
Abstract
The ideal location of air bubble detector (ABD) placement on the cardiopulmonary bypass (CPB) circuit is debatable. There is, however, very little data characterizing the prevalence of specific ABD placement preferences by perfusionists. Therefore, the purpose of this study was to survey the perfusion community to collect data describing the primary locations of air bubble detector placement on the CPB circuit.
In June 2011, an 18-question on-line survey was conducted. Completed surveys were received from 627 participants. Of these, analysis of the responses from the 559 certified clinical perfusionists (CCP) was performed.
The routine use of ABD during CPB was reported by 96.8% of CCPs. Of this group, specific placement of the bubble detector is as follows: distal to the venous reservoir outlet (35.6%), between the arterial pump and oxygenator (3.8%), between the oxygenator and arterial line filter (35.1%), distal to the arterial line filter (ALF) (23.6%), and other (1.8%). Those placing the ABD distal to the venous reservoir predominately argued that an emptied venous reservoir was the most likely place to introduce air into the circuit. Those who placed the ABD between the oxygenator and the arterial line filter commonly reasoned that this placement protects against air exiting the membrane. Those placing the ABD distal to the ALF (23.6%) cited that this location protects from all possible entry points of air. A recent false alarm event from an ABD during a case was reported by 36.1% of CCPs.
This study demonstrates that the majority of CCPs use an ABD during the conduct of CPB. The placement of the ABD on the circuit, however, is highly variable across the perfusion community. A strong rationale for the various ABD placements suggests that the adoption of multiple ABD may offer the greatest comprehensive protection against air emboli.
Introduction
Air bubble detectors (ABD) alert the perfusionist to the presence of air in the cardiopulmonary bypass (CPB) circuit and have become an important safety device used to guard against massive air embolism during open-heart surgery. Since their introduction over 30 years ago, the ABD (which can be attached to the tubing of the extracorporeal circuitry), has rapidly been adopted by practicing perfusionists in the United States of America. 1,2 Perfusion safety surveys indicate that the use of ABD during cardiopulmonary bypass (CPB) procedures has increased from 47.9% in 1986 to 87.8% in 2000. 3,4
Currently, the prudence of ABD use during the conduct of CPB has been collectively accepted and articulated in the Practice Guidelines by both the American Society of ExtraCorporeal Technology (AmSECT) and the American Academy of Cardiovascular Perfusion (AACP). Each organization recommends that a bubble detector be used during the conduct of CPB. 5,6
Despite this professional consensus on using the ABD during CPB, the ideal placement of the device on the extracorporeal circuit is unclear and can vary greatly. 7,8 Apart from a single unscientific poll in 1993, there is an absence of information that characterizes the specific location of ABD placement that perfusionists select during the conduct of CPB. 9
To further develop best practice guidelines, it may be important to understand the current application of the use of this safety device by perfusionists. Therefore, the purpose of this study is to survey the perfusion community to: (i) collect data describing the primary locations of air bubble detector placement, and (ii) understand the rationale of this placement.
Methods
Institutional review
Following review by the SUNY Upstate Medical University Institution Review Board (IRB), this study was granted approval.
Survey time frame
The survey was conducted during June 2011 – August 2011.
Survey instrument
The survey contained 18 questions covering three core sections: (1) Demographics, (2) Perfusion Work Details, (3) Details of Bubble Detector Use. The questions were formatted on a web-based commercial survey site (www.surveymonkey.com). The survey data security and confidentiality of participants were ensured through physical protection, software devices and hardware features.
Target population and data collection
The target population was perfusionists certified by the American Board of Cardiovascular Perfusion (ABCP). To collect responses from this population, members of the American Society of Extracorporeal Technology (AmSECT) and members of Perfusion.com were asked to participate in the confidential voluntary survey via the online forums, PerfList and PerfMail, respectively. To increase participation, a second follow-up posting on these forums was performed four weeks later. Finally, for under-represented geographic regions in the survey, as compared to the ABCP database, direct emailing requests to perfusionists were made using the CTSnet database.
Selection criteria
Respondents who indicated that they were certified by the AACP were included in the analysis. Non-CCP and incomplete surveys where participants failed to answer questions on the details of bubble detector placement were excluded.
Statistical analysis
Confidence intervals of the survey were calculated using a confidence level of 95% and a population of the 2011 ABCP certified clinical perfusionists (n=3760). All other data are expressed as percentages (%) within the total number of respondents.
Results
Respondent rate and confidence limits
A total of six hundred and twenty-seven individuals submitted a survey. Of these, 559 surveys met the inclusion criteria of individuals with CCP status, for a response rate of 14.9% of ABCP certified perfusionists in the year 2011. The confidence interval of the survey is ± 3.8%.
