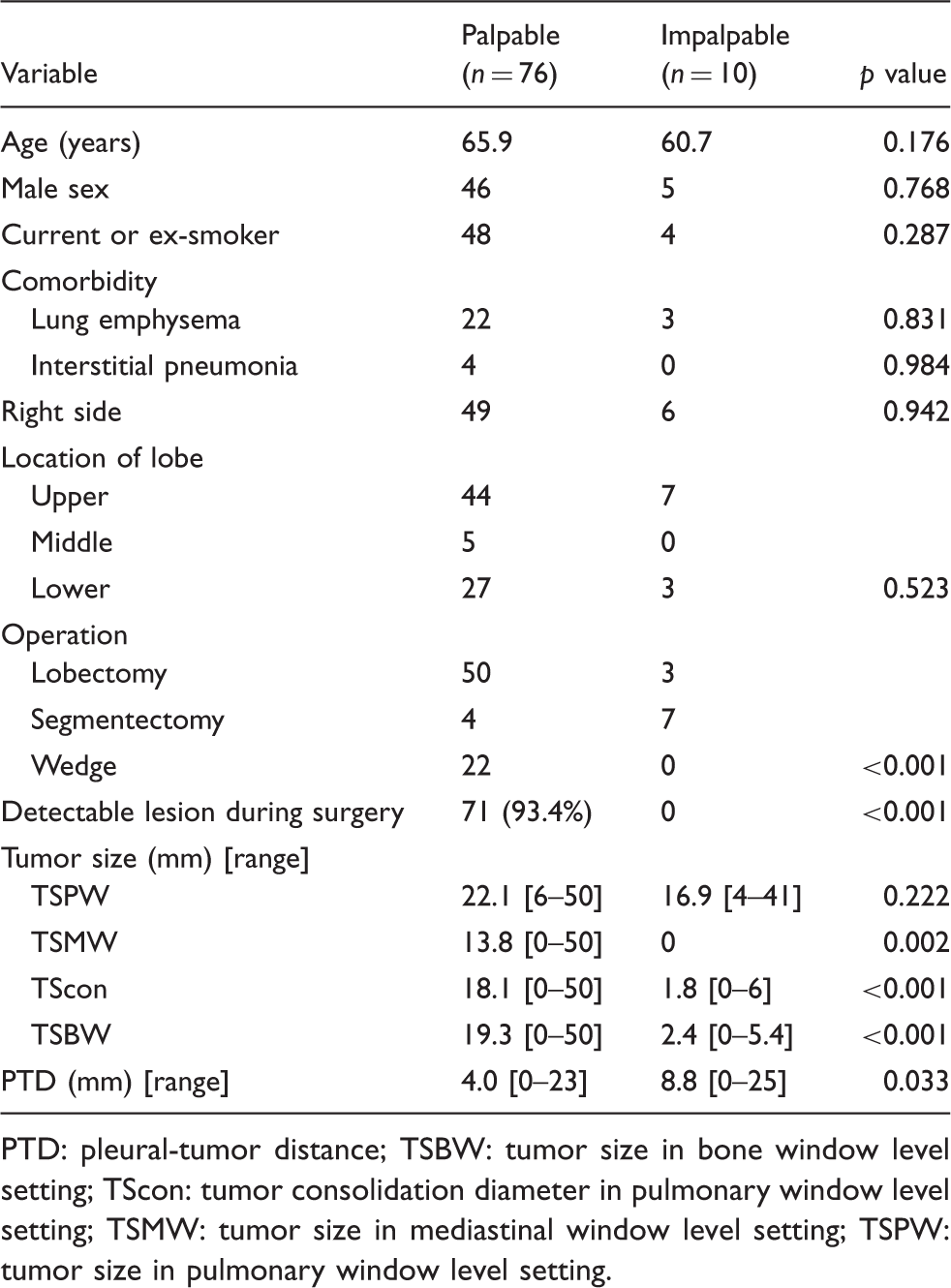
PTD: pleural-tumor distance; TSBW: tumor size in bone window level setting; TScon: tumor consolidation diameter in pulmonary window level setting; TSMW: tumor size in mediastinal window level setting; TSPW: tumor size in pulmonary window level setting.
