
Abstract
Background
Few prognostic tools are currently available to predict hospital mortality in patients with acute type A aortic dissection. The aim of this study was to validate the performance of two existing risk-assessment tools, the original and the adjusted Leipzig-Halifax scorecards, to predict hospital mortality among Armenian patients with acute type A aortic dissection.
Methods
This retrospective cohort study included all consecutive patients with acute type A aortic dissection who were admitted to two tertiary cardiac centers in Armenia and underwent surgery from January 2008 to April 2018. We evaluated the predictive power of the original and adjusted Leipzig-Halifax scorecards using logistic regression analysis.
Results
Overall, 211 patients (76% males, mean age 57 ± 9 years) were included in the study, of whom 37 (17.5%) died during hospitalization. The adjusted Leipzig-Halifax score, but not the original Leipzig-Halifax score, was a significant predictor of hospital mortality. Patients with medium and high adjusted Leipzig-Halifax scores had a significantly higher odds of death compared to patients with low scores (odds ratio = 3.0 vs. 3.9, 95% confidence interval: 1.3–6.9 vs. 1.0–14.9, respectively). The areas under the receiver operating characteristic curves were 0.58 and 0.63, respectively, p > 0.05.
Conclusion
The adjusted Leipzig-Halifax score performed slightly better than the original Leipzig-Halifax score in the Armenian acute type A aortic dissection population. The adjusted Leipzig-Halifax score should now be applied prospectively to generate more data for further validation and potential improvement.
Keywords
Introduction
Acute type A aortic dissection (AAAD) is a life-threatening pathology of the aorta. Without surgery, the risk of mortality is 50% during the first 48 h and 80% during the first two weeks, increasing by 1%–2% per hour if untreated. 1 AAAD prevalence ranges from 0.2% to 0.8%, 2 and the incidence is 2.9 to 6.0/100,000 person-years.3–5 Risk factors for AAAD include systemic hypertension, 3 , 6 , 7 older age, male sex, smoking, 8 congenital heart defects such as bicuspid aortic valve and coarctation of the aorta, and genetic disorders such as Marfan syndrome. 6 , 9 According to data from the International Registry of Acute Aortic Dissection, the surgical mortality of AAAD has been decreasing over time, from 25.0% in 1996–1999 to 18.4% in 2010–2013. 6 , 10 Independent predictors of mortality in patients surgically treated for AAAD are preoperative shock, cardiac tamponade, preoperative malperfusion, and advanced age.11–13 Considering the high surgical risk, estimating the preoperative risk is crucial in selecting the optimal management strategy. Because AAAD is a relatively rare condition, few prognostic tools are currently available to predict operative mortality. The Penn classification is one tool, based on preoperative end-organ and/or generalized ischemia. 14 , 15 More recently, the Leipzig-Halifax (LH) scorecard was developed for the German and Canadian populations, and was further validated for the Swedish AAAD population. 16 , 17 Risk-adjustment scores need external validation when applied to patient populations potentially different from the population in the tool’s development cohort. In the case of Armenia, care must be taken when generalizing parameters derived from the experience in developed countries. External validation of risk-adjustment scores becomes more crucial to system development and quality improvement efforts. Only two tertiary centers in Armenia, Nork Marash Medical Center (NMMC) and Astghik Medical Center (AMC), perform AAAD surgery. Benchmarking Armenia’s AAAD surgical outcomes against other countries is important for quality assurance efforts and for further advancement of care. Accurate comparisons of outcomes between different centers can be achieved only by using validated risk-adjustment tools. This study sought to validate the existing risk-adjustment tools to predict operative mortality in patients with AAAD in Armenia.
Patients and methods
We conducted a retrospective cohort study that included all consecutive patients who were admitted to either NMMC or AMC, were diagnosed as acute cases (time from symptom onset to surgery <14 days), and underwent surgery from January 1, 2008 to April 1, 2018. We excluded patients with chronic dissections, traumatic dissections, or congenital heart diseases such as aortic coarctation.
