
Abstract
Although a growing body of evidence indicates superiority of minimized cardiopulmonary bypass (mCPB) systems over conventional CPB systems, limited venous return can result in severe fluctuations of venous line pressure which can result in gaseous emboli. In this study, we investigated the influence of sub-atmospheric pressures and volume buffer capacity added to the venous line on the generation of gaseous emboli in the mCPB circuit.
Two different mCPB systems (MEC - Maquet, n=7 and ECC.O - Sorin, n=8) and a conventional closed cardiopulmonary bypass (cCPB) system (n=12) were clinically evaluated. In the search for a way to increase volume buffer capacity of mCPB systems, we additionally evaluated the ‘Better Bladder’ (BB) in a mock circulation by simulating, repeatedly, decreased venous return while measuring pressure and gaseous embolic activity.
Arterial gaseous emboli activity during clinical perfusion with a cCPB system was the lowest in comparison to the mCPB systems (312±465 versus 311±421 with MEC and 1,966±1,782 with ECC.O, counts per 10 minute time interval, respectively; p=0.03). The average volume per bubble in the arterial line was the highest in cases with cCPB (12.5±8.3 nL versus 8.0±4.2 nL with MEC and 4.6±4.8 nL with ECC.O; p=0.04 for both). Significant cross-correlation was obtained at various time offsets from 0 to +35 s between sub-atmospheric pressure in the venous line and gaseous emboli activity in both the venous and arterial lines. The in vitro data showed that incorporation of the BB dampens fluctuations of venous line pressure by approximately 30% and decreases gaseous emboli by up to 85%.
In conclusion, fluctuations of sub-atmospheric venous line pressure during kinetic-assisted drainage are related to gaseous emboli. Volume buffer capacity added to the venous line can effectively dampen pressure fluctuations resulting from abrupt changes in venous return and, therefore, can help to increase the safety of minimized cardiopulmonary bypass by reducing gaseous microemboli formation resulting from degassing.
Introduction
A growing body of evidence indicates the superiority of minimized cardiopulmonary bypass (mCPB) systems compared to conventional cardiopulmonary bypass (cCPB) systems, regarding inflammatory reactions and transfusion requirements. Additionally, a more complex patient population has renewed the interest in further improvement of cardiopulmonary bypass (CPB) circuits in terms of reducing priming volume and subsequent hemodilution1-4.
Evident benefits of mCPB systems, however, do not come without consequences 5 . In mCPB systems, the pump flow is dependent on the venous filling 6 . The equilibrium of venous filling is a delicate one: for myocardial preservation, one needs a very limited venous filling (an empty right heart); on the other hand, for an acceptable pump flow, a certain venous filling is necessary. Moreover, venous filling is, among others, dependent on the position of the venous cannula and repositioning of the heart. So, in a mCPB system, the pump flow is directly related to the conditions of (reduced) venous return. During limited venous return, kinetic-assisted drainage, as used in these circuits, can result in severe fluctuations of venous line pressures. Some studies demonstrate that sub-atmospheric venous line pressures can cause large amounts of gaseous microemboli (GME)7-9. These air emboli may be sucked into the venous line at the site of cannulation. Also, there might be the introduction of GME to the circuit by degassing of blood-dissolved gasses whenever venous line pressure drops severely to sub-atmospheric levels.
Without safety mechanisms to remove or circuit modifications to handle venous air, gaseous emboli can easily travel through a mCPB system, causing a greater potential risk for continuous micro air embolization during perfusion8,10-14. A bubble trap embedded in the venous line can decrease the amount of gross air entering the centrifugal pump15-17. Such traps are mainly intended to act as buoyancy. They prevent larger bubbles from entering the pump in which they can be milled to smaller emboli 18 . These emboli will then become suspended in the blood.
It is clear that every effort should be made to prevent air from being entrained in the venous line to decrease the risk of arterial GME. A possible way of reducing the risk of arterial GME is by reducing sub-atmospheric pressure peaks in the venous line. As described by Tamari et al., adding volume buffer capacity (i.e. ‘windkessel’) to the venous line by using the ‘Better Bladder’ can reduce pressure fluctuations at the inlet of roller or centrifugal pumps during kinetic-assisted venous drainage 19 and might, therefore, reduce patient embolic load and improve clinical neurological outcome.
The aim of this study was to investigate the influence of sub-atmospheric pressures and volume buffer capacity added to the venous line on the generation of GME in extracorporeal bypass circuits. The influence of sub-atmospheric pressure was performed clinically, whereas the effect of volume buffer capacity was tested in vitro.
