
Abstract
Introduction
Cardiac surgery is fraught with increased consumption of blood and blood products. Various strategies for blood conservation have been described. Our aim was to study the impact of a structured blood conservation protocol (BCP) on the utilization of blood and patient outcome.
Methods
Retrospective analysis of prospectively collected data comparing adult patients undergoing open heart surgery with BCP with those undergoing surgery without BCP. The primary objective was to compare the amount of blood utilized and the hematocrit at discharge. The secondary objective was to compare the parameters of patient outcomes. The level of significance was set at 0.05.
Results
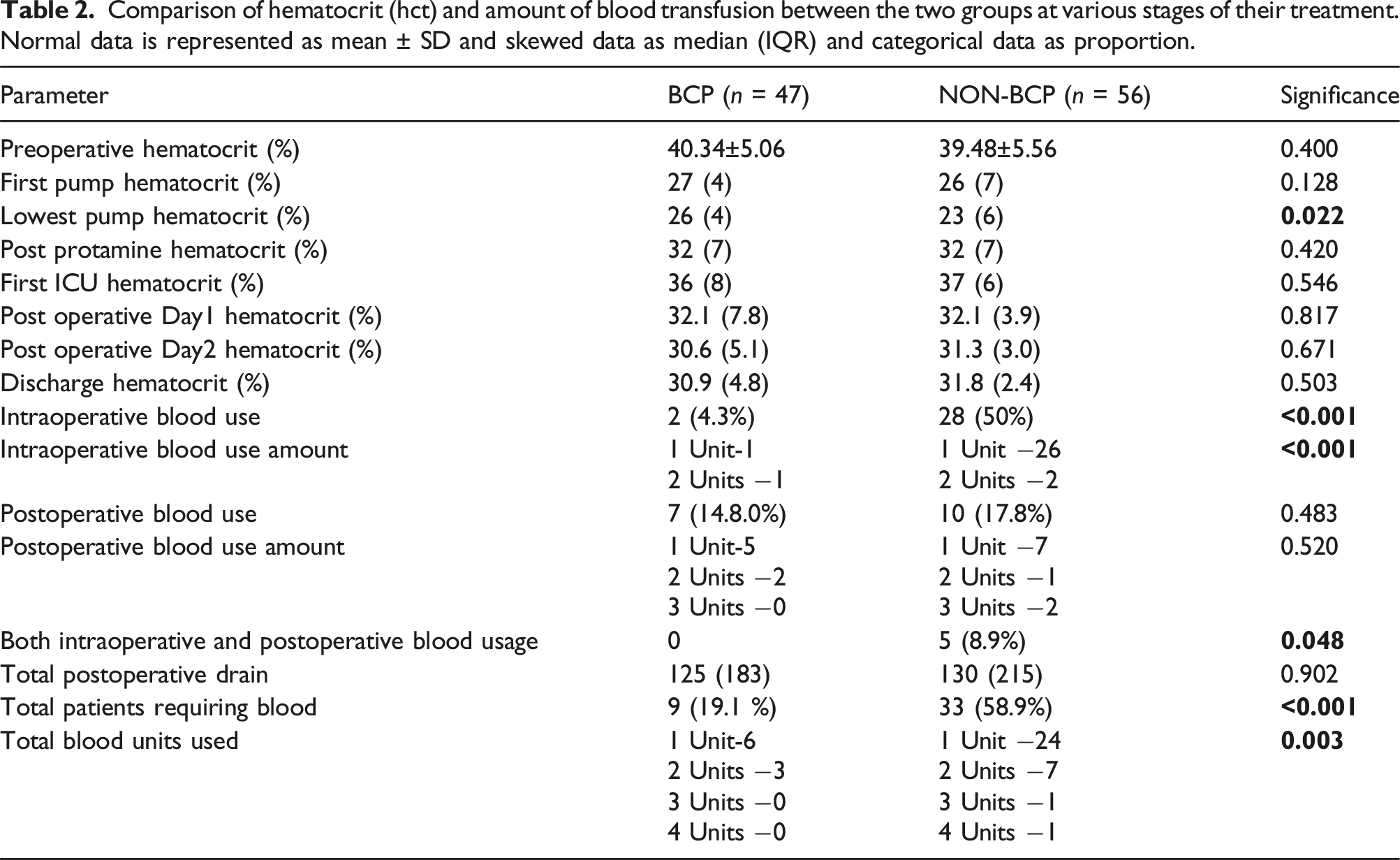
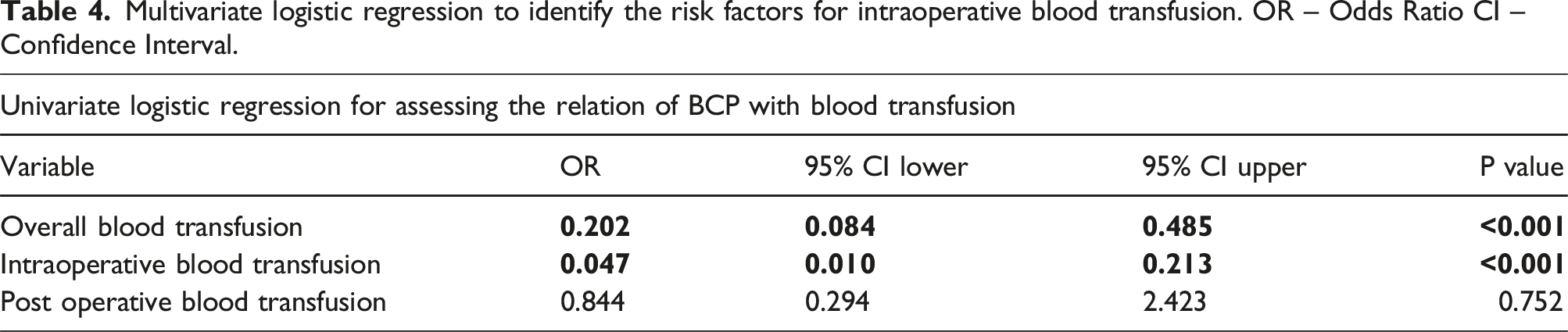
The proportion of patients requiring transfusion (19.1% [9/47] vs 58.9% [33/56]; p < 0.001) and the quantity of blood transfused (12 units vs 45 units; p 0.003) in the BCP group was significantly lower. Interestingly, the hematocrit level at discharge was comparable between the groups (30.9 (4.8) versus 31.8 (2.4), p-0.671). The average cost incurred for transfusing blood in the BCP group was ₹ 370.2 as compared to ₹1165.1 in the other (p < 0.001). BCP reduced the odds of overall blood transfusion by 79.8% (OR 0.202 (0.084-0.485); p < 0.001) and intraoperative blood transfusion by 95.3% (OR 0.047 (0.010-0.213); p < 0.001). The morbidity and mortality were comparable between the groups.
Conclusion
Implementing a structured blood conservation protocol in patients undergoing open heart surgery significantly reduces the need for blood transfusion. It also has a promising impact on patient recovery after surgery and significant positive cost implications.
Introduction
Cardiac surgery is a resource-intensive speciality and is fraught with increased consumption of blood and blood products. 1 This is often attributed to the use of cardiopulmonary bypass and the various strategies used to run the pump, high-pressure vascular suture lines which have a higher propensity to bleed and frequent use of anticoagulation. Blood is a precious resource, and its transfusion is known to increase patient morbidity and mortality and has significant cost implications.2–6