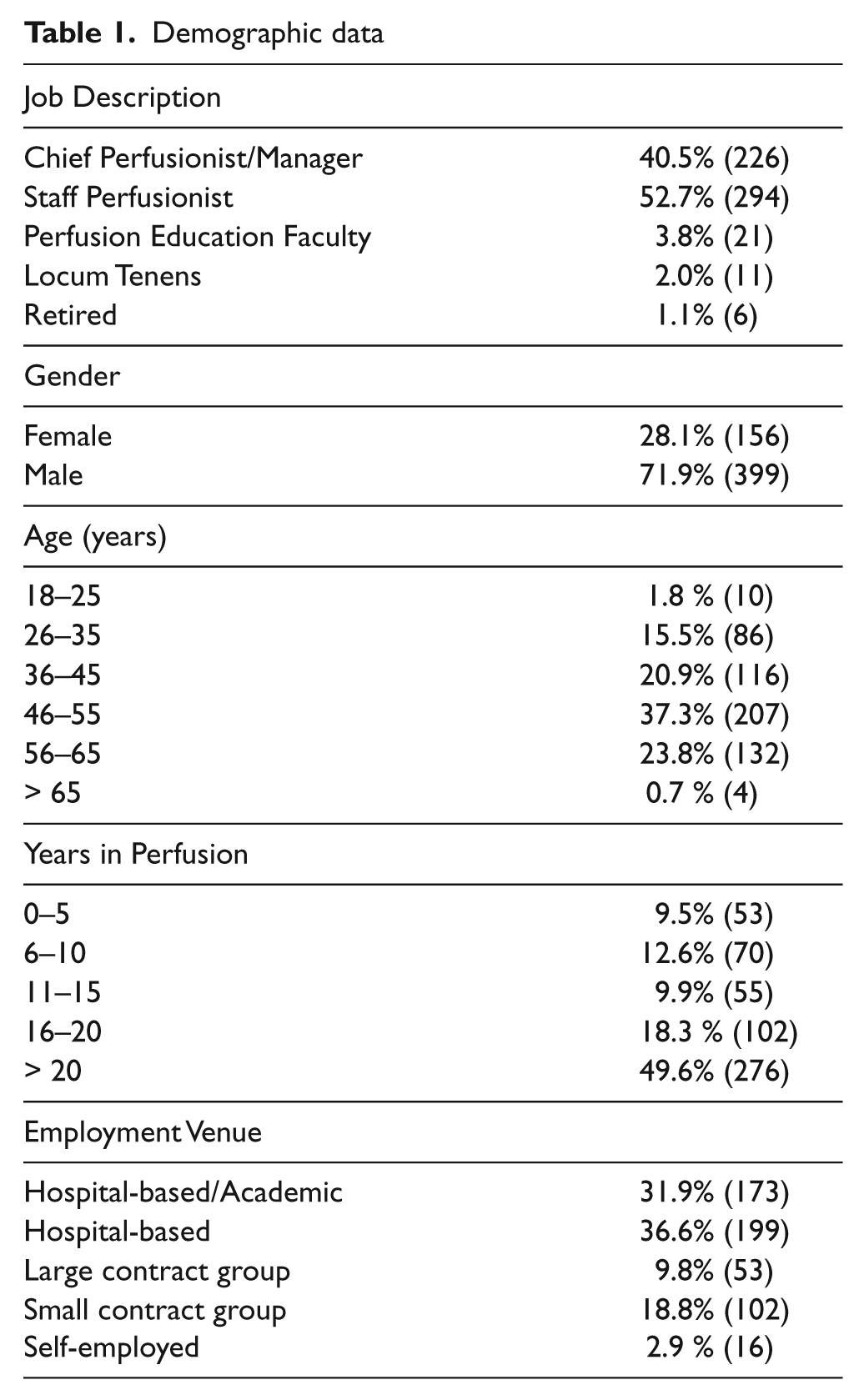
Demographics
The respondent characteristics are shown in Table 1. Regarding the titles of respondents, the majority identified themselves as staff perfusionists (52.7%), with the second largest group being chief perfusionists (40.5%). With concern to the gender distribution, there is 71.9% male and 28.1% female. The respondent age range was diverse, with the largest group being between 36-45 years old (37.3%). Nearly half of the respondents (49.6%) had been practicing for >20 years. Most participants worked as either an employee of a hospital-based practice (36.6%) or in an academic/hospital-based (31.9%) institution.
