
Abstract
Introduction:
Use of extracorporeal life support (ECLS) has significantly increased in critically ill patients refractory to medical management. ECLS requires systemic anticoagulation to avoid thromboembolic complications and superimposed coagulopathies are common. Transesophageal echocardiography (TEE) is frequently employed to assess cannula position and cardiac function during extracorporeal therapy. The goal of this study was to assess whether TEE probe insertion and removal in systemically anticoagulated ECLS patients was safe compared to patients without ECLS and normal coagulation studies.
Methods:
Eighty-seven separate TEE examinations in 53 adult ECLS patients were analyzed. Detailed complication profiles were logged for each patient from initiation through discontinuation of ECLS. Routine coagulation testing was recorded within two hours prior to the TEE exams. Controls consisted of age- and gender-matched patients undergoing perioperative TEE without ECLS and normal coagulation (N=87).
Results:
Overall TEE-associated morbidity in ECLS patients was 2.3% and consisted of minor oropharyngeal bleeding (2/87 TEE exams) exclusively. The patients presenting with oropharyngeal bleeding received heparin for anticoagulation and had two or more abnormal coagulation studies at the time of TEE. Seventy-nine percent of ECLS patients received intravenous heparin infusions, 6.8% argatroban and 3.4% epoprostenol. Ten-point-eight percent of patients were not anticoagulated at the time of TEE because of pre-existing bleeding complications and/or deranged plasmatic coagulation profiles. No major complications (e.g., esophageal perforation, gastrointestinal bleeding, accidental extubation) were recorded in either group.
Conclusions:
TEE remained safe in critically ill patients under ECLS, despite systemic anticoagulation, during probe insertion, manipulation and removal. TEE-related complications pertained solely to oropharyngeal bleeding amenable to conservative management.
Keywords
Introduction
Transesophageal echocardiography (TEE) has become a routine and invaluable diagnostic tool in standard clinical practice. Its impact spans clinical decision-making in cardiac surgical operating rooms, cardiology suites and intensive care units by providing crucial real-time information on valvular function and cardiac performance, thereby, facilitating accurate hemodynamic management and the diagnosis of congenital heart defects or the pathology of the great vessels. TEE is considered relatively safe and semi-invasive. The reported overall incidence of TEE-associated complications ranges between 0-0.5%, with mortality rates between 0-0.02%.1–7 The majority of TEE-associated complications arise from oropharyngeal trauma, comprising up to 13% of all reported complications.2,3
ECLS systems (i.e., veno-venous extracorporeal membrane oxygenation (ECMO) or veno-arterial extracorporeal life support) have become important assist devices to support gas exchange and/or cardiac function in patients with respiratory and/or cardiac failure refractory to conventional respiratory and pharmacological management. The use of ECLS devices for temporary support through life-threatening heart and lung failure has dramatically increased over the past decade.8–10
In order to avoid device-related thromboembolic or hemorrhagic complications from platelet activation by contact with artificial surfaces, patients on ECLS support require systemic anticoagulation.11,12 In addition, these patients often suffer from coagulopathies from pharmacologic platelet inhibition or mechanical damage of platelets and von Willebrand factor. 13
The clinical management of ECLS patients frequently necessitates comprehensive echocardiographic examination in order to assess correct cannula position and cardiac function, to investigate sudden hemodynamic changes and, ultimately, to facilitate ECLS weaning. While TEE has become standard practice during cardiac surgery, probe insertion during surgery usually happens before anticoagulation and the probe is removed after reversal of the anticoagulants. The morbidity of TEE probe insertion, manipulation and removal in ECLS patients with coagulopathies has not been examined to date.
The goal of this observational study was to examine whether critically ill patients under systemic anticoagulation during ECLS therapy and possible concomitant coagulopathies had higher TEE-related complication rates than a control group of age- and gender-matched patients with normal coagulation studies receiving routine TEE during cardiac surgery.