Immediate, early, and late adverse outcomes of blood transfusion have already been described.2–5,7 Techniques like using anti-fibrinolytic agents, retrograde autologous priming, miniaturization of cardiopulmonary bypass circuit, minimizing on-pump hemodilution and restrictive strategy of blood transfusion in the postoperative period have been described to reduce the utilization of blood.1,3,5,8–14
Most of the studies performed to evaluate the risk factors that lead to an increase in blood transfusion and its effect on patient outcomes are retrospective in nature. The few large prospective studies performed, evaluate the effect of a particular strategy of blood conservation on patient outcomes. And it has been observed that retrospective studies demonstrate worse outcomes with transfusion, probably related to the selection bias. 15
We have designed this study to prospectively assess the impact of a structured blood conservation protocol on the utilization of blood in the treatment of patients undergoing cardiac surgery and study their immediate outcomes. Also, to compare it with patients undergoing cardiac surgery without a blood conservation protocol.
Aims and objectives
The study aimed to assess the effect of structured blood conservation protocol on the consumption of blood and the outcome of patients undergoing open heart surgery. The primary objective was to compare the amount of blood used and hematocrit level at discharge between adult patients who underwent open heart surgery with blood conservation protocol versus those who underwent surgery without blood conservation protocol. The secondary objectives were to compare the effect of blood conservation protocol on the postoperative recovery (vasoactive inotrope score, duration of inotrope use, duration of mechanical ventilation, duration of ICU stay, and duration of hospital stay), cost implications, morbidity (surgical site infection, stroke, requirement of dialysis) and mortality. Also, the strength of association and relation of the various components of the blood conservation protocol on the significant patient outcome parameters was studied.