Materials and methods
Clinical
Bubble counts and pressure data of patients who were routinely scheduled for elective coronary artery bypass surgery using CPB were evaluated. Perfusions were performed with three different CPB circuits routinely used at our institution:
The first system, MEC (Figure 1), is a custom designed mCPB (Maquet Cardiopulmonary AG, Hirrlingen, Germany). This system consists of coated 3/8-inch tubing (Bioline, Maquet), a centrifugal pump (Rotaflow, Maquet), and an oxygenator with integrated arterial filter (Quadrox-I BE-HMO71000, Maquet). Additionally, a hard-shell venous reservoir (VHK 2001, Maquet) is connected in parallel to the venous line (Figure 1), but clamped out during perfusion. In case of an emergency, the circuit can be converted to an open system using a vacuum source. The total bypass circuit requires a priming volume of approximately 800 ml. The needle vent is attached to the venous line and cardiotomy blood is transferred to a cell saver.
The ExtraCorporeal Circulation Optimized (ECC.O) system (Sorin Group Italia, Mirandola, Italy) is a mCPB phosphorylcholine-coated system (3/8-inch tubing) equipped with an active venous air removal device (VARD). The arterial line filter (Leukoguard-6, Pall, East Hills, NY, USA) is incorporated in the arterial line and a hard-shell venous reservoir (Dideco D970 s/v PHISIO, Sorin Group, Italy) is connected in parallel to the venous line (Figure 2), but clamped out during perfusion. As in the MEC circuit, the circuit can be converted to an open system using a vacuum source. The priming volume of this system is approximately 900 ml. Separate roller pumps are used for the needle vent and cardiotomy suction, and blood is transferred to the cardiotomy reservoir from which it is given back to the circulation by occasionally opening the clamped reservoir outlet line.
The conventional closed CPB (cCPB) system (Figure 3) consists of a hollow-fibre oxygenator (Capiox SX18, Terumo Cardiovascular Systems, Tokyo, Japan), 1/2-inch venous and 3/8-inch arterial line tubing, 1/2-inch medical grade silicone arterial pump tubing, an arterial line filter (Leukoguard-6, Pall), a collapsible venous reservoir (JVR 1900, Maquet), and a cardiotomy reservoir (Capiox SX hard-shell reservoir, Terumo). This system requires approximately 1600 ml of prime. Separate roller pumps are used for the needle vent and cardiotomy suction, and blood is transferred to the cardiotomy reservoir from which it is given back to the circulation.
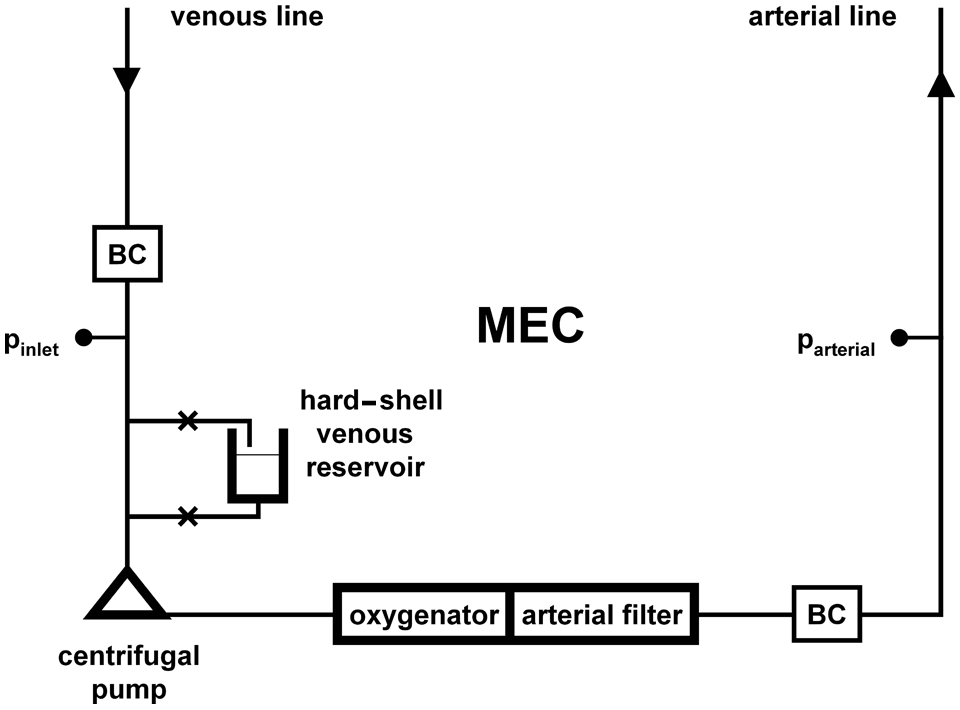
Minimized cardiopulmonary bypass circuit (MEC) using a centrifugal pump, oxygenator with integrated arterial filter, bubble counters (BC) and pressure measurement near the pump inlet and in the arterial line.
