
Abstract
A large number of children around the world are currently living in residential children’s homes and a central figure in those settings is the caregiver. The relationship children establish with their temporary caregivers can be a crucial factor in their lives. However, little research has been conducted with caregivers working in institutional settings regarding their experience and the relationship they establish with the children they care for. This article presents the results of a qualitative study conducted with 43 caregivers working in eight different residential children’s homes in Chile. The information was gathered through focus groups, and thematic analysis was conducted. The results show that caregivers report their experience of work and their relationship with children very positively and that this is characterized by their emotional involvement with children. This perspective appears to differ from that observed in large institutions in Europe, where there is some evidence that a more impersonal approach is predominant. However, it is acknowledged that this is based on caregiver perceptions which may or may not reflect cultural variations. The conclusion highlights the potential positive impact that caregivers can have on children’s lives, alongside some factors that negatively affect caregivers’ work, which could inform policy and procedures in order to provide better care for these children who (for various reasons) remain in residential care rather than family-based care.
Keywords
A large number of children live in residential children’s homes of varied characteristics and sizes around the world. Over several decades, a large body of research has highlighted the effects of being raised in large institutions with a model of caregiving characterized by its impersonal approach and focus on physical care (see Hamilton-Giachritsis & Garcia Quiroga, 2014). As a result of these findings, international recommendations (United Nations, 2009) have prioritized placement in foster care, especially for children under three, and in many countries, institutions have been closed or changed into smaller and more family-like homes.
However, in many countries, the implementation of foster care has been difficult, failing to effectively provide protection and better care for children (Maluccio, Canali, & Vechiato, 2006; Mapp, 2011; UNICEF, 2010). Many children live in residential children’s homes, and this situation is likely to continue for some time. Thus, there is an urgent need to study factors that can improve the conditions these children experience (McCall, 2013), in order to provide them with the care they need and protect their rights.
A central element in residential children’s homes is the caregiver—the person who spends most time with the children and plays an important role in their daily life. Potentially, caregivers can become positive, significant figures in children’s lives, providing stability, love and support, and a secure base from which children can develop (Garcia Quiroga & Hamilton-Giachritsis, 2015). Studies in attachment have shown that even after very difficult early years, having one significant adult providing unconditional love and responsivity can make a significant, positive change in child’s development (Lecannelier, Silva, Hoffmann, Melo, & Morales, 2014; McCall et al., 2010; The St. Petersburg-USA Orphanage Research Team, 2008).
Although the importance of caregivers as potential significant figures is clear, little research has been conducted to identify caregiver factors that can be linked to better outcomes for children. Exceptions to this are the recent study conducted in Latin American orphanages to explore the relationship between child–caregiver interactions and outcomes for children (Groark, McCall, McCarthy, Eichner, & Gee, 2013) and the study about infant and caregiver characteristics associated with secure attachment in institutions (Bakermans-Kranenburg et al., 2011). Research has shown that caregivers working in big orphanages have high levels of stress, anxiety, depression, and job dissatisfaction, but this finding does not hold true for those working in smaller homes (Heron & Chakrabarti, 2002). One possibility for this difference may be that in smaller homes, there is a chance to establish affectional bonds with children and have a rewarding experience, but this has not been studied.
Similarly, little research has been conducted to study the impact of intervention programs with caregivers. In one of the few studies of its kind, The St. Petersburg-USA Orphanage Research Team (2008) designed an intervention considering structural changes (e.g., reduction of child–caregiver ratios, assigning primary caregivers and formation of stable “family-like” groups) and specific training for caregivers with an emphasis on achieving an emotional bond with the children. The results showed important changes both in children’s outcomes and caregivers’ perceptions for the group that received both training and structural changes compared with (a) the group receiving training only and (b) the control group. Similar results were found in a recent study conducted in Nepal (Wright, Lamsal, Ksetree, Sharma, & Jaffe, 2014).
In Chile, an important debate has taken place concerning the quality of care for children in need. Foster care has been implemented, with numerous difficulties, and new quality standards for institutional setting have been established (Garcia Quiroga & Hamilton-Giachritsis, 2014). A recent study reported a positive impact of a pilot intervention program with caregivers working in an infant home (Lecannelier et al., 2014). However, little research has considered caregivers’ experiences and perceptions in the relationship they establish with children under their care. Given that all these factors play a significant role in the quality of care provided, it is vital to study caregivers’ experiences in order to design future intervention programs. Therefore, this study seeks to explore caregivers’ experiences in the relationship they establish with children in the context of residential children’s homes in Chile. The main focus of the study is caregivers’ views and experiences about their relationship with the children, the way they perceive their work, and the perspectives they have about the care system in which they work.
Methods
This project was approved by the University of Birmingham (UK) Ethics Committee (ERN_13-0830) and by the local body of each institution in Chile, to ensure the protection of participants. Participation was voluntary and consent forms were signed by all participants. All data were anonymized and all recordings were destroyed after the transcription.
Participants
In total, 43 caregivers working in eight different residential children’s homes participated in this study (see Table 1 for a description of characteristics of residential homes included in the study). All caregivers were females, with a mean age of 41.3 years old (range 21–59).
Characteristics of residential homes.