Patients and Methods
Patient selection and data acquisition
Approval for this retrospective study was obtained from the Institutional Review Board of the University Hospital of Tübingen. Patient records were anonymized and de-identified prior to data analysis.
Electronic charts of 53 patients over 18 years who received one or more TEE examinations on ECMO or ECLS therapy during their stay in the Intensive Care Unit (ICU) between 2011 and 2013 were reviewed. A total of 87 separate TEE examinations, including probe insertion and removal, were performed in these patients. A total of 145 ECLS systems were implanted during the study period, but only TEE exams performed in the ICU were analyzed. TEE was performed at the discretion of an interdisciplinary care team and was indicated either because transthoracic echocardiography (TTE) was not possible due to inadequate acoustic windows or because TTE failed to visualize the targeted cardiac structures. The TEE exams were exclusively performed by experienced attending intensivists, board-certified in perioperative TEE.
Indications for ECLS initiation included cardiogenic shock following myocardial ischemia, myocarditis, failure to wean from CPB after valve surgery and aortic dissection repair, low cardiac output state after pulmonary embolism, myocarditis, post partum cardiomyopathy and mediastinal mass syndrome. Indications for ECMO included sepsis with concomitant acute respiratory distress syndrome (ARDS) and H1N1-associated respiratory failure.
The control group consisted of age- and gender-matched patients undergoing non-emergent cardiac surgery requiring routine TEE exams (Table 1).
Demographic data, indications for ECLS and surgical procedures.
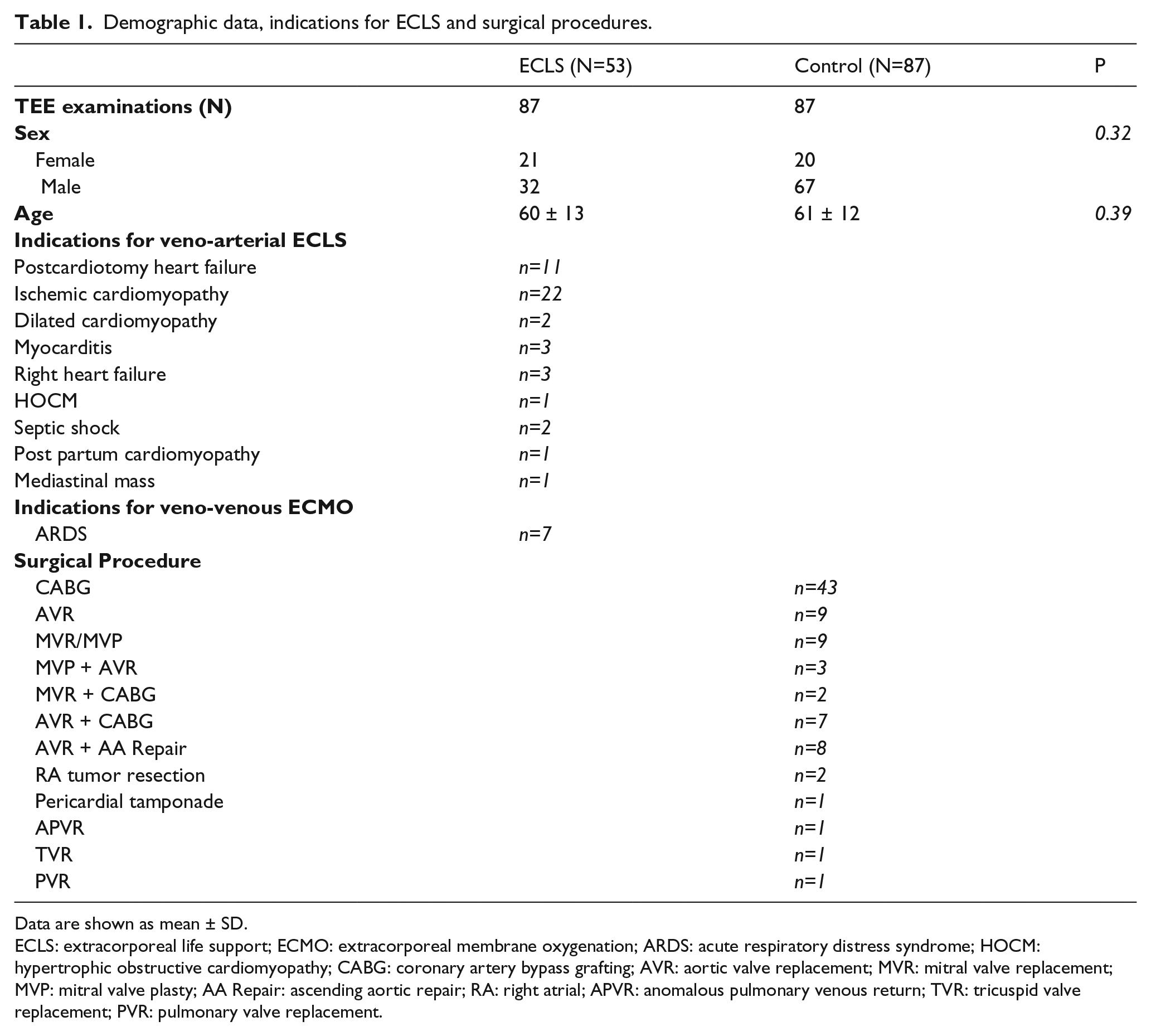
Data are shown as mean ± SD.
ECLS: extracorporeal life support; ECMO: extracorporeal membrane oxygenation; ARDS: acute respiratory distress syndrome; HOCM: hypertrophic obstructive cardiomyopathy; CABG: coronary artery bypass grafting; AVR: aortic valve replacement; MVR: mitral valve replacement; MVP: mitral valve plasty; AA Repair: ascending aortic repair; RA: right atrial; APVR: anomalous pulmonary venous return; TVR: tricuspid valve replacement; PVR: pulmonary valve replacement.
