
Abstract
Objective
To compare and analyze the efficacy and safety of different methods for injecting polidocanol in the treatment of venous malformations.
Methods
The medical records of patients with venous malformations in our hospital from April 2021 to April 2023 were analyzed retrospectively, and they were divided into control group (n = 38) and observation group (n = 20) according to different treatment methods. Control group was injected with polidocanol under ultrasound guidance, while observation group was injected with polidocanol under digital subtraction angiography (DSA) monitoring. Therapeutic effects of observation group and control group after 3-6 months of treatment were compared and analyzed, and complications that can be used to reflect the safety of treatment in two groups were collected and recorded.
Results
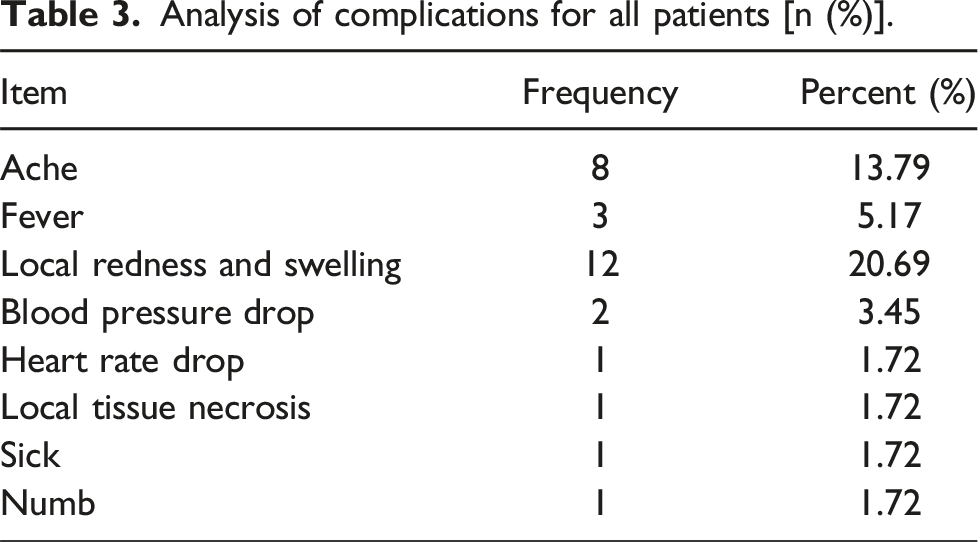
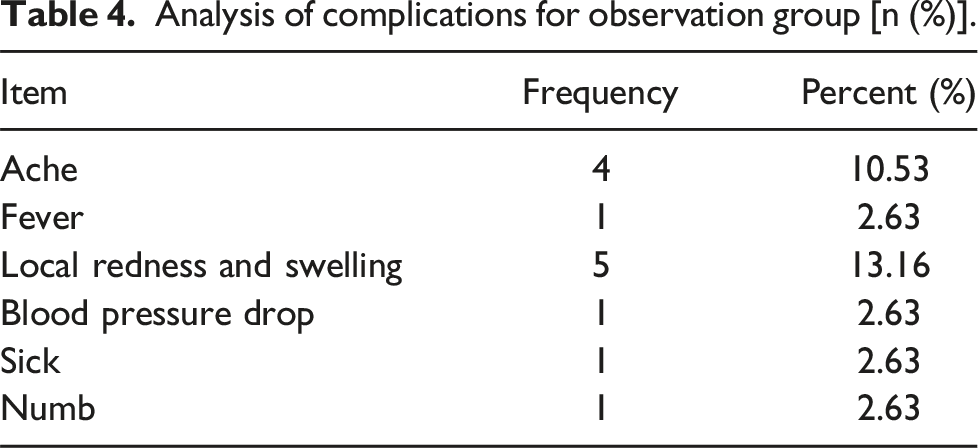
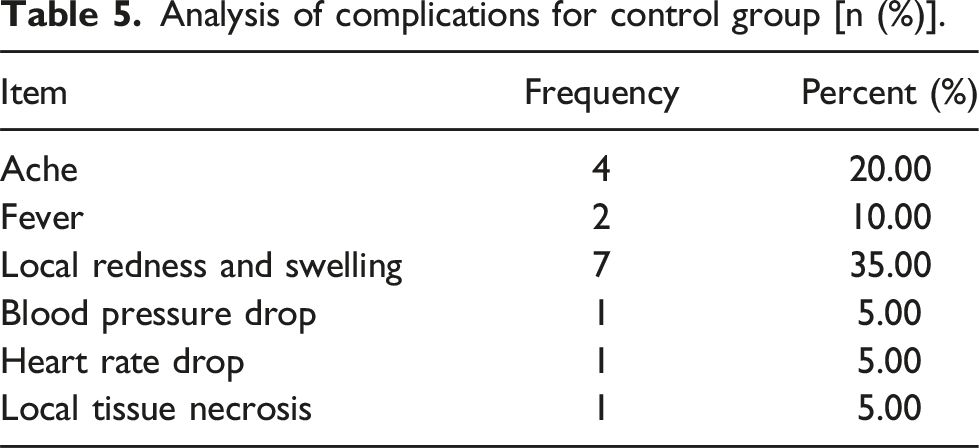
After treatment, the total effective rates of observation group and control group were 97.37% (37/38) and 75.00% (15/20) respectively, with significant differences (both p < .05). After 3-6 months of treatment, 13 complications occurred in observation group, while 16 occurred in control group. The number of complications in observation group was 6, with an incidence rate of 15.78%; while that in control group was 9, with an incidence rate of 45.00%, with a significant difference (p < .05). There were no significant differences among other baseline data, age and complications between two groups (all p > .05).
Conclusion
Injection of polidocanol in patients with venous malformations under DSA monitoring was more effective and safer.
Introduction
Venous malformation is a common congenital vascular malformation disease. A study shows that venous malformation accounts for about 70% of congenital vascular malformation. 1 Venous malformation is mainly caused by abnormal collection of thin-walled, irregular-shaped, and abnormally smooth muscle containing venous vessels, which can lead to appearance abnormalities and dysfunction, and even disability in severe cases, increasing the risk of death of patients. 2 In addition, venous malformation is a kind of low-flow vascular disease that can cause a decrease of venous blood flow rate in patients, resulting in venous blood stasis. At this time, the pressure of internal vein increases, and the volume of lesion site also increases, which will oppress and even invade normal tissues around the deformed vein.3,4 It is found that the incidence of venous malformations is about 0.2%, and the ratio of male to female is 1:1, with no gender difference. 