
Abstract
Pulmonary arterial hypertension (PAH) is a severe disease characterized by a progressive increase of pulmonary pressure and resistance, leading to right heart failure. PAH is commonly diagnosed at a late stage of the disease and is associated with progressive clinical deterioration and premature death. The treatment of PAH continues to be complicated, especially when considering treatment with extracorporeal membrane oxygenation (ECMO). A case is described that involves a heart failure patient placed on a ventricular assist device as a bridge to heart transplantation with recent onset of PAH. The goal was to rest the entire pulmonary circulation during ECMO while allowing the ventricular assist device to continue to function using a modified veno-arterial (VA) cannulation strategy. This configuration allowed the patient’s right heart to rest and ultimately recover while the left ventricular assist device (LVAD) maintained systemic perfusion, successfully allowing the patient to maintain a United Network for Organ Sharing (UNOS) status 1a listing.
Keywords
Introduction
The treatment of chronic pulmonary hypertension continues to be a challenge related to many complex medical mechanisms. Pulmonary hypertension may be transient or fixed and can result from a wide array of pathologies, including heart disease, thromoboembolic conditions, liver disease and low oxygen conditions. 1 Pulmonary hypertension may be treated medically with vasodilatory drugs, endothelin receptor antagonists, anticoagulants, diuretics and oxygen therapy. When conventional medical therapy fails, surgical intervention may be the only option available. Surgery may include an atrial septostomy to relieve the pressure in the right heart. If no other therapies are successful, the patient may be evaluated for a double lung transplant or heart-lung transplant. 2 One dilemma often encountered during the interim time period of failing medical therapy and transplant is related to the wait time. The wait time for a heart transplant may widely vary, ranging from days to years due to the blood type of the patient, as well as the wait list for other patients awaiting transplantation. 3
Extracorporeal membrane oxygenation (ECMO) is one option for patients that may serve as a bridge to heart transplant for those too sick to survive on conventional medical therapy. 4 One challenge that persists is the cannulation strategy for patients with pulmonary hypertension. In patients with primary respiratory failure, it is common to cannulate in a veno-venous (V-V) fashion. In order for V-V ECMO to be successful, both the right and left heart must have normal function. Patients with pulmonary hypertension may fail V-V ECMO cannulation support as their right heart function is often compromised and the right ventricle cannot overcome the increased pulmonary pressure. 5 There have been reported cases of patients with pulmonary hypertension supported on veno-arterial (V-A) ECMO via the subclavian artery. 6 V-A support may present problems, including left heart distension and inadequate decompression, with possible thrombus formation. 7 Although some patients with pulmonary hypertension and failing right ventricles have a preserved left ventricular function, there are situations in which the left ventricle also fails. 8
This report describes a patient awaiting heart transplant, with pulmonary hypertension while supported on ECMO. The patient was being supported on an HVAD (Heartware Inc., Framingham, MA, USA) left ventricular assist device and it was determined that the device required supplemental blood flow to continue to function without thrombus formation related to device stasis. The problem related to secondary pulmonary hypertension for the native right ventricle not providing adequate blood supply across the lungs and into the LVAD. Therefore, a means to transport blood from the right side of the heart to the left side of the heart while still resting the pulmonary vasculature was required to support the patient’s circulation.
Case Report
The patient was a 51-year-old female diagnosed with a non-ischemic cardiomyopathy, supported medically on Milrinone, who was listed as status 1a for heart transplantation. Prior to admission, the patient had experienced increased dyspnea, with several syncopal and ventricular tachycardia episodes. A right heart catheterization, completed upon admission, revealed elevated pulmonary artery pressures (59/28/39 mmHg) with an increased pulmonary vascular resistance (PVR) (13.6 Wood units). With an ejection fraction of 10% and worsening left ventricular failure, the decision was made to implant a HeartWare (HeartWare Inc.) ventricular assist device.
On postoperative day 8, the patient developed hypoxemic respiratory failure related to pneumonia. Although the patient was supported on inotropes and pulmonary vasodilators, she remained in refractory ventricular tachycardia, requiring multiple defibrillations. In order to provide right ventricular and respiratory support, the decision was made to support the patient on ECMO.
The patient was transported back to the operating room. Upon redo sternotomy, it was noted that the right heart was severely dilated. V-A ECMO was establishedby using a Centrimag (Thoratec Corp., Pleasanton,CA, USA) blood pump and a Quadrox-iD (Maquet Cardiovascular, Rastatt, Germany) oxygenator. The right femoral artery and vein were isolated before administering 5000 units of systemic heparin. The patient wascannulated in the right femoral artery by direct cut-down and a 6-mm graft was sewn end to side. An 18 French (Fr) elongated one-piece arterial cannula (Medtronic Inc., Minneapolis, MN, USA) was inserted into the graft and connected to the ECMO circuit. The femoral vein was cannulated with a 21 Fr Biomedicus (Medtronic Inc.) cannula and connected to the ECMO circuit. ECMO was initiated and the patient’s ventricular tachycardia was resolved; however, inadequate and unsustainable flows were noted from the patient’s HVAD. It was hypothesized that, although the pulmonary hypertension created a lack of blood flow to the left heart, the ECMO circuit diverted even more flow from the HVAD.
Due to the low HVAD flows, secondary to the veno-venous (V-V) ECMO support, the patient was converted to pulmonary right-heart oxygenator (PROxy) or OxyRVAD by diverting blood from the right atrium, bypassing the lungs and returning the blood to an 8-mm graft sewn to the right upper pulmonary vein. This allowed for optimal pulmonary venous return and allowed for better HVAD performance (see Figure 1).