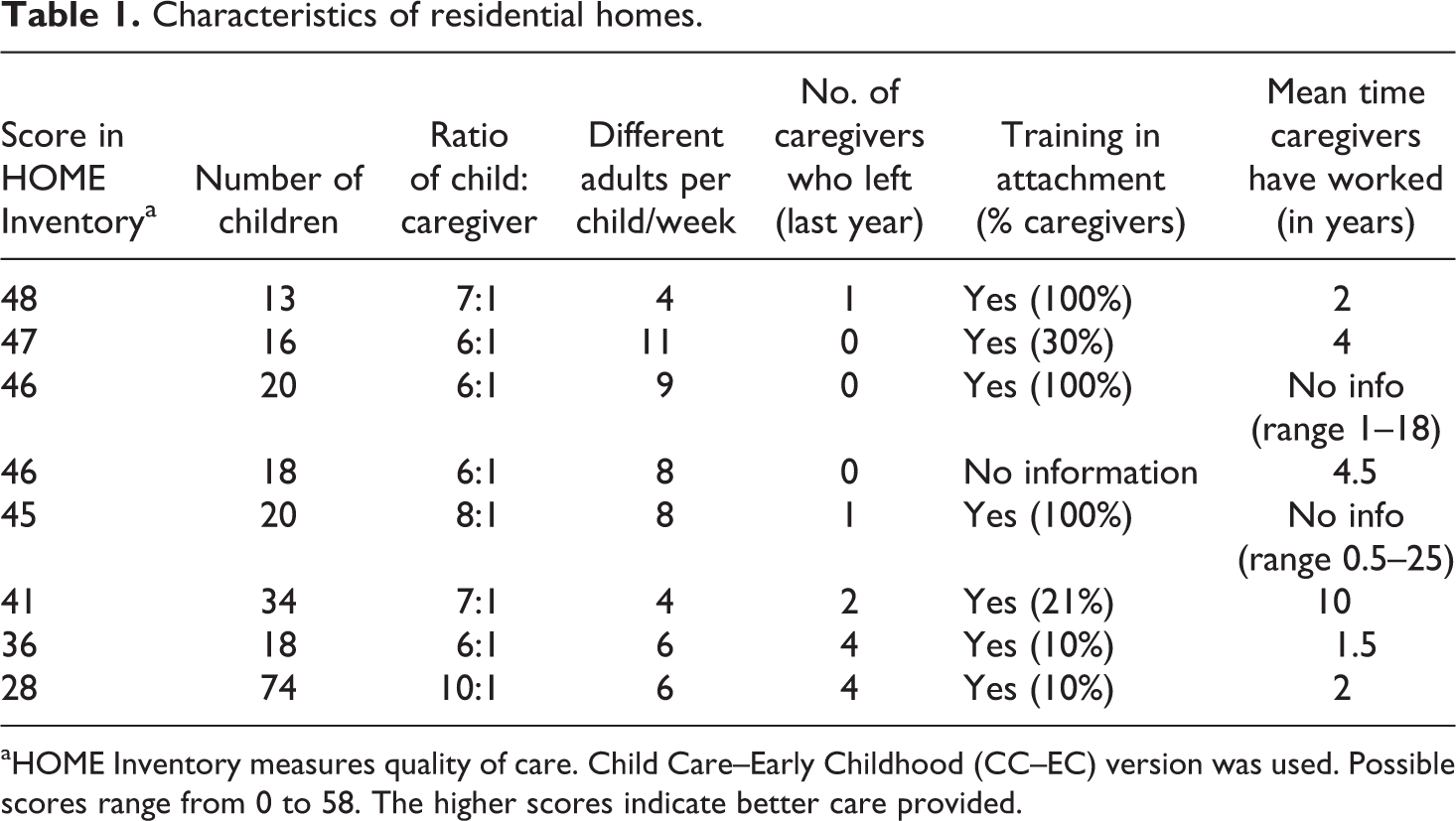
aHOME Inventory measures quality of care. Child Care–Early Childhood (CC–EC) version was used. Possible scores range from 0 to 58. The higher scores indicate better care provided.
The mean time caregivers had been working in their institution was 7.4 years (median = 5.5, range of 0–27 years), and they had been working as caregivers in any residential home for a slightly longer period (M = 9.3 years, median = 7.0, range 0–32 years). The vast majority of participants did not have any specialized professional training in education or childcare. Characteristics of this sample of residential homes are representative of the general characteristics in the regions of the country included in the study regarding, number of children, caregiver ratios, staff turnover, and level of training, with the only exclusion (due to voluntary participation) of a few bigger and older institutions that still exist in the country (Garcia Quiroga & Hamilton-Giachritsis, 2014).
Procedures
This study is part of a wider research project on attachment in alternative care conducted with a sample of 17 residential children’s homes (457 children in total). The 17 homes were all situated in the two main regions of Chile that have the largest number of children’s homes. For this part of the study, which focused on caregivers’ experiences and views, all caregivers working with children from 3 to 7 years old were invited to take part (as this was the inclusion criteria for the wider project). From a total of 74 caregivers invited, 43 (58.1%) agreed to participate. An invitation letter was sent to the managers via e-mail and further details were agreed with those willing to participate during a meeting in which all the details about the study, confidentiality of the data, consent forms, and information sheets were provided.
In order to gather multiple views and emotional experiences of the participants, focus groups were conducted with a duration time of approximately 1.5 hr each. This method facilitates the gathering of a large amount of data in a short period of time (Gibbs, 1997), which was considered important for practical reasons as well as minimizing disruption to the normal functioning of the children’s homes. To enable full attention from the interviewer to all participants, focus groups were video recorded and no notes were taken.