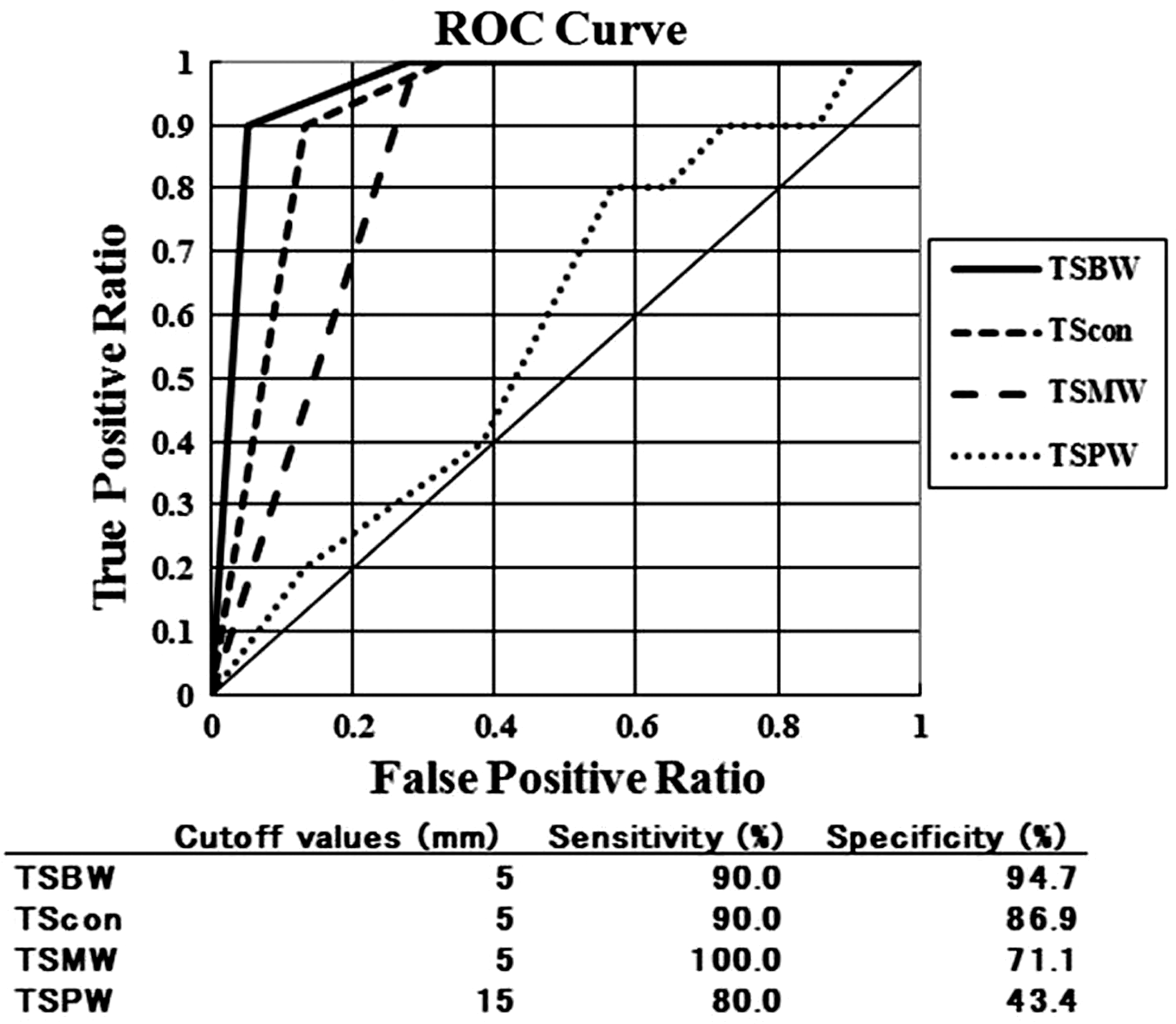
Receiver-operating characteristic (ROC) analysis was conducted for each tumor size. The tumor size in bone window level setting (TSBW) and tumor consolidation diameter in a pulmonary window level setting (TScon) had the highest areas under the curve. The sensitivity and specificity for identifying impalpable pulmonary lesions were: 90.0% and 94.7%, respectively, when TSBW ≤ 5 mm; and 90.0% and 86.9%, respectively, when TScon ≤ 5 mm. TSMW: tumor size in mediastinal window level setting; TSPW: tumor size in pulmonary window level setting.