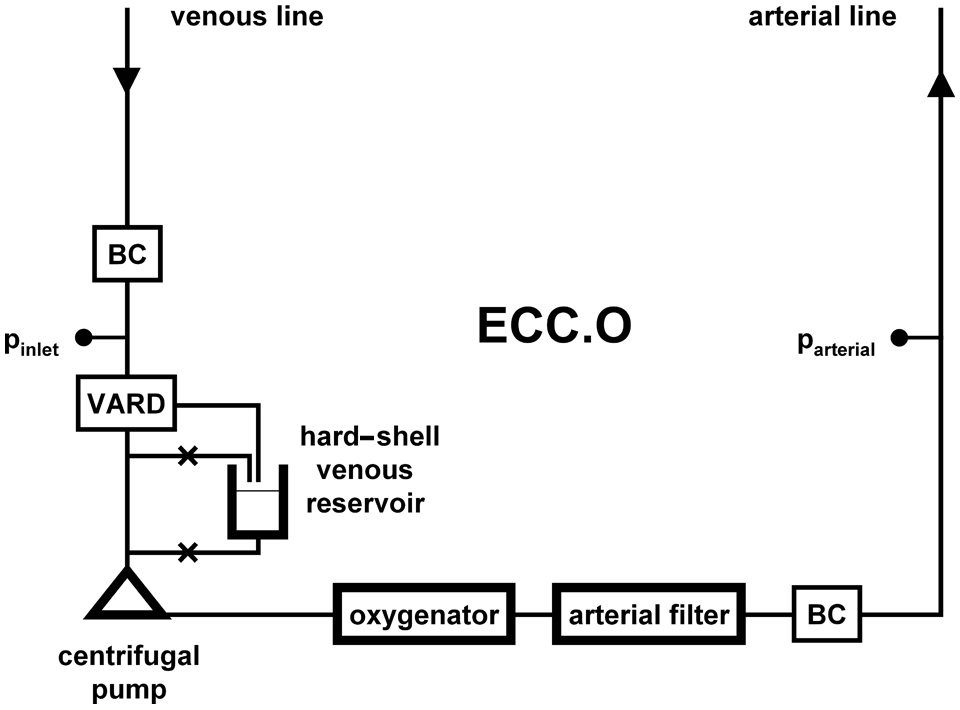
Minimized bypass circuit with active venous air removal device (VARD), oxygenator, arterial filter, bubble counters (BC) and pressure measurement near the pump inlet and in the arterial line.
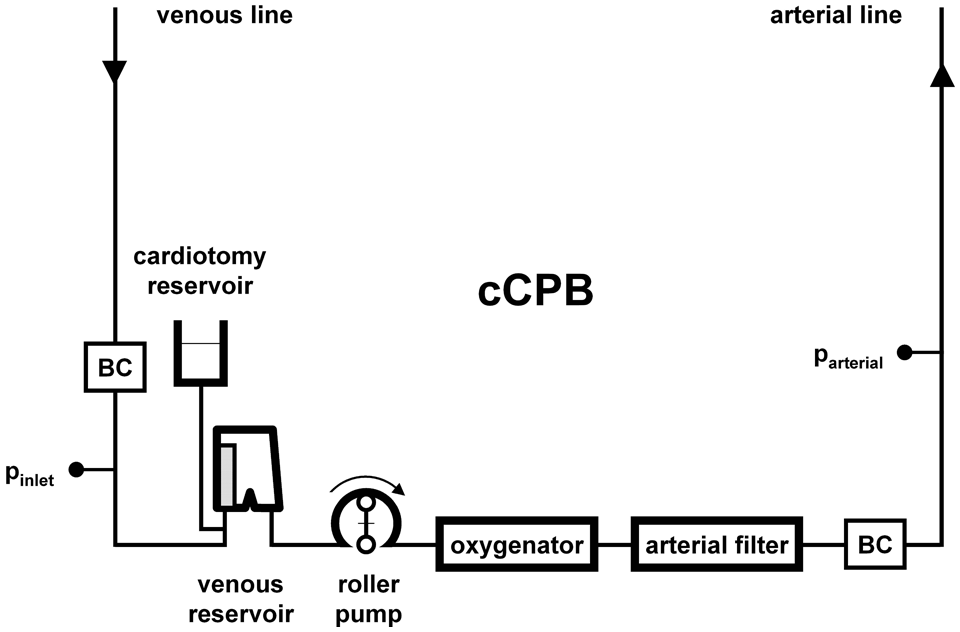
Conventional cardiopulmonary bypass circuit with soft-shell venous reservoir, cardiotomy reservoir, roller pump, oxygenator, arterial filter, bubble counters (BC) and pressure measurement near the inlet of the venous reservoir and in the arterial line.