Methodology
The study was performed in the Department of Cardiothoracic and Vascular Surgery, Sri Sathya Sai Institute of Higher Medical Sciences, Bangalore, India, after ethical committee approval (ECR/1407/Inst/KA/2020).
Inclusion criteria
All adult patients aged more than 18 years undergoing open heart surgery were included in the study.
Exclusion criteria
1. Blood prime used in the cardiopulmonary bypass circuit. 2. Cyanotic congenital heart disease
Blood conservation protocol
Two operating surgeon out of the six at our centre performed surgery using blood conservation protocol, which included Intraoperative blood conservation strategy Patients were administered Epsilon amino caproic acid (50 mg/kg) before performing sternotomy. After cannulation, retrograde autologous priming was performed and the volume of the same was recorded. Myocardial protection was achieved using St Thomas cardioplegia or Modified Del Nido blood cardioplegia (Blood from the reservoir with Del Nido cardioplegia). No hemofilter was used. After weaning from cardiopulmonary bypass, the blood remaining in the reservoir, oxygenator and arterial line was returned back to the patient and this volume was recorded. The threshold for adding blood on cardiopulmonary bypass was a hematocrit of less than 24. After completion of protamine, Epsilon amino caproic acid (50 mg/kg) was administered again. Postoperative blood transfusion threshold Blood was transfused in the postoperative period if the hematocrit was less than 27%.
Surgery without blood conservation protocol
Four operating surgeons out of the six at our centre performed surgery without blood conservation protocol, which included Intraoperative strategy Pre-sternotomy and post-protamine epsilon amino caproic acid was used at surgeon’s discretion. Retrograde autologous priming and post-cardiopulmonary bypass transfusing the blood remaining in the oxygenator and pump were performed at surgeon’s discretion. Cardioplegia options for myocardial protection included St Thomas cardioplegia, Del Nido cardioplegia and modified Del Nido blood cardioplegia (blood from the reservoir with Del Nido cardioplegia). No hemofilter was used. The threshold for adding blood on cardiopulmonary bypass was a hematocrit of less than 24. Postoperative blood transfusion threshold Blood was transfused in the postoperative period if the hematocrit was less than 27%.
Data collection
All the data were collected prospectively and recorded in Microsoft Excel (Version 16.65).
Statistical analysis
Data were entered into Microsoft Excel (Version 16.65) and analyzed using the statistical software SPSS (Version 28.0). The Kolmogorov-Smirnov test was used to check the normality of the data. Normal data were represented as mean ± standard deviation and descriptive statistics of skewed data were represented as median (interquartile range). Categorical data were expressed as proportions. Student t-test was used to compare continuous data between normally distributed variables and the independent-sample Mann-Whitney U test was used to compare the continuous variables between the two groups with skewed distribution. Pearson Chi-square test was used to compare categorical variables between the two groups. Univariate and multivariate logistic regression was used to study the association of the need for blood transfusion with risk factors. Univariate and multivariate linear regression was used to study the relation of significant continuous outcome variables with risk factors. Kaplan-Meier plots were used to study the time to discharge after surgery and the Mantel-Cox log-rank test was used to compare the difference between the groups. Patient death was censored. The level of significance was set at 0.05.
Results
From June 1, 2022, to November 30, 2022, a total of 582 patients underwent cardiac surgery at our unit. The inclusion criteria were met by 103 patients, with 47 (46.6%) patients undergoing cardiac surgery with blood conservation protocol and 56 (53.4%) patients undergoing cardiac surgery without blood conservation protocol. The remaining patients were excluded as 209 patients underwent off-pump coronary artery bypass grafting, 126 patients were less than 18 years of age, 113 patients had cyanotic congenital heart disease and 31 patients required blood priming.
Preoperative and intraoperative parameters of the two groups of patients. Normal data is represented as mean ± SD and skewed data as median (IQR) and categorical data as proportion.
