
Abstract
Background
Increasing the levels of physical activity (PA) is widely recommended for people with chronic venous insufficiency (CVI). However, studies investigating the patterns of PA and adherence to PA guidelines using objective measures are lacking.
Objective
The primary aim was to examine the patterns of PA and adherence to PA guidelines among patients with CVI. A secondary aim was to identify whether adherence to PA recommendations differed according to patients’ sociodemographic and clinical characteristics.
Methods
This cross-sectional study included 96 patients with CVI with Clinical-Etiology-Anatomy-Pathology (CEAP) C3 to C6 (69.1% women 59 ± 11 years; 51.5% C5-C6 on CEAP classification). Objective time spent in PA was measured by a triaxial accelerometer. To examine adherence to PA guidelines, patients were grouped as meeting (or) the recommendations if they had at least 150 min/week of moderate to vigorous PA. Sociodemographic and clinic characteristics were obtained by self-report. Binary logistic regression was employed to examine whether sociodemographic and clinical characteristics were associated with adherence to PA guidelines. T-tests were employed to compare PA levels at different intensities according to patients’ age.
Results
Patients spent an average of 311.4 ± 91.5 min/week, 42.1 ± 28.0 min/week, and 19.8 ± 17.8 min/week in low-light PA, high-light PA, and moderate-to-vigorous PA, respectively. The proportion of patients meeting PA recommendations was 36.2%, and older patients had lower odds (OR = 0.94; 95%CI: 0.89 to 0.99). Additional analysis reinforced that by showing lower time in high-light PA (51.2 ± 30.0 min/day vs. 31.9 ± 21.8 min/day; p = .001) and moderate-to-vigorous PA (24.3 ± 15.8 min/day vs. 14.8 ± 18.8 min/day; p = .012) among older patients than their peers younger.
Conclusion
Our findings showed that 36,2% of CVI patients met PA recommendations, with lower odds found among older patients. Public health interventions to enhance PA engagement among CVI patients should prioritize those who are older.
Introduction
Chronic venous insufficiency (CVI) is characterized by increased venous pressure, due to valve insufficiency or venous obstruction. The prevalence of CVI is controversial due to the lack of studies that address it globally. However, a survey revealed that of 23 Latin America countries evaluated, 32,3% of subjects presented CVI of C3-C6. 1 Furthermore, more recent evidence supports these trends, but also shows that the prevalence of CVI and varicose veins varies widely by region, although they are highest in Western countries. 2 The clinical severity of CVI is often determined using the Clinical-Etiology-Anatomy-Pathologic (CEAP) classification, which classifies the disease into seven stages, ranging from no visible or palpable venous disease (C0) to active ulcers (C6). 2
Individuals with the most severe type of venous disease (C3-C6 stages) are classified as CVI, which is prevalent in 10%–40% of the adult population3,4 and is known to negatively impact the individual’s functional capacity and physical activity participation. 5 Furthermore, it has been suggested that some CVI patients might fear the aggravation of their symptoms with the practice of physical activity (PA), 6 which can exacerbate limitations in daily activities.
Although there are no specific PA recommendations for these patients, in clinical practice they are commonly advised to perform a minimum of 150 min of moderate or 75 min of vigorous PA or the combination of moderate-to-vigorous PA (MVPA) per week, which is the current recommendation for the overall adult population. 7 Despite the scenario denoting reduced engagement in PA, to our knowledge, no prior study has identified the number of CVI patients who do not reach the PA recommendations, which is an important gap in the literature.
To fill this gap, we aimed to describe the patterns of PA and the proportion of CVI patients who achieve the current PA recommendations. The secondary aim was to identify whether adherence to the recommendations differs according to the patient’s sociodemographic and/or clinical profiles.
Methods
Study design
This cross-sectional study was performed following the strengthening of the reporting of observational studies in epidemiology (STROBE) guidelines. 8 The study was approved by the institutional ethics committee, and written informed consent was obtained from each participant prior to the investigation.
Participants and setting
Patients with CVI were conveniently recruited from two hospitals (Adriano Jorge Hospital and Araujo Lima Hospital) in Manaus, Brazil between September 2021 and July 2023 during routine consultations. A questionnaire was used to collect socio-demographic data. An experienced physician diagnosed the disease severity based on clinical examination. The six-minute walk test was used to assess functional capacity, and physical activity level was measured using an accelerometer. To be included in the study, participants were required to be adults aged 18 or older, of both sexes, with a CVI classification between C3-C6, and no lower limb amputation.