A colloidal solution was used for system prime and normothermic perfusion was standardized by clinical practice. Pump flow was maintained around 2.5 L·min·m2 to keep venous saturation in the range of 65-70%. The mean arterial pressure was kept around 80 mmHg using phenylephrine infusion, if necessary.
Microbubble activity was recorded in the venous line and in the arterial line downstream of the arterial filter at a sample frequency of 0.2 Hz, using a bubble counting device (Bubble Counter BC200, Gampt GmbH, Zappendorf, Germany). Flow was measured at the outlet of the oxygenator using an ultrasonic clamp-on flow probe (H9XL, Transonic Systems Inc., Ithaca, NY, USA). Pressures were measured in the venous line, approximately 80 cm from the cannulae, and at the outlet of the oxygenator, using pressure transducers (PX604, TruWave, Edwards Lifesciences, Irvine, CA, USA). Electronic data were acquired with a sampling frequency of 250 Hz using a programmable PC-based acquisition system (MPAQ amplifier with IDEEQ software, Instrument Development Engineering & Evaluation, Maastricht University Medical Centre, Maastricht, the Netherlands).
In vitro
The effect of volume buffer capacity added to the venous line on the generation of sub-atmospheric pressure and GME was studied in a mock circulation of a mCPB circuit primed with 0.9% NaCl solution (Figure 4). Volume buffer capacity was provided by a Better Bladder (Circulatory Technology Inc., Oyster Bay, NY, USA). The centrifugal pump flow (Rotaflow, Maquet) was set to approximately 5 L/min with an initial pressure of -80 mmHg at the inlet side of the pump (pvenous line), whereas a non-occlusive single-roller roller pump (20 rpm) partially, periodically and transiently obstructed the venous line, thereby, simulating recurring short-lasting reduced venous return as it may occur in clinical minimized cardiopulmonary bypass. A hollow-fibre oxygenator was used intermittently for the elimination of gaseous bubbles from the circulation to minimize re-entering using vacuum, or to restore gaseous dissolved content in the fluid. The effect of the Better Bladder during transient reduced venous return on pressure and bubble count was evaluated by respectively opening clamp A while closing clamp B and vice versa.
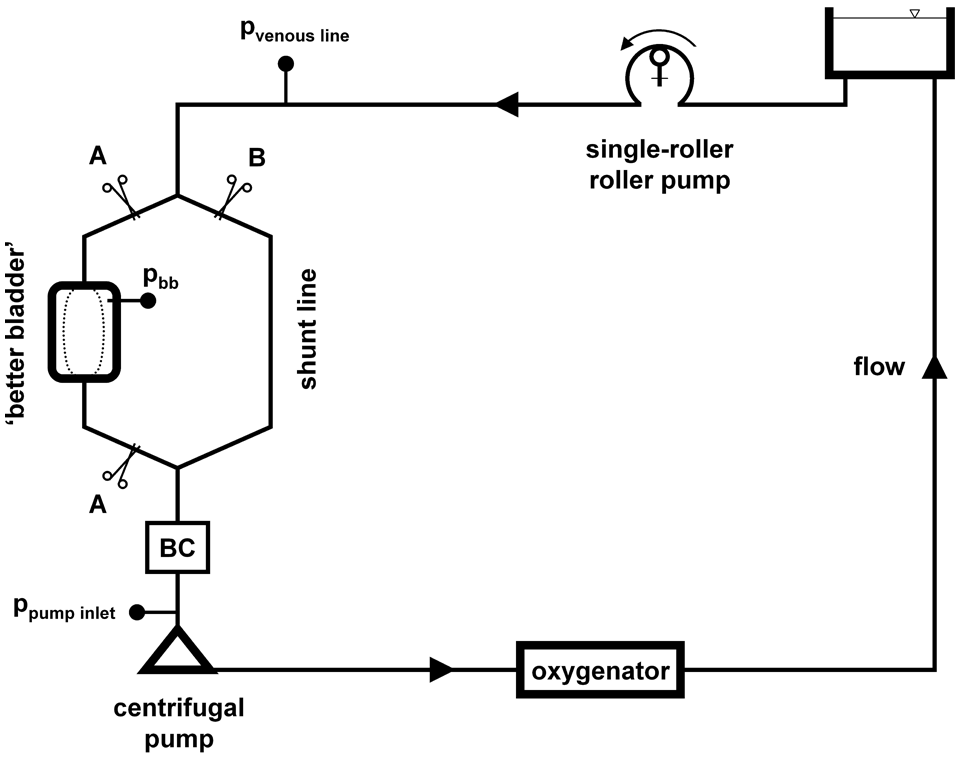
Mock circulation of a minimized circuit with incorporated Better Bladder, pressure measurement and bubble counters (BC). The single-roller roller pump is set non-occlusive and simulates repeatedly developing transient reduced venous return.
