
Abstract
Haemolysis, thrombosis and haemorrhage are well-documented complications of extracorporeal membrane oxygenation. This case report outlines an unusual case of haemolysis, thought secondary to a large mobile thrombus in the inferior vena cava.
Keywords
Introduction
Although extracorporeal membrane oxygenation (ECMO) may be a lifesaving measure in patients with severe cardiac or respiratory failure, 1 it has a high rate of complications, including bleeding (33%), haemolysis (18%) and venous microthrombosis (10%). 2 Haemolysis during ECMO support occurs due to erythrocyte trauma, especially from turbulent circuit flow.3-6 Turbulent flow can occur due to partial obstruction of the ECMO cannulae (e.g. with thrombus), fluctuating flow in the (negative pressure) access line from the patient or fibrin deposition in the centrifugal pump head.
The ECMO circuit (pump and oxygenator) should be changed if haemolysis occurs. 5 However, in the case presented, haemolysis persisted despite changing the ECMO circuit and replacing the cannulae. The cause of the haemolysis was ultimately ascribed to mobile thrombus formation in the inferior vena cava (IVC). This has not previously been reported as a cause of haemolysis in patients on ECMO support and should, therefore, be considered when other causes have been excluded.
Case report
A 33-year-old male patient was commenced on veno-venous ECMO support for severe acute respiratory distress syndrome. This was established via a femoro-jugular circuit (23Fr right femoral vein to 18Fr right internal jugular), using a Rotaflow pump and a Quadrox D oxygenator (all from Maquet, Getthinge, Germany). The patient was anticoagulated with heparin to a target activated partial thromboplatin time (APTT) of 50-70. However, this was ceased on day three of ECMO due to significant posterior pharyngeal bleeding which persisted despite nasopharyngeal packing and tranexamic acid administration and required the transfusion of two units of packed red cells. Heparin was recommenced 48 hours later, with no further bleeding.
On day six of ECMO (24 h post recommencement of heparin), the patient had clinical evidence of haemolysis (dark brown urine). The plasma free haemoglobin was significantly elevated (0.6 g/L, normal <0.1 g/L) as was his LDH (lactate dehydrogenase). The ECMO circuit was changed the following day, the right femoral access cannula was removed and a new 23Fr access cannula was inserted into the IVC via the left femoral vein. The ECMO pump, oxygenator and explanted cannula were drained and were all normal on inspection. However, there was only partial resolution of the haemolysis, subsequently, with a further increase in plasma free haemoglobin on day 11 of ECMO support (Figure 1)
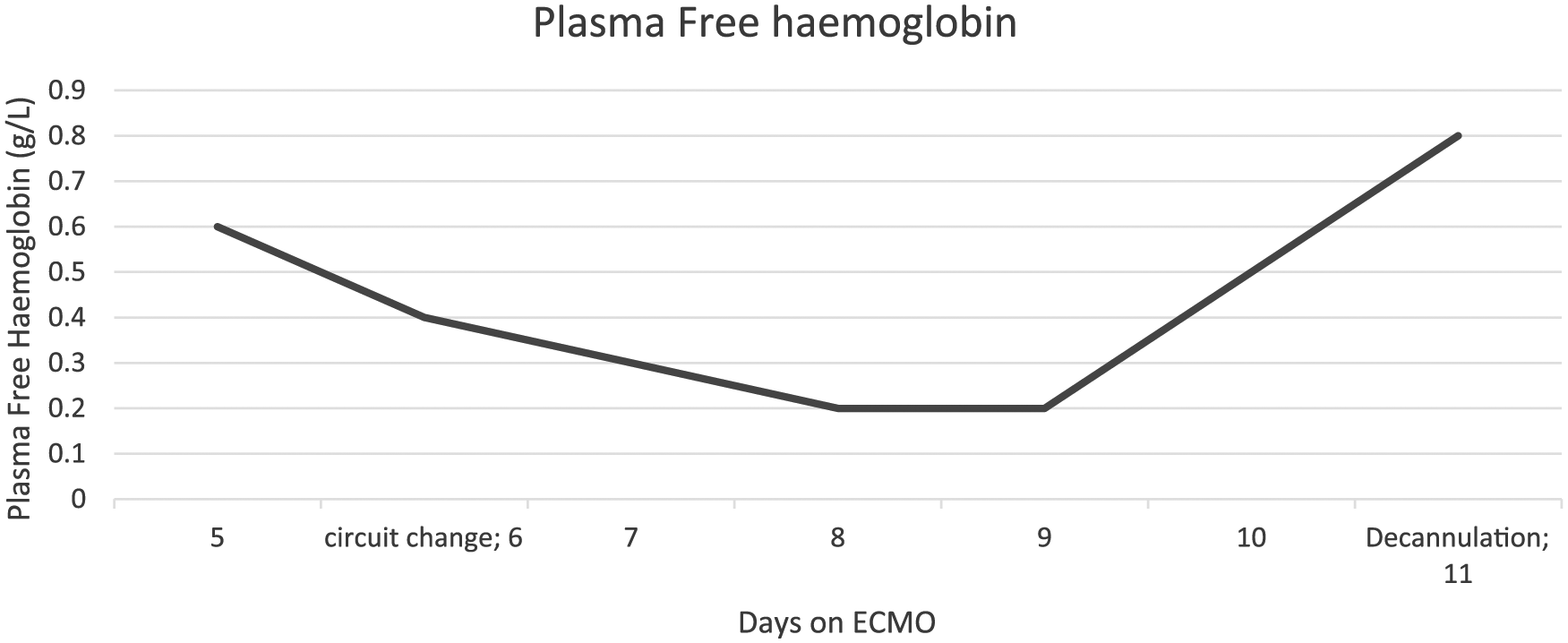
Plasma free haemoglobin levels.