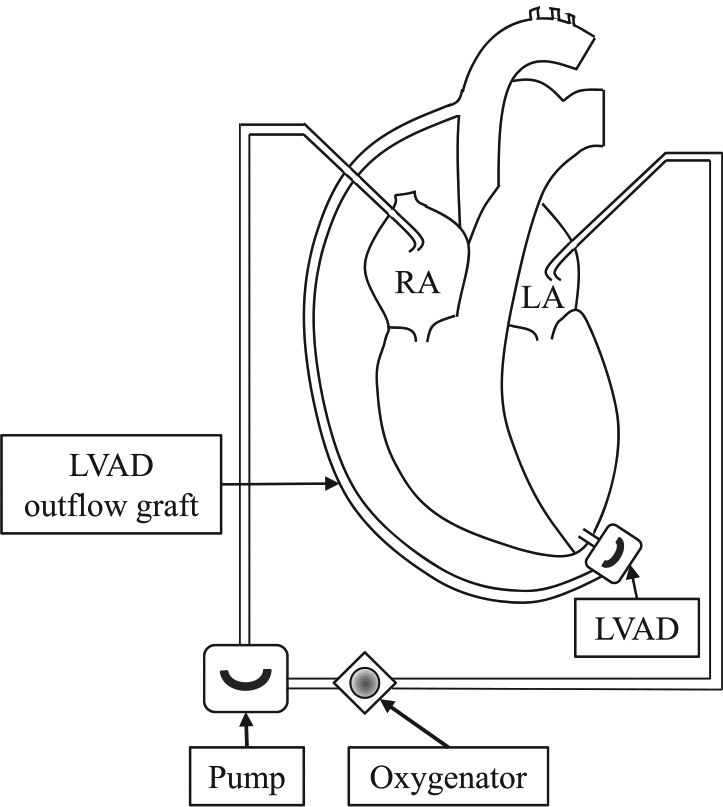
Figure 1 reflects the final cannulation strategy. The patient was cannulated in the right atrium. Blood returned to the pump and was delivered through an oxygenator. The blood was then returned to the left atrium, into the ventricular assist device and, ultimately, to the HVAD outflow graft to the aorta.
A 24 Fr elongated one-piece arterial (EOPA) cannula was inserted into the pulmonary venous graft. The ECMO flow was interrupted in order to reconnect the arterial limb to the EOPA cannula in the pulmonary vein graft. ECMO flow was reinitiated, which resulted in an improved HVAD flow and right ventricular (RV) decompression. A 28 Fr right-angle, plastic-tipcannula (Edwards Lifesciences, Irvine, CA, USA) was then inserted into the right atrial appendage. The ECMO flows were again interrupted to remove the venous line and the right femoral venous cannula. The venous drainage was reconnected to the 28 Fr right atrial cannula and ECMO flows were re-established. There was markedly improved right heart decompression, confirmed by transesophageal echo, along with left ventricular filling and increased HVAD flows. Blood flow through each device was initially matched and balanced at 3.65 L/min. The sternum was closed and the patient was transported back to the intensive care unit.
The patient was awakened and allowed to ambulate. The post-operative course consisted of physical therapy. Heparin therapy was maintained to achieve an activated partial thromboplastin time (aPTT) of 60-70 seconds. Pulmonary vasodilation was achieved by continued medical treatment while on ECMO, along with aggressive diuresis. On post-operative day 10, right ventricular function had improved and ECMO flow was weaned by 100 to 200 cc/min/day. On post-operative day 18, with ECMO support weaned down to 1.0 L/min and HVAD flows between 4.0 to 5.0 L/min, the decision was made to remove her from the PROxy ECMO circuit. The patient was ultimately transitioned to oral pulmonary vasodilators and she was discharged home on her HVAD. The patient’s pulmonary hypertension ultimately resolved and the patient is a candidate for future heart transplantation.
Discussion
There is an increasing trend to awaken patients and allow them to ambulate while on ECMO.9,10 ECMO support has expanded to broader indications for use, such as more complicated pathologies, including bridge to lung transplant, chronic obstructive pulmonary disease (COPD), bridge to recovery for pneumonia, acute respiratory distress syndrome (ARDS) and influenza. 11
ECMO support in adults was successfully used following the H1N1 outbreak in 2009. 12 Cannulation for the pulmonary hypertension population often requires special consideration for those with a failing right and/or working left ventricle, making both conventional V-A and V-V ECMO less optimal. With the modified V-A ECMO cannulation strategy using a PROxy platform, as described in this case report, a technique such as this may be used to allow the patient to be adequately supported, preserving the left side of the heart and allowing the patient to either recover from the pulmonary hypertensive crisis or bridge to their heart transplant.
Footnotes
Presented at the 36th Annual Seminar of the American Academy of Cardiovascular Perfusion, San Antonio, TX, 5–8 February 2015.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Discussion: ECMO cannulation strategy for pulmonary hypertension: an alternative approach to traditional Veno-Arterial ECMO
Presenter, Linda Mongero
This discussion is taken from the dialogue that followed the presentation of the previous paper at the 36th Annual Seminar of the American Academy of Cardiovascular Perfusion. Although the paper has been through Perfusion’s stringent peer-review process, the discussion is a transcript of the dialogue, edited for clarity, and the views expressed in the discussion are those of the commentators and do not necessarily represent, and should not be attributed to, the journal Perfusion, the Editors, authors or the Publisher, SAGE.