5 And venous malformations can occur throughout the body, but mainly in limbs and head and neck, with the incidence of limbs and head and neck accounting for 40% respectively. Venous malformations in airways and muscles are also common, which can invade some other tissues, such as bones, joints and internal organs. 6 Investigation shows that venous malformations occur in deep or superficial areas, which can be localized or sporadic, and there are single or multiple cases. Therefore, this systemic onset feature can lead to different clinical symptoms in patients. 7
At present, early treatment of venous malformations is advocated in clinical practice, for the purpose of controlling the development of the disease, improving patients’ physical condition and avoiding affecting the appearance. Additionally, sclerotherapy, surgical resection and interventional therapy are the main treatment methods for venous malformations. Direct surgical treatment is easy to cause damage to the important structures and tissues of patients, and can produce various complications, which is easy to cause recurrence of lesions. 8 At this stage, the International Venous Association recommends sclerotherapy as the first choice for the treatment of venous malformations, and polidocanol is one of the most widely used sclerosing agents in clinic. The process of injecting polidocanol is relatively simple, making it generally well-tolerated by patients. It offers a high level of treatment safety, involves minimal trauma, and helps reduce patients’ medical expenses.9,10 It is found that under the guidance of digital subtraction angiography (DSA) or ultrasound, polidocanol can achieve high curative effect in the treatment of venous malformations. It allows for dynamic observation of the lesion site, providing a visual advantage. On the other hand, ultrasound procedures are non-invasive and convenient, but real-time monitoring can be challenging, potentially leading to inadvertent injection of sclerosing agents into normal blood vessels. 1 However, there is currently limited research in clinical practice comparing the efficacy of polydocanol injection under DSA or ultrasound guidance. Therefore, the aim of this study was to investigate and compare the efficacy and safety of these two methods of polydocanol injection.