Demographic data
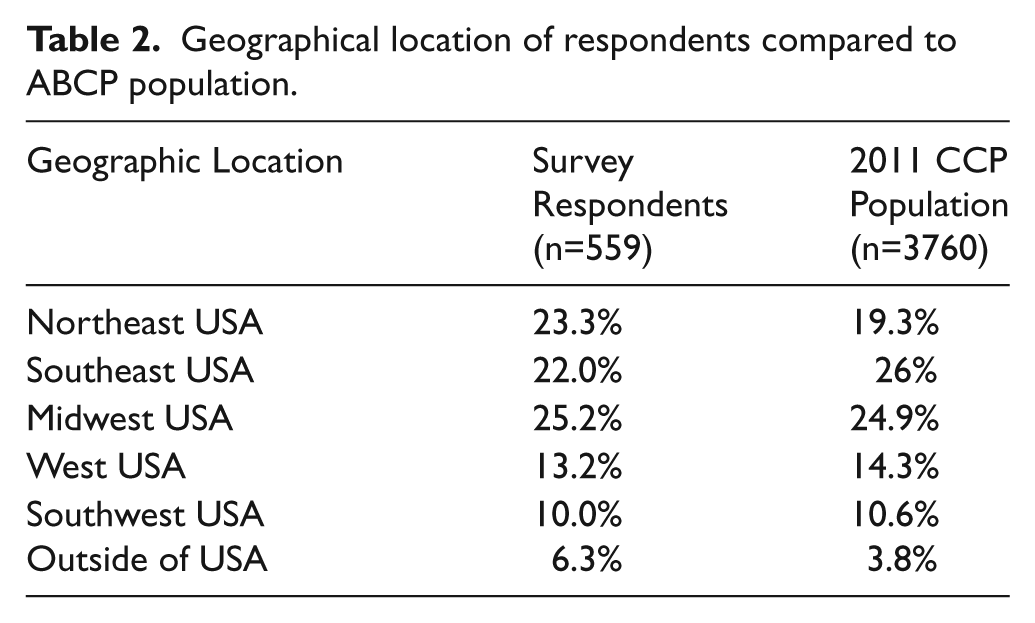
The geographic regions represented by the respondents were compared to the 2011 ABCP published data indicating CCP locations (Table 2).
Geographical location of respondents compared to ABCP population.
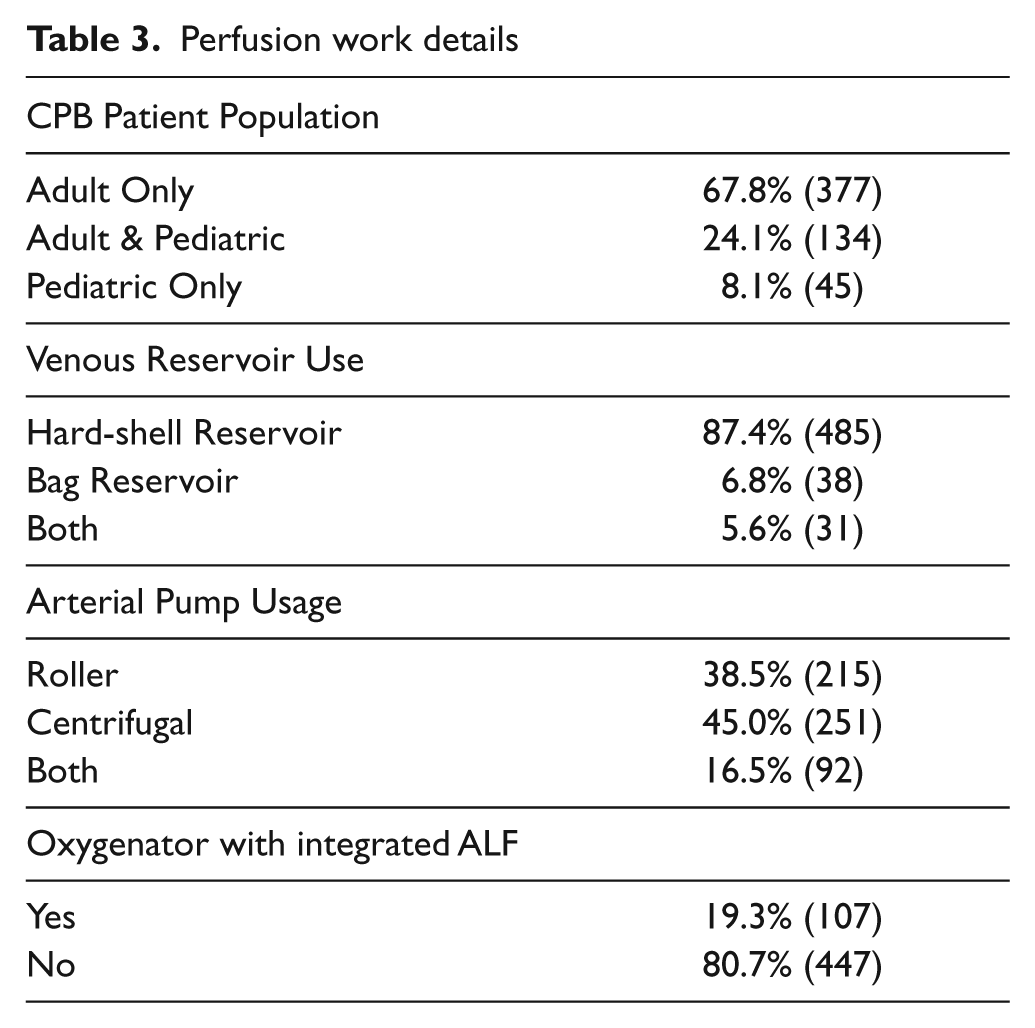
The patient population and circuitry details are shown in Table 3. Perfusionists who work primarily with adult patients represented 67.8% of the participants. In regards to circuitry, hard-shell venous reservoirs and centrifugal arterial pumps were used most often (87.4% and 45%) among participants, respectively. Oxygenator units with an integrated arterial line filter (ALF) were used by 19.3% of the respondents.