Focus groups were conducted in the caregivers’ language (Spanish) and followed a semi-structured format with three general open questions: “Let’s talk about your experience as caregivers,” “How have you experienced your relationships with the children?,” and “If you could change something, what would you choose to change?” Following that, vignettes were used to prompt discussion regarding attachment-related issues. The vignettes briefly presented three situations: one related to the convenience of the caregiver getting emotionally involved and the impact this would have in children, a second one describing a child with indiscriminate friendliness behaviors and asking caregivers to explain these behaviors, and the one last describing a child with signs of an avoidant attachment style and asking caregivers to express their thoughts about the child’s behaviors. This technique allows the discussion of sensitive topics in a less threatening way and the exploration of beliefs and perceptions of an action in context (Barter & Renold, 1999).
In addition to the focus groups, an observation was conducted in all homes and quality of care was assessed using the Home Observation for Measurement of the Environment (HOME) Inventory, Child Care–Early Childhood version (Caldwell & Bradley, 1984). This measure provides a general score (higher scores indicate better quality of care) and subscales with scores for specific components of care.
Data analysis
After conducting the focus group, the researcher did an exact transcription of the video recording. Files were then imported to Nvivo10 qualitative software.
Thematic analysis was conducted to identify main themes and recurrent patterns in the data. This method was chosen due to its flexibility, freedom from specific theoretical framework, ability to explore a rich and detailed set of data, and enable the identification and analysis of repeated themes (Braun & Clarke, 2006). The analysis was content driven (bottom-up approach), with an interest in reflecting the participants’ perspective without imposing preconceived theoretical limits (Quest, MacQueen, & Namey, 2012). The first author transcribed, translated into English, and analyzed each focus group. All the groups were coded and each excerpt was allocated to one or more nodes, giving the same importance to all the transcribed data. At this phase, the second author, an experienced researcher in the field of institutional care, verified the themes to promote reliability of the analysis, checking sections of the texts and codes. On the few occasions where there were different opinions, codes were discussed and consensus regarding themes and subthemes was achieved. Once all transcripts were coded, they were all rereviewed through an iterative process to ensure no codes present in the last transcripts were missing on the transcripts that had been coded first.
A set of approximately 145 codes was established, and the analysis of themes and superordinate themes was then conducted. If very similar contents were revealed, codes were condensed. Tree nodes and analysis of frequencies were then conducted in order to identify the repeated patterns and only codes that had at least 15 individual references or were present in five or more focus groups were considered for the analysis. These were established as criteria to represent themes that were present in the majority of the focus groups (i.e., revealing themes present across different institutions) or themes of a majority of caregivers in one or more groups (i.e., to allow the expression of particular views across different residential children’s homes). The cutoff point was established at 15 references because codes either appeared to have more than 15 references or many fewer references (e.g., 1 to 5). This process was discussed with the second author at several stages in order to ensure a better reflection of the data in the final themes.
Results
Four main overarching themes were collected from the focus groups: negative first impression/fear, emotional involvement, positive experience, and difficulties.
Negative first impression/fear
Usually, the first experience of working as a caregiver was a difficult one. Many caregivers reported an initial impression of being in a difficult environment and having very few tools for managing children (combined with little training). They also expressed some stereotypes they had about children living in homes and concerns about the conditions of their care. This was mentioned as their first experience by a vast majority of carers, regardless of whether they started working recently or had been there for many years. For example, “I thought a lot about it, I was scared, I had no experience working with children” (Focus Group (FG) 3/Participant (P) 1); “When I first came to work here at this home, I had a concept of residential children’s homes as bad” (FG12/P3);“My first impression was that I wouldn’t come back to work again … I felt very sad for the children because I said ‘this is like a children’s prison [20 years ago]’” (FG16/P1); and “I did not know what the work was like and the girls were very complicated. So the first time at work, I got scared, I began to cry from helplessness” (FG12/P1).
Emotional involvement
Following the initially negative impression, caregivers described a change to a more positive experience once they started to get emotionally involved with children, such as “And then when the children say ‘I love you’ that is so rewarding! One forgets the tantrums, everything” (FG3/P1). Other quotes include: And at the beginning I daily thought “when is he [child] giving me a hug? Or a kiss?” Until I achieved it! And seeing these things [children expressing love for them], feels good, it is very satisfying. (FG12/P1) But then, after, that started to calm down when we started to know each other, to know the problems that each of them had, their character … One gets to know the children and they get to know you … so you start a relationship with them. (FG3/P4)
As a part of overarching theme of “emotional involvement”, there were three identified subthemes: affectional bond, like a second home (24/7), and loss. These are presented below.
Affectional bond
Caregivers’ narratives included many comments about the affectional relationship they establish with children, rather than merely the practical tasks of feeding, cleaning, and educating children. Caregivers described this as a natural process that occurs even if they do not want it to—by virtue of engaging with the children, an emotional bond is formed—and described the generation of an affectional bond as a central part of their experience. Notably, this was mentioned in all the focus groups in all the homes. Indeed, some also commented that this was necessary to do the job well; for example, “I become very attached to the children, I like being with them. Even though you are not wanting to get attached, you do” (FG16/P1), “Yes, it is not difficult to engage with them, I mean, if one does not engage, then you are just not good for this” (FG12/P3), and “You have a bond, there is affect, there is love” (FG7/P2).