Materials and methods
Research objects
A retrospective cohort statistical analysis was conducted on the medical records of venous malformation patients admitted to our hospital from April 2021 to April 2023. A total of 58 patients with venous malformations were included in this study, and they were divided into control group (20 cases) and observation group (38 cases) according to different treatment methods. This study was approved by the Ethics Committee of The First Affiliated Hospital of Gannan Medical University (No. LLSC-2023, NO. 219).
Diagnosis and selection criteria: (1) Those who conformed to the diagnostic criteria of venous malformations in Venous Malformation and Haemangioma: Differential Diagnosis, Diagnosis, Natural History and Consequences 11 ; (2) patients with complete clinical data; (3) patients without history of interventional sclerotherapy; (4) patients with normal liver and kidney function, and complete cardiopulmonary function.
Exclusion criteria: (1) Patients complicated with other vascular diseases; (2) Patients suffering from mental illness who cannot cooperate with the treatment; (3) Pregnant women and lactating patients.
Drugs and instruments
Polydocanol injection (produced by Siegfried Hameln GmbH, Germany, specification 2 mL: 10 mg, national medicine approval number of HJ20160032); disposable syringe (produced by Shandong Zhuquetang Medical Equipment Jinan Branch); medical tee (produced by Shanghai Shangyao Xinyi Pharmaceutical Co., Ltd.); disposable venous infusion needle (produced by Jinan Qinlu Pharmaceutical Technology Co., Ltd.); color Doppler ultrasound machine (Nanjing Baden Medical Co., Ltd., Model: GE medical color ultrasound diagnostic instrument VOLUSONS6); DSA machine (Siemens, Germany, ANGIOSTAR PLUS).
Treatment
Firstly, the foam hardener was configured on site, and a syringe filled with 0.5 mL of 3% concentration polydocanol injection and a syringe filled with 2 mL of air were connected by using a medical tee, so that the two syringes formed a 90-degree angle, and the syringe was quickly pushed for 15-20 times to convert the polydocanol liquid into the foam hardener.
Patients under the age of 12 were given general anesthesia, while patients over the age of 12 were given local anesthesia. Control group was given polidocanol injection under the guidance of ultrasound. The venous malformations were detected by ultrasound and the appropriate puncture points were selected. Under the real-time guidance of ultrasound, the lesion was punctured percutaneously with No.7 needle, and polidocanol was injected when the puncture needle returned blood until the tension of the lesion increased or the injection resistance increased. In cases where the lesion area was too large, multiple injection points could be used to repeat the above procedure. Observation group was injected with polidocanol under DSA monitoring, and the lesion site was punctured with a puncture needle. Venous blood was drawn back after puncture, and then the success of puncture was confirmed using DSA. When successful, polidocanol was injected until it filled the venous malformation tumor nest and drained into the vein, and the injection was stopped.
After injection, the patients were given dexamethasone intravenously and rehydrated for 1 week. Thirty days after the injection, all patients were rechecked by color Doppler ultrasound to evaluate the therapeutic effect. If the size of the venous malformation was less than 2/3, or symptoms recurred, DSA monitoring or ultrasound guided injection of polydocanol was required again.
Postoperative treatment and follow-up
After operation, patients applied local compression with gauze to concentrate the sclerosing agent at the lesion site, preventing the agent from dispersing too rapidly with blood flow, and the compression time was not less than 30 min. If patients experienced severe pain at the lesion site, analgesic medications were administered. If a patient’s body temperature rised above 38.5°C, antipyretic drugs were given. Following treatment, patients were observed in the hospital for 24 h, and if they were comfortable with no discomfort, they could be discharged. All patients underwent a follow-up examination after a 4-weeks interval. After the final treatment, patients were followed up with at a time interval of 3-6 months to observe and record changes in lesion size and improvements in clinical symptoms.