Perfusion work details
Bubble detector use and placement
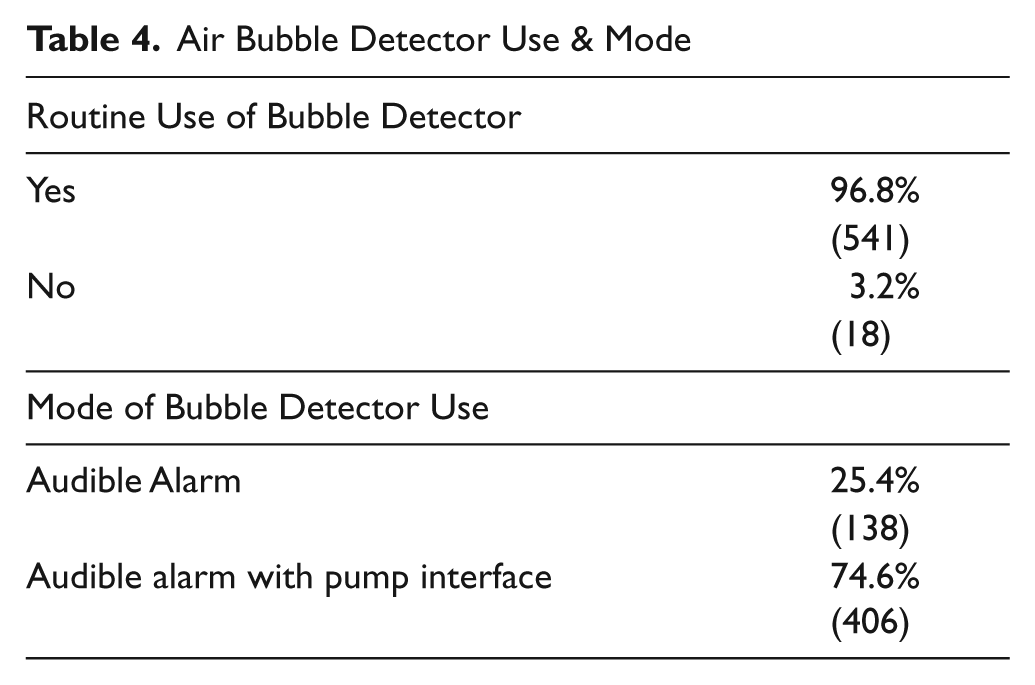
Of the 559 CCP participants, 541 (96.8%) routinely use an air bubble detector during the conduct of CPB (Table 4). For this group, 74.6% indicated that the air bubble detector is in modes that will automatically servoregulate the system (pump stop, coast, or clamp).
Air Bubble Detector Use & Mode
The specific placement of the bubble detector in the CPB circuit is shown in Figure 1. Briefly, 35.6% were placed distal to the venous reservoir outlet, 3.8% were between the pump outlet and the oxygenator, 35.1% between the oxygenator and the arterial line filter, and 23.6% placed the bubble detector distal to the ALF. Additionally, 1.8% of perfusionists stated that they use multiple bubble detectors in their primary circuit so a single location could not be verified.
