
Abstract
Objective
To compare the use of thermoreactive nitinol clips with the classic Robicsek technique for treatment of sternal dehiscence after cardiac surgery.
Methods
Eighty-two (2.3%) of 3564 open heart surgery patients underwent reoperation for sternal dehiscence between October 2011 and 2012. Prospectively collected data from 26 (31%) consecutive patients who underwent reoperation using thermoreactive nitinol clips were compared with those of a retrospective cohort of 42 (51.2%) who were treated with the classic Robicsek technique. To overcome baseline and operative variations, we constructed a propensity model using logistic regression.
Results
Overall mortality occurred in 3 (5%) patients and a second revision was performed in 2 (7.7%) in the nitinol clip group and 2 (6.3%) in the control group (p > 0.05). Postoperative results were similar except for the mean time of operation which was significantly shorter in the nitinol clip group, and patients in this group required substernal dissection slightly less frequently than those in the control group.
Conclusions
Thermoreactive nitinol clips allow the surgeon to perform a rapid and less challenging technique for sternal reoperations, without additional complications. Using this technique in an identical group with a finite sample size, we accomplished similar early results to those of the classic Robicsek technique.
Keywords
Introduction
The preferred approach for the majority of cardiothoracic operations is the classic median sternotomy. Sternal closure using steel wires has been performed safely since Julian and colleagues 1 described it in 1957. Novel techniques have been introduced for closure of the sternum after open heart procedures, including transverse titanium plate fixation, the Sternal Talon device, and thermoreactive nitinol clips (TRNC). Of these techniques, primary use of the TRNC system has been shown to reduce postoperative complication rates in prospectively designed randomized studies.2–6 The TRNC system was also reported to be useful in the treatment of sternal dehiscence. 7 However, it is not well established whether the TRNC system can be used routinely instead of established methods such as the Robicsek technique for the treatment of sternal dehiscence. The purpose of this study was to compare the novel TRNC technique that was established on the principle of bringing both hemi-sternums together without harming the intercostal structures, with the Robicsek technique which entails rewiring the sternum around strengthening parasternal steel wires. To avoid various confounding risk factors, a comparison was carried out on the basis of propensity score matching.
Patients and methods
Pre-matching comparison of baseline characteristics.
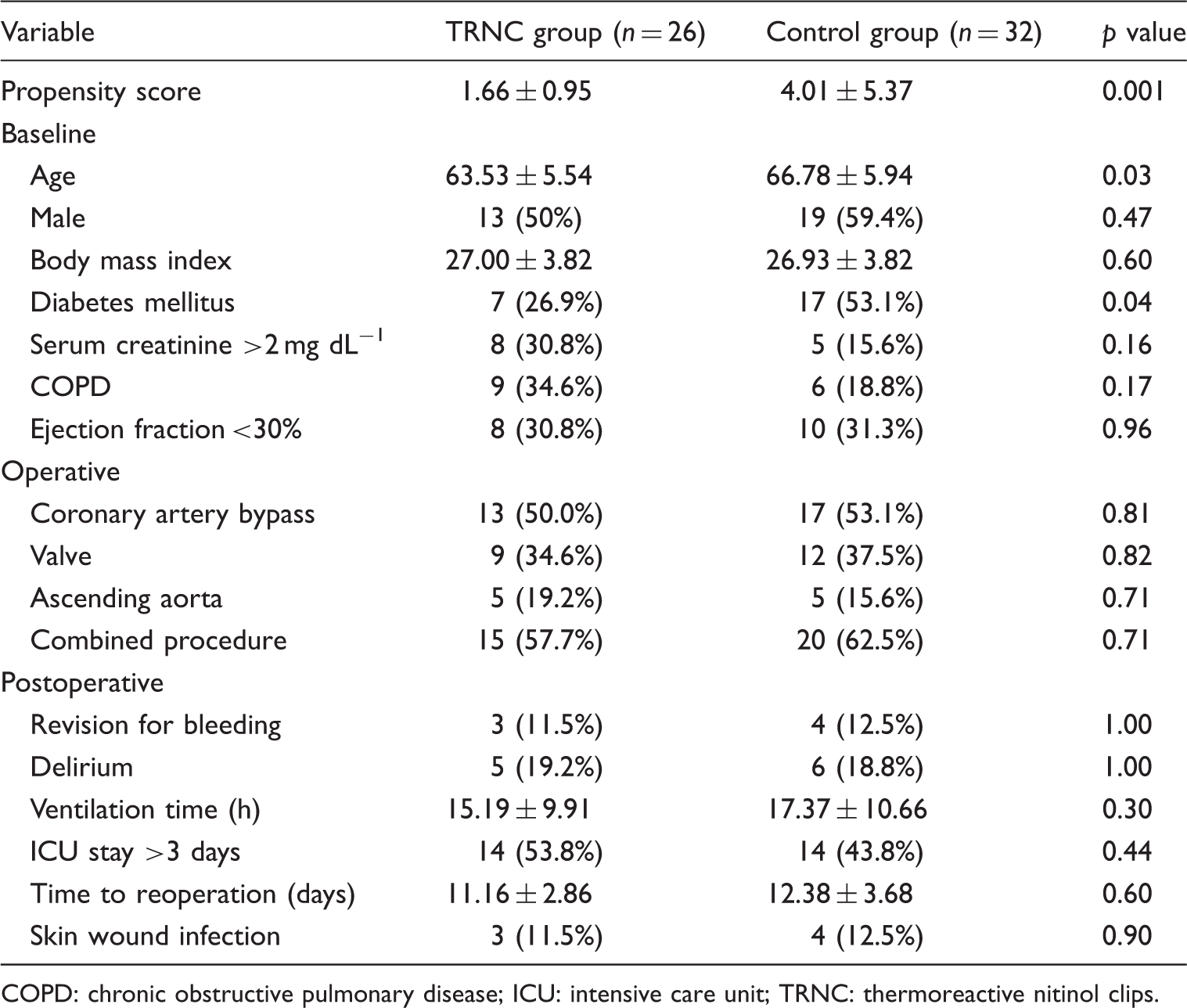
COPD: chronic obstructive pulmonary disease; ICU: intensive care unit; TRNC: thermoreactive nitinol clips.