The affectional bond theme had several components, including engagement, differential bond, empathy, giving love, and thoughts about attachment.
Engagement
Complementarily with caregivers expressing them having an affectional bond with the child, caregivers described children also emotionally engaging with them. They reported that the children miss them and express love for them in different ways, which generates a sense of mutual reward. Caregivers say they feel loved by the children and they feel they receive even more than what they give. They feel children can recognize them as someone special and important, and that this is a rewarding experience. Participants said, “Small children recognize our voice, especially the babies, they turn their faces to look at us when we arrive and speak in the doorway of their room” (FG7/P7). We receive much unconditional love from them, when they call us “mummy”… or when you come back from holidays and [they say] “you are back!” (with open arms) and hence it makes you feel that the embrace they give us is unconditional love and they get attached to us. (FG16/P1)
Differential bonds
However, the affectional bond was noted to be characterized as different with each child. Differential bonds were mentioned in almost all focus groups (with the exception of the one with a lower HOME score). Caregivers described how they tend to have a special bond with some children more than with others and that this generates natural dyads between caregivers and children. In most of the homes, there was no key person system, so this was seen as a natural process based on the individual characteristics of both child and caregiver. This was linked to the experience of knowing each child with his/her individual characteristics, “With some of them we form something special, a closeness more than with others” (FG7/P5); “We recognize the way each of them cry. [A child is heard crying at that moment in the residential home]. Listen! That is E. crying. This is fantastic, it’s a magic” (FG2/P7). Another participant said: All of them stand out for something and it’s typical that the one you like sees you and greets you and pulls his arms and hands towards you and you too and it’s mutual, you always have one that without you meaning it to happen, touches your heart more. (FG7/P7) We are one and if there is one child or 10 children, for us the 10 children are important so if you get involved only with one … they realize that, so then it’s a bit cruel to the rest. (FG8/P1) And sometimes it’s bad because there are some children who do not get any. Especially those who behave badly and it becomes worse because they continue behaving badly because they don’t have a special caregiver. So we try to make sure that our favoritism to one child isn’t noticed much by the others. (FG16/P1)
Empathy
A key component of establishing affectional bonds was empathy, caregivers put themselves in the place of the children and described feeling touched by their experiences, which in some occasions was described as emotionally painful. These feelings led them to protect and take care of the children and their emotional well-being: “It was very difficult to see that—being so small, they are so abandoned—and one becomes part of them and at first it was hard for me because I suffered” (FG8/P1); “When I started to build the relationship with the kids I tried to put myself in their place, to have their perspective … if I am not empathic with the child, the child will never feel confident with me” (FG15/P1); and “I began to suffer with the pain of each of the children, of every experience they had and I began to feel dismay” (FG7/P2).
To give love
One sign of the affectional bond was the expressed wish to give love; this was reported as a main role, both from a theoretical point of view (what should they do) and from their practical experience. Caregivers described different expressions of love, characterized by physical proximity, pampering, and cuddling children: “At night, a kiss to each one and they even climb up above me but I give them all the same affection” (FG8/P11) and “One gives love to all, I’m always kissing and hugging and playing and making jokes” (FG12/P3). This is described as occurring in their day-to-day working life and is seen as very important for children’s lives. I think the best way to help is by giving lots of love and security, show them that we love them and we care for them … to give them a lot of affection, so that then tomorrow they won’t say “I was in a home and I had a bad time” so I think that is it, to make them feel that this is their home. (FG8/P1)
Thoughts about attachment
Linked to the experience of an affectional bond were their thoughts about attachment and the importance of this in residential settings. From a more theoretical point of view, when prompted with the vignettes (see description of the vignettes in “procedures” above) and when not talking directly about their own experiences, many caregivers could recognize that children have the need to establish an attachment bond with a significant adult, even if they will face separation in the future. For example, “Attachment is needed to form the person, and if they don’t have it, then children become aggressive” (FG8/P4); “To provide security, which is important, it is very important to reassure the child regardless of where you are. Because if it is in a foster home or in a residential home you must reassure children, it is very important for them to feel safe with you” (FG8/P1); and “I think for the child is good to get attached to us, it gives them a little more security from the insecurity that they bring when they arrive” (FG12/P2).
Caregivers also mentioned that this relationship would be positive for the child’s present and future emotional development: “Children who have been attached to us do well in future and you can notice that because they can express the words ‘I love you’, they feel safe, and it is totally different” (FG8/P1); “The child must be attached with you, with the person who protects and cares for her not with anyone because if they go with anyone they can be abused” (FG16/P1); and “When they grow, problems will arise if he did not receive affection, because if he didn’t receive love, what will he be able to deliver when he grows up, when forming a family? So I think it’s important what one gives” (FG8/P1).