Transoesophageal echocardiography (TOE) at that time revealed a large mobile thrombus in the intrahepatic vein which was flipping in and out of the tip of the access cannula (Figure 2 and Figure 3) and impeding venous flow.
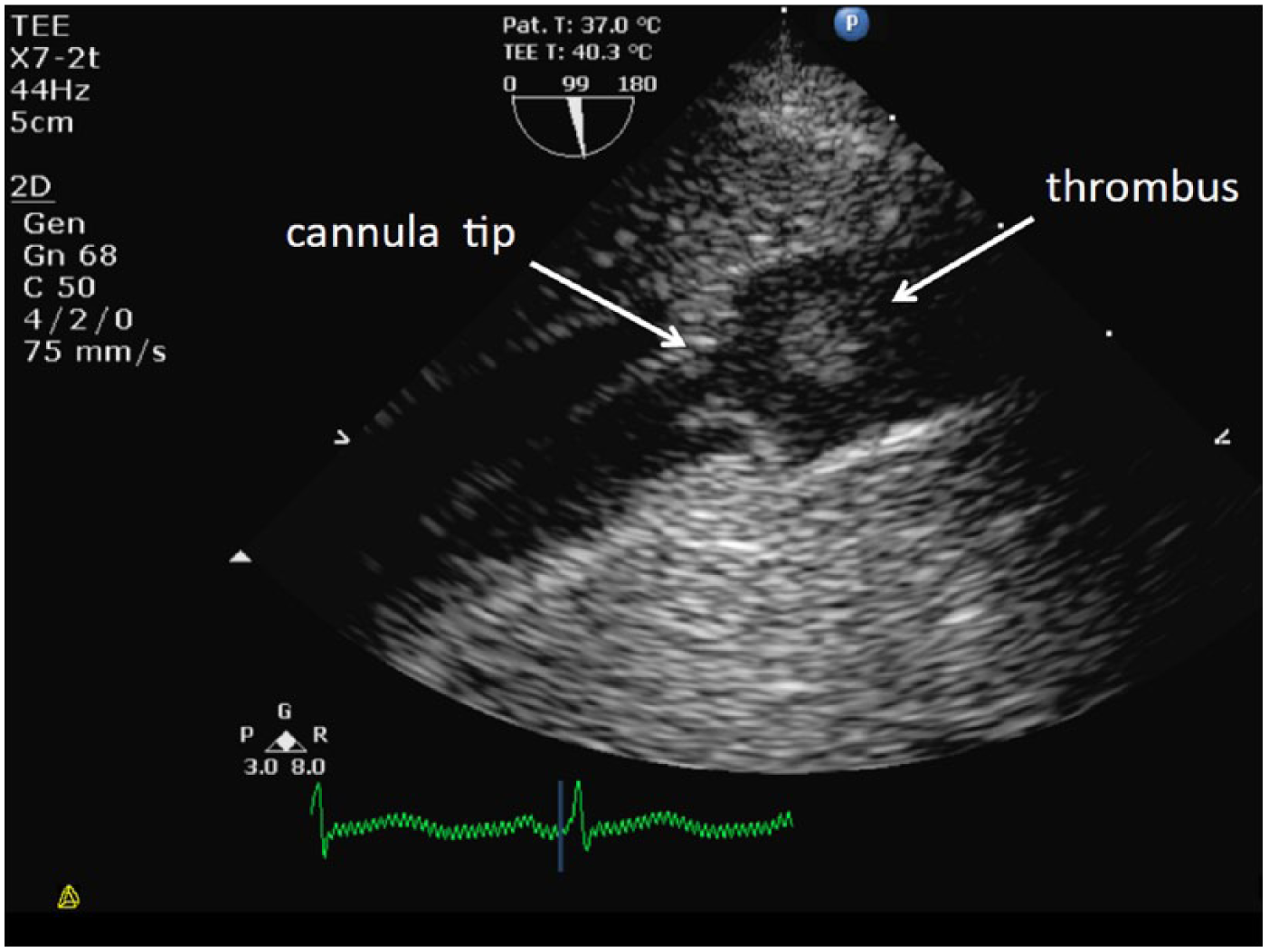
Thrombus above cannula tip in the inferior vena cava (IVC).