Institutional protective measures against major wound infection and sternal dehiscence include: a bath with chlorhexidine soap the night before the operation, surgical site antisepsis with povidone iodine 10%, whole body shaving two days before the operation, antibiotic prophylaxis with 1 g cefazolin (with the dose doubled in those >80 kg) and activity restriction for 6 to 8 weeks after the surgery. In our operations, assistants generally undertake sternal closure after the primary operation, and the usual application is placement of no. 6–7 stainless steel wire U-sutures, one by one without crossing.
In reoperations, previous wire sutures were removed, mediastinal tissue and fluid cultures were collected in patients with apparent or suspected infection. Necrotic and infected tissues were carefully debrided. TRNC were placed either with or without the dissection of the substernal tissues, depending on the extent and depth of infection. In patients in whom dissection of the substernal tissues was not performed, initial holes were opened through the intercostal spaces close to the parasternal edges, using electrocautery. Both hemi-sternums were put together and stabilized with two Backhaus forceps, which were applied at the holes. The sternal horizontal diameters were measured with aid of the sizing tool provided. The clips were put into refrigerated (<5℃) sterile saline solution. They became forgeable in minutes and adequately enlarged by bending. The clips were inserted into the holes, beginning from the superior to the inferior, and at least 4 horizontal placements were made for each patient. The clips were then heated with warm water (above 45℃). After they resumed their original shape and regained stiffness, the Backhaus forceps were removed. In cases of segmental sternal fractures, bone stumps were initially put together at both upper and lower ends, and the fractured segment was stabilized with longitudinally placed clips of appropriate size (Figure 1). In patients in whom dissection of the substernal tissues was required, substernal tissues or adhesions were dissected close to the costochondral junction using electrocautery. TNRC were placed at the intercostal distances without using steel wires. Care was taken to avoid vascular injury, especially when opening holes for TRNC insertion. In the control group, substernal tissues or adhesions were dissected first. Preliminarily, each half of the sternum was fastened by continuous parasternal wire sutures, as described by Robicsek and colleagues.
8
The hemi-sternums were approximated with a number of single parasternal stitches that were passed laterally and perpendicularly to the previous parasternal suture line. Adequate reinforcement was provided and the two ends of the sutures were tied together. Skin layers were then closed appropriately.
(a) The thermoreactive nitinol clips. (b) Thermoreactive nitinol clips placed longitudinally. (c) Thermoreactive nitinol clips placed crosswise horizontally. (d) Thermoreactive nitinol clips inserted through the intercostal holes.