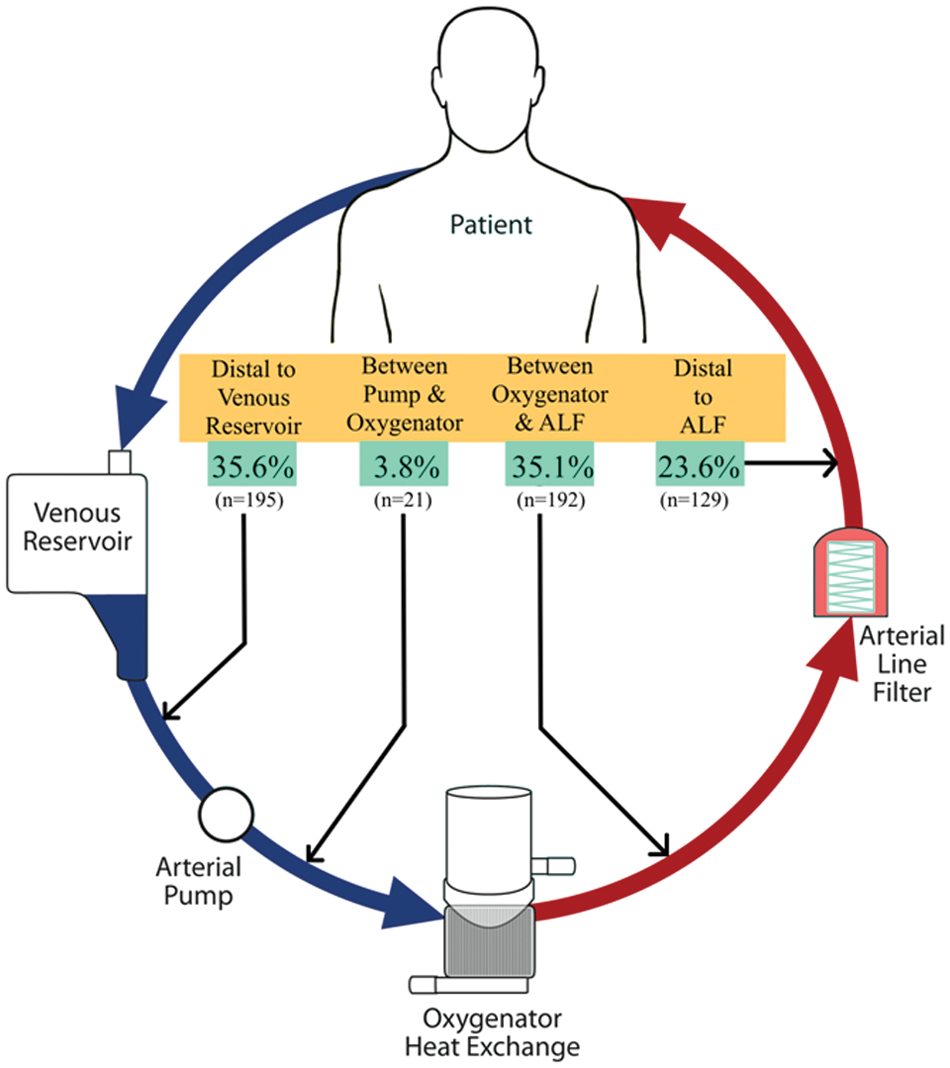
Air bubble detector placement locations by certified clinical perfusionists. Arrow shows the CPB circuit location indicated by survey respondents. (There was also a 1.8% “Other” response associated with the use of 2 bubble detectors).
By cross-tabbing the data and comparing the distribution of ABD locations between centrifugal pump to roller pump, users showed no significant differences between groups. Cross-tabbing data and comparing primarily pediatric CCPs with adult only CCPs revealed that the pediatric-only group placed the ABD distal to the arterial line filter more often than their adult-only counterparts (33.0% vs. 19.0%). Similarly, users of an oxygenator with an integrated ALF place the ABD in locations before the oxygenator inlet more when compared to CCPs who use a conventional oxygenator (51.9% vs. 36.1%, respectively).
Regarding the selected placement of the bubble detector, 89% indicated that this was a standardized location used by their department (40.1% written departmental protocol, 48.9% unwritten consensus agreement). The remaining 11.0% stated that it is not standardized at their institution and can vary from perfusionist to perfusionist.
Rationale for bubble detector placement
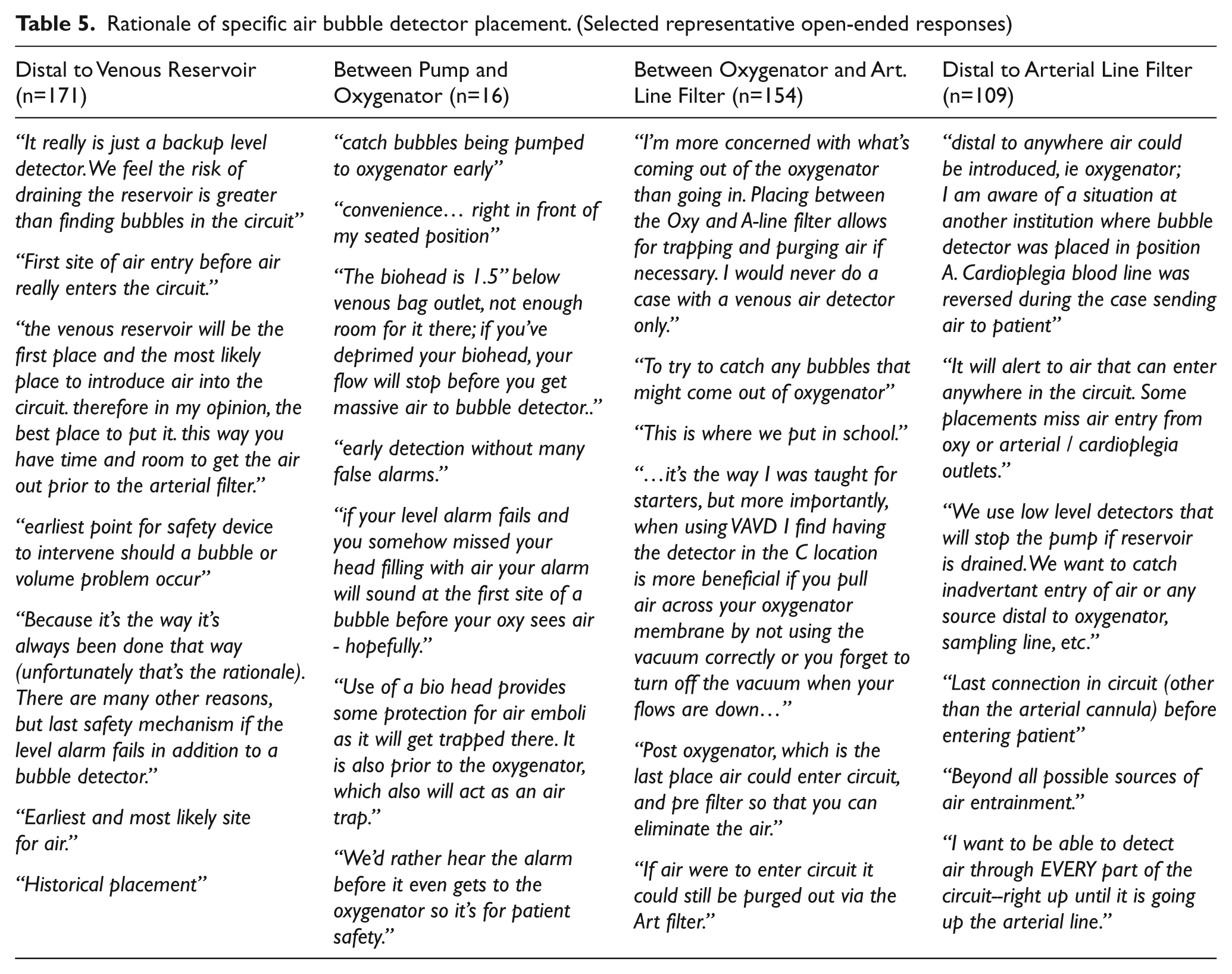
Selected comments provided by respondents on their rationale of the selected ABD placement is shown in Table 5. Briefly, those placing the ABD distal to the venous reservoir (35.6%) argued that an emptied venous reservoir was the most likely place to introduce air into the circuit and, therefore, was the best location. Those who placed the ABD between the oxygenator and arterial line filter (35.1%) commonly reasoned that this placement protects against air exiting the membrane while also providing a means for removal of air through the ALF purge. Those placing the ABD distal to the ALF (23.6%) most often cited that this protects the patient from all possible entry points of air. Some CCPs stated that the use of multiple ABD would be ideal to allow for more than one location.