All information on TEE-associated complications was collected prospectively and was retrospectively assessed by review of electronic patient charts, daily attending physician and nursing notes as well as surgical morbidity and mortality data. A complication log linked to each TEE exam was established for each patient from start until discontinuation of ECLS. Complications were assessed before and after TEE probe placement and removal and consisted of the following parameters: diffuse oral bleeding, upper gastrointestinal hemorrhage, esophageal perforation, dental injury, endotracheal tube malposition or dislodgement and odynophagia (when assessment was possible). Bleeding complications were graded as ‘minor’ by detailed chart review (MNM, HM, JNH) and the absence of subsequent therapeutic interventions.
Transesophageal echocardiography (TEE)
In the study group, TEE examinations were performed exclusively in intubated and sedated, non-paralyzed patients. In the control group, TEE exams took place after the induction of anesthesia and concomitant use of muscle relaxants. After placement of upper and lower tooth guards, a lubricated multiplane transducer TEE probe (Philips S7-2t Omni or Philips X7-2t Matrix, Philips Healthcare, Inc., Andover, MA) was placed into the esophagus. The use of direct laryngoscopy to facilitate insertion was based on operator preference. The procedure was immediately abandoned when resistance was met during probe placement or advancement. All exams were performed or supervised by the attending cardiac anesthesiologists or intensivists with extensive experience in perioperative TEE.
Laboratory coagulation studies and anticoagulation
Routine coagulation tests were evaluated within two hours prior to TEE probe insertion and consisted of prothrombin time (INR), activated partial thromboplastin time (aPTT) and platelet count. The respective anticoagulation regimen at the time of TEE was recorded and consisted of intravenous heparin infusion, argatroban infusion, epoprostenol sodium infusion or no systemic anticoagulants. Moreover, the concomitant use of platelet-inhibiting drugs was recorded.
Statistical Analysis
Results are expressed as mean ± standard deviation (SD). Groups were compared by Student’s t tests. P<0.05 was considered significant.