Computerized data of the patients were reviewed for reassessment of those in whom the Robicsek technique was used (median time interval was 9 days, range 7 to 11 days). TRNC patients were called back for a follow-up visit after the operation (median time 8 days, range 7 to 9 days) and reassessed by the surgical team who performed the operation.
To overcome intergroup variations and create two identical groups with regard to potential risk factors, a non-parsimonious propensity score analysis was performed using 16 parameters. As described by Blackstone, 9 by assigning the group variable as the dependent, a coefficient (β) was calculated for each risk parameter using logistic regression. The model was well-calibrated (Hosmer-Lemeshow test p = 0.604). The coefficient was put into the formula: 1/[1 + exp(-β1*variable1) + (β2*variable2) + (βn*variable-n) + model intercept)], and a propensity score was calculated for each patient. Paired nearest-neighbor matching was performed for construction of the matched population. A specified caliper of 0.85 was used with the pooled standard deviation of the propensity score being 4.18. The final model included 21 patients from each group who had similar propensity scores. All statistical analyses were performed using SPSS version 16.0 software (SPSS, Inc., Chicago, IL, USA). Visual histograms and analytical methods (Kolmogorov-Smirnov or Schapiro-Wilks test) were used for determination of a normal distribution. Continuous parameters are presented as mean ± standard deviation. Categorical data are presented as number and percentages, and proportions between the two groups were compared using the chi-square test or Fisher’s exact test. The Mann Whitney U test was used for comparison of nonparametric variables, and the independent samples t test was used for comparison of parametric variables. p < 0.05 was considered significant.
Results
Post-matching comparison of baseline characteristics.
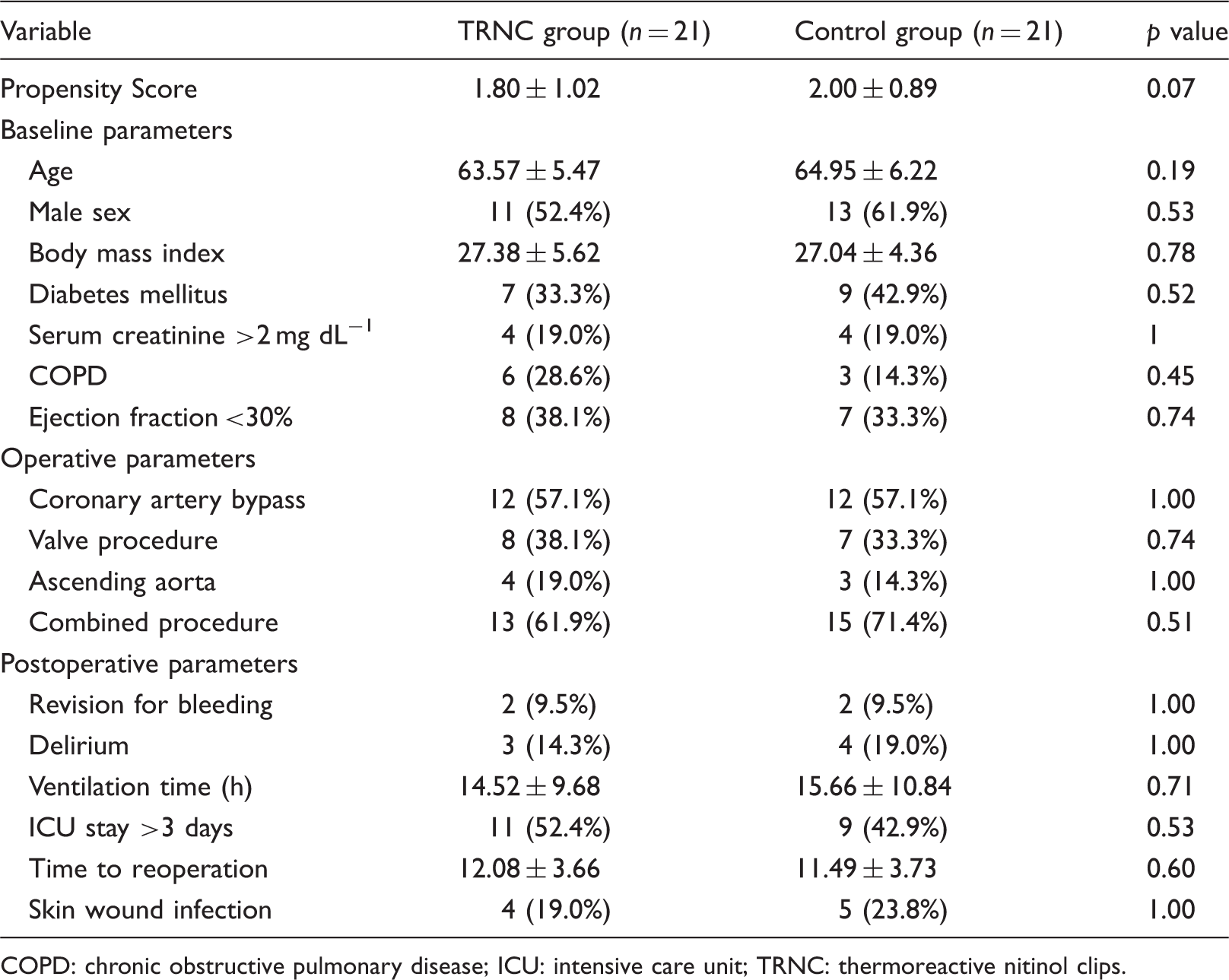
COPD: chronic obstructive pulmonary disease; ICU: intensive care unit; TRNC: thermoreactive nitinol clips.
