
Abstract
Background
Although thoracoscopic surgery is widely performed for early-stage lung cancer, only a few small studies have evaluated the role of video-assisted thoracoscopic surgery in patients with locally advanced lung cancer who had received preoperative chemotherapy.
Methods
Among 1655 patients who underwent anatomical lung resection for lung cancer between January 2009 and December 2014 in our institution, we retrospectively examined the short- and long-term outcomes of 110 (6.6%) who had undergone induction therapy. Thoracoscopic surgery was performed in 79 of these patients and thoracotomy in 31.
Results
In the thoracoscopic group, conversion to a thoracotomy was required in 4 patients. More combined resections were included in the thoracotomy group, and combined resection of large vessels or the carina was carried out only via a thoracotomy. Postoperative complications of grade 3 or above were found in 15 (13.6%) patients, and there was no significant difference in the incidence of postoperative complications between the 2 groups. The 3- and 5-year survival rates for the patients overall were 58.6% and 50.3%, respectively. Although there was no significant difference in overall outcome between the 2 groups, the patients with postoperative ypN2 status in the thoracoscopic group had a significantly better outcome than those in the thoracotomy group.
Conclusion
Although video-assisted thoracoscopic surgery was not suitable for central advanced lung cancer requiring angioplasty or carinal resection, it seems to be useful for patients with locally advanced lung cancer who had undergone induction therapy, especially patients with peripheral lung cancer and mediastinal lymph node metastasis.
Keywords
Introduction
Lung cancer continues to be a major cause of cancer mortality worldwide, and approximately one-third of patients with lung cancer are diagnosed as having locally advanced disease. For patients with stage II and III non-small-cell lung cancer (NSCLC), multimodality treatment remains the standard of care, and surgical resection is an important part of the treatment in locally advanced cases. Although thoracoscopic surgery for early-stage lung cancer is widely performed, the role of thoracoscopic surgery in locally advanced lung cancer is not clear, and only a few studies have evaluated the role of video-assisted thoracoscopic lobectomy in patients with locally advanced NSCLC who had received preoperative chemotherapy.1–8 Therefore, we retrospectively examined the short- and long-term outcomes of patients who had preoperative chemotherapy followed by resection via thoracotomy and those who had undergone video-assisted thoracoscopic surgery (VATS) in order to clarify whether the use of VATS is associated with any significant differences in terms of safety and oncologic outcomes in comparison with resection via thoracotomy.
Patients and methods
The institutional review board approved this retrospective study. The need for subsequent individual consent from patients whose records were evaluated was waived because the individuals were not identified in this study. Among 1655 patients who underwent anatomical lung resection for lung cancer between January 2009 and December 2014 in our institution, 132 (8.0%) received preoperative induction therapy. Among these patients, 14 who had undergone preoperative treatment in other hospitals and 8 who had small-cell lung cancer were excluded, leaving 110 patients for study enrollment. Clinical data were obtained from the medical records and reviewed retrospectively.
There were 100 (90.9%) men and 10 (9.1%) women, and the mean age was 64.1 years (range 41–83 years). The choice of preoperative chemotherapy alone or chemoradiotherapy was decided by consensus of the respiratory physicians, according to the condition of the individual patient and the degree of tumor progression. The chemotherapy protocol did not remain the same during the study period. Although platinum agents were mainly used, other anticancer drugs were used in various combinations. Sixty-two patients received cisplatin-based chemotherapy (mainly cisplatin + vinorelbine) and 47 had carboplatin-based chemotherapy (mainly carboplatin + taxanes). Pemetrexed was administered as a single agent in one patient. The patients received an average of 2.5 courses. Radiotherapy was performed in 21 cases, and an average of 51.4 Gy (range 14–60 Gy) was administered.