Rationale of specific air bubble detector placement. (Selected representative open-ended responses)
Air bubble detector false alarms
Of the respondents, 36.1% believed that they have experienced a bubble detector false alarm during the conduct of CPB. The majority (96.4%) indicating that this event had minimal impact and was only a minor inconvenience; however, the remaining 5.1% did believe that the false alarm had a significant impact on the case.
Open-ended comments
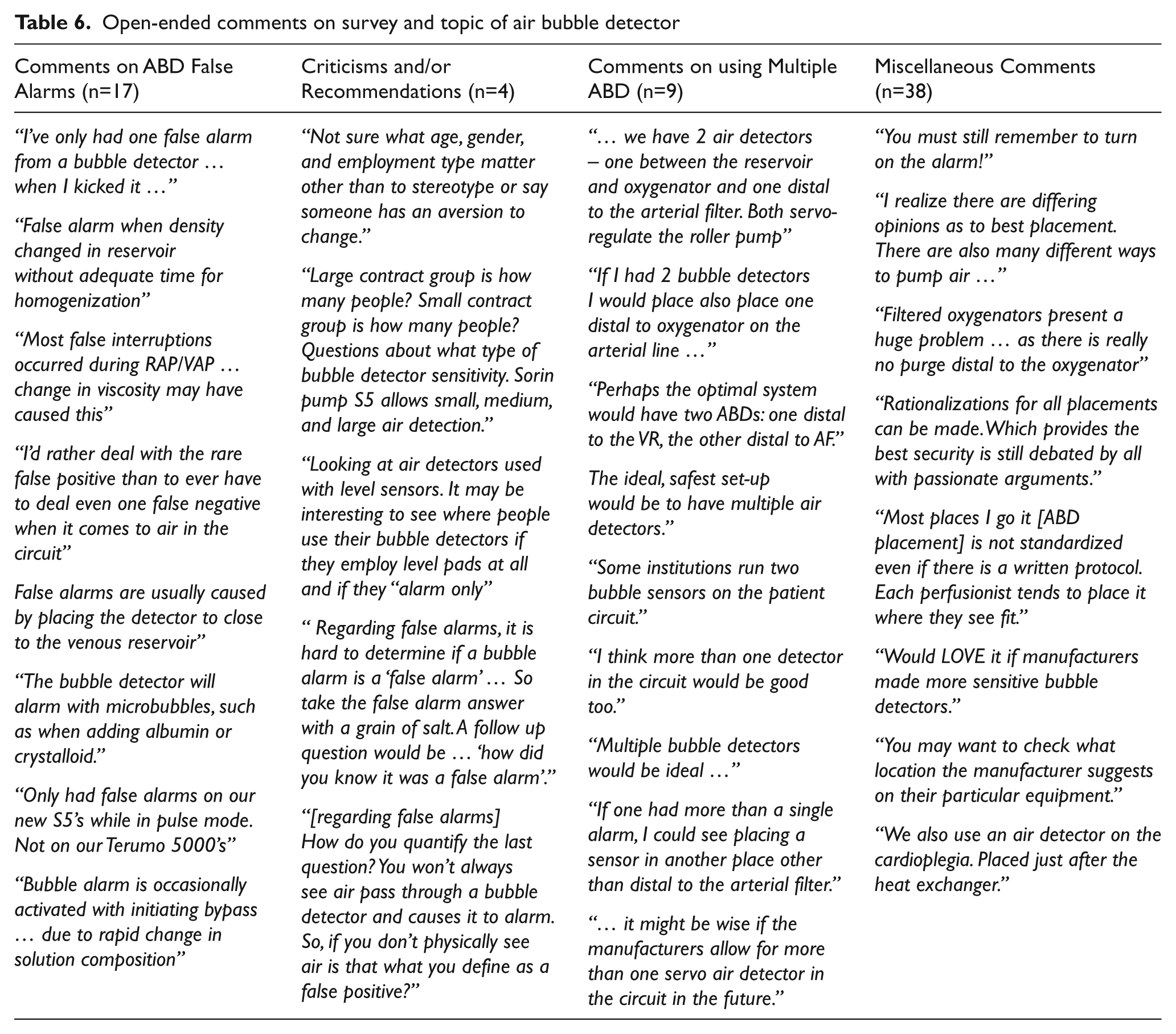
Participants were given the opportunity to add any comments on the survey and the topic of air bubble detectors. Of the 559 respondents, 118 (21%) entered comments. Of these, 42.4% were comments of support and/or encouragement to publish results. The remaining comments could be generally categorized into four groups: False Alarms (n=17), Criticisms and/or Recommendation (n=4), Multiple ABD (n=8) and Miscellaneous Comments (n=38). Selected comments are shown in Table 6.
Open-ended comments on survey and topic of air bubble detector
Discussion
A principle finding of this study is that 96.8 (± 3.8%) of certified clinical perfusionists routinely employ the use of an air bubble detector during the conduct of CPB. This adds to previous surveys revealing the progressive adoption of air bubble detectors by perfusionists during the conduct of CPB. 3,4
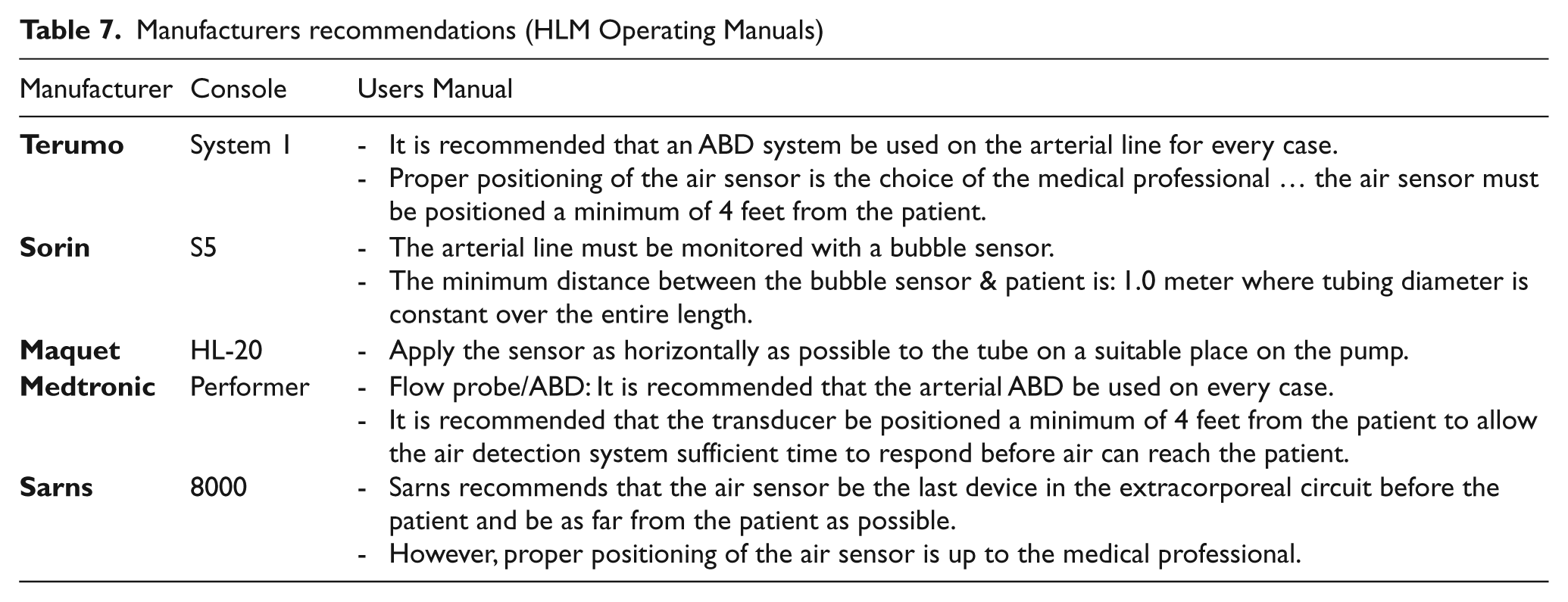
Additionally, this study, for the first time, moves the discussion beyond simply whether an ABD is used or not, to where on the CPB circuit the perfusionist chooses to place this safety device. It is evident from this survey that the placement of the ABD is far from universally agreed upon by certified clinical perfusionists. Nearly 36% of CCPs will place the ABD distal to the venous reservoir. This placement is supported in a major textbook, Cardiopulmonary Bypass: Principles and Practice, 8 that states, “… for most prompt air detection, the sensor should be placed between the CPB reservoir and the systemic pump.” This statement suggests that air will most likely