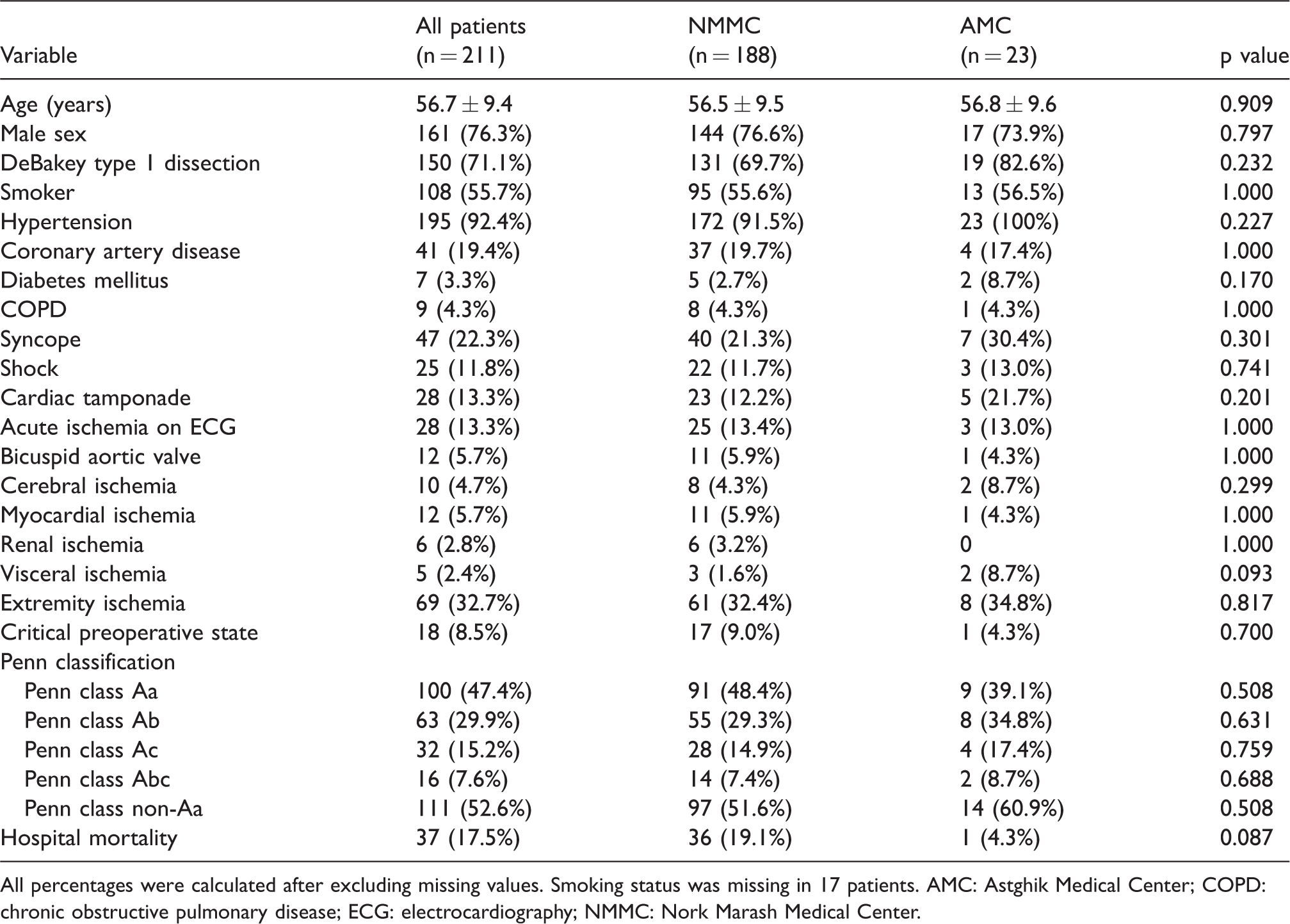
We used the NMMC and AMC computerized databases to identify patients for inclusion in the study. For those eligible, we retrieved their inpatient and outpatient medical records and extracted data into an anonymized structured database. Specifically, we extracted information on patients’ demographic characteristics, risk factors, comorbidities, operative characteristics, postoperative complications, and hospital mortality to calculate the predictive scores and assess outcomes. The Institutional Review Board of the American University of Armenia approved the study and granted a waiver of consent for the abstraction of anonymized medical records data. We identified 211 patients who underwent AAAD surgery during the study period. Of these, 188 were treated at NMMC and 23 at AMC. No differences were found in the patients’ baseline characteristics between the 2 centers (see Appendix 1), and we proceeded with pooled sample analysis.
We considered two risk prediction tools for validation in the Armenian AAAD population: the original LH scorecard developed for the German and Canadian populations, 16 and the adjusted LH scorecard validated for the Swedish population. 17 We calculated the original and adjusted LH scores following the definitions and instructions in the relevant published studies. 16 , 17 Figure 1 schematically depicts the original and adjusted score calculations.