Postoperative results of matched groups.
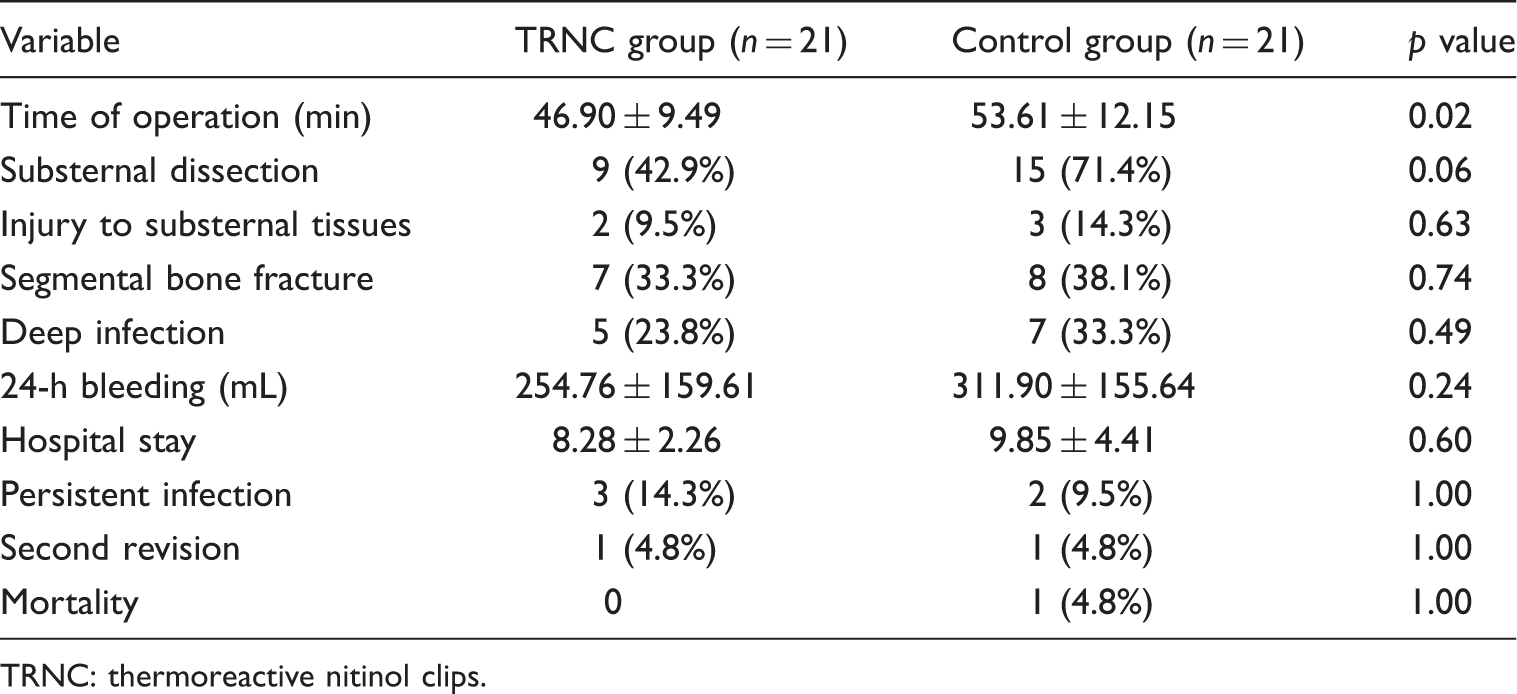
TRNC: thermoreactive nitinol clips.