enter the CPB system via the emptying of the venous reservoir and, therefore, having the ABD just distal to the reservoir will halt the infiltration of air. This rationale is strengthened by the Australian and New Zealand College of Perfusionists voluntary incident reporting system, Perfusion Incident Reporting System (PIRS), which suggests that the emptied venous reservoir is the dominant mechanism for air entering a CPB system (personal communication, T. Willcox C.C.P.). The majority of respondents (59%), however, place the ABD on the arterial line; ~35% between the oxygentaor and arterial line filter and ~24% distal to the arterial line filter. This arterial line placement is also supported by textbooks with statements that “… the ideal position is arguably close to the outlet of the oxygenator” 7 and “it is usual practice to have the bubble detector on the arterial outlet of the circuit” and that “bubble detector[s] on the arterial line are desirable safety devices.” 10 Furthermore, many of the manufacturers’ operator manuals recommend that the ABD be placed on the arterial line (Table 7). Additionally, there is often a recommendation to position the ABD a certain distance from the patient’s arterial cannula (presumably to allow adequate time to detect and stop the pump to avoid air embolism). The dominant rationale for arterial line placement is the notion that air can enter the system in other ways (besides an empty venous reservoir) and positioning the detector on the arterial line protects against other possible sources of air entry.
Manufacturers recommendations (HLM Operating Manuals)
As seen by the open-ended comments in Table 5, it appears that there is valid rationale for the each of the various ABD placement positions indicated by certified clinical perfusionists. Perhaps the use of more than a single ABD would provide the greatest safety from air embolism. This notion of multiple ABD is not new; 11 however only a small percentage (< 2%) of respondents in our study use more than a single ABD on the primary CPB circuit. One limitation to