Like a second home (24/7)
Getting emotionally involved appears to give their work a different dimension for caregivers; their commitment increases and they continue to feel their emotional bond with children even after they end their shifts, when they are at home, or even during holidays. Many caregivers described the place they work in as a second home for them and mentioned they cannot just “shut the door,” leave, and disconnect themselves from the children. They feel their bond with the children, and their responsibility of what happens at the residential home continues after their working hours, just as if it was a family of their own. One participant noted that it is hard not to think about what has happened at the children’s home, “They [children] become a part of us and we are always concerned, even when we are at home, we are thinking ‘shoots!’ … It’s like a second home for us” (FG12/P3). Similarly, another commented: But one gets involved, very involved. I went on vacation and I think that 15 of the 21 days of my holidays I was in contact [with the residential home] in some way—I called and I also came in on two days, I could not resist it. (F12/P2)
Loss (mixed feelings, worries)
An important theme experienced by caregivers is the feeling of loss when children leave the home. As caregivers have become emotionally involved and have established particular relationships with different children, the caregiver experiences loss and grief when the child leaves. Coping strategies varied, some more positive than others (e.g., sharing feelings of loss and memories with other members of the team vs. hiding feelings or future emotional blocking). This latter refers to caregivers choosing to remain more distant emotionally from children so that they do not suffer the pain of saying goodbye at some point. Loss is linked with mixed feelings when children leave (i.e., happy because they found a family but sad about losing them) and worries about their future (particularly when it is felt that the system for placement endings is not good). Participants’ comments included, “Then, when they leave … that emptiness remains and one misses them” (FG7/P5); “Then, suddenly we have a day off and when you come back the child is gone. Uhhh, that’s terrible, last time it happened to me I said ‘I will never become attached again’” (FG8/P6). One participant also noted, though, that they had to remain emotionally “present” for the sake of the child: When they said that she was going to leave I tried not see her so much but it’s difficult. I tried not to be the one who was always there or not carry her in my arms all the time, but you can’t because the child gets like “what happened?” So the only thing left is just to hug her and look to another side. (FG8/P5)
Positive experience
The third main theme was positive experience, with subthemes of like to work with children, positive team, psychologist support, and Rewarding. Overall, caregivers described their experience as a very positive one; they enjoy working with children and describe being happy as caregivers. When analyzing the differences within groups, this positive experience was more frequently mentioned in those residential homes with a high score on HOME scale. Their narratives are full of happy expressions regarding their experiences and humorous comments when recalling memories of past years in this job. And it was a nice experience, very nice, and I’m still here, stuck until God wants (laughs) … I have been 8 years in this home and 25 years working with children, and these have been the nicest years of my life, I would not change them and if I went back in time, I would start the same again, beautiful experience. (FG15/P4)
Enjoyment in working with the children
A main subtheme mentioned in their positive experience is the fact that working with children is something that they enjoy. Caregivers describe their experience as rewarding; this is linked to feeling that children give them love and that they have achieved important things caring after them, “To me, the most rewarding thing is when the child (without asking anything in return) gives you a hug” (FG12/P2). Other participants commented on the emotional rewards or thanks they get: It’s a job that I love, is my vocation, I love working with children specially with the little ones, I feel like a mama, I have a lot of closeness with them, it’s a work that I love, I like it a lot. (FG15/P2) For me, wonderful. For years I’ve been here. I have seen children who have gone with their family and then later you know that they are happy, they are big, they are nice, or after some time we get a letter thanking us for the way he was raised. (FG3/P4)
Positive team
For caregivers, especially for those working in residential homes that scored higher in HOME scale, their team is an important aspect of their experience. They describe feeling supported by other caregivers, and this support has been a crucial element from the beginning of their job (getting advice and practical support) to the present day. More broadly, they highlight the importance of supporting the norms and limits that other caregivers have established with the children: Maybe we have different characters but we try to enforce all things equally, if she [Colleague] leaves a penalty … then I enforce it … so even if we are different hands, children know that we support each other. (FG12/P2) She [colleague] started teaching me bit by bit every day, she gave me courage to continue because I used to say, “I don’t want to continue, I wanna go.” Then she said to me “I understand you because the same happened to me.” (FG3/P1)
Psychologist support
Another important source of support, which links with having a positive experience, is provided by the psychologists, who are core members of staff in all homes. Caregivers describe the psychologists as supporting not only the children but also the caregivers, providing training and tools to improve the relationships with children: We have a meeting once a month and she [Psychologist] always brings a subject or she asks us, “What subject interests you? In which area are you failing?” We also analyze case by case, we explain which child had problems, “This child is having these tantrums” and she tells us the reason and gives us tools. (FG16/P1)
Difficulties
The fourth important superordinate theme identified in the focus groups was related to difficulties that caregivers found in their experience in residential children’s homes. When present, these difficulties appear to become barriers for the development of other superordinate themes (i.e., emotional involvement and positive experience). However, some of these difficulties were only mentioned in a few focus groups because they are related to specific characteristics and functioning of a specific organization. The difficulties can be organized on two different levels (system and relationship) and have different implications for their work. At the system level, difficulties include the visiting system, end of placement system, lack of information, and ratios. At the relationship level were issues related to relationships with older children and those with behavioral problems, as well as with children’s families, professionals, and managers, and with family–work conflict.
System level
This level groups together all the difficulties reported as deriving from limitations and imperfections of the care system in general. It refers to rules and procedures that, from the caregivers’ point of view, are negative and should be changed.