Discussion
In this study, we compared the surgical results of the TRNC technique and the classic Robicsek technique for treatment of sternal dehiscence after open heart surgery. The main findings with the TRNC system are that it provides an easier technique and a shorter operation time. It is also a safer technique because it may require less need for substernal dissection compared to the Robicsek technique. The TRNC technique cannot be considered inferior to the Robicsek technique in terms of early postoperative outcomes.
Use of the TRNC technique in patients with the complication of postoperative sternal dehiscence was reported previously. Guler and colleagues 10 reported satisfactory results in 16 patients in whom they performed the technique. Gucu and colleagues 11 reported similar results in patients with noninfective sternal dehiscence. However, results of both studies are far from being superior to any other technique because they failed to include a control group. The prospective study of Negri and colleagues 6 randomized 1000 patients who underwent primary open heart operations to receive either classic wiring or application of the TRNC system for primary sternal closure. The incidence of infection-free dehiscence was 14/500, whereas this ratio is 1/500 in sternal closure using TRNC (p = 0.002); the incidence of infected dehiscence in conventional sternal closure was 9/500 while the ratio was found to be 0/500 in sternal closure via TRNC (p = 0.007). In contrast to these findings, it was observed that development of superficial wound infection and sternal aseptic necrosis was not significantly different between groups. The most recent prospective randomized study also compared the classic technique and TRNC for primary sternal closure. The authors included a cost analysis and showed that the TRNC system was associated with a lower incidence of sternal wound complications. The nitinol clip system was proven to be cost-effective in cardiac surgery. 5 Our study group comprised only patients with sternal dehiscence, and the wound infection rate was somewhat higher compared to these studies. The deep infection incidence was slightly higher in the control group, whereas persistence of infectious signs and symptoms was more commonly observed in the TRNC group although both differences did not reach statistical significance.
Nitinol clips have shown some significant advantages in comparison to steel wires in that they contact 5–7-times more of the bone surface than traditional wires and keep the sternum under pressure, thus there is much less risk that the bone is torn. They are also applied faster, more easily, and without harm to the bone. The thermoreactive characteristics also allow them to be removed when required (nitinol clips are not integrated into the bone). Compatibility of the material with computed tomography scans and nuclear magnetic resonance is no different from that of steel wires. The risk of bleeding is less than that with conventional wires. They are also 10%–15% more flexible under conditions in which tension increases, such as during intensive coughing episodes or overload.4,6 The classic technique described by Robicsek and colleagues 8 in 1977 has some advantages: it stabilizes a fragile and defective sternum, prevents the bone from being cut through by wires, and relocates the pressure over the sternum. The shortcoming of this technique is the effect on the blood flow to the area. During Robicsek operations, when intercostal arteries are squeezed by the ring formed by anterior-posterior up-and-down passing of steel wires around the rib bone, sternal blood flow may be interrupted, and an effective sternal approach cannot be reached.12,13 Moreover, bilateral internal mammary artery usage also interrupts sternal blood flow and these patients display a 5% incidence of sternal wound complications. 14 Because TRNC systems do not directly contact the rib bone, nor do they have direct metal-tissue contact, technically, they do not affect sternal blood flow. In our study, the rates of coronary artery bypass grafting were similar between the two groups and a second revision was required in one patient from each group. Due to the finite sample size and lack of long-term data, the most we can say currently is that using the TRNC system does not constitute an additional risk in the treatment of sternal dehiscence in patients who underwent coronary artery bypass grafting using the left internal mammary artery.
The retrospective control group and small population size were the major limitations of this study. Because our study did not include patients with primary closure, we could not come to a conclusion about extending the usage of the TRNC system for various conditions. Finally, a follow-up visit would have provided useful information, however, the patients did not respond to the invitation because they lived in distant regions of country. We concluded that thermoreactive nitinol clips may be used effectively and safely not only in primary closure of the sternum but also in the treatment of postoperative sternal dehiscence. The technique allows the surgeon to perform a rapid and less challenging technique without the risk of additional complications. Using the technique in an identical group with finite sample size, we accomplished similar early results to those of the classic Robicsek technique.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commerical, or not-for-profit sectors.
Conflict of interest statement
None declared.