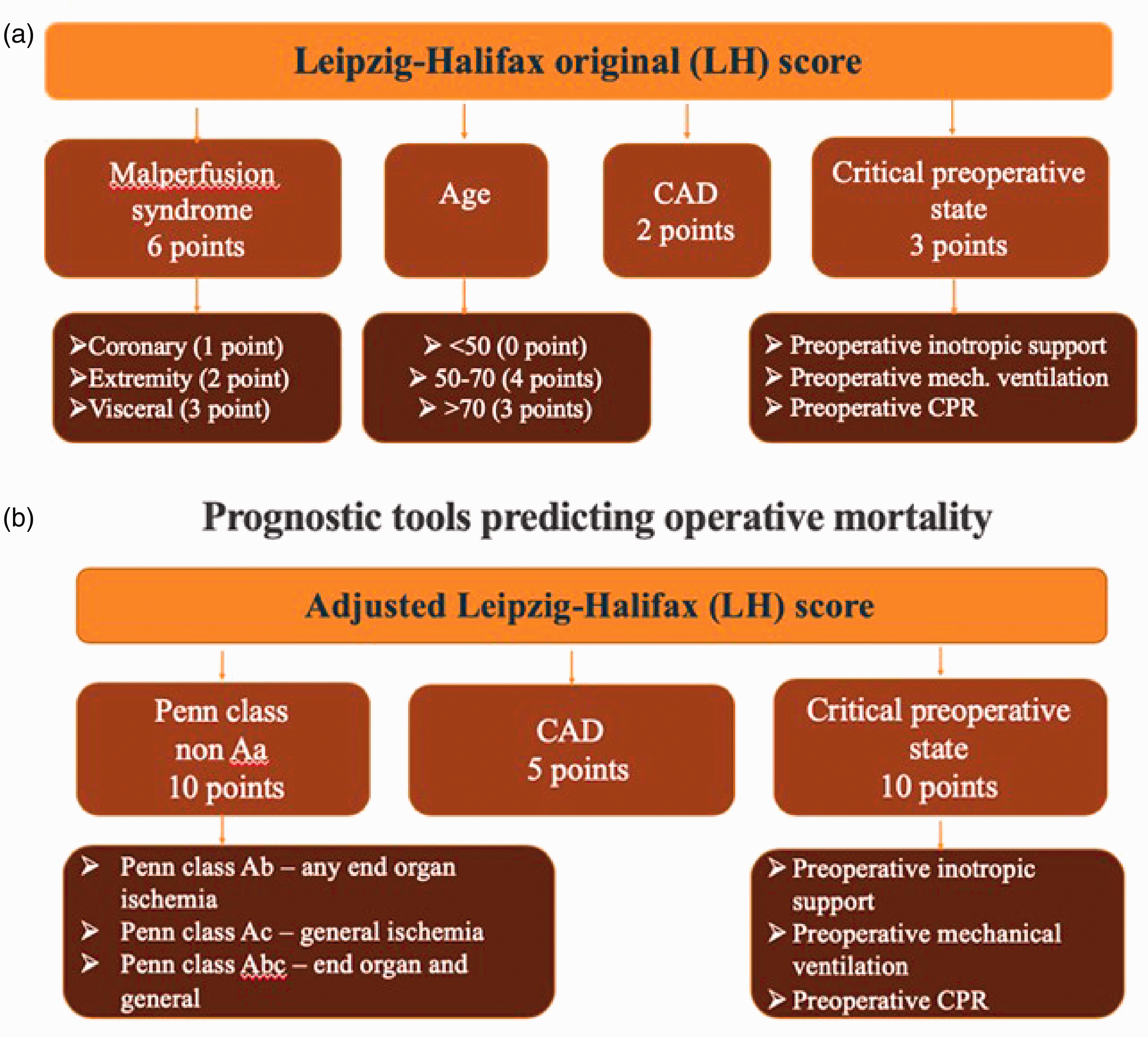
Schematic presentation of the prognostic score calculations using (a) the original and (b) the adjusted Leipzig-Halifax scorecards. CAD: coronary artery disease; CPR: cardiopulmonary resuscitation.
The original LH score is a composite score constructed by addition of the scores assigned to each of the following preoperative variables: age < 50 years (score = 0), 50–70 years (score = 4), > 70 years (score = 3); critical preoperative state (score = 3) defined as preoperative inotropic support and/or preoperative mechanical ventilation and/or preoperative cardiopulmonary resuscitation; malperfusion syndrome, particularly coronary (score = 1), extremity (score = 2), and visceral (score = 3); and coronary artery disease (CAD; score = 2). Based on the LH cumulative scores, each patient was classified into one of four risk groups: low (score = 0–3) with < 10% risk of hospital death, medium (score = 4–6) with a 10%–25% risk of hospital death, high (score = 7–10) with a 25%–50% risk of hospital death, and very high (score > 10) with > 50% risk of hospital death.