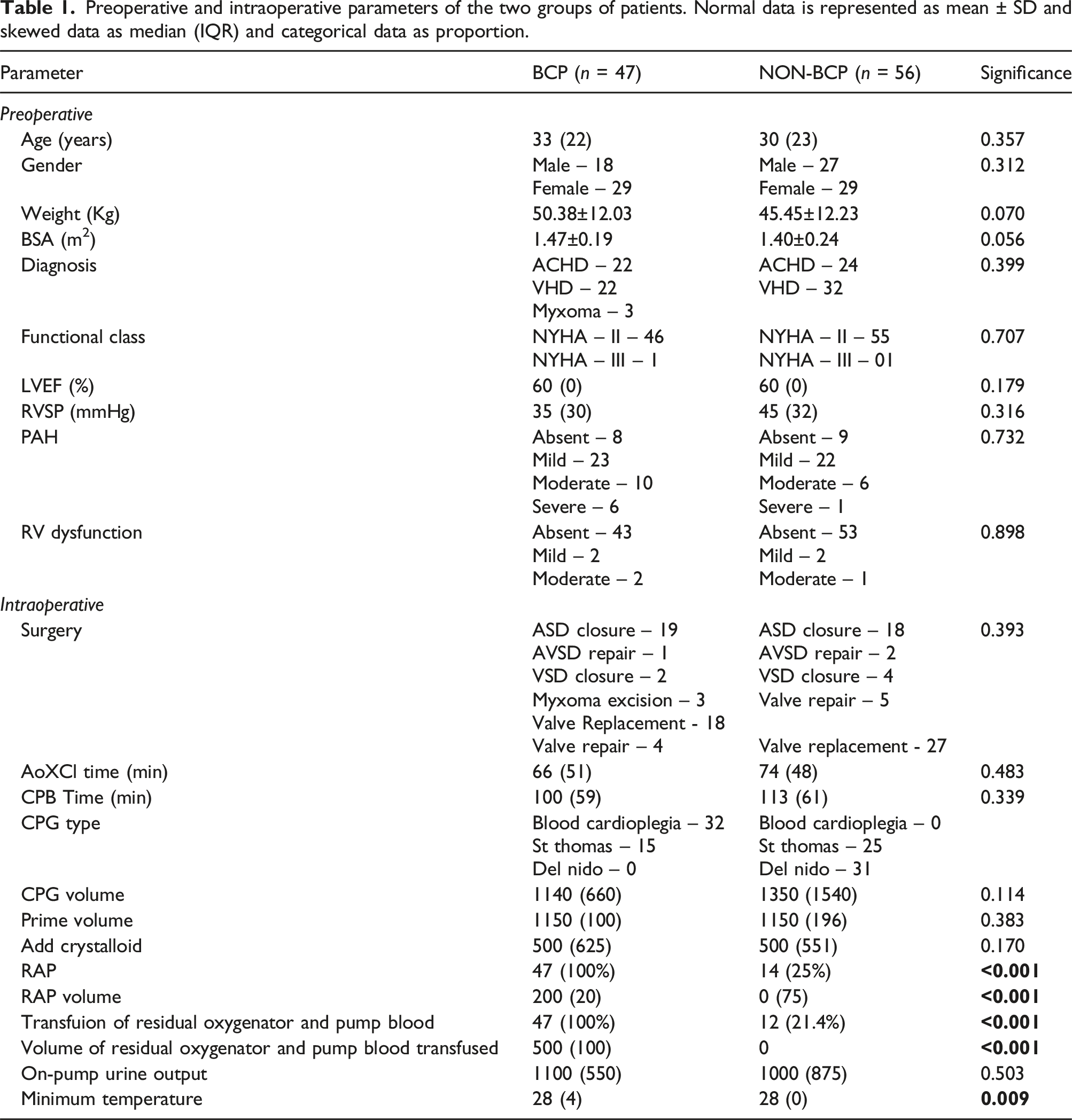
Patients in both groups were comparable in terms of the surgeries performed and the time taken to perform the procedure (clamp time and the cardiopulmonary bypass time). RAP was performed in all patients undergoing surgery with BCP compared to only 25% of patients undergoing surgery without BCP (p < 0.001) and there was also a significant difference in the volume of RAP done in the two groups (p < 0.001). Similarly, the proportion of patients in whom the remaining pump volume was transfused back to the patient was significantly more in the BCP group (100% vs 21.4%; p < 0.001) (Table 1).
Comparison of hematocrit (hct) and amount of blood transfusion between the two groups at various stages of their treatment. Normal data is represented as mean ± SD and skewed data as median (IQR) and categorical data as proportion.