Statistical analysis
The ANOVA procedure was used to test the difference of mean values in groups. The relationship between venous sub-atmospheric line pressure and GME activity in both venous and arterial lines was analyzed by cross-correlation function and regression procedure (SPSS version 16.0, SPSS Inc., Chicago, IL, USA). P-values less than 0.05 were considered statistically significant. All values are expressed as mean ± standard deviation.
Results
Clinical data
GME activity in the arterial line during clinical perfusion with a cCPB system (n=12) was the lowest in comparison to the minimized systems (312±465 with cCPB versus 311±421 with MEC (n=7) and 1,966±1,782 with ECC.O (n=8) cumulative counts per 10 minute time interval, respectively; p=0.03) (Figure 5). Figure 6 shows the corresponding cumulative volume of gas bubbles registered in the venous and arterial lines per 10 min intervals. However, the average volume per bubble in the arterial line was highest in cases with a cCPB (12.5±8.3 nL versus 8.0±4.2 nL in MEC and 4.6±4.8 nL in ECC.O; p=0.04 for both; data not graphically displayed). Overflow bubble count, i.e. signals coming from bubbles of more than 500 μm in diameter, were registered during 2 cases with MEC (28%), 2 cases with ECC.O (25%) and 3 cases with cCPB (25%). In all cases, the postoperative period was uneventful.
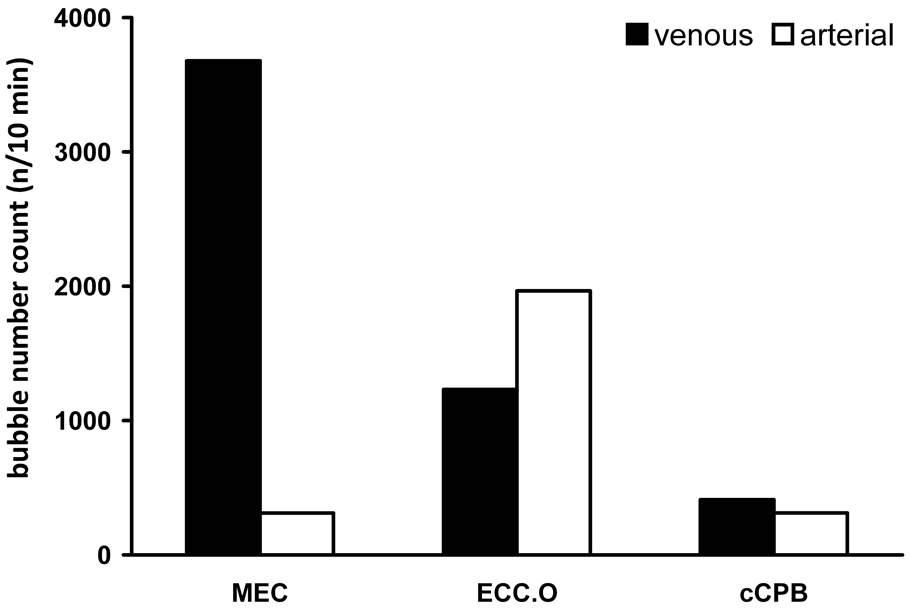
Cumulative number of microbubbles registered in both venous and arterial lines, per cardiopulmonary bypass circuit, per 10 minute interval.