Observation indexes and efficacy evaluation
Efficacy evaluation: After 30 days of treatment, the therapeutic effect was evaluated according to the clinical symptoms, physical examination and color Doppler ultrasound examination of the patients, and the therapeutic effect was divided into four grades: cure, significant remission, partial remission and ineffective. The specific evaluation criteria were: Cure: venous lesion size reduction of 76% to 100%, B-ultrasound showed the disappearance of blood flow, and the lesion cavity contained a significant amount of thrombus; Significant remission: venous lesion size reduction of 51% to 75%, minimal abnormal blood flow was visible on B-ultrasound, and there was a significant amount of thrombus in the venous malformation; Partial remission: venous lesion size reduction of 26% to 50%, B-ultrasound indicated the disappearance of most of the blood flow; Ineffective: venous lesion size reduction of 0% to 25%, B-ultrasound showed an increased or unchanged non-echogenic area within the vessels, and blood flow remained abundant. Total effective rate = (cure + significant remission + partial remission) cases/total cases ×100%.
The end point of treatment: (1) No significant change in lesion size and no significant improvement in clinical symptoms after three or more treatments; (2) the venous lesions were reduced to less than 10% of the original volume; (3) patients or their families request to stop treatment.
Safety: The complications of patients in two groups within 3-6 months after the end of the final treatment were analyzed, and the relationship between age and postoperative complications was analyzed. The fewer complications, the higher the safety.
Statistical analysis
The normality of the measurement data was tested by SPSS26.0 statistical software, the normal measurement data were expressed as “mean ± standard deviation”, and the independent sample t test was used for intergroup comparison. Enumeration data were expressed by % and n, using χ2 test, and rank sum test was used for rank data. p < .05 was considered to be statistically significant.