The patients were divided into two groups: a VATS group and a thoracotomy group. Seventy-nine patients had thoracoscopic surgery (VATS group) and 31 had a thoracotomy (thoracotomy group). For clinical staging, all patients underwent a physical examination, chest radiography, computed tomography (CT) of the chest and abdomen, magnetic resonance imaging of the head, fiber bronchoscopy, and positron-emission tomography (PET). Preoperative staging of lymph nodes was usually carried out using CT and PET. Lymph nodes with a short-axis diameter of 10 mm or greater on CT and positive on PET were identified as lymph node metastases. Preoperative pathological staging of lymph nodes using endobronchial ultrasonography was undertaken in only 2 patients. Total dissection of regional lymph nodes (ipsilateral hilar and mediastinal lymph nodes) was performed in all patients. The histological type of the tumor was determined according to the 3rd edition of the World Health Organization classification. Pathological staging was determined according to the 7th edition of the American Joint Committee on Cancer guidelines for lung cancer staging.
Surgical resection was performed under general anesthesia using a double-lumen endotracheal tube. At our institution, anatomical lung resection in patients with lung cancer is mainly by VATS, and a thoracotomy is chosen only when angioplasty of major vessels, resection of the tracheal bifurcation, bronchoplasty of the left lung, resection of a large tumor, or resection of the chest wall is required. If there are obvious signs of vascular invasion on chest CT, resection is undertaken via a thoracotomy; otherwise, we try to perform resection by VATS even when enlarged lymph nodes are present. In the VATS procedure, the entire surgry was carried out while viewing a monitor through the thoracoscope, without any rib spreading. A minithoracotomy incision approximately 3–4-cm long was made in the 4th intercostal space on the anterior axillary line as an access port. Two other stab wounds, each approximately 2-cm long, were made: one was in the 7th intercostal space on the mid-axillary line and used as the camera port, and the other was in the 6th or 7th intercostal space at the lower edge of the scapula, and used as an assist port. The thoracoscope was 10 mm in diameter and had a 30-degree lens. The pulmonary arteries were usually ligated using absorbable thread, and the pulmonary veins were dissected using an Endo-Stapler with staple dimensions of 2.0–2.5 mm. The main bronchus, lobar bronchus, segmental bronchus, interlobar fissures, and the intersegmental plane were divided using an Endo-Stapler with staple dimensions of 3.5–4.0 mm. The operative specimens were carefully removed via the wound in the anterior 4th intercostal space. When the tumor adhered firmly to the surrounding organs, dissection was carefully carried out using scissors forceps.
The criteria for conversion to a thoracotomy in our institution were: angioplasty necessitated by pulmonary artery invasion by the tumor, metastatic lymph nodes, or silicotic lymph nodes; difficulty in achieving complete resection by VATS because of a large tumor; the need for complicated anatomical lung resection to avoid pneumonectomy; the need for chest wall resection because of tumor invasion; intraoperatively large vessels and bronchial injury; and mechanical failure of the automatic suturing device.
Postoperative complications were classified according to Common Terminology Criteria for Adverse Events (CTCAE) version 4.0, and we considered only those with a CTCAE grade of 2 or more. Prolonged air leak persisting over 7 days was defined as a grade 2 postoperative complication. Operative mortality was defined as death at any time during the initial hospitalization or within 30 days postoperatively.
Data were compared using the chi-square test. The Mann-Whitney U test was used to assess associations between quantitative variables. Survival rate were calculated by the Kaplan-Meier method, and comparisons among the survival curves were made using the logrank test. Zero time was the date of pulmonary resection, and the terminal event was death attributable to cancer, noncancerous causes, or unknown causes. Univariate analysis was performed using the Cox proportional hazards model. Differences with a p value <0.05 were considered to be significant. Statistical analysis was carried out using the Stat-View version 5.0 software package (SAS Institute, Inc., Cary, NC, USA).