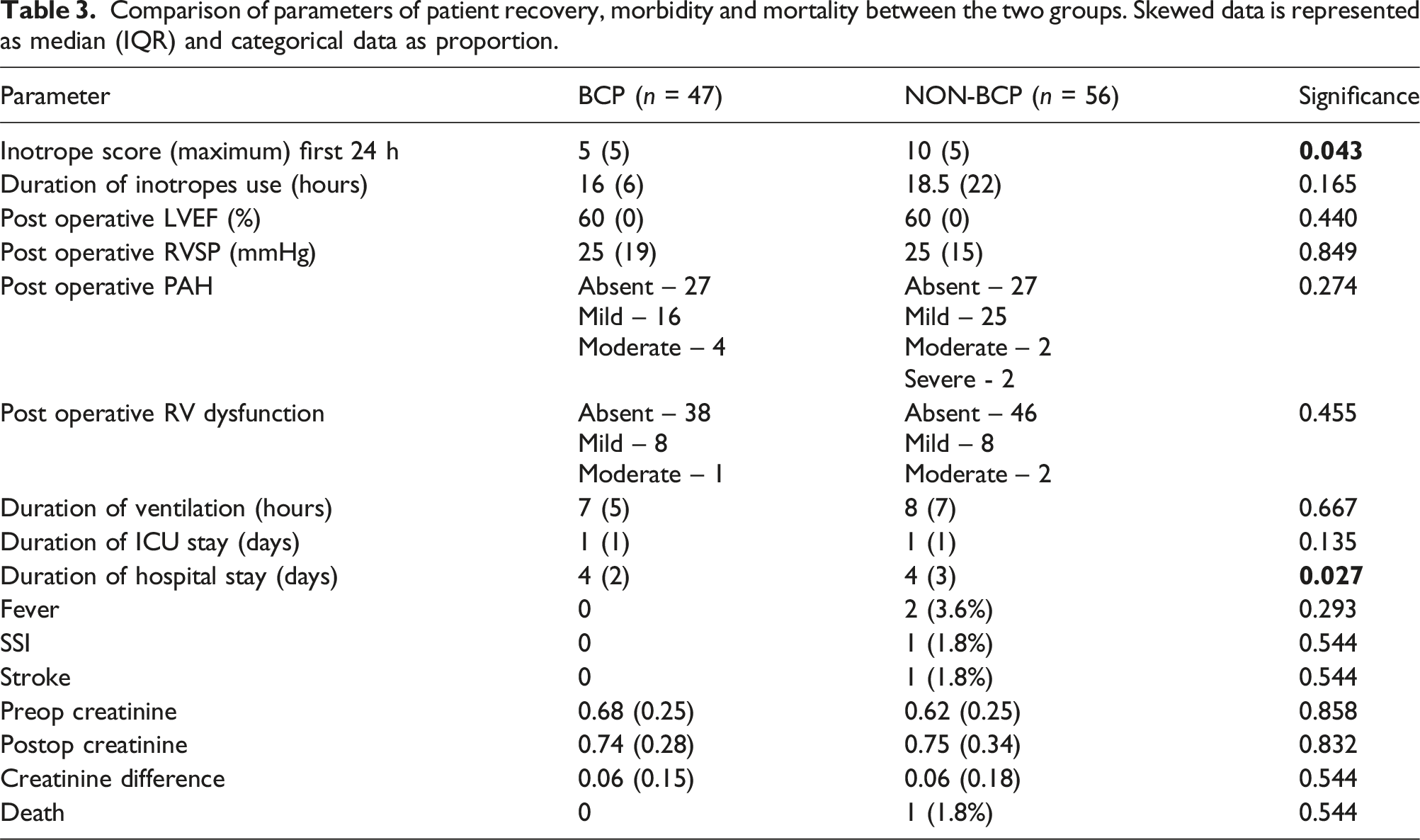
Comparison of parameters of patient recovery, morbidity and mortality between the two groups. Skewed data is represented as median (IQR) and categorical data as proportion.