Results
General information
Comparison of baseline data [
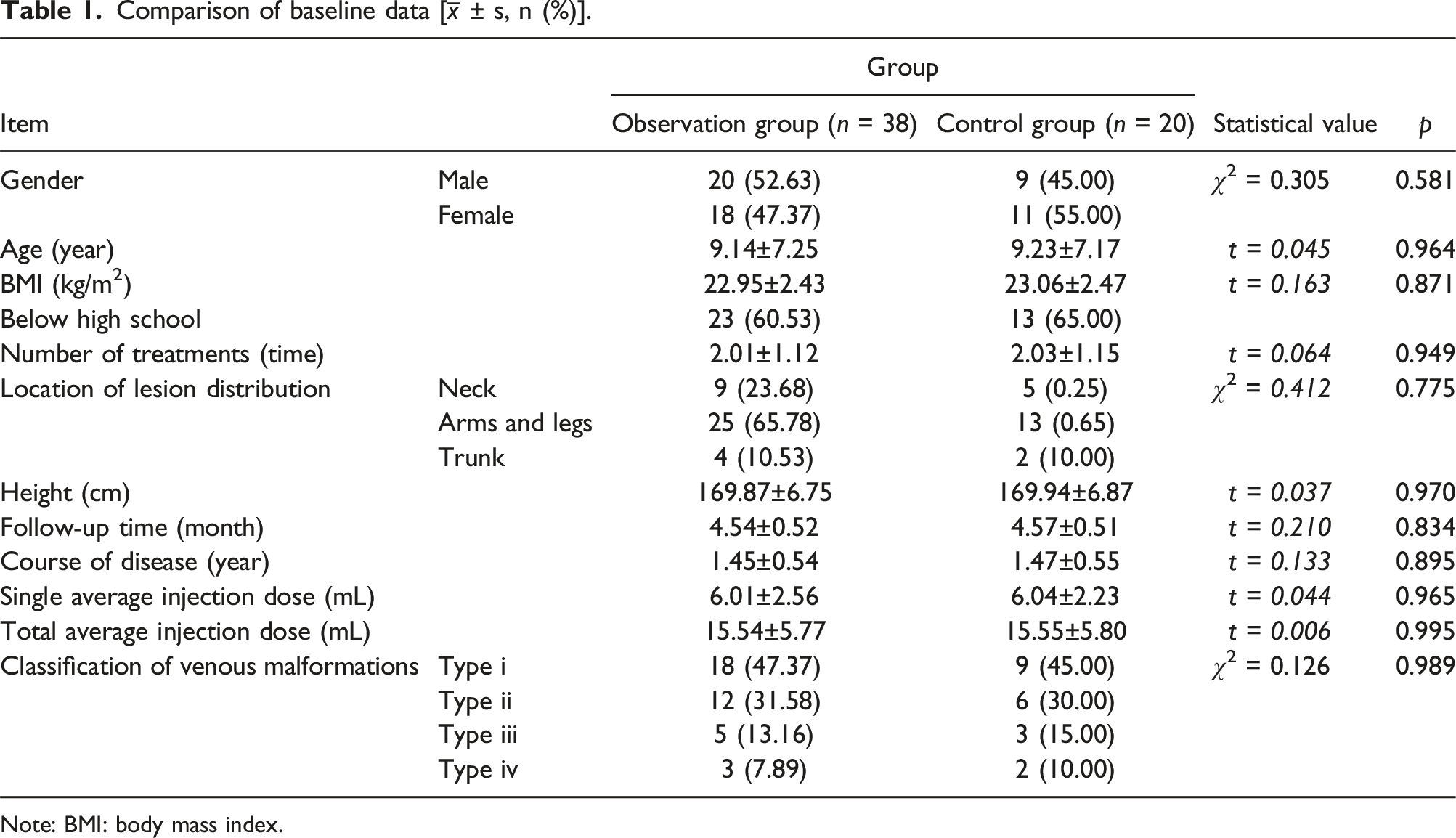
Note: BMI: body mass index.
Comparison of clinical efficacy
Comparison of clinical efficacy [n (%)].

Safety analysis
Analysis of complications for all patients [n (%)].
Analysis of complications for observation group [n (%)].
Analysis of complications for control group [n (%)].
Analysis of complications for two groups [n (%)].

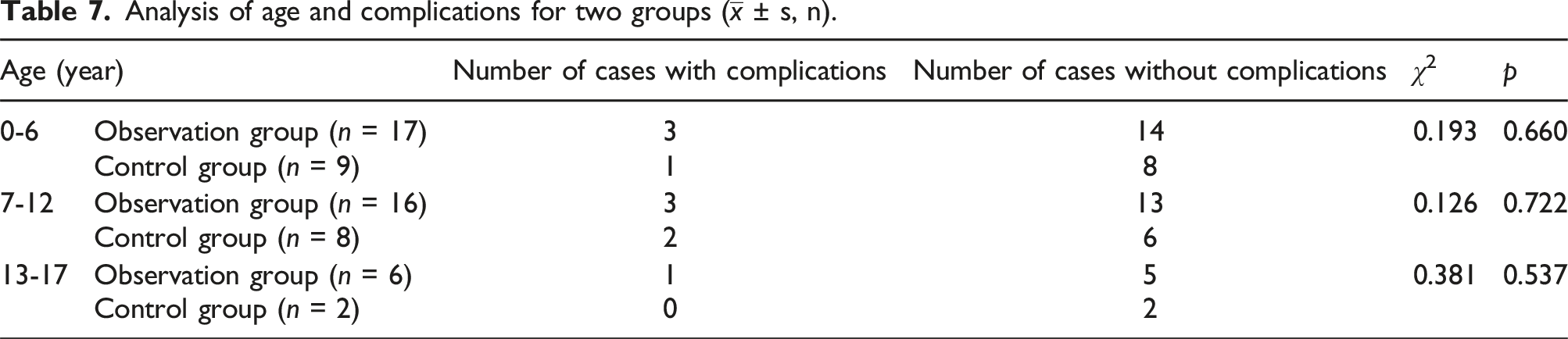
Analysis of the relationship between age and complications
Analysis of age and complications for two groups (
Discussion
Venous malformation is a congenital vascular malformation caused by abnormal morphological development of embryonic vessels, which can affect the function and morphology of patients’ blood vessels and lead to abnormal blood flow status of blood vessels. It is difficult to predict and control the clinical symptoms and the progress of the disease course of patients. 12 In the initial stage of suffering from venous malformations, the clinical symptoms of patients are relatively mild, and there are almost no typical clinical symptoms, so it is easy for patients to be directly surgically removed because of misdiagnosis, but venous malformations will recur after a few years. 13 Most clinical symptoms are caused by trauma and infection. Common clinical symptoms include: pain, appearance abnormality, lump, edema, varicose veins, etc. With the progress of the disease, the lesions of venous malformations will gradually expand, and it will not subside by itself, with no self-healing.14,15 Because the clinical symptoms of venous malformations are complicated, the treatment plan for venous malformations should be personalized and need to be combined with many disciplines. Sclerosing agent is a low-invasive treatment method, which can avoid large-scale surgical incision and reduce bleeding and muscle injury. It is recommended for the treatment of venous malformations, and most patients can obtain better treatment results by using this treatment method. 