Results
Conversion to an open thoracotomy was required in 4 patients. Among these, metastatic lymph nodes could not be detached from the pulmonary artery due to tumor invasion in 2, and conversion to an open thoracotomy was needed for angioplasty. In the other 2 cases, conversion was necessary because of difficulty in securing a good view due to a large tumor with phrenic nerve invasion in one patient, and for resection of the chest wall in the other. These 4 patients were included in the VATS group for later analysis. The thoracotomy group had significantly more patients with squamous cell carcinoma. Bronchoplasty was undertaken in 10 patients including 4 who underwent a right pneumonectomy with carinal resection. Bronchoplasty was performed via thoracotomy in 7 patients and by VATS in 3 (including one with conversion to open thoracotomy). Combined resection was performed more often in the thoracotomy group (74.2% vs. 30.4%, p < 0.0001). All cases involving combined resection of large vessels (pulmonary artery, superior vena cava) were treated via thoracotomy. In 5 cases, lobectomy was performed by VATS and resection of the chest wall via a small incision. There were no differences in clinical and pathological stages between the 2 groups. Three patients who underwent induction therapy in clinical stage I had double-lung cancer or a tumor diagnosed as small-cell lung cancer before induction therapy. Representative CT images of VATS, conversion, and thoracotomy cases before induction chemotherapy are shown in Figure 1. In the patients featured in Figures 1A and Figure 1B, all enlarged lymph nodes could be dissected by VATS. In the patient shown in Figure 1C, we tried VATS but enlarged lymph nodes involved in the tumor could not be detached from the pulmonary artery, so conversion to an open thoracotomy was performed for angioplasty. In the patient shown in Figure 1D, because tumor invasion into the superior vena cava was strongly suspected by preoperative CT, resection via thoracotomy was scheduled. Postoperative complications with CTCAE grade ≥2 occurred in 39 (35.5%) patients (VATS group: 36.7%, thoracotomy group 32.2%), among whom, 15 (13.6%) had CTCAE grade ≥3 complications (VATS group: 11.4%, thoracotomy group: 19.4%). There was no significant intergroup difference in the incidence of grade ≥2 postoperative complications. There were 2 perioperative deaths (one in each group) and the mortality rate was 1.8%. Both deaths were due to acute exacerbation of interstitial pneumonia. Intraoperative blood loss was significantly less and operative time was significantly shorter in the VATS group. Although there was no difference in postoperative drainage duration, postoperative hospital stay was significantly shorter in the VATS group. There was no significant intergroup difference in the proportion of patients who underwent postoperative adjuvant treatment. Seven patients had incomplete resection: 4 were p-stage IV (malignant effusion and pleural dissemination) and 3 had microscopic residual tumors at the surgical margin; therefore, complete resection was achieved in 103 cases. Fifty-four patients suffered tumor recurrence during study period, but there was no significant difference in recurrence rates between the VATS (50%) and thoracotomy (59.3%) groups. There was a tendency for local recurrence in the thoracotomy group, and for distant metastasis in the VATS group. We examined long-term outcomes in the 103 patients who had complete resection. The median follow-up was 34.2 months. Figure 2 shows the overall survival curves for patients who underwent complete resection; 3- and 5-year survival rates were 58.6% and 50.3%, respectively. Although the VATS group survived for longer, the difference between the 2 groups was not significant (Figure 3A). The relapse-free survival curve for the VATS group was also better although not to a significant degree (Figure 3B). In univariate analysis, younger patients had a significant better prognosis than the older age group. Although sex, histological type, preoperative radiation therapy, type of surgery, and combined resection had no significant influence on prognosis, patients with postoperative adjuvant therapy had a significantly better prognosis than those without adjuvant therapy. Patients with progressive disease on radiography had a worse prognosis, but the histological effect of induction therapy had no significant influence on prognosis. When we examined the outcome of patients with locally advanced lung cancer (clinical stages II and III), there was no significant difference in survival curves between the VATS and thoracotomy groups (Figure 4A). Because the clinical N factor was not confirmed pathologically, we examined the outcome of patients with postoperative pathological N2 (ypN2) status to investigate whether VATS was useful even in obvious N2 cases. We found that postoperative ypN2 patients in the VATS group had a significantly better outcome than those in the thoracotomy group (Figure 4B).