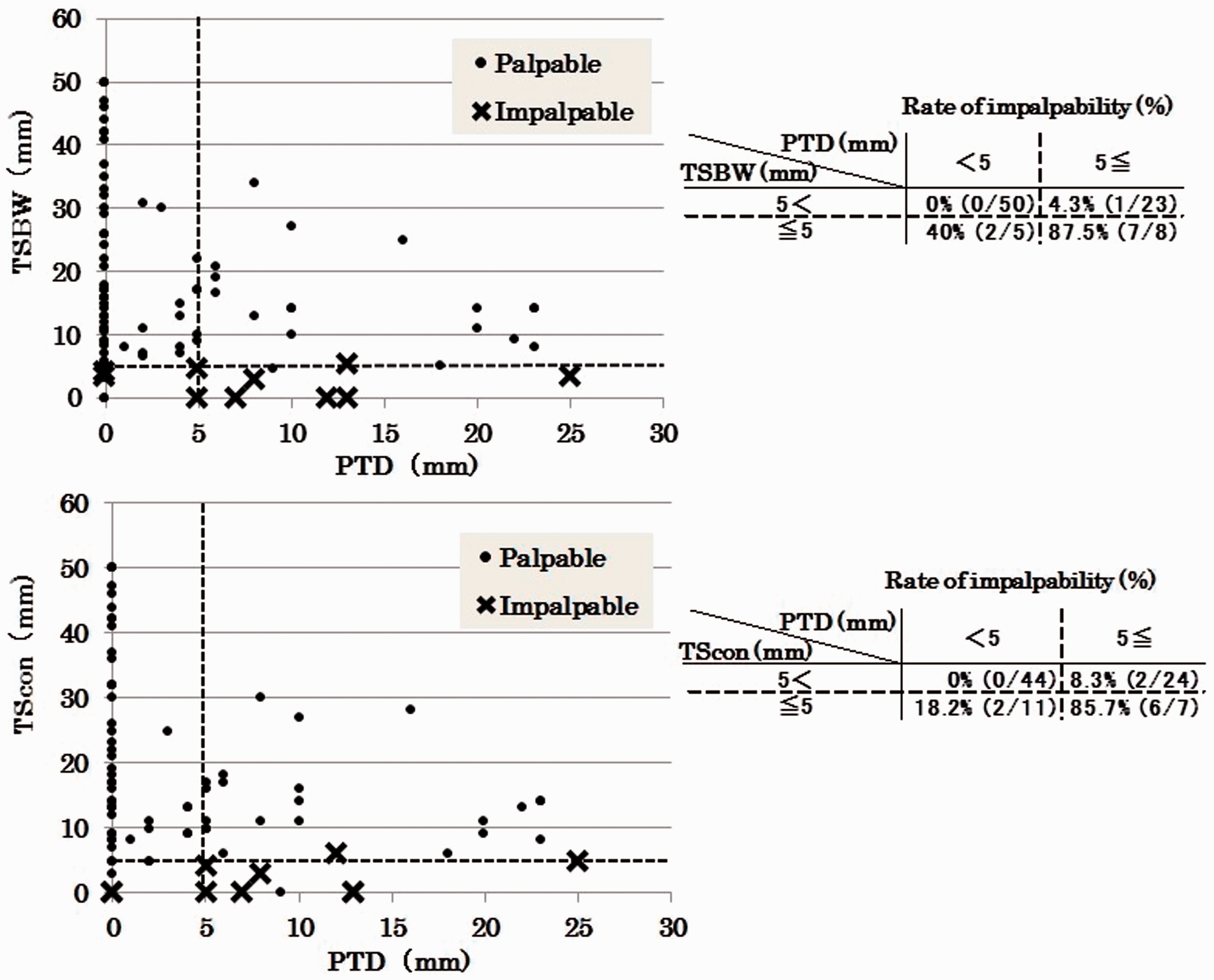
Pulmonary lesions with a tumor size in bone window level setting (TSBW) ≤ 5 mm and a pleural-tumor distance (PTD) ≥ 5 mm or tumor consolidation diameter in a pulmonary window level setting (TScon) ≤ 5 mm and PTD ≥ 5 mm were impalpable with probabilities of 87.5% (7/8) and 85.7% (6/7), respectively. When PTD < 5 mm, the probability of predicting an impalpable pulmonary lesion decreased to 40% (2/5) and 18.2% (2/11) when TSBW and TScon were ≤5 mm, respectively.