Results
The overall morbidity attributable to TEE in this study on ECLS patients was 2.3% (2/87 TEE exams). Both complications were described as ‘minor’ diffuse oropharyngeal bleeding (Table 2). Probe insertion and handling was reportedly uncomplicated in both cases (HM, JNH) and the patients were treated conservatively without the need for surgical or procedural intervention. Of note, neither of the patients with oropharyngeal bleeding underwent repetitive TEE exams. Among the patients who received more than one TEE exam, no case of oropharyngeal bleeding was witnessed. Two study patients were diagnosed with upper gastrointestinal hemorrhage by esophagogastroduodenoscopy prior to the TEE exam and were medically cleared in advance. No esophageal perforations, dental injuries or dislodged endotracheal tubes were reported in our patient population (Table 2).
Complications related to TEE examination.
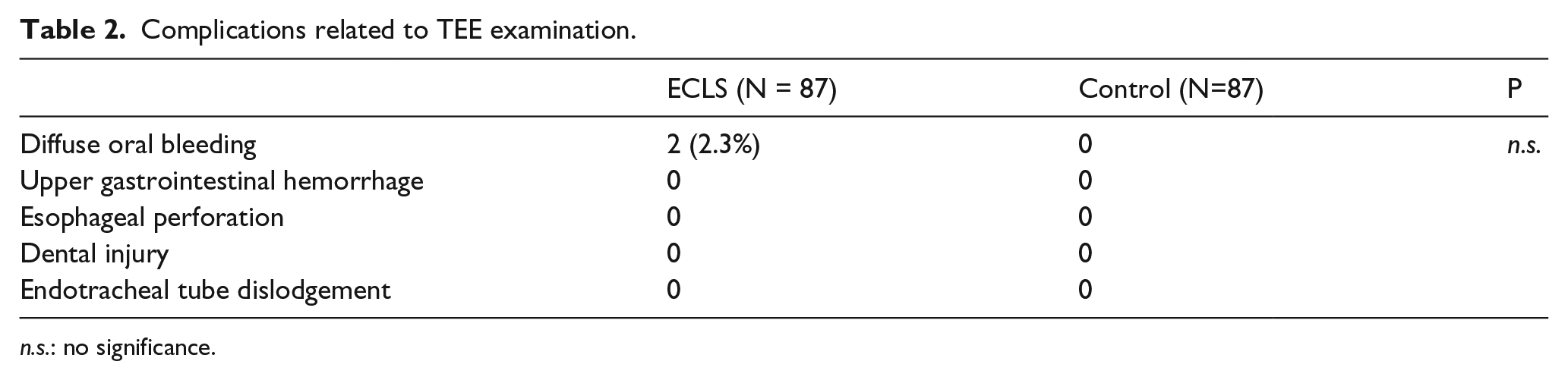
n.s.: no significance.
Profiles of plasmatic coagulation were measured and recorded within 2 hours prior to TEE probe insertion. In the study group, the mean aPTT at the time of TEE probe insertion and removal was 61 ± 30.4 s (range 28-160 s) compared to 25.0 ± 3.5 s in the control group (p< 0.001); the mean INR was 1.44 ± 0.3 (range 0.9-2.6) compared to 1.0 ± 0.2 (p<0.001). The mean platelet count was 109 ± 63.8 x109/L (range 21-287 x109/L) in the study group, which was significantly deranged lower than the controls (227 ± 63.7 x109/L, p<0.001) (Table 3).
Plasmatic coagulation studies prior to TEE probe insertion.