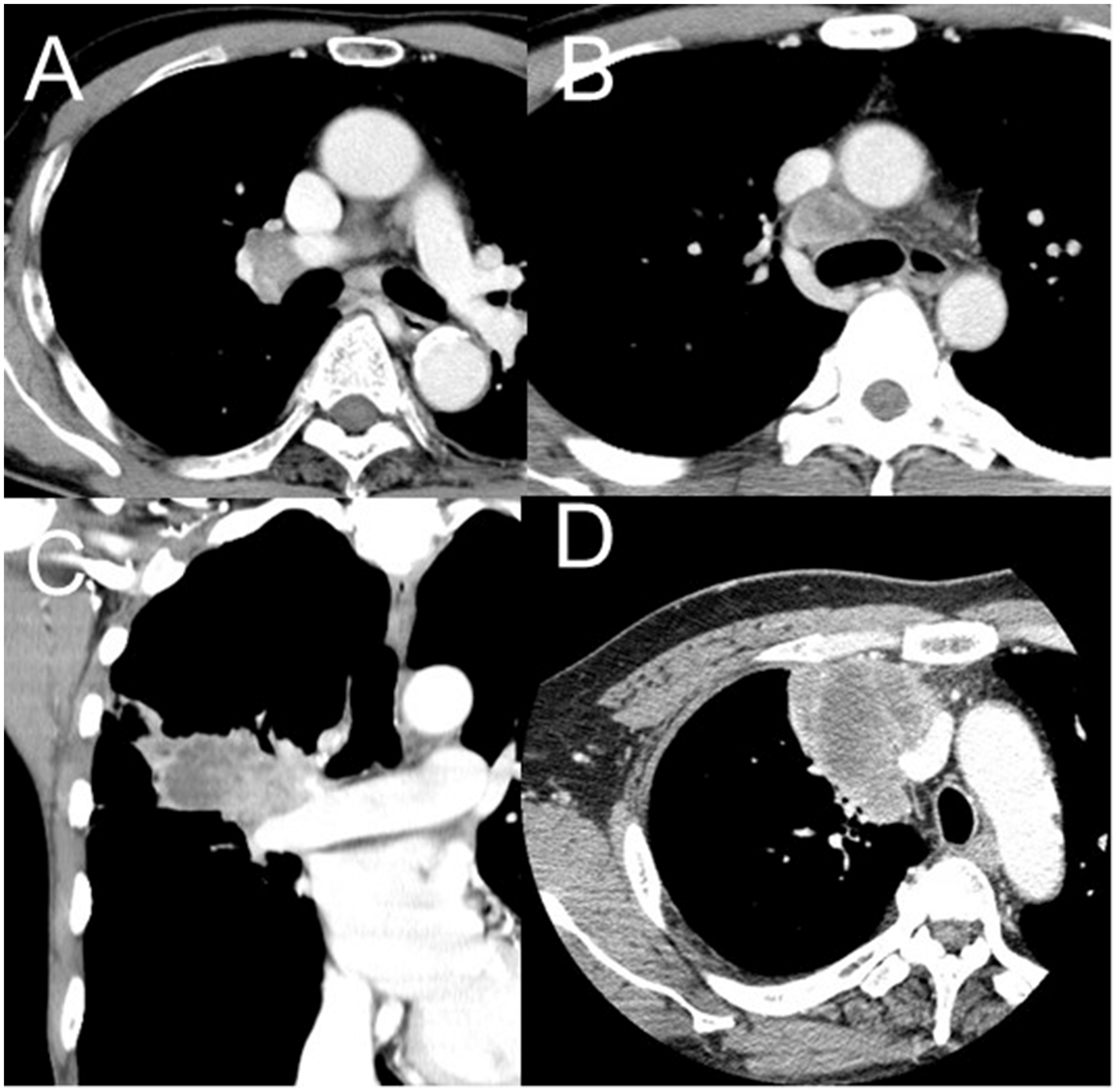
Representative computed tomography images. (A, B) Enlarged lymph nodes could be dissected completely by video-assisted thoracoscopic surgery. (C) A case of conversion to thoracotomy. Resection by video-assisted thoracoscopic surgery was tried, but enlarged lymph nodes involved in the tumor could not be detached from the pulmonary artery. Therefore, conversion to an open thoracotomy was performed for angioplasty. (D) Before induction chemotherapy: because tumor invasion into the superior vena cava was strongly suspected by preoperative chest computed tomography, resection via thoracotomy was scheduled.