Visiting system
Caregivers described important difficulties in the visit system related to the authorization of parents’ visits. In particular, they were concerned about the harmful effect of parents inconsistently exercising their right to visits. This happens in the context of Chilean regulations in which parents are encouraged to visit children. Laws establish that if the child is visited at least once every 2 months (or once every 30 days if the child is younger than 1 year old) she/he will not be eligible for adoption. While this is meant to work toward reunification of families, some parents can visit their children every now and then in an irregular pattern to keep their rights as parents, rather than visiting more regularly, which would be in the interests of the child. Caregivers described how this can be harmful for children as it generates expectations and further frustrations in children: Yes, because they are left here and it turns out that they [parents] come to see them the first few months but then they forget. For example there is a little girl here, L., that when her mum does not come to see her she gets aggressive. So how can we end this? What explanation can you give to the girl? (FG8/P5) And it is sad when they see the day pass [that the parent should have visited] and nobody comes to see them, that’s very sad, because it’s reflected in their faces and in their attitude that no one came to see them. (F8/P1) What I would change if I could, would be the subject of taking the kids out, because as she [colleague] said earlier, when we had [previous system], all the caregivers would split the children and took them to their houses … we spent Christmas, New Years with the kids … And now it is harmful to them because they would like to spend a day with us. (FG3/P4)
End of placement system
There are important difficulties perceived in the end of placement system that were mentioned in almost all the focus groups, particularly regarding how children leave and to where they go. For example, caregivers mentioned that on many occasions they did not have the opportunity to say goodbye to the child due to a rapid, unplanned end of placement that was inconsistent with their working hours. This point is relevant considering that children and caregivers have established an affectional bond but also indicates that insufficient time is being given to preparing the child for his/her move to a new location, “Because here they do not have that system that this child is leaving in a month but rather it’s that suddenly one has a day off and comes back and the child is gone” (FG8/P6); “So sometimes we don’t see the children when they go, for example in the weekend we see that my colleagues wrote in the log that children left” (FG3/P2).
In many instances, the future placement is perceived as inappropriate by caregivers even though it has been approved by their managers and other people in the system. This can be due to considering that the family will not care appropriately for the child (e.g., sometimes this occurs with a return to the biological family) or because the child is moved to a different home (in most cases when they reach a certain age); this last option is perceived as the worst. What family can they really go to? As they said [other caregivers in FG], here we see the people and when they leave we more or less feel it will go well or will go wrong. So why the ones above, the court or social workers or psychologist or director do not see it? Why do not they perceive it, do not feel it? (FG3/P2) It was very hard that day because it’s not that she’s gone happy with her parents but went to another home and that kind of made me angry because if she was all right here, here I loved her, then why? I got angry, an anger I had never felt, impotence. (FG8/P6)
Lack of information
This theme was present in only two focus groups but was mentioned by almost all caregivers in these homes. It refers to the need to have more information about children when they arrive in order to properly support them according to the children’s previous histories, “The information when a child arrives, is very minimal. We try to be told something and they tell us nothing” (FG8/P9). In Chile, every individual has a national ID number. Caregivers commented, “We are given only the name and personal ID number of the child” (FG8/P4), and said that this may not be the same in other children’s homes. “The situation we have here is that we do not have the information we should have so we do not know with whom we are working, if they are abused children, battered children, the child’s history” (FG15/P1).
Ratios
Child–caregiver ratio is another factor experienced as a difficulty for the achievement of a personalized relationship with each child, “To dedicate more personalized time is difficult, it’s super tricky because one has to stand for everyone” (FG12/P3). Importantly, participants noted that this is also to ensure the safety of all children when the caregiver(s) has to attend to one particular child who is having difficulties, “The situation is very complicated when one child does have a crisis because you leave the others aside” (FG12/3). This is especially true with the night shifts in the large number of homes in which there is only one caregiver per shift, “We work alone at night, that’s a big failure” (FG16/P2).
Relationship level
Difficulties at this level refer to a variety of areas, including children and their families, as well as conflicts with members of the staff and with their own families.
Behavioral problems and older children
Although caregivers’ narratives were usually very positive when referring to their relationship with children, there were two aspects in which difficulties could be seen. First, the managing of behavioral problems, and second, problems regarding older children. A wide range of behavioral problems are present at different ages, and caregivers usually need some kind of support to be able to face and manage them properly. Caregivers worry for the safety of children and also describe the impact these behaviors have on children and them as caregivers, “Sometimes they hurt themselves or hurt their classmates and controlling such situations, it’s hard for us, that’s the most difficult thing [P2 nods]” (F16/P1). Another participant commented on how it felt to be on the receiving end of this behavior: But when they are in that age of tantrums, what to do? How to contain them? Or we sometimes have children that hurt themselves. So I struggled with that and also, as she says [colleague], the issue of swearing. My second day here was “Hey you … beeeep” [all laugh and nod]. And I said “Oh my God what am I hearing? Young children and they treat me like that!.” (FG3/P4) Especially when children get older [P5 and P3 nod], because maybe small children, and many people who work with young children can say that, the relationship with them is much more fluid and easier to handle. But when children enter adolescence and pre adolescence … Hard. (FG15/P7) Especially when girls of 14 or 13 years old arrived … because they revolutionized everyone else and became disrespectful to us and it was so new that they would swear at you … besides we had to deal with something else. We had seen sexual games in young children [sexual exploration] but here we had to be twice as careful! (FG3/P5)
Relationships with children’s families
The relationship of caregivers with children’s families is complex and varied. The main source of conflict reported was the inconsistency in visits to children and lack of proper care toward them, “Yes, it’s complicated because sometimes parents come and then parents do not come anymore and then uncles come and then uncles are not allowed to visit them anymore and that child is left here, abandoned” (FG16/P2).