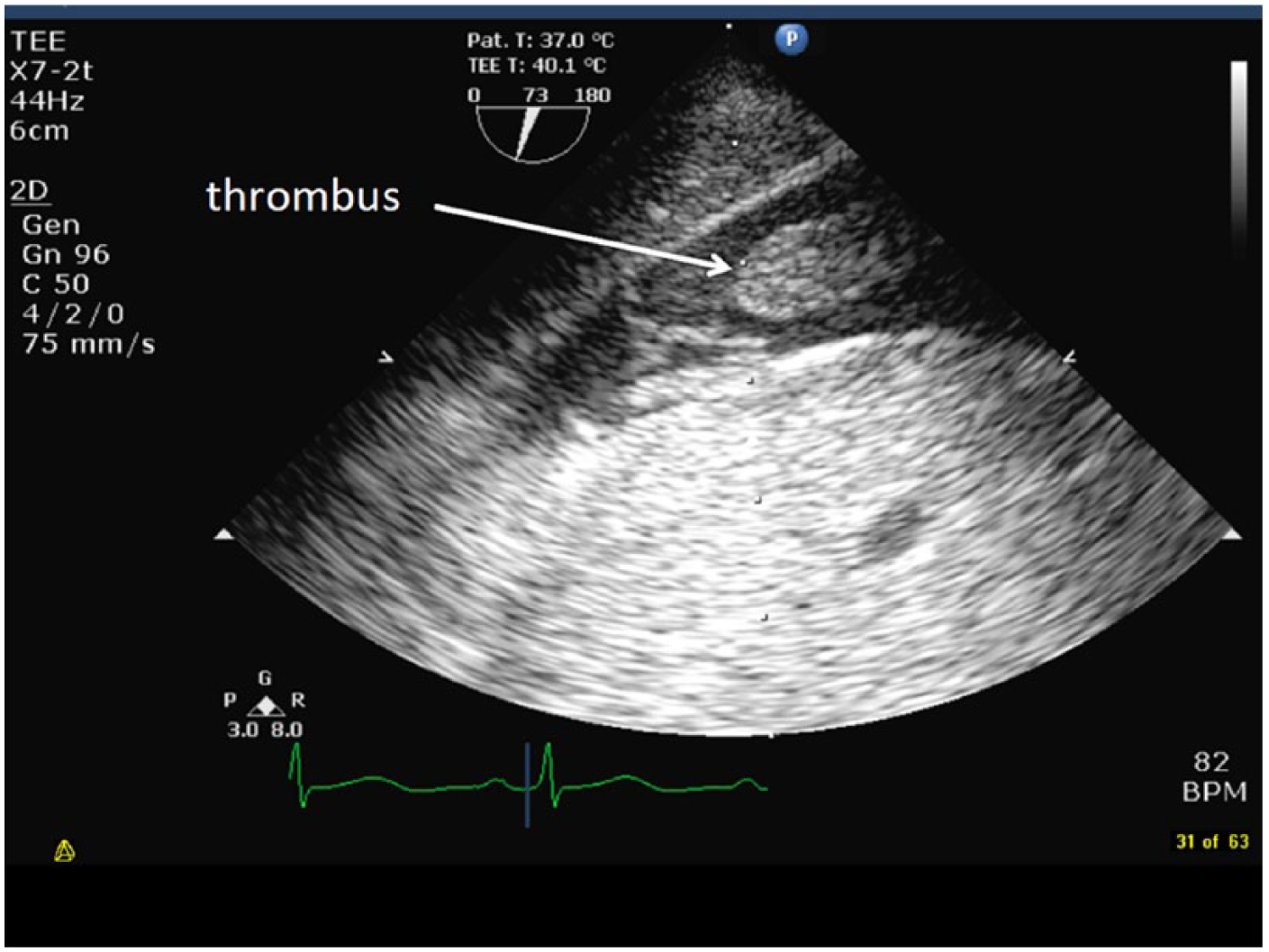
Thrombus post decannulation.
The patient was successfully weaned from ECMO the same day and decannulated; once again, the ECMO pump, oxygenator, circuit and cannulae revealed no thrombus formation within the circuit. Intravenous heparin was recommenced. He subsequently made an uneventful recovery and was discharged on day 32 on warfarin.
Discussion
Haemolysis is a common complication of ECMO support. It is caused by erythrocyte trauma which is exacerbated by turbulent flow within the circuit or cannulae.3-5 Usually, haemolysis rapidly resolves after changing the circuit, with the return of normal plasma free haemoglobin levels (<0.1 g/L), hence, persisting haemolysis suggests that the cannulae may be responsible. 3 In this case, however, it did not resolve, despite changing both the circuit and cannulae. The finding of a large mobile thrombus in the intrahepatic IVC was thought to have caused haemolysis in our patient by creating turbulent flow in the access cannula.5,6
This case highlights the common clinical challenge of finding the right balance between the risks of thrombus formation and bleeding in ECMO patients. Initiation of ECMO support causes consumption and dilution of clotting factors. 7 Thrombi form within the circuit in areas of low flow, 8 hence, systemic heparinisation is recommended to prevent clot formation, both within the circuit and the patient. 7 However, if significant bleeding occurs, heparin may need to be decreased or ceased.7,8 However, this will increase the risk of deep vein thrombosis and may also contribute to haemolysis in these patients.
Written informed consent was gained from the patient’s guardian prior to writing the case report.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.