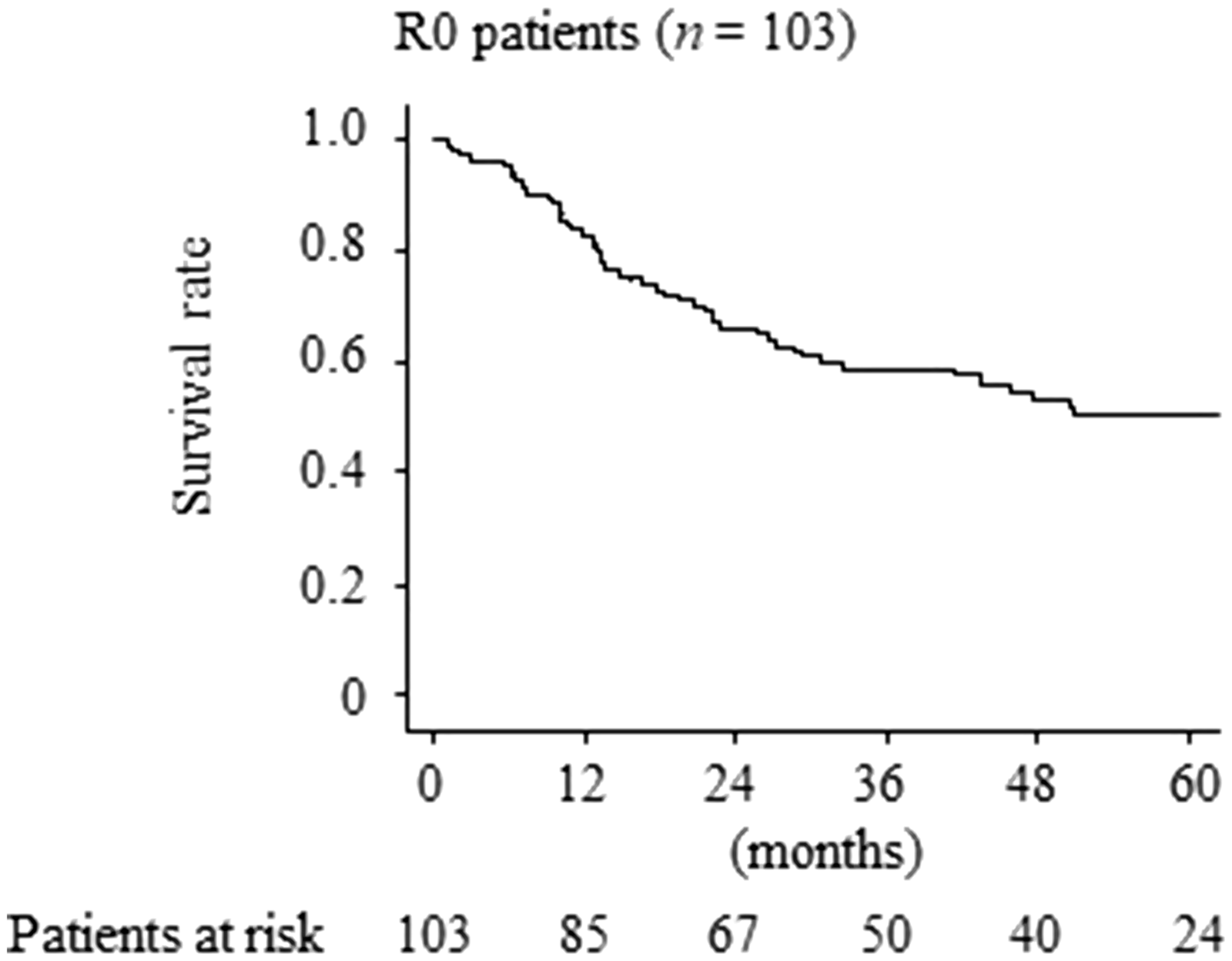
Overall survival curves of patients with complete resection. The 3- and 5-year survival rates for the patients who underwent complete resection were 58.6% and 50.3%, respectively.