The adjusted LH score is also a composite score but it includes slightly different conditions: critical preoperative state (score = 10, see definition above); Penn class non-Aa ischemia (score = 10); and CAD (score = 5). The Penn classification stratifies patients into four classes based on ischemia type. 14 , 15 , 18 Penn class Aa patients have no ischemia. Penn class Ab patients have any type of end-organ ischemia: cerebral ischemia (stroke or transient ischemic attack on presentation before surgery), extremity ischemia (pain in extremities and/or loss of pulses and/or difference in arterial pressures in 4 extremities), renal ischemia (malperfusion identified by computed tomography), or visceral ischemia (abdominal tenderness and bowel paralyses or ischemia on computed tomography). 16 Penn class Ac includes patients with shock (a drastic drop in systolic blood pressure < 80 mm Hg), cardiac tamponade (acute accumulation of fluid in the pericardial space), and myocardial ischemia with ST-segment elevation > 0.1 mV on electrocardiography. 14 Penn class Abc includes patients with both end-organ and generalized ischemia. Penn class non-Aa is a composite class that includes Penn Ab, Ac, and Abc classes. The adjusted LH cumulative score ranges from 0 to 25 with 5-point increments. Based on the LH cumulative scores, each patient was classified into low (score < 10), medium (score = 10–15) or high (score > 15) hospital mortality risk groups. 17
Continuous variables are reported as means and standard deviations, and categorical variables as frequencies and proportions. For comparison purposes, we have reported the baseline characteristics of the Armenian population along with those of the cohorts that were used to develop the original and adjusted LH scores. 16 , 17 Next, we have reported the observed mortality rates by LH score categories. Finally, we tested the effect of the individual components and composite scores on hospital mortality using univariable logistic regression analysis. To check the diagnostic accuracy of the composite scores, we measured the area under the receiver operating characteristic curve. 19
Results
Table 1 lists the baseline characteristics of our 211 patients alongside those of the patients in the original and adjusted LH score development cohorts. Some of the notable differences in baseline characteristics include a higher prevalence of current smokers, hypertension, and moderate to severe aortic regurgitation in the Armenian population compared to the other cohorts. Additional operative and postoperative characteristics are summarized in Appendix 2. Hospital complications are summarized in Appendix 3. Table 2 lists the distribution of LH scores in patients who were discharged alive and those who died during the index admission. Of the 211 patients, 37 (17.5%) died during hospitalization, 11 (31.4%) of whom met the original LH high-risk criteria, and 4 (28.6%) met the adjusted LH high-risk criteria. No patient met the original LH very high-risk criteria. Univariable regression analyses of individual components of the original LH scorecard showed that cerebral ischemia was a significant predictor of hospital mortality while extremity ischemia demonstrated borderline significance in the Armenian population (Table 3). Among the adjusted LH scorecard components, Penn class non-Aa was the only significant predictor of hospital mortality. Neither CAD, age, nor critical preoperative state were associated with hospital death. The composite adjusted LH score (but not the original LH score) was a significant predictor of hospital mortality in Armenia. Patients in the medium and high adjusted LH score categories had significantly higher odds of mortality compared to those in the low score category (Table 3). The model with the adjusted LH scorecard showed slightly better discrimination than the model with the original LH scorecard (area under the receiver operating characteristic curve: 0.63 vs. 0.58, respectively, p = 0.363; Figure 2).
Patient baseline characteristics at presentation.
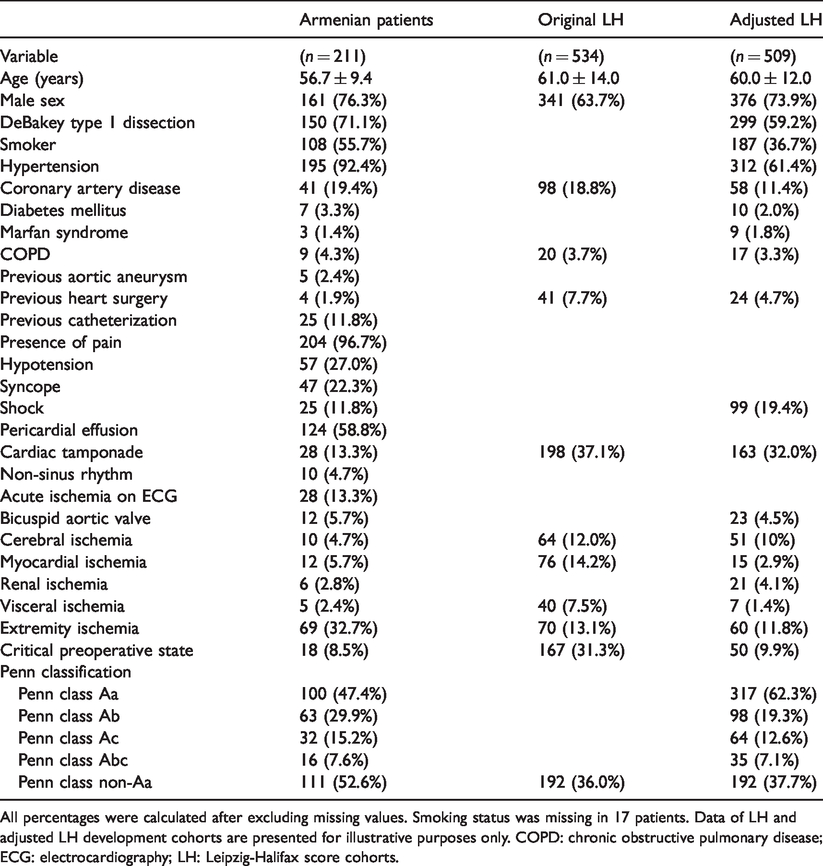
All percentages were calculated after excluding missing values. Smoking status was missing in 17 patients. Data of LH and adjusted LH development cohorts are presented for illustrative purposes only. COPD: chronic obstructive pulmonary disease; ECG: electrocardiography; LH: Leipzig-Halifax score cohorts.
Hospital mortality rates in Armenian patients and cohorts used for development of the original and adjusted Leipzig-Halifax scores.