more widespread adoption of the use of multiple bubble detectors (e.g. concurrently using one distal to the venous reservoir and one on the arterial line) is the availability of such a configuration. While cardioplegia ABD are becoming more common, only the Terumo System 1 (Terumo Cardiovascular Systems, Ann Arbor, MI) offers the user the option of multiple ABD for the primary circuit.
Approximately 36% of respondents indicated that, within the last 2 years, they have experienced an ABD false alarm during the performance of CPB. Often, the false alarm was associated with the initiation of retrograde autologous prime (RAP) procedures where the rapid change from crystalloid prime to blood was thought to trigger the false alarm. A small percentage (~5%) of those reporting ABD false alarms felt that the disruption had a significant impact on the case. Some respondents pointed out that the question was unclear and did not define what constituted a false alarm. In retrospect, this could have been better clarified.
There are other limitations within this study. The authors assume that this was a representative sample of the CCP population and constitutes the power of a scientific survey. The response rate was 559 (~15% of the CCP population) with a geographic, gender and age distribution that approximates the ABCP 2011 database, yet, since this was conducted via the internet, it could be open to some selection bias. Additionally, though unlikely, it could be possible for an individual to enter a duplicate survey and, thereby, skew the results.
In summary, this study establishes that the use of the ABD during the conduct of CPB is nearly universally practiced by CCPs. Additionally, this survey demonstrates that clear differences exist between perfusionists regarding the placement of ABD on the CBP circuit. The thoughtful and strong rationale for the different characterized site locations suggests that the use of multiple ABD on the primary CPB circuit should be considered.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of Interest Statement
None declared.