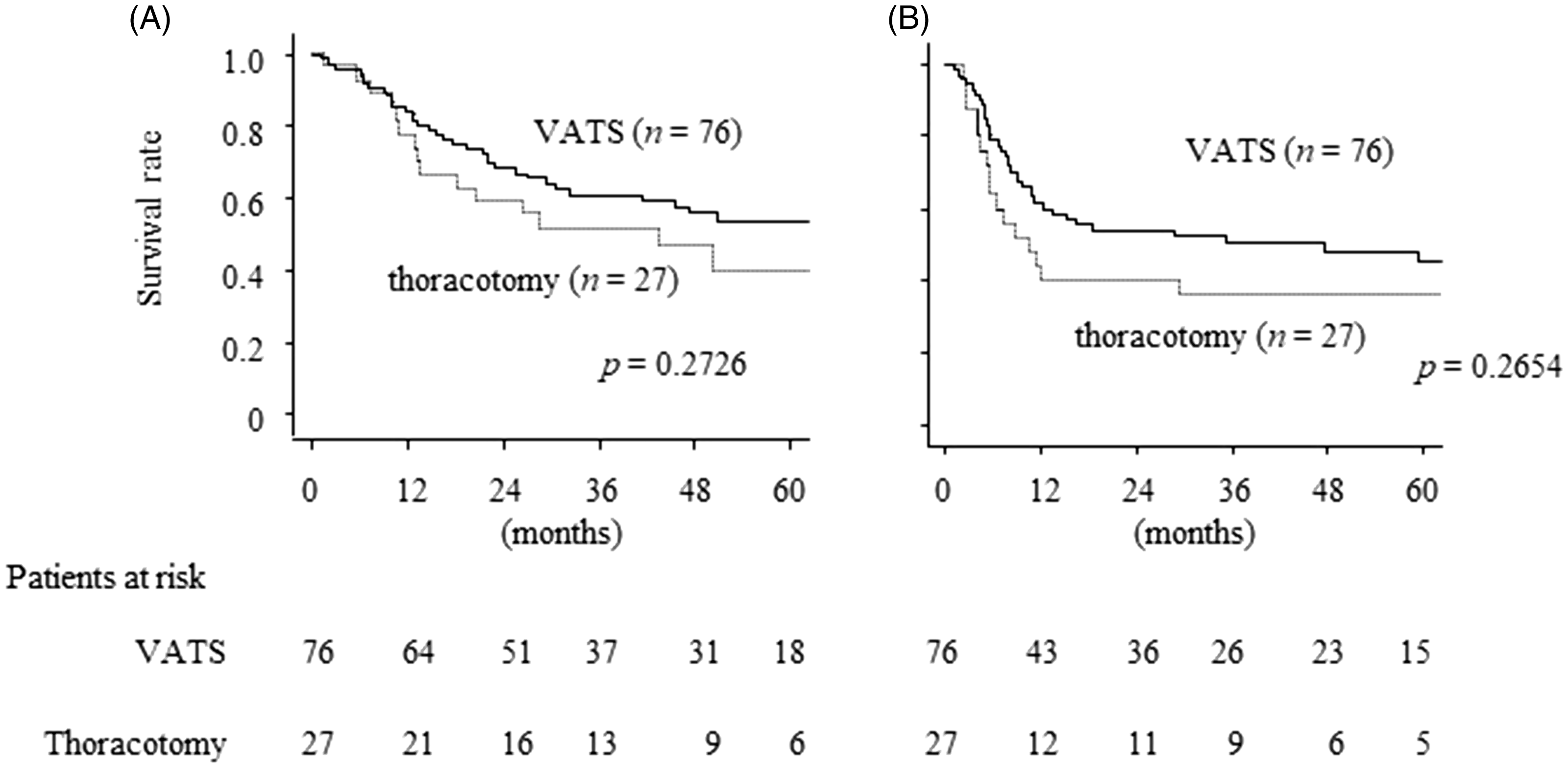
(A) Overall survival curves and (B) relapse-free survival curves of the video-assisted thoracoscopic surgery and thoracotomy groups.