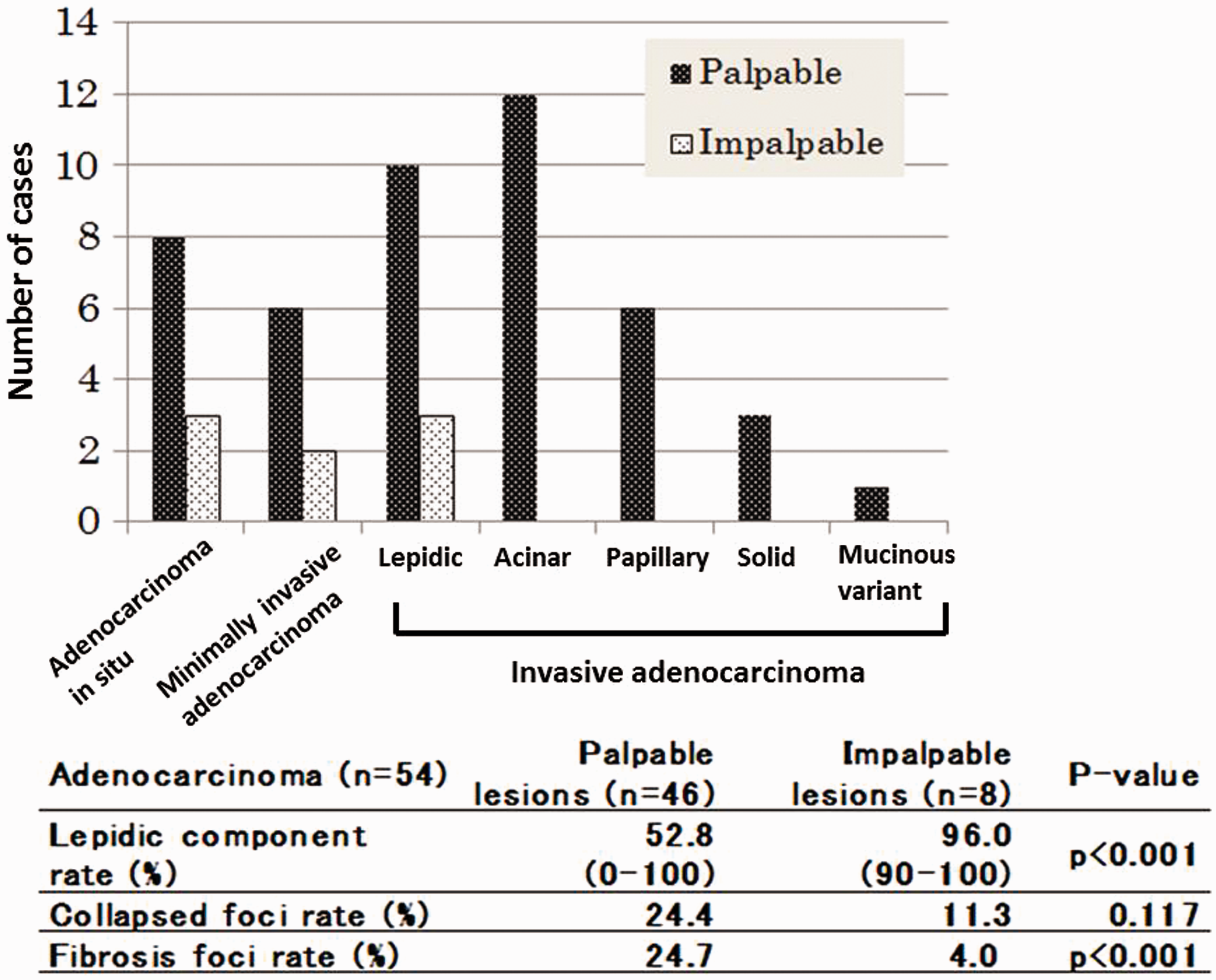
Three adenocarcinomas in situ, 2 minimally invasive adenocarcinomas, and 3 invasive lepidic-predominant adenocarcinomas were impalpable, but all other adenocarcinoma types were palpable. The lepidic component rate of impalpable lesions was significantly higher than in palpable lesions. There was a significant difference in fibrosis foci rate between impalpable lesions and palpable lesions.
Discussion
Small pulmonary lesions with GGO are being detected more frequently as HRCT becomes increasingly common. Complete resection of lung cancer with GGO appearance using minimally invasive surgery has a favorable prognosis. 14 These lesions should be removed with sufficient margins by wedge resection or segmentectomy, which requires that the pulmonary lesions are identifiable intraoperatively. However, deep GGO lesions are often difficult to identify intraoperatively because they are usually not palpable or visible.3,10 Preoperative marking, such as hookwire placement, CT-guided bronchoscopic barium marking, virtual-assisted lung mapping, or CT-guided percutaneous marking, is necessary to accurately resect the lesion, allowing the thoracic surgeon to identify the lesion location with certainty.5–8 However, these preoperative procedures are invasive and risk life-threatening complications. Hookwire marking is a common technique but it risks pneumothorax, pulmonary hemorrhage, and air embolism, and considered costly at 200 USD.3,15 Because there are no standard criteria for performing preoperative marking, redundant techniques may be employed in some cases, which needlessly increase risk as well as costs. Preoperative marking has been performed on palpable pulmonary lesions in previous reports, but these techniques should be carried out exclusively on impalpable pulmonary lesions.