This generates feelings of anger in caregivers (linked to their empathy and emotional involvement with children). Caregivers usually see adoption as a better option for children than biological family and they criticize the adoption process as very slow and prioritizing parents’ opportunities to the detriment of the child, “Some will go for adoption and leave here very happy, but there are others that have to return with their family so we have to teach the children some things” (FG16/P1). The other thing that really bothers me and I have seen here is … if you as a mother already have three [sons] and they are all in different homes and you continue to have more children, I say what do these mothers have in their heads? Why bring more children to the world to suffer? (FG3/P3)
Relationship with professionals and managers
As mentioned earlier, the team relationship is an important source of support, but conflicts were also reported between caregivers and other levels of staff (i.e., professionals and managers). This was mentioned only in three of the homes but was shared by a significant amount of caregivers in those focus groups. In these homes, caregivers feel their role is not valued enough and that professionals and managers often impose their own criteria (e.g., when the caregivers did not appear to understand the reasoning for the change or agree with them), “Because we can place a rule and the psychologist or social worker or [Director] do not agree with the rule that we place … And they break it” (FG7/P8); “Sometimes people that come as the heads of the work, are allowed to interfere but I feel that if one has been so long here and the work you have done has been successful, they shouldn’t question it” (FG12/P2); and “One is just the caregiver nothing more. We are a number here even though we get the heaviest work [P1 nods]” (FG12/P2).
Family–work conflict
Participants reported that their relationships with their own families are often affected by their work as caregivers, especially due to the emotional involvement they have with their work that produces emotional exhaustion to the detriment of their own children. This is also linked with the system of shifts that leads to them missing important family and friendship events: The thing about this work is that as you are here for 12 hours, you work hard with your emotions as well as the physical part and in the afternoon there is almost nothing left to take home, and this is every day. (FG7/P9) I would change the public holidays … [All laugh]. We have to work on a holiday, New Year, 18th [national day] … Your turn! … It kills you not having family life … your family or friends get together and they ask “What shift are you on?” “I am in day, or on Evening” and of course at the end they choose not to call you, because you are at the Home. I have had many times the response “quit! you’re killing yourself!” but this is what I like so I feel good, but I also know that you leave aside your family. (FG7/P5)
Discussion and conclusions
It is of note that a key concept in caregivers’ experiences in residential children’s homes is emotional involvement. This seems different to previous findings of studies conducted in large institutions in Europe, which are characterized by deprivation and mechanical care of children, with a focus on physical health, hygiene, and nutrition (The St. Petersburg-USA Orphanage Research Team, 2008). Possibly this difference may be related to cultural factors present in Chile; for example, emotional expression and affection are valued in educational and residential settings, caregivers and other significant adults are called “Aunties,” and usual greetings include hugs and kisses. In this sense, emotional expression and protection may be more valued than independence in children, all of which may be very different from other European countries. Another factor that may be linked to these results is the smaller size of residential homes (or the internal division in small groups in the few bigger homes), which allows more family-like routines and more personalized child–caregiver relationship. Certainly, compared to previous studies, caregivers in this study expressed a different view of their role, with an emphasis on establishing affectional bonds with each child and having a sense of loss and grief when they leave. Two recent studies have found similar results in some orphanages in Ukraine and China, where emotional components in the relationship with children were seen by caregivers as a central part of their work (Neimetz, 2011; Vashchenco, Easterbrooks, & Miller, 2010).
All this gives potential for considering the possibility of integration of family-like dynamics and routines in residential children’s homes. In this perspective, the figure of the caregiver is central and fundamental: They can establish a close, stable, and supportive relationship with children, which has been linked with better outcomes for children (Bakermans-Kranenburg et al., 2011; Lecannelier et al., 2014). In order to make this possible, some structural changes are needed (e.g., improved child–caregiver ratios, less changes of caregivers, better planning for ends of placement, and revision of the visit system), together with training and support for caregivers. Such training should enable them to manage challenging behaviors, have a better understanding of children’s needs, and to provide caregivers with the support they need in processing the loss and grief when children leave.