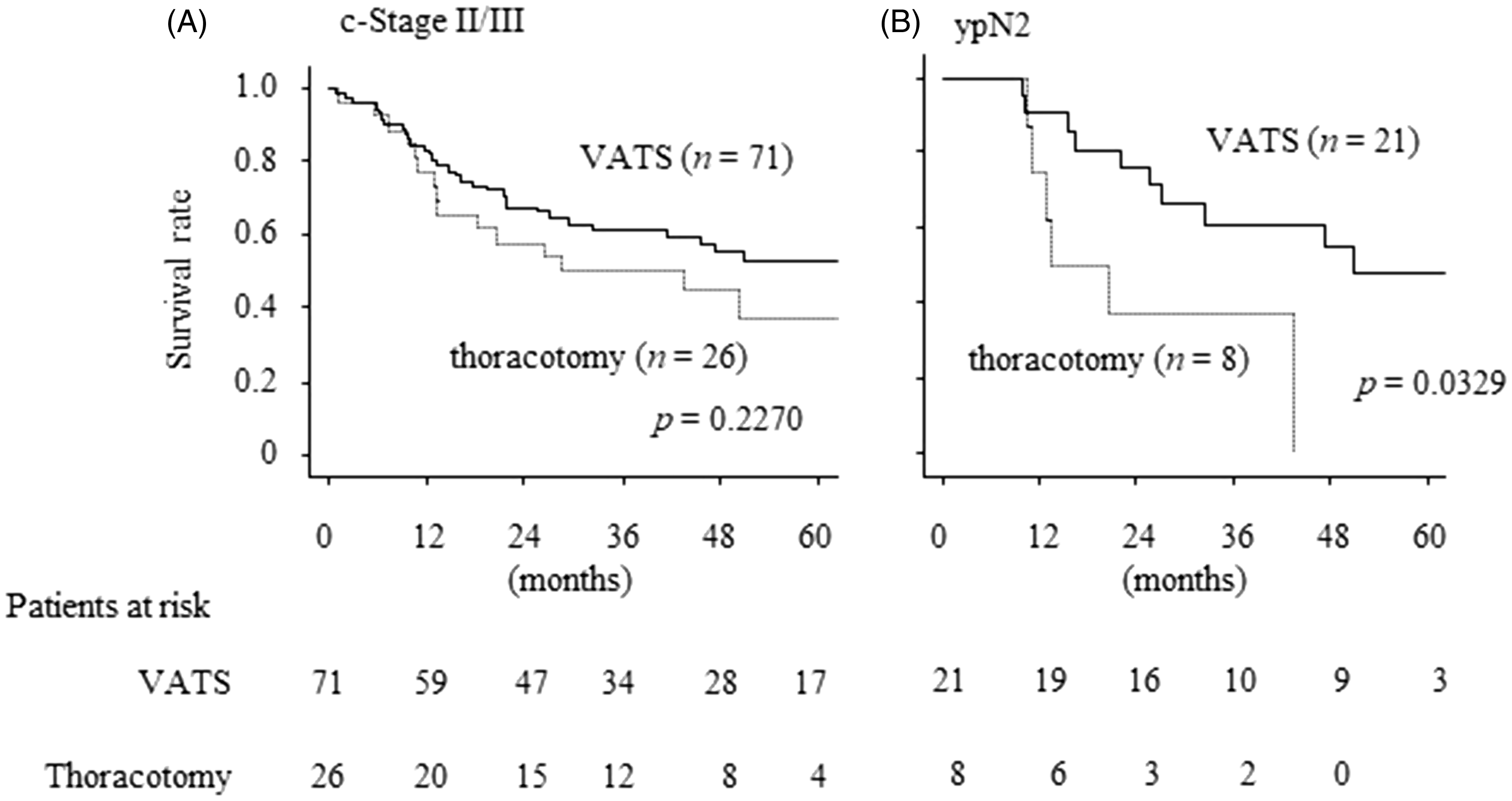
Survival curves of patients with clinical stage II or III and those with ypN2. VATS: video-assisted thoracoscopic surgery.