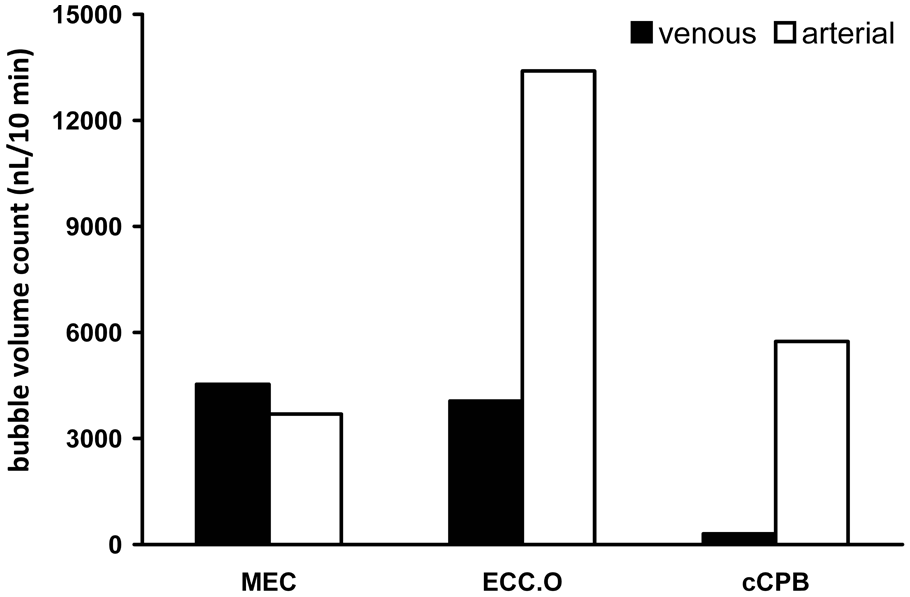
Cumulative volume of gas bubbles registered in venous and arterial lines, per cardiopulmonary bypass circuit, per 10 min interval.
Cross-correlation function showed a significant correlation between gas bubbles and sub-atmospheric pressure peaks in the venous line in 56% of MEC cases, in 43% of the ECC.O cases, and in one case with the cCPB system (12%). In other words, the appearance of GME in the venous line of MEC was directly related to peaks of sub-atmospheric pressure. In cases with cCPB using gravity drainage, GME in the venous line cannot be explained by ‘extreme’ suction. The bivariate correlation procedure showed a significant correlation between sub-atmospheric pressure peaks and GME in the venous line (Pearson’s correlation factor -0.35 for MEC). Much lower was this relationship in ECC.O cases (0.02) and in cases using the cCPB (-0.06).
Gas bubble activity in the arterial line was significantly related to gas bubbles in the venous line (Pearson’s correlation factor for MEC=0.25; ECC.O=0.65). There was no such correlation in cases of cCPB.
Table 1 shows the average venous line and venous line peak pressures during periods with and without emboli counts. Pump flow values in the three groups are comparable (Table 1). With the ECC.O system, both average venous line pressures and venous line peak pressures are higher than when using the MEC.