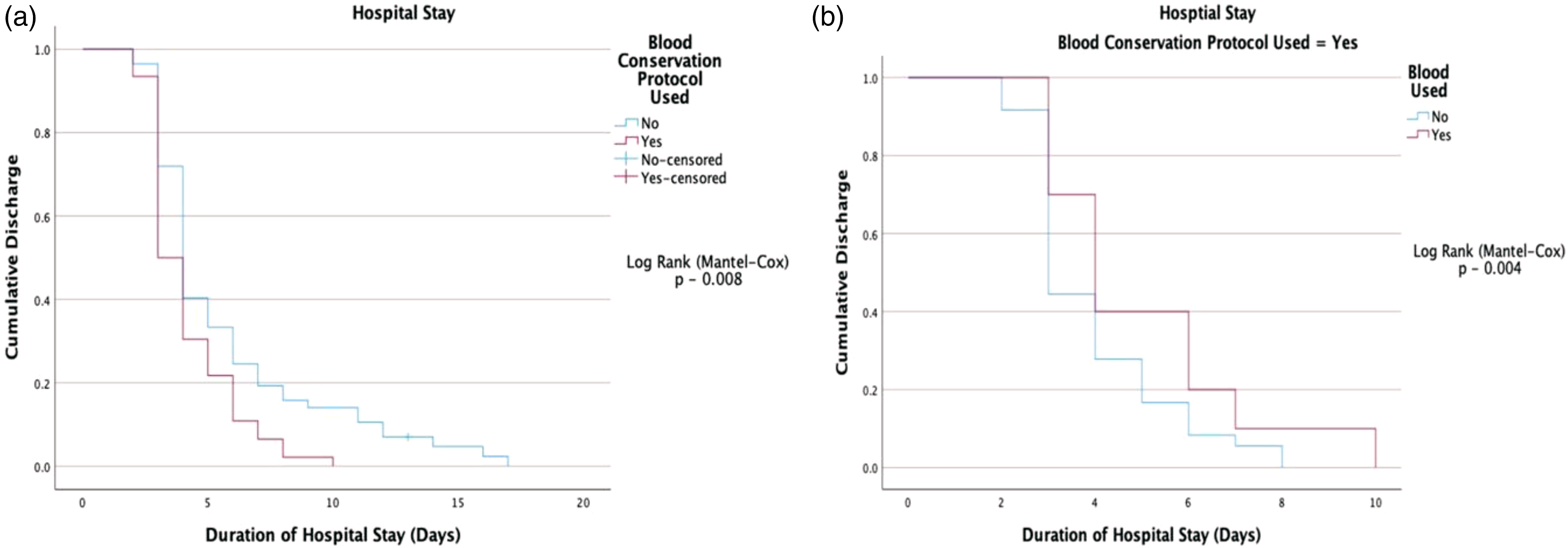
(a)Kaplan-Meier plots demonstrating a significantly shorter duration of hospital stay in patients following BCP. (b) - Subgroup analysis in the BCP group, demonstrating longer time to discharge in patients who received blood transfusion.
Two patients had a postoperative fever, one had a surgical site infection, and one had an ischemic stroke, and all these patients underwent surgery without BCP, however, this occurrence was not statistically significant. The preoperative, and postoperative creatinine levels were comparable between the groups and none of the patients required renal replacement therapy (Table 3). There was one mortality, the patient underwent ASD closure without BCP and had a thrombotic stroke which had a hemorrhagic transformation followed by brainstem herniation. This patient had received 3 units of blood transfusion.
The cost of 1 unit of packed red blood cells in India as per the Indian Red Cross Society database is ₹ 1450. 16 Excluding the overhead charges of storage and administration of blood, the average cost incurred for transfusing blood in the BCP group was ₹ 370.2 as compared to ₹1165.1 in the other (p < 0.001)
Multivariate logistic regression to identify the risk factors for intraoperative blood transfusion. OR – Odds Ratio CI – Confidence Interval.