Discussion
Recently, it has been widely accepted that VATS offers advantages over thoracotomy in patients with early-stage NSCLC, including less postoperative pain, shorter hospitalization, less morbidity, and improved overall survival.9–12 Although VATS is commonly performed for the treatment of early-stage lung cancer, the use of thoracoscopic procedures for locally advanced NSCLC remains controversial, most likely due to concerns about safety, technical feasibility, and the likelihood of achieving complete oncologic resection.1,9,11,12 However, the increased use of VATS has shown that even advanced tumors can be safely resected with this approach.1,2,5,13,14 Although there are restrictions in the viewing angle and manipulation of forceps because of the need to perform surgery through small wounds, VATS has a local magnifying ability that is beneficial for identification of intraoperative vessels and bronchi, small bleeding spots, and bronchial fistulas, thereby reducing the occurrence of operation-related complications. Moreover, delicate delamination may be easier to perform than in a thoracotomy. These merits of VATS make it ideal for mediastinal lymph node dissection in cases of advanced lung cancer.
We found no significant difference in mortality and morbidity rates between the VATS group and the thoracotomy group. The incidence of grade ≥2 or ≥3 postoperative complications was 35.5% and 13.6%, respectively, which is similar to the rates in previous studies.2–4,6 It has already been reported that VATS is associated with fewer postoperative complications than thoracotomy in patients with early-stage lung cancer.9–12 In the present study, the incidence of grade ≥3 postoperative complications was lower in the VATS group, but not to a significant degree. Although VATS surgery after induction therapy has generally been regarded as technically difficult, the amount of intraoperative bleeding was smaller and the operative time was shorter in comparison with thoracotomy in this study. Among our 79 VATS cases, only 4 required conversion to thoracotomy. Considering that the frequency of CTCAE grade ≥3 postoperative complications was lower in the VATS group, it appears that VATS can be performed safely after induction therapy.
The outcome of lung cancer patients who underwent surgery after induction therapy in our hospital agrees with previous reports,2–4 although accurate evaluation was difficult due to differences in the clinical and pathological stages of the patients. We found no significant difference in recurrence rates or outcomes between the VATS and thoracotomy groups; however, local recurrence tended to be more frequent in the thoracotomy group, and distant metastasis tended to be more frequent in the VATS group. Because the thoracotomy group included many central lung cancers requiring combined resection of other organs such as the great vessels, the rate of local recurrence might have been higher than in the VATS group. Because the VATS group included many patients who underwent induction therapy due to N factor, and there were many N2 patients, the proportion of patients with distant metastasis appears to be high. For ypN2 cases, the VATS group had a significantly better outcome and better 5-year survival rate than the thoracotomy group. Although complete oncologic mediastinal lymph node dissection with VATS has been considered difficult, the low local recurrence rate and better prognosis in the VATS group suggests that N2 metastatic lymph nodes had been properly resected by VATS. VATS is therefore considered to be useful for patients with locally advanced lung cancer after induction therapy, especially those with peripheral lung cancer with hilar or mediastinal lymph node involvement.
This study had some limitations. First, because it was retrospective in design, a patient selection bias existed. There were differences in the patient population in the VATS and thoracotomy groups. For example, patients requiring angioplasty or carinal resection could only undergo a thoracotomy. A higher proportion of patients in the thoracotomy group had cT3/T4 tumors requiring combined resection. Therefore, it was impossible to directly compare the clinical results between the 2 groups. Second, clinical N status was diagnosed using CT and PET, and was not confirmed pathologically. Third, this study included all patients who had undergone induction therapy followed by resection, and although the majority received induction therapy for stage IIIA disease, it had been applied for a wide range of reasons including chest wall invasion and large tumors. Fourth, because we analyzed a small number of patients in a single institution, a further large-scale study will be necessary to investigate the role of VATS in the treatment of locally advanced lung cancer.
We concluded that among patients with lung cancer who underwent surgery after induction therapy in our hospital, there were no significant differences in the recurrence rate and prognosis between those treated by VATS and those who underwent a thoracotomy. The VATS group had a significantly less intraoperative blood loss, a shorter operative time, and a shorter postoperative hospitalization than the thoracotomy group. Although thoracoscopic surgery is not indicated for central lung cancers requiring angioplasty or carinal resection, it seems to be useful for patients with locally advanced lung cancer after induction therapy, especially those with peripheral lung cancer with mediastinal or hilar lymph node metastasis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.