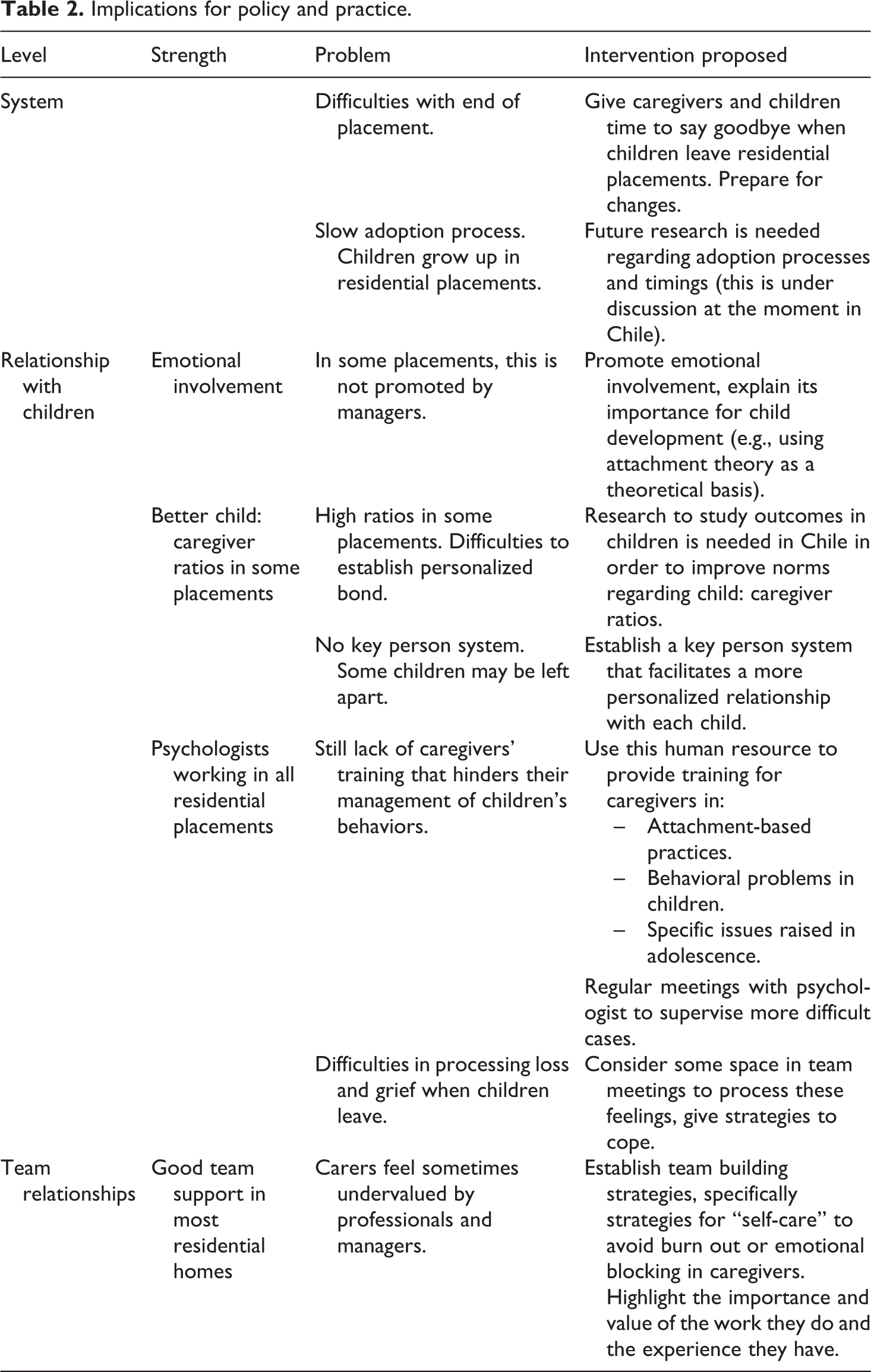
In order to provide better environments for children and caregivers, residential placements need to improve their quality of care. While this has begun in some settings in Chile in the last few years, there is much still to be done. Achieving a better quality of care will enable caregivers to experience a better and more rewarding relationship with children and their team, which will have an important impact on children’s development and well-being. This research exploring caregivers’ experiences has highlighted some important issues that need to be addressed (strengthened if positive or changed if negative) in the care system in order to provide better conditions for caregivers and better care for children (see Table 2). From a broader perspective, and as outlined above, some topics were raised more frequently in those residential homes with a higher score in HOME Inventory (which indicates a better quality of care). For example, the establishment of a differential bond was particularly sensitive to this, as were positive experience and positive team and support.
Implications for policy and practice.
Strengths and limitations of the study
Limitations of this study include the relatively small sample and the fact that the participation was voluntary, which may have an impact on the sample as it is possible that those institutions that agreed to participate may have better conditions than those who declined to do so. Similarly, these findings may reflect the conditions of caregivers in these particular settings and may not be generalizable to all other residential children’s homes in Chile or other countries. Further studies are needed in Chile and other Latin American countries with caregivers working in a diversity of different institutions to be able to have a wider perspective of their experience and the relationship they establish with children under their care.
Another limitation is derived from the fact that the data are self-report, as the main aim was to gather information about caregivers’ experiences. Therefore, it may not reflect an accurate account of the relationship between caregivers and children, but rather their perception of it or the view they wish to present.
It is, however, important to recognize that this study provides a useful insight of caregivers and their views, which are not often considered. This study has highlighted the potential positive figures caregivers can become for children living in residential children’s homes as well as some aspects that need to be improved in order to provide better quality of care for children without parental care.
In conclusion, this study suggests caregivers have an important emotional involvement in the relationship with the children they work with. There is a need for further research, especially regarding possible cultural differences and variations in care, being careful to avoid making decisions based on mainly European and U.S. research. One important consideration is that, traditionally, institutional settings have been seen as opposed to foster family settings, with the debate focusing on which of them can provide better care for children. A new approach has been looking at how to incorporate family-like roles and routines in residential children’s homes (Neimetz, 2011), providing better care for children in need that, for several reasons, do not have access to good quality family care. A large number of children are living in residential children’s homes and, if we want to ensure the best outcomes for all children, we need to allow the debate to occur about how best to house children in residential children’s homes without losing the perspective that good quality family-based care is the better option but might not always be available. Caregivers (in residential children’s homes or foster care) are central figures in this process, and changes in system should consider their role in providing better care for children.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.