Measurements
Prior to commencing the study, all healthcare professionals and students involved in data collection received comprehensive joint training sessions to ensure that the data collected were both accurate and of high quality.
Sociodemographic and clinical data
Sociodemographic and clinical data were obtained by self-report through a standardized face-to-face interview. Participants self-reported their age (in years) and biological sex (male or female), as well as whether they had any diagnosed chronic diseases (hypertension, diabetes, and dyslipidemia) and/or took any regular medication (anti-hypertensive, anti-diabetic, anti-lipemic, or antiplatelet). Obesity was objectively defined as a body mass index (BMI) ≥30.0 kg/m2, calculated as body weight (in kilograms) divided by height squared (in meters). For the analyses, variables related to each chronic disease and medication were treated as dichotomous (0 = absence; 1 = presence).
Disease severity
The clinical severity of CVI was measured using the CEAP (Clinical, Etiology, Anatomy, and Pathophysiology), a widely used classification system to describe and categorize the severity of CVI. Patients are classified as C1 (no visible or palpable signs of venous disease), C2 (varicose veins), C3 (edema/swelling without skin changes), C4 (skin damage due to varicose veins or hidden varicose veins – venous reflux), C5 (healed venous ulcer), or C6 (active venous ulcer). In the current study, only those classified from C3 to C6 were included, and, for analysis, patients were grouped as C3-C4 (without ulcer) or C5-C6 (with ulcer), as previously recommended. 2 All measurements of clinical disease severity were performed by an experienced, blinded evaluator.
Walking capacity
Walking capacity was assessed using the six-minute walk test. The test was carried out in a 30-m-long corridor following a previously described procedure. 9 Briefly, two cones were placed 30 m apart in a marked corridor. Before initiating the test, patients were given the instruction to walk as many laps around the cones as possible at their usual pace and were allowed to take breaks or rest if they felt the need to do so. The total distance walked was defined as the maximum distance achieved by the patient at the end of the six-minute walk test.
Physical activity levels
The objective measurement of PA levels was performed using triaxial accelerometers (GT3x, Actigraph, Pensacola, FL, USA), which are wearable devices that measure accelerations of the body segment to which the monitor is attached (ie., waist, wrist). In the current study, accelerometers were attached to the right side of the waist by an elastic band and patients were counseled to wear the device for 7 consecutive days, removing it only for sleeping, showering, and other water-based activities. The patient’s accelerometer data was only considered valid if he/she had a minimum of 600 min/day of wear time during the waking period, on at least 3 weekdays and 1 weekend day. Periods of 60 min of consecutive zero counts (with a 2 min spike tolerance) were considered as non-wear time and were excluded from the analysis. 10
The acceleration of the body segment is captured, filtered, and processed to obtain activity counts, which are the measurement units commonly used to classify activity intensity. In the current study, the intensity of physical activity derived from accelerometry was determined using Copeland and Eslinger cut-points, which were validated for older adults as 11 : low-light PA 100–1.040 counts/min, high-light PA 1.041 to 1.951 counts/min, and MVPA ≥1.952 counts/min on the vertical axis, and analyzed in min/days, adjusted for the number of days and daily hours that the device was worn. Accelerometry data were downloaded using ActiLife, version 6.13.4, and converted to 60-s epoch files. Considering the current recommendations for the overall adult population, patients in this study were classified as physically active or insufficiently active if they met or did not meet 150 min/week of moderate-to-vigorous PA, respectively.
Statistical analysis
Data normality was checked using the Shapiro-Wilk test. Descriptive statistics of numerical variables included mean and 95% confidence interval using 1000 bootstrap samples, while categorical data are described using absolute and relative frequencies. Crude and adjusted binary logistic regression models were created to analyze the sociodemographic and clinical characteristics (i.e., age, sex, time of disease diagnosis, disease severity, and walking capacity) associated with adherence to physical activity recommendations, and the results are described as odds ratio and their respective 95% confidence intervals. Indepenent T-tests were employed to compare PA levels between older and younger patients. A p < .05 was set as statistically significant, and all analyses were conducted using SPSS version 20.0.