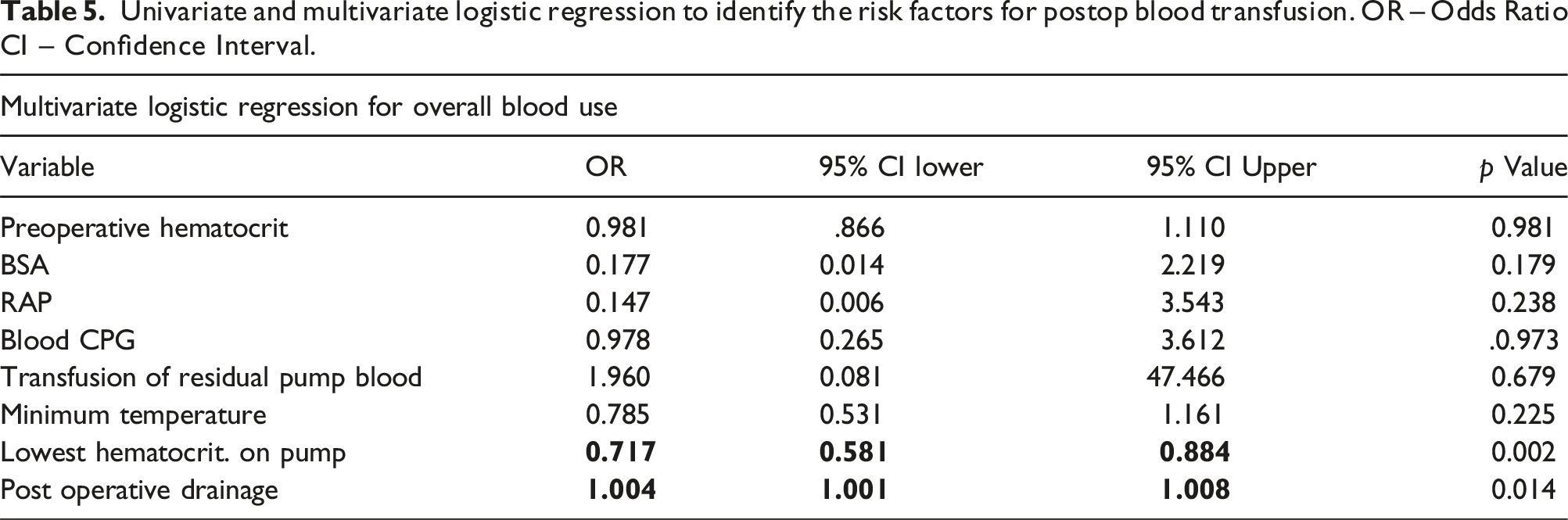
Univariate and multivariate logistic regression to identify the risk factors for postop blood transfusion. OR – Odds Ratio CI – Confidence Interval.
Discussion
Patients undergoing cardiac surgery are among the highest recipients of blood transfusion, with most of the hospital blood supply used by this group. 1 Our study demonstrates the impact of a structured blood conservation protocol on the consumption of blood and patient outcome.
Blood utilization
Also, the volume of blood transfused in this group was significantly lower than that in the comparison group (12 units vs 45 units). It was interesting to note that with comparable baseline BSA and preoperative hematocrit levels, a similar profile of surgeries being performed and a restrictive postoperative blood transfusion strategy in the BCP group, the hematocrit at discharge was comparable between the groups (30.9 vs 31.8). This suggests blood can truly be conserved in cardiac surgery.
Intraoperative blood conservation strategies
Retrograde autologous priming of the CPB circuit is recommended by both the STS and EACTS as a measure to prevent hemodilution on the pump and conserve blood during surgery.3,5 Hou and associates showed a significant decrease in transfusion requirement in patients who underwent RAP compared to those who underwent surgery without RAP (26.7% vs 83.3%;p < 0.01). 10 In our study, all patients of the BCP group underwent RAP and it was identified as a significant risk factor for transfusion during the course of the patient’s treatment on univariate analysis (p < 0.001). Sun et al observed a significant reduction in the risk of intraoperative transfusion after RAP (0.39, 95% CI 0.29, 0.53; p < 0.00,001). 8 We observed that patients undergoing RAP had significantly higher levels of nadir hematocrit on CPB (26% vs 22.5%; p-0.003), which indirectly reduced the utilisation of blood on the pump as confirmed on multivariate analysis. These findings are in line with previous studies and corroborate the role of RAP in the conservation of blood during cardiac surgery.
Ranucci and associates demonstrated excessive hemodilution and the lowest hematocrit (especially below 25%) achieved on-pump were independent risk factors for morbidity, even in the absence of blood transfusion. 12 Implementation of measures to avoid excessive hemodilution like doing RAP, administering blood cardioplegia, using miniaturised circuits, reducing priming volume and performing surgery under normothermia have been suggested to reduce the risk of bleeding and the need for blood transfusion.3,5,12 In our study, patients following the BCP had a nadir hematocrit of 26% compared to 23% in the other group. We too identified low hematocrit on-pump as the predictor for intraoperative blood administration.
After waning off CPB, by transfusing the perfusate remaining in the oxygenator and the aortic line tubing, we were able to transfusion about 500 mL of autologous blood to the patient. This let us achieve a post-protamine hematocrit comparable to the other group, where 50% of patients received intraoperative transfusion.
STS and EACTS guidelines recommend the use of antifibrinolytics therapy (tranexamic acid and epsilon aminocaproic acid) as a measure to reduce blood loss and blood transfusion during cardiac procedures (Class I, Level A)3,5,14 All patients in the BCP group received the same, however, due to erratic use of antifibrinolytics in the comparison group, the contribution of antifibrinolytics in conserving blood due BCP could not be ascertained.