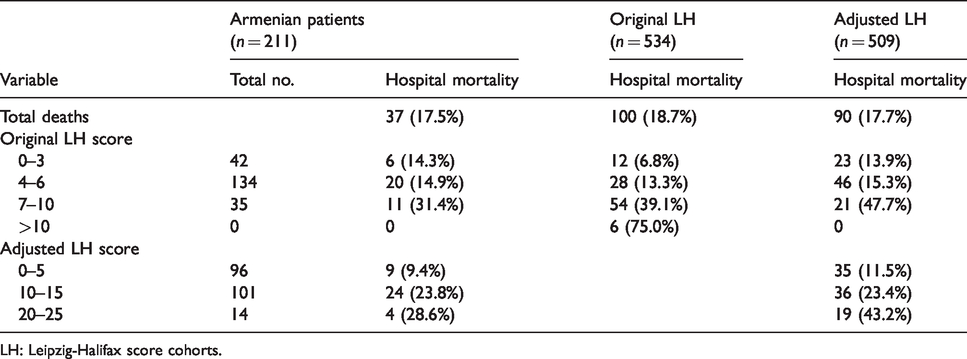
LH: Leipzig-Halifax score cohorts.
Prediction of hospital mortality by original and adjusted Leipzig-Halifax scores.
CI: confidence interval; LH: Leipzig-Halifax; OR: odds ratio.
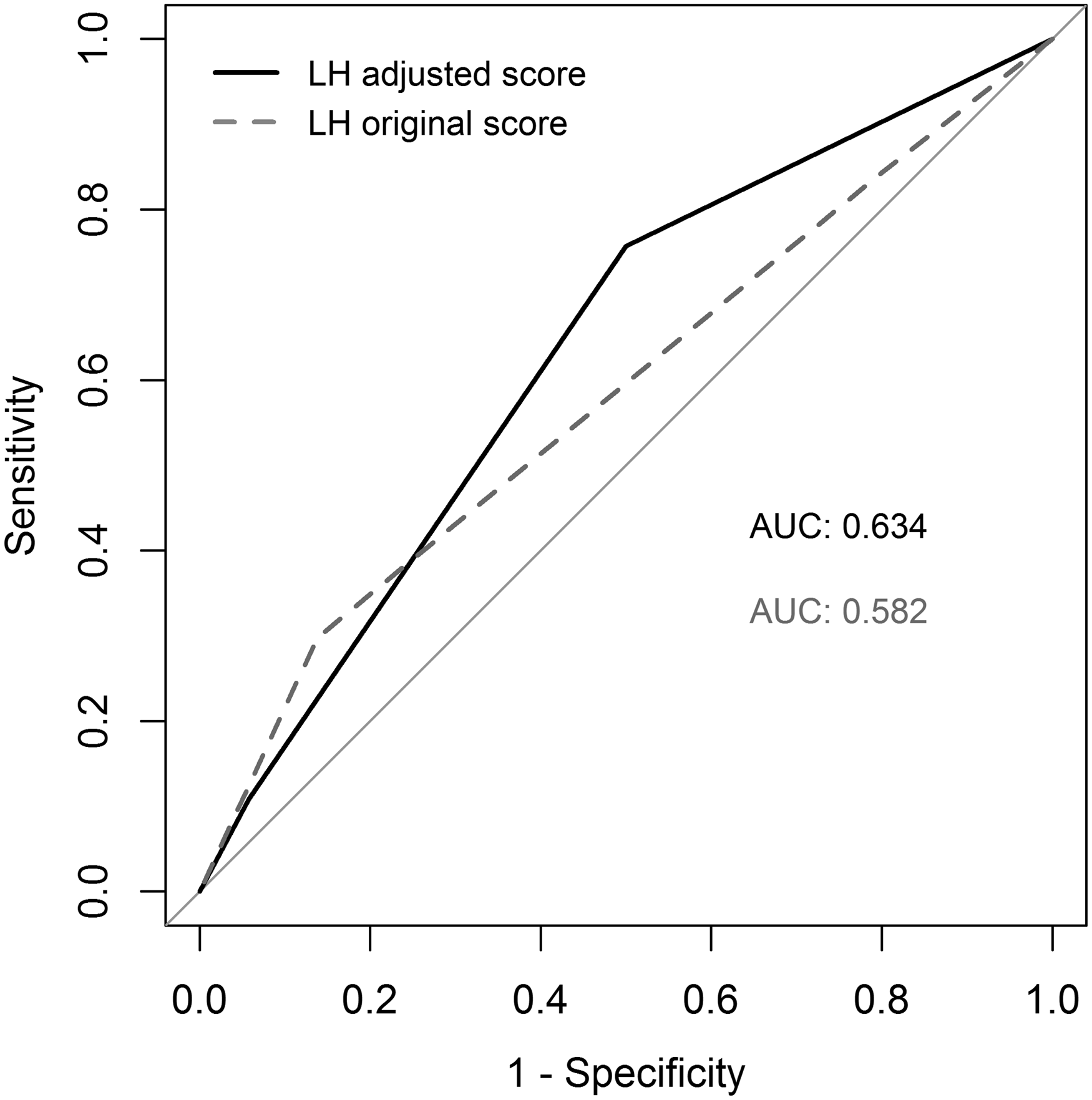
Receiver operating characteristic curve of the Leipzig-Halifax (LH) original and adjusted scores. AUC: area under the curve.