Venous line pressures and corresponding pump flows.
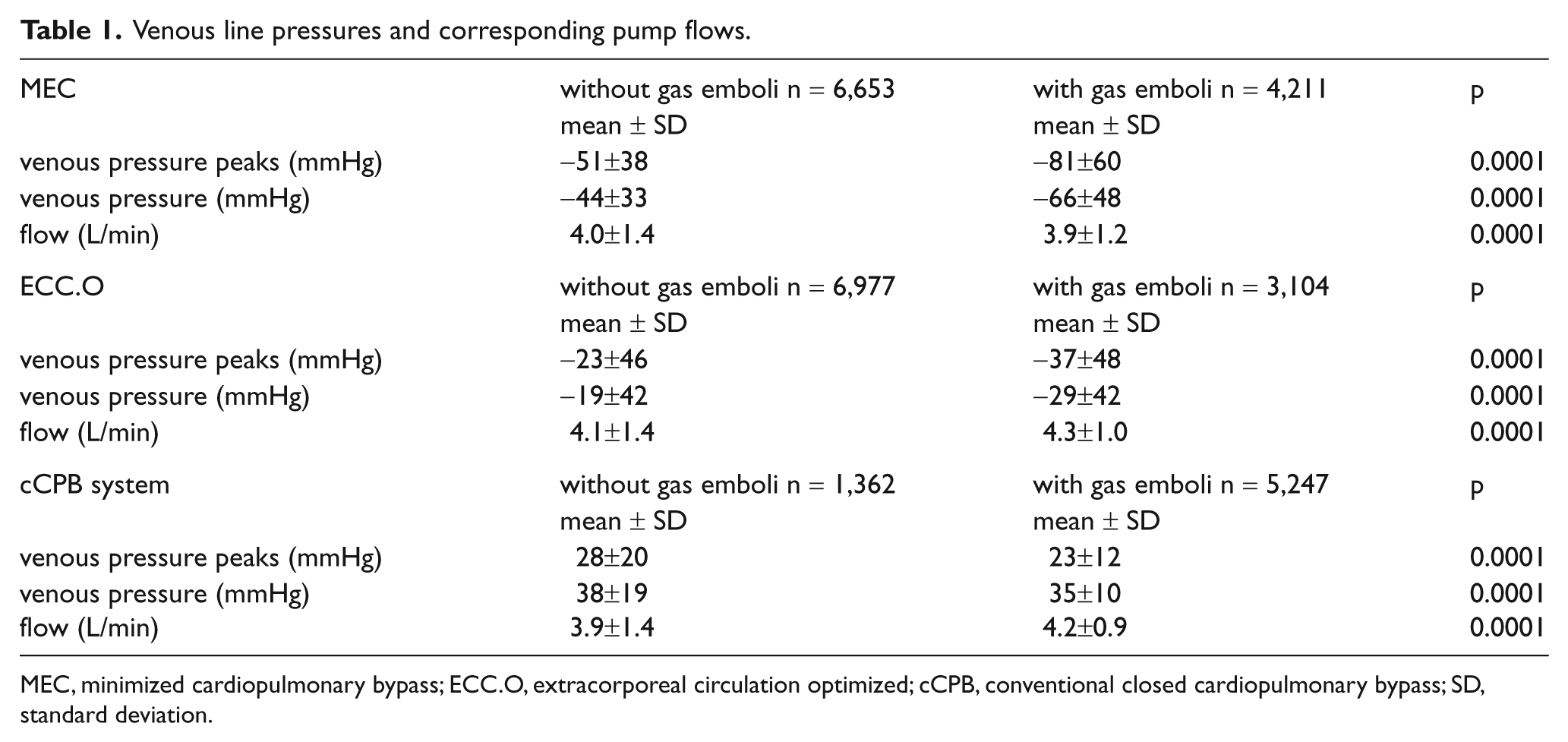
MEC, minimized cardiopulmonary bypass; ECC.O, extracorporeal circulation optimized; cCPB, conventional closed cardiopulmonary bypass; SD, standard deviation.
In vitro data
The incorporation of the BB can dampen fluctuations of the venous line pressure during transient conditions of reduced venous return in mCPB by approximately 30%. Figure 7 shows the effect of the Better Bladder during limited venous return on venous line pressure and gaseous emboli measured in the mock circulation. By dampening, the Better Bladder decreased the number of GME by up to 85%.
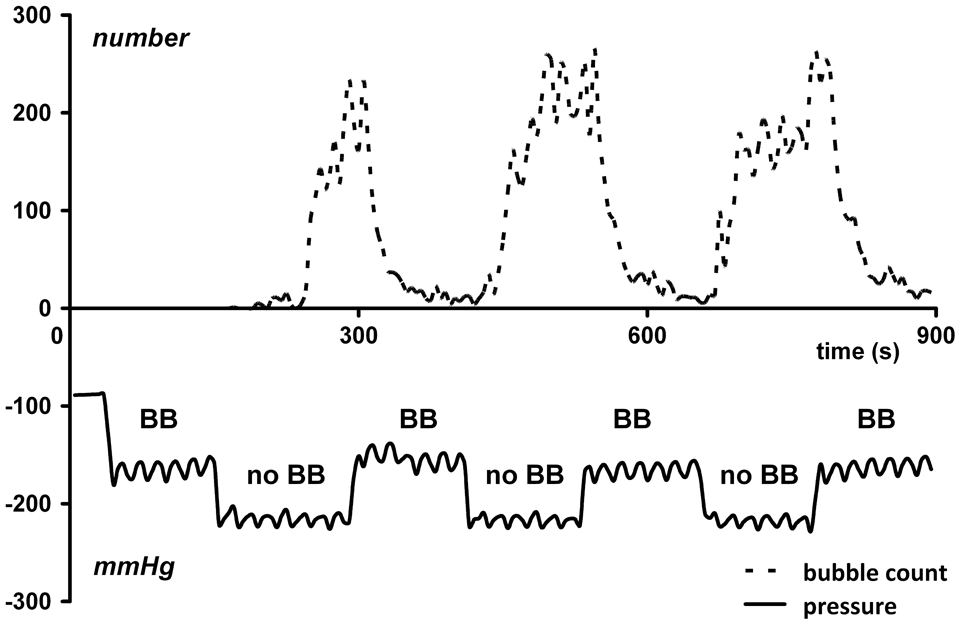
Venous pressure and resultant bubble count during conditions of reduced venous return with (BB) and without (no BB) Better Bladder in-line the minimized bypass circuit. With the Better Bladder included, venous pressure is higher and bubble count is clearly diminished.
Discussion
This study investigated the influence of sub-atmospheric pressures and added volume buffer capacity on the generation of gaseous microemboli (GME) in minimized cardiopulmonary bypass (mCPB) systems. Lower sub-atmospheric pressures tend to induce higher amounts of GME, whereas volume buffer capacity added to the venous line dampens fluctuations of venous line pressure and reduces GME generation.