Postoperative blood conservation strategy
Mazer and associated demonstrated a restrictive strategy of blood transfusion after cardiac surgery was not inferior to a liberal strategy in terms of patient outcome. 1 However, a decrease in the proportion of patients receiving transfusion was observed and transfusion was identified as an independent risk factor for late mortality (72.6% vs 52.3%).1,17 Clinical patient management guidelines for patients undergoing cardiac surgery now recommends a restrictive allogeneic blood transfusion strategy for perioperative blood conservation (Class I, Level A).3,5 In our study, a hematocrit trigger of 27% was used in both groups for postoperative blood transfusion and the utilisation of blood was found to be comparable (14.8% vs 17.8%). Post-operative mediastinal drainage was the only predictor of postoperative transfusion.
Patient recovery
We observed a lower inotrope requirement in patients following the BCP, however, the duration of inotrope use and time of mechanical ventilation was comparable between the groups. Although the duration of ICU stay was similar, patients in the BCP group had a significantly shorter time to discharge from the hospital. Interestingly, patients who received transfusions showed a trend towards a longer hospital stay within the BCP group.
Morbidity and mortality
Blood transfusion has been associated with an increased risk of infection secondary to immunosuppression, ischemic complications like stroke and myocardial infarction, renal dysfunction requiring hemodialysis, increased incidence of atrial fibrillation and mortality.2,4,7,18–21 Studies have demonstrated a two times higher mortality risk at 5 years in patients who received perioperative transfusion and this risk is seen to extend beyond a decade after the surgery.2,21 Murphy and colleagues found patients undergoing transfusion had 3 times higher odds of infection and ischemic complication. They also observed transfused patients were less likely to be discharged from the hospital (hazard ratio [HR], 0.63; 95% CI, 0.60 to 0.67) and more likely to have mortality after discharge (0 to 30 days: HR, 6.69; 95% CI, 3.66 to 15.1; 31 days to 1 year: HR, 2.59; 95% CI, 1.68 to 4.17;1 year: HR, 1.32; 95% CI, 1.08 to 1.64) 4 Our study did not detect a difference in the rate of occurrence of these complications between the two groups, however, a longer follow-up is required to truly determine the same.
Cost implication
The cost of blood and blood products differs in various countries. For one unit of packed red blood cells, the cost in India is ₹ 1450 16 compared to $210 6 in the USA and £ 130 4 in the UK. This excludes overhead charges of storage, additional laboratory testing, administration of blood and cost incurred in managing complications associated with transfusion. Murphy and associates found transfusion was associated with an increased relative cost of admission (any transfusion, 1.42 times [95% CI,1.37 to 1.46], varying from 1.11 times for 1U to 3.35 times for 9 U). 4 As the transfusion requirements in the BCP group were less, we observed that the expenditure per patient towards blood transfusion was significantly less compared to patients undergoing surgery with BCP.
Importance of a structured blood conservation protocol
Our study highlights the importance of a structured protocol for utilising blood conservation approaches as compared to unsystematically applying the same. A structured BCP comprising simple strategies significantly reduced the consumption of blood and had a positive impact on patient outcomes. The STS now recommends the institution of a comprehensive multimodality blood conservation program led by a multidisciplinary team of health care providers to be part of any patient blood management program to limit the utilization of blood. 3
Limitation
It was a retrospective analysis of prospectively collected data. The data was skewed, and a larger sample would be required to normalise the distribution. The study was not adequately powered to study the study population’s risk factors for low hematocrit on-pump. The use of antifibrinolytics in the control group was not uniform and hence was difficult to ascertain its effect on the utilization of blood and it was a confounding factor.
We appreciate that different surgeons in the two groups is another confounding factor. However, the two groups were comparable with regard to the preoperative characteristics of the patients (diagnosis and functional class), the type of operative procedure performed, operative times and postoperative blood loss. Although these similarities do not eliminate the potential for bias, it doesn’t seem to have an obvious impact on the outcomes. Also, we acknowledge these heterogeneities has a potential for statistical bias, but we believe it reflects the real-world scenario where subtle differences in individual practice exist within a given centre and may have an impact on patient outcomes.
Conclusion
Implementing a structured blood conservation protocol in adult patients undergoing open heart surgery significantly reduces the need for blood transfusion. It also has a promising impact on patient recovery after surgery and significant positive cost implications.
Footnotes
Authors’ note
Presentation - This manuscript has been presented at IACTSCON 2023 held in Coimbatore, Tamil Nadu, India on 17.02.2023.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.