16 Polydocanol, as a sclerosing drug, is widely used in the treatment of venous malformations. Polydocanol has the characteristics of low sensitization and anesthetic, and can produce local anesthesia. It has high safety in clinical application. Its therapeutic mechanism is: it damages endothelial cells of blood vessels, causes thrombosis, fibroses the lesions of venous malformations, and then atresia, thus achieving the therapeutic effect.17,18 However, due to the anesthetic characteristics of polidocanol, cardiovascular complications such as blood pressure drop, heart rate drop and cardiac arrest may occur when treating venous malformations. Therefore, it is necessary to monitor the injection of polidocanol in real time and strictly control the injection amount of polidocanol to reduce the occurrence of the above complications. A study has found that the injection of polidocanol under ultrasound guidance or DSA monitoring is more accurate, can maximize the therapeutic effect. This approach can also reduce the radiation exposure to patients, lower their medical expenses, and alleviate their financial burden. 5 Ultrasound is a non-invasive examination without radiation, which can accurately determine the location of the lesions, and the ultrasound equipment is mobile and convenient to use. 19 DSA can avoid the influence of bones and gas, identify the scope of venous malformations and the situation of returning blood vessels, and dynamically monitor the flow direction of foam hardener in many directions to prevent foam hardener from flowing into normal blood vessels and reduce the occurrence of complications such as fever, pain and tissue necrosis. 3 Both ultrasound guidance and DSA monitoring have their advantages, but there is relatively limited research comparing their accuracy in polidocanol injection. Therefore, this study aimed to compare the efficacy of polidocanol injection under ultrasound guidance and DSA monitoring and analyze the safety of injecting polidocanol using both methods.