The use of cardiopulmonary bypass (CPB) may result in the introduction of gaseous emboli into the patient's arterial circulation. These may be introduced during drug infusion via the central venous lines of the anaesthesia or via infusion into the CPB circuit itself20,21. Although decreasing venous line pressure increases the risk of air aspiration at the cannulation site, to the best of our knowledge, there is no clinical data available correlating data on GME occurrence with low venous line pressure and degassing in CPB systems. According to Henry’s Law, a sudden decrease of line pressure results in gaseous bubble formation in the blood 22 , as a pressure decrease disturbs the dissolved gas equilibrium. This study discusses the often underestimated, or even unknown, but present risk of bubble formation when blood is exposed to sub-atmospheric pressures.
The venous line pressures measured in the MEC group were significantly lower than to those in the ECC.O group (Table 1). This is due to the fact that the circuit and, in our cases, the pressure measurement site is located lower in relation to the patient’s position when compared to the MEC system, where it is located nearly at table height. The positive pressure measured in the cCPB group can be explained by the hydrostatic column pushing on the sensor located in the venous line near the reservoir inlet. In the ECC.O group, arterial GME count and volume were higher than in the MEC and cCPB group. This can be explained by the fact that both the ECC.O and cCPB use cardiotomy suction which can introduce bubbles into the circuit, but the cCPB features a collapsible venous reservoir that can collect bubbles. In contrast, the average arterial bubble volume was highest in the cCPB group, which can be explained by the absence of a centrifugal pump that can mill air emboli into smaller bubbles. Moreover, GME resulting from degassing are expected to be smaller, which is seen in the MEC and ECC.O groups.
GME can be quantified using bubble-counting devices, commercially available for clinical application. Two common devices used are the GAMT BCC200 and the Emboli Detection and Classification quantifier (Luna Innovations, Roanoke, VA, USA) 23 . Both devices, however, show major limitations when used for studying ‘worst-case’ scenarios. A worst-case scenario can be a situation of embolic showers or macro air emboli, conditions in which the bubble counters cannot discriminate between individual bubbles (bubble count overflow). Threshold levels, however, can vary between devices and results obtained by one device in a first study cannot be compared or exchanged with results from another device in a second study 24 . Therefore, great care should be taken when correlating measured data with neurocognitive outcome.
As mentioned before, mCPB systems have an increased risk of air entrainment25,26. The data in this study suggest that there is also the risk of introducing GME, even if venous blood is GME free. GME might come from degassing and could add to the explanation that some studies fail to translate the salutary effects of mCPB into clinical benefit5,27.
Bubbles found in the arterial line can have their origin in the venous line when entering the circuit at the cannulation site. With mCPB systems, some surgeons, therefore, suggest using a double purge-string suture to prevent any air from being sucked into the circulation. This double snaring, however, cannot prevent the induction of GME resulting from degassing. The degassing occurs in the venous line and inside the centrifugal pump during conditions of reduced venous return. With extreme blood loss, luxation of the heart, cannula obstruction or tube kinking, pump flow is drastically diminished and venous line pressure can transiently peak down to -300 mmHg or even less. Like Tamari et al., we also noticed the Better Bladder dampened pressure fluctuations (Figure 7) 19 . In addition to the reduction of sub-atmospheric peak pressures, we found a decrease in GME formation. Nevertheless, the Better Bladder remains a passive device that adds volume buffer capacity to the venous line. It does not solve the underlying mismatch of venous return and pump flow. Pump control using servo-regulation and improved venous cannula design has been proposed to optimize venous drainage28-30. Minimized CPB systems with Better Bladder and pump servo-regulation, combined with anti-obstructive venous cannula design, could prevent venous line pressures from peaking down to excessively low levels with concomitant GME formation, while pump speed adapts to venous drainage to maintain the maximal level of support available at that instance.
In conclusion, severe sub-atmospheric fluctuations of venous line pressure during kinetic-assisted drainage, as used in minimized cardiopulmonary bypass systems, are related to gaseous microemboli. Volume buffer capacity added to the venous line can effectively dampen pressure fluctuations resulting from abrupt changes in venous return and, therefore, can help to increase the safety of minimized cardiopulmonary bypass by reducing gaseous microemboli formation resulting from degassing.
Footnotes
Acknowledgements
The authors would like to acknowledge Miss Anouk A.M.A. Lindelauf for her assistance during data collection. The authors are grateful to the American Academy of Cardiovascular Perfusion who distinguished this work with the Best Paper Award at the 2011 Annual Academy Meeting.
Presented at the 32nd Annual Seminar of The American Academy of Cardiovascular Perfusion, Reno, Nevada, 27-30, January, 2011
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
The authors declare that there is no conflict of interest.