Discussion
In this study, we validated the performance of two existing risk assessment tools, the original and the adjusted LH scorecards, in predicting hospital mortality in the Armenian population with AAAD. The hospital mortality rate was 17.5% in our cohort of surgical patients, with greater rates observed in patients with higher LH scores. The composite adjusted LH score (but not the original LH score) was a significant predictor of hospital mortality in Armenia. The adjusted LH scorecard had slightly better discrimination than the original LH scorecard.
We observed notable differences between the characteristics of our Armenian patients and the patient cohorts involved in developing the LH scorecards. The prevalence of current smokers, for example, was higher in Armenian patients compared to Swedish patients (55.7% vs. 36.7%), 17 indicating also that the chronic obstructive pulmonary disease prevalence was likely underreported in Armenia (4.3%). Higher smoking rates may explain the higher rate of concomitant coronary artery bypass procedures performed in our cohort (20% of cases) compared to the Swedish cohort (7%). The rates of CAD were comparable between the Armenian and Canadian/German populations (19.4% and 18.8% respectively), 16 but differed from that in Swedish patients (11.4%). 17 The rate of hypertension was also very high (92.4%) in Armenian patients compared to the Swedish (adjusted LH) patients (61.4%). Compared to the original and adjusted LH development cohorts, the percentage of extremity ischemia was quite high in our cohort (32.7%). It is likely that cerebral ischemia was underreported in our sample, and we counted only those with an apparent neurological deficit who carry a higher risk of mortality. Therefore, these patients had a higher odds of mortality than those without a diagnosis of cerebral ischemia. Of note, the confidence interval of the odds ratio was wide due to the low frequency of this event in our sample population.
The percentage of patients presenting in a critical preoperative state (8.5%) was similar to that of the adjusted LH cohort (9.9%), 17 but much lower than in the original LH cohort (31.3%). 16 This variability could be attributable to accessibility because only relatively healthy patients reach the Armenian clinics, both of which are located in the capital city and are the only clinics in the country treating these patients. This factor might also explain why the Armenian cohort was 4 years younger than the two compared cohorts.
The hospital mortality rate in our cohort (17.5%) was comparable to the German/Canadian (18.7%) 16 and Swedish (17.7%) 17 mortality rates. The International Registry of Acute Aortic Dissection reported a slightly higher surgical mortality rate (25.0%) in the 1996–1999 cohort, which decreased to 18.4% in the 2010–2013 cohort. 6 The latter reflected data from 28 referral centers and 2952 patients. Similar to the original and adjusted LH development cohorts, mortality rates in Armenian patients increased with increasing LH scores. When comparing the original LH score categories in patients who died in all three cohorts, the distribution of scores in the Armenian population was closer to that of the Swedish cohort. 17 Of note, the proportion of patients in the higher score groups (i.e., sicker patients) was lower in the Armenian cohort than in the two compared cohorts. This finding could be explained by differences in the performance of the scores or it may reflect the fact that only the healthier patients in Armenia reach a hospital. We believe that the availability of emergency transportation plays an important role in AAAD outcomes. Unfortunately, it is difficult to retrospectively compare the delivery of this and other healthcare services between countries. In Armenia, patients living in regions far from the capital might be transported late or might die during transportation, creating a study sample more biased toward healthier patients. Late referral of patients, rather than late emergency transportation, could be another factor contributing to a biased selection. The latter could be associated with provider or patient-related factors (e.g., socioeconomic, educational, cultural). Differences in patient profiles, healthcare services, and practices between countries further emphasize the need for an external validation of risk-adjustment models before adopting them for local practice.
In univariable analysis, neither age, CAD, nor critical perioperative state were significant predictors of hospital mortality in Armenian patients, thus explaining the poor prognostic power (0.58) of the original LH score. As noted, Armenian patients were on average 4 years younger than patients in the original LH developmental cohort (56.7 ± 9.4 vs. 61.0 ± 14.0 years). Similarly, AAAD patients enrolled in the International Registry of Acute Aortic Dissection were older (61.5 ± 14.6 years). 6 Life expectancy in Armenia is 75 years (the median age of the population is 35.6 years), compared to Germany’s 81 years (median age 45.9 years) and Canada’s 82 years (median age 42.6 years). 20 Thus, the age difference could be explained by the differences in life expectancy (relative age) and not necessarily a bias in selection for treatment. Older patients generally have a higher comorbidity burden. In our cohort, only 2.4% presented with visceral ischemia compared to 7.5% in the original LH cohort. 16
Of the predictors in the adjusted LH score, only Penn non-Aa class was a significant predictor of hospital mortality. Individual components of Penn non-Aa class, such as cerebral ischemia, cardiac tamponade, and shock, were also significantly associated with hospital mortality. Consequently, the adjusted LH score showed better discrimination than the original LH score. Most importantly, the area under the receiver operating characteristic curve for the adjusted LH score in the Armenian population (0.63) mirrored that of the adjusted (Swedish) LH score cohort (0.66). 17
As risk prediction tools, the LH scores include only preoperative factors. Studies have reported operative factors such as longer cardiopulmonary bypass time and deep hypothermic circulatory arrest time as risk factors for hospital mortality after AAAD surgery. 18 The mean cardiopulmonary bypass time was longer in our population (245.5 ± 111.5 min) compared to the original LH and adjusted LH populations (202.0 ± 77.0 and 198.0 ± 69.0 min, respectively). The mean deep hypothermic circulatory arrest time was 42.6 ± 27.1 min compared to the Canada/German and Swedish populations (20.0 ± 17.0 and 34.0 ± 20.0 min, respectively). 16 , 17 These differences might have influenced hospital mortality in our Armenian study population.