In this study, it was found that there were no differences in the number of treatments, the location of lesions, the average single injection dose and the total average injection dose between two groups, without significant differences (all p > .05). Follow-up for 3-6 months, comparing the therapeutic effect of polidocanol injection under DSA monitoring and ultrasound guidance in observation group and control group, it was found that the therapeutic effect of polidocanol injection under DSA monitoring was significantly better than that under ultrasound guidance, with a significant difference (p < .05). Comparing the complications between two groups, the incidence of complications in observation group was significantly lower than that in control group, with a significant difference (p < .05). There were no significant differences in age and incidence of complications between two groups (both p > .05). The above situation suggested that the efficacy and safety of polidocanol injection under DSA monitoring was better than that under ultrasound guidance. The superior efficacy and safety of polidocanol injection under DSA monitoring could be attributed to several factors: (1) DSA monitoring helped avoid the influence of lesion depth, bones, and gas, allowing for the maximal delineation of the extent of venous malformations and precise determination of the lesion’s location and size. It also provided insights into the surrounding conditions of the lesion. During polidocanol injection under DSA monitoring, it was possible to visualize whether the needle had shifted and if there was any extravasation of the sclerosing agent. After polidocanol injection under DSA monitoring, real-time observation of the dynamic replacement of contrast agent by the polidocanol sclerosing agent in the lesion site and the closure of draining veins could be achieved. The entire DSA monitoring process effectively enhanced the efficacy of sclerotherapy and reduced the occurrence of complications20,21; (2) the injected contrast agent dose could be used to estimate the volume of the venous cavity, so as to determine the injection dose of the sclerosing agent. When injecting the sclerosing agent, the contrast agent within the venous cavity appeared as a white area in the contrast state, and the injection dose of the sclerosing agent could be adjusted according to the diffusion range of the white part when the contrast agent was squeezed, and an appropriate amount of sclerosing agent dose could prevent excessive sclerosing agent from extravasating to the surrounding normal tissues and reduce the occurrence of tissue necrosis complications. Otherwise, the extravasated sclerosing agent might lead to congestion and swelling of the soft tissues around venous malformations, and might also cause ulceration of the surrounding skin, so DSA monitoring was conducive to determining the injection dose of sclerosing agent and improving the safety and effectiveness of treatment.22,23 This was consistent with the research results of Saji et al. 24 Injection of polidocanol under DSA monitoring was more conducive to defining the size, range and drainage vein of the lesions, and could judge the injection dose and the drug arrival range, which had more obvious advantages compared with ultrasound guidance.
However, injection of polidocanol under DSA monitoring still has some disadvantages, such as high cost, long operation duration, and the possibility of inducing nephropathy and ionizing radiation by contrast agent, especially when the patient is relatively young and may need repeated operation. A study has found that treatment safety can be improved through the following measures: (1) Repeated blood drawing during injection to prevent the sclerosing agent from entering the normal site; (2) consider administering treatment in small doses multiple times. Typically, monthly intervals for treatment can help control the dosage and avoid complications such as skin tissue necrosis, pain, and blood pressure drop caused by excessive drug injection; (3) after operation, apply pressure with gauze at the lesion site to facilitate a prolonged interaction between the sclerosing agent and the lesion cavity; (4) venous malformation is a benign condition, so the primary goal of treatment is symptom control. When treating, it’s essential to balance the efficacy of treatment with the risk of complications. Treatment can be discontinued when symptoms improve. 25
In conclusion, injecting polidocanol under DSA monitoring appeared to be more effective compared to ultrasound-guided treatment. It could significantly reduce the size of the lesion, alleviate clinical symptoms, improve patient functionality, and offer higher treatment safety. This approach was minimally invasive, radiation-free, and reduced the incidence of complications, making it a promising choice for clinical promotion and application.
Ethical statement
Ethical approval
The study was reviewed and approved by the Ethics Committee of The First Affiliated Hospital of Gannan Medical University (No. LLSC-2023,NO.219).
Footnotes
Authors contribution
Conception and design: Wei Peng and Haijin Liu. Method: Xin Li, Shiyu Xiong and Rongjie Wu. Data Collection: Haijin Huang, Yong Zeng and Feng Chen. Manuscript Writing: Wei Peng, Xin Li and Rongjie Wu. Manuscript revision: Qian Liu and Haijin Liu. Research supervision: Qian Liu and Haijin Liu. All authors contributed to the article and approved the submitted version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Key Project of Natural Science Foundation of Jiangxi Province (No.20192ACBL20005) and the Youth Project of Jiangxi Provincial Department of Education (No. GJJ201550).
Guarantor
Haijin Liu takes responsibility for the accuracy and appropriateness of this article.
Data availability statement
The simulation experiment data used to support the findings of this study are available from the corresponding author upon request.