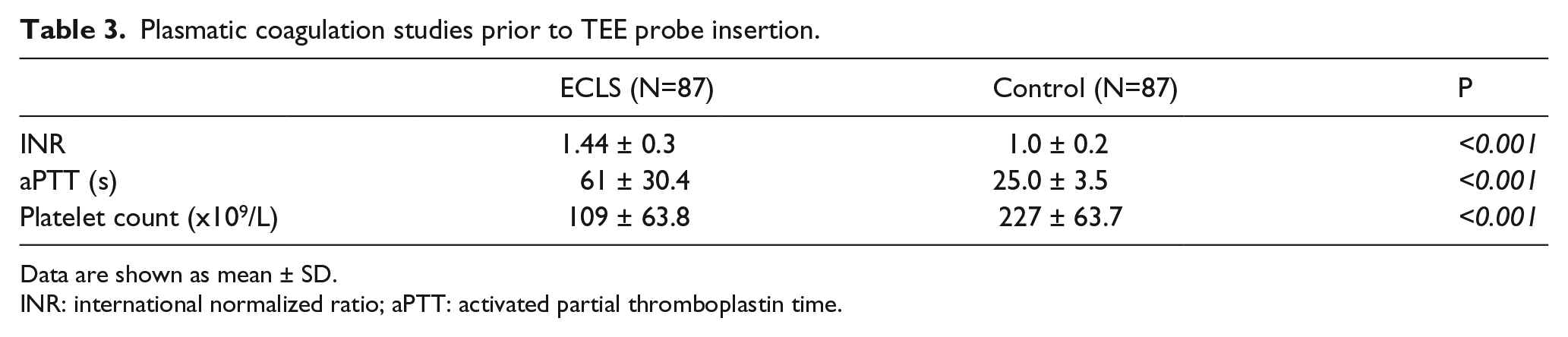
Data are shown as mean ± SD.
INR: international normalized ratio; aPTT: activated partial thromboplastin time.
Sixty-nine of 87 patients (79%) received a continuous heparin infusion to achieve the goal aPTT of 50-60 s. Six patients (6.8%) received a continuous infusion of argatroban due to anti-PF4 antibody positive heparin-induced thrombocytopenia (HIT) screening tests. Three patients (3.4%) received a continuous infusion of epoprostenol sodium during renal replacement therapy on ECLS. Nine patients (10.3%) were not systemically anticoagulated during their TEE exam because of pre-existing bleeding complications and an already deranged plasmatic coagulation profile.
Both patients with diffuse oropharyngeal bleeding had received heparin for anticoagulation. Seven study patients (8%) had received additional anticoagulant medications within 5 days prior to the TEE exam. These consisted of activated protein C (1 patient), abciximab + ticagrelor + aspirin (1 patient), recombinant tissue plasminogen activator (1 patient), aspirin + coumadin (1 patient), aspirin + clopidogrel (2 patients) and coumadin only (1 patient). Interestingly, none of these seven patients experienced TEE-associated bleeding complications.
Discussion
TEE is a safe diagnostic tool widely used in clinical practice.14,15 The overall reported incidences of TEE-related complications range between 0-0.5%, with mortality rates between 0-0.02%. 2 The majority of complications arise from minor oropharyngeal injuries (0-0.2%) which account for up to 13% of all complications.3,16 Available literature stems mostly from investigations in either ambulatory patients or in paralyzed (cardiac) surgical patients when TEE probes are inserted intraoperatively under ideal conditions after the induction of anesthesia, the use of muscle relaxants and before the initiation of systemic anticoagulation, thus, normal coagulation studies. Very little data exists on TEE-related complications in the subset of critically ill patients and the unique challenges of TEE probe handling in anticoagulated patients on ECLS have not been investigated to date.17,18 Therefore, judging the risk of trauma or bleeding from TEE probe placement in patients under therapeutic systemic anticoagulation remains a clinical controversy. Nevertheless, the American Society of Anesthesiologists’ practice guidelines for perioperative TEE recommend TEE to be used whenever diagnostic information which is expected to alter management cannot be obtained by TTE or other modalities in a timely manner.19,20
Our study found mild oropharyngeal bleeding in 2/87 TEE exams in ECLS patients and none in the control group with normal coagulation tests. The incidence of 2.3% of oropharyngeal bleeding in our study group is slightly higher than previously reported in the literature on routine TEE use. It is important to state, however, that the hemorrhagic complications remained self-limited and clinically insignificant and no major complications impacting patient outcome occurred. Also, the incidence of oropharyngeal bleeding seemed unchanged when anticoagulated patients had to undergo multiple TEE exams with separate TEE probe manipulations.