The following study limitations warrant further discussion. This retrospective study used chart abstraction with the inherent risk of misinterpretation or underreporting of some of the variables (e.g., chronic obstructive pulmonary disease, renal ischemia, visceral ischemia). In addition, the medical records of 23 patients were not available. For these cases, we collected data from the outpatient discharge documents and electronic databases that had missing values for some of the variables (e.g., smoking status, operation time, and ventilation time). However, our study is representative and was limited to the Armenian population, and we included all patients who had undergone AAAD surgery in Armenia during the study period.
Because AAAD is relatively rare, it is logistically difficult to develop a risk prediction tool specific for each country. Therefore, an external validation of existing tools is the most efficient approach. Our next step will be the prospective application and evaluation of the adjusted LH score in our Armenian population with the potential to revise it and consider including additional factors for optimal performance in this population as more data accumulate over time.
We concluded that the hospital mortality rate after AAAD surgery remains high. Although both the original and adjusted LH scores had a poor discriminatory power, the adjusted LH score performed marginally better in the Armenian population. The adjusted LH score should now be applied prospectively to generate more data for further validation and further improve and refine the model while ensuring it allows comparison of Armenian hospital outcomes against international benchmarks.
Patient baseline characteristics at two centers.

All percentages were calculated after excluding missing values. Smoking status was missing in 17 patients. AMC: Astghik Medical Center; COPD: chronic obstructive pulmonary disease; ECG: electrocardiography; NMMC: Nork Marash Medical Center.
Operative and postoperative characteristics.
All percentages were calculated after excluding missing values. Operation time was missing in 3 patients, minimal temperature in 5, ventilation time in 19 (6 patients died intraoperatively), and intensive care unit stay in 9. CABG: coronary artery bypass grafting; CPB: cardiopulmonary bypass; DHCA: deep hypothermic circulatory arrest; LH: LH: Leipzig-Halifax.
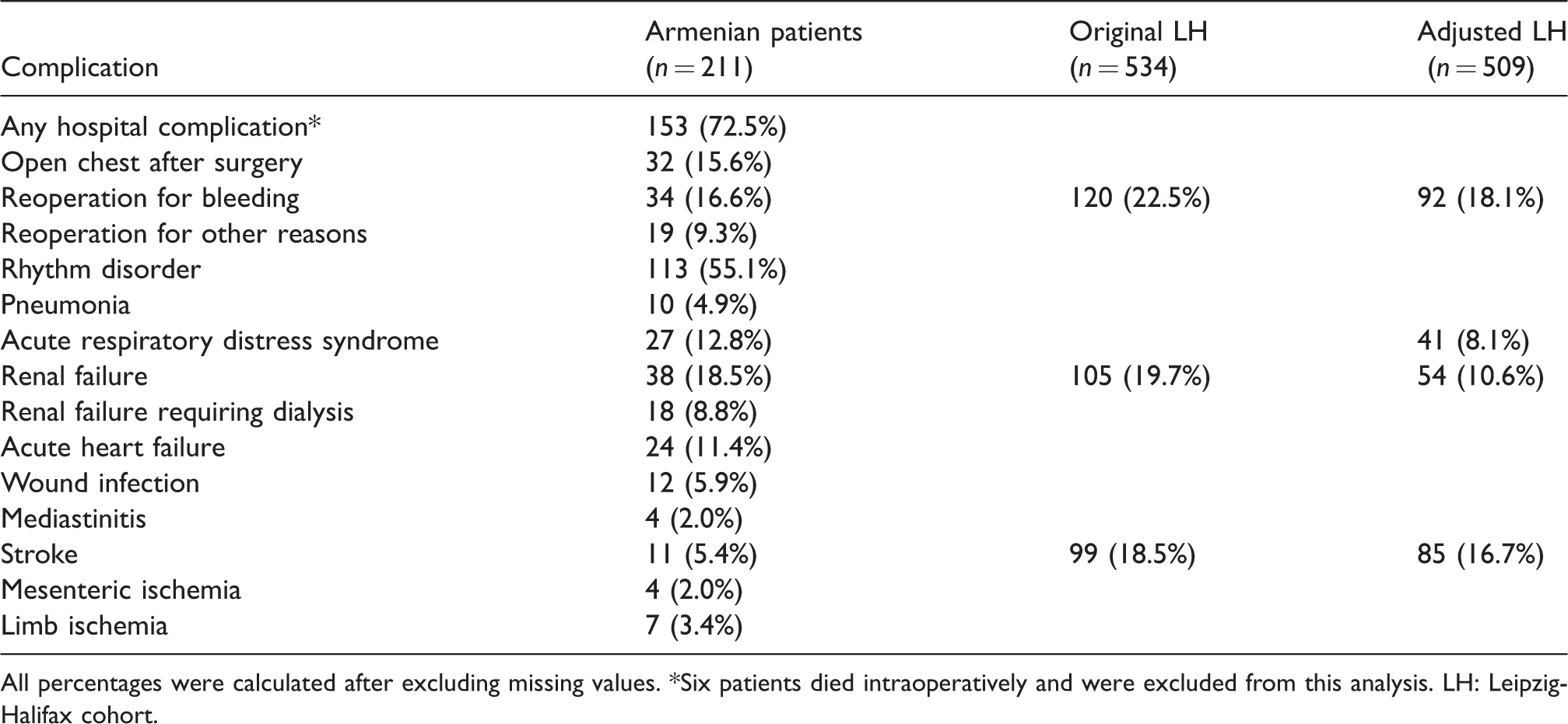
Hospital complications.