TSPW, PTD, tumor hardness, skin incision length, magnitude of intraoperative lung collapse, and the expertise of the surgeon are associated with the predictability of impalpability. Palpation of the fresh resected lung specimen could minimize the effect of surgical factors such as incision length and the magnitude of intraoperative lung collapse, which would improve the palpation quality beyond what can be achieved intraoperatively. This hypothesis is supported by the fact that all pulmonary lesions that were palpable in the fresh resected lung specimens were also detectable intraoperatively (Table 1). TSBW ≤ 5 mm and PTD ≥ 5 mm, or TScon ≤ 5 mm and PTD ≥ 5 mm were found to be simple criteria to predict impalpable tumors at higher probabilities (87.5% and 85.7%, respectively) compared to previous reports. Several studies have implicated TSPW and PTD as factors associated with palpability during VATS.9–12 Suzuki and colleagues 9 recommended that localization techniques be used for lesions with TSPW ≤ 10 mm and PTD ≥ 5 mm before performing VATS, because these lesions were impalpable with a 63.0% probability. Similarly, Saito and colleagues 10 reported that pulmonary lesions requiring localization during VATS could be discerned using the formula PTD = (0.836 × TSPW) −2.811. Tamura and colleagues 11 reported that a non-solid tumor located at a PTD > 3 mm or a solid tumor located at a PTD ≤ (0.4 × TSPW) −0.9 mm required preoperative marking due to impalpability during VATS. 11 In contrast to these reports, we demonstrated that the TSPW was less important for palpability, and the most important factor was the size of the solid portion of the pulmonary lesion where tumor cells were actively proliferating with fibrotic changes. CT density correlated with tumor hardness previously. 3 Based on our findings, TSBW and TScon, which represent the size of the solid portion of the lesion, were most responsible for palpability. We found that lesions with TSBW ≤ 5 mm and PTD ≥ 5 mm, or TScon ≤ 5 mm and PTD ≥ 5 mm were impalpable in both the resected specimen and during thoracotomy; therefore, these tumors require preoperative marking definitively. Several lesions were palpable despite TSBW ≤ 5 mm or TScon ≤ 5 mm because they were located immediately beneath the pleural surface (PTD < 5 mm). These lesions were slightly visible, which allowed the surgeon to palpate the lesion more easily.
Pulmonary adenocarcinoma with predominately lepidic components is typically impalpable even when the tumor is large or located near the pleural surface. 3 Tamura and colleagues 11 reported that adenocarcinomas (Noguchi types A and B, or AIS) were impalpable. Suzuki and colleagues 9 found that 30% of granulomas and 22% of intrapulmonary lymph nodes were impalpable during VATS. In our study, all granulomas were palpable, but 8 impalpable lesions were adenocarcinomas with a lepidic component rate ≥ 90%. We found that an important pathological factor affecting adenocarcinoma palpation was a higher fibrosis foci rate combined with a lower lepidic component rate, although collapsed foci were less associated. However, AIS lesions were palpable at times. Because 8 (72.7%) AIS lesions were palpable, we hypothesized that palpable AIS lesions visible on HRCT in a bone window level setting comprised a high tumor cell density. Moreover, AIS residing superficially beneath the pleura may be detected using both palpation and visual examination.
In a previous study, impalpable lesions underwent either preoperative marking or were diagnosed and treated using anatomical segmentectomy. 16 Anatomical segmentectomy was performed without preoperative marking for 7 impalpable lesions (70%) in this study, and the frozen section analysis showed that the pulmonary lesions were resected completely with sufficient margins. It is one of the alternative strategies to perform anatomical segmentectomy for the unmarked lesions with a TSBW ≤ 5 mm and PTD ≥ 5 mm, or a TScon ≤ 5 mm and PTD ≥ 5 mm. The data employed were of high quality and reliable because HRCT was performed in all window level settings for every pulmonary lesion. However, this study is limited because some lesions that were deemed palpable in the resected specimen might be difficult to detect during surgery due to intraoperative factors such as the skin incision length and the lesion location, which were both associated with the success of intraoperative localization. Because this study was a retrospective investigation with small numbers, a further prospective study in a large patient population is necessary to demonstrate the utility of TSBW, TScon, and PTD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.