A large study on intraoperative TEE complications reported morbidity and mortality rates of 0.2% and 0%, respectively, in 7200 cardiac surgical patients. 3 The most common TEE-associated complications were severe odynophagia (0.1% of the study population), dental injury (0.03%), periprocedural endotracheal tube malposition (0.03%), upper gastrointestinal hemorrhage (0.03%) and esophageal perforation (0.01%). Probe placement was performed solely in anesthetized and paralyzed patients and occurred before systemic anticoagulation for cardiopulmonary bypass and the probe was removed after systemic anticoagulation was fully reversed. Another multicenter survey of 10,419 patients undergoing TEE under conscious sedation and, thus, able to aid probe placement by active swallowing, reported similarly low complication rates of 0.18%, but included one mortality. 1 In our study, no major complications were found from TEE probe insertion or removal other than an increased incidence of mild, self-limited, oropharyngeal bleeding. The differences in patient populations and clinical settings between operating room and intensive care unit could explain the higher proportion of oropharyngeal bleeding. Additionally, in ECLS patients, TEE exams often have to be performed before coagulopathies are effectively corrected or while patients are systemically anticoagulated. It is, therefore, not entirely surprising that we experienced significantly higher rates of oropharyngeal bleeding in this patient population. Of note, the occurrence of oropharyngeal bleeding was not increased in the patients who underwent repeated TEE exams with multiple probe placements. Reassuringly, both the reported cases of perioral, pharyngeal or upper gastrointestinal tract bleeds were amenable to conservative management or were self-limited and resolved within a short time period. Both patients who experienced bleeding complications in our population had two or more abnormal coagulation tests prior to TEE probe manipulation. In order to confirm whether the risk of bleeding increases in relation to the number of abnormal coagulation tests or whether there is prognostic value in certain coagulation tests over others, larger studies and patient cohorts are needed.
All TEE examinations in our patient cohort were performed because TTE quality was suboptimal due to inadequate acoustic windows or failure to visualize the targeted cardiac structures. In contrast to patients under conscious sedation who can facilitate TEE probe insertion by actively swallowing, we analyzed a sedated, critically ill, ECLS patient cohort. Neuromuscular blockade or heavy sedation leads to oropharyngeal space collapse and probe passage can become more difficult and could be another reason for the reported higher rates of oral bleeding.2,26
Limitations of our analysis are the relatively small size of the study cohort and the retrospective, observational nature of our analysis. Our focus on ECLS patients in this single-center setting, however, rendered the inclusion of a larger patient population difficult. Secondly, the known paucity of complication events with TEE makes it difficult to draw steadfast conclusions. Nevertheless, we believe that reporting our increased complication rate in ECLS patients compared to the available literature is still important.
Conclusions
In this observational study, TEE remained a safe imaging modality, even in patients during ECLS therapy. Despite underlying critical illness, coagulopathies and systemic anticoagulation, no major complications and morbidity (i.e., esophageal injury, lower gastrointestinal bleeding) compared to a control group was found. Two-point-three percent of ECLS patients, however, suffered minor self-limiting oropharyngeal bleeding associated with TEE probe manipulation. These numbers represent a higher incidence of bleeding complications than previously published with routine TEE use. Thus, the indications for TEE exams in ECLS patients should be critically discussed on a case-by-case basis.
Footnotes
Authors’ Contributions
Conceived and designed the experiments: JNH, HM, PR, MN-M. Performed the experiments: MN-M, CC, HM, JNH, ES, HAH. Analyzed the data: HM, JNH, PR, CS, MN-M. Wrote the paper: MN-M, JNH. The authors attest to having approved the final manuscript and the integrity of the original data and the analysis reported in the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Departmental funding, Eberhard Karls University, Tübingen, Germany. The funder had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.