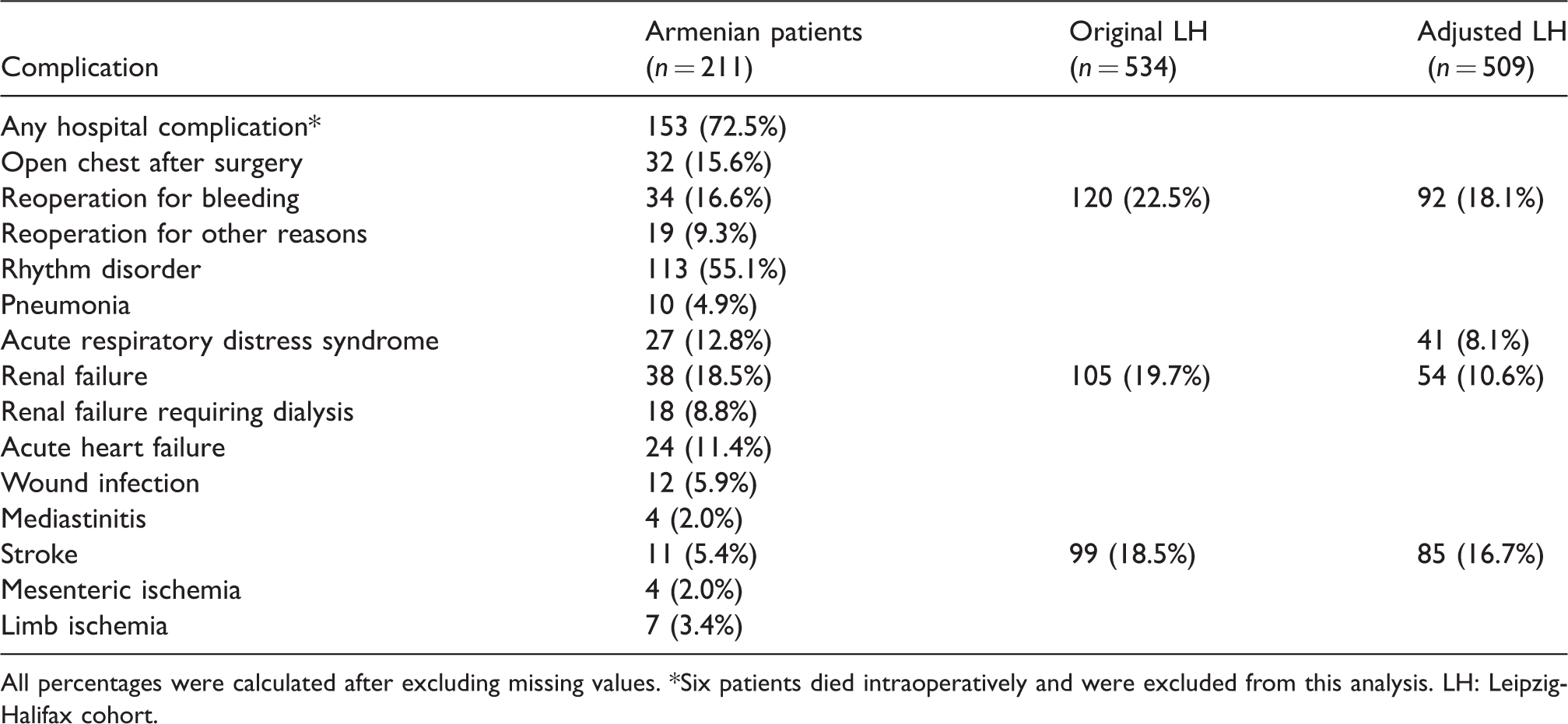
All percentages were calculated after excluding missing values. *Six patients died intraoperatively and were excluded from this analysis. LH: Leipzig-Halifax cohort.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.