Results
Of the 185 patients who were invited to participate in the current study, 18 did not return the invitation, 49 did not agree to participate, and 22 did not meet the inclusion criteria (i.e., 19 had a C1-C2 CEAP classification, two presented a physical disability, and one had undergone vascular surgery). Thus, 96 patients were considered eligible, performed the six-minute walk test, and wore the accelerometer to measure PA levels. Eight out of the 96 patients did not present valid accelerometer data (i.e., did not wear the device for at least 4 days or did not wear it on at least one weekend day) and were excluded. Thus, the final sample of the study consisted of 88 patients with CVI. The flowchart of the study is presented in Figure 1. Study sample flowchart.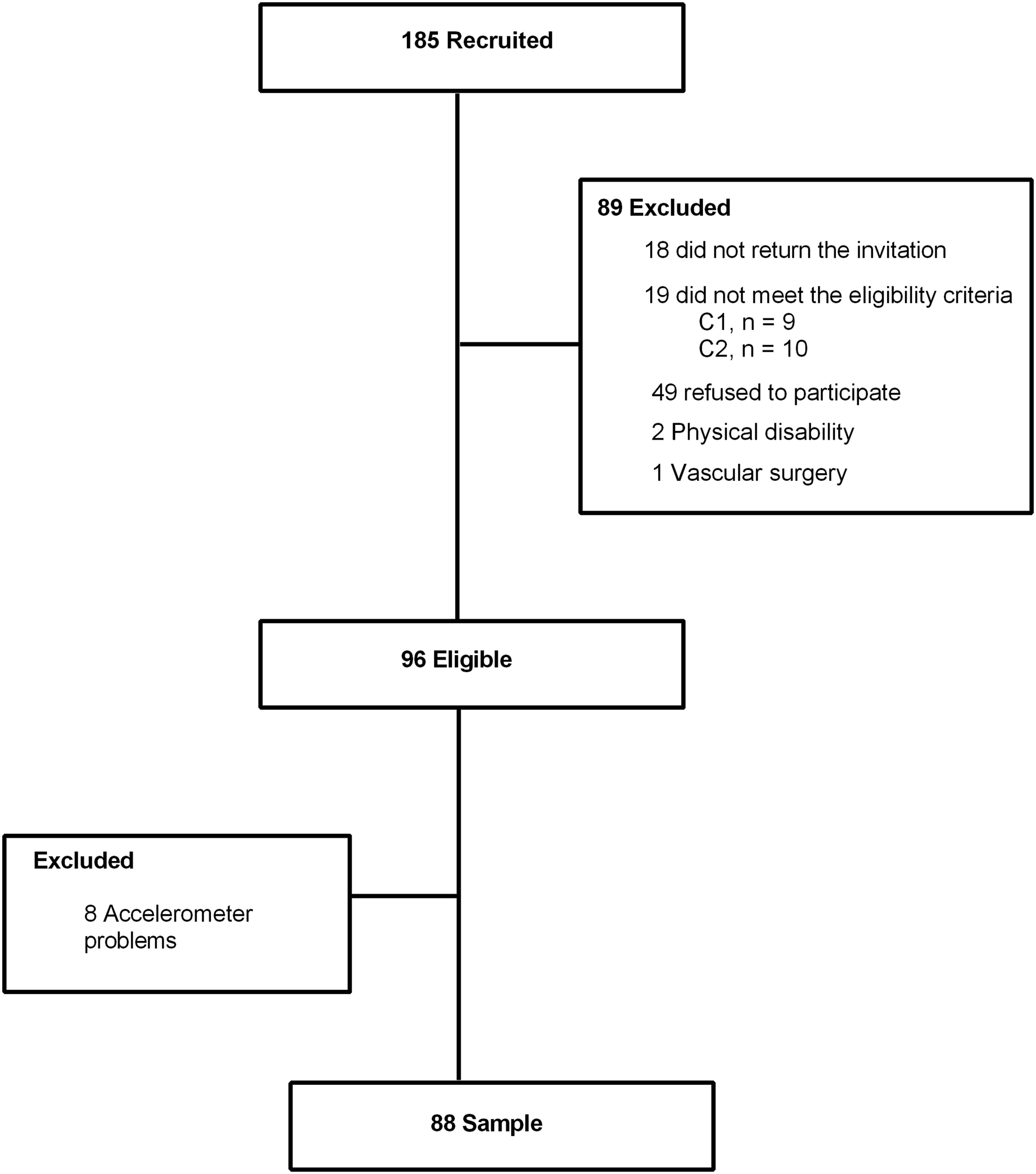
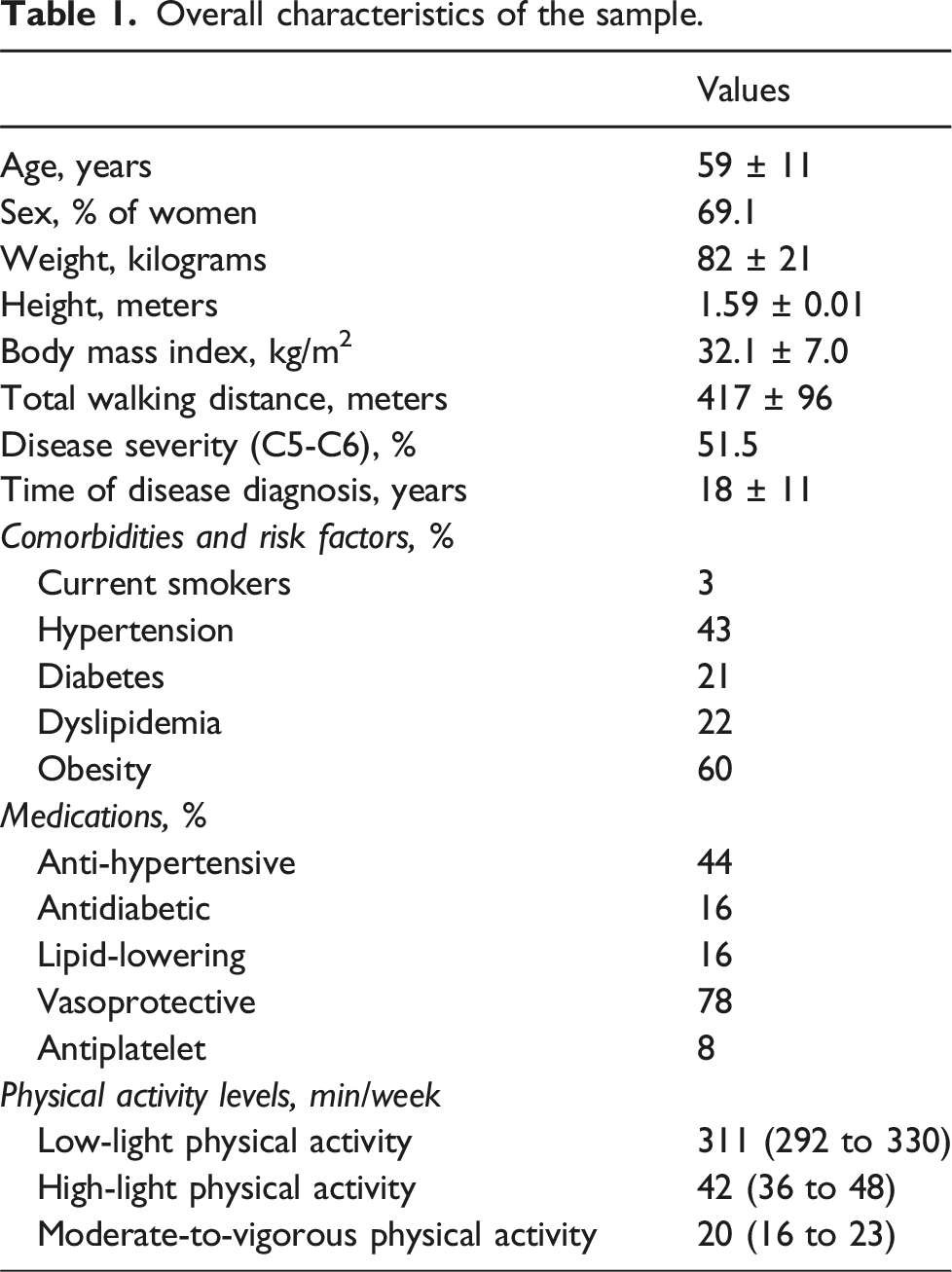
Overall characteristics of the sample.
Crude and adjusted associations between sociodemographic and clinical characteristics with adherence to physical activity recommendations in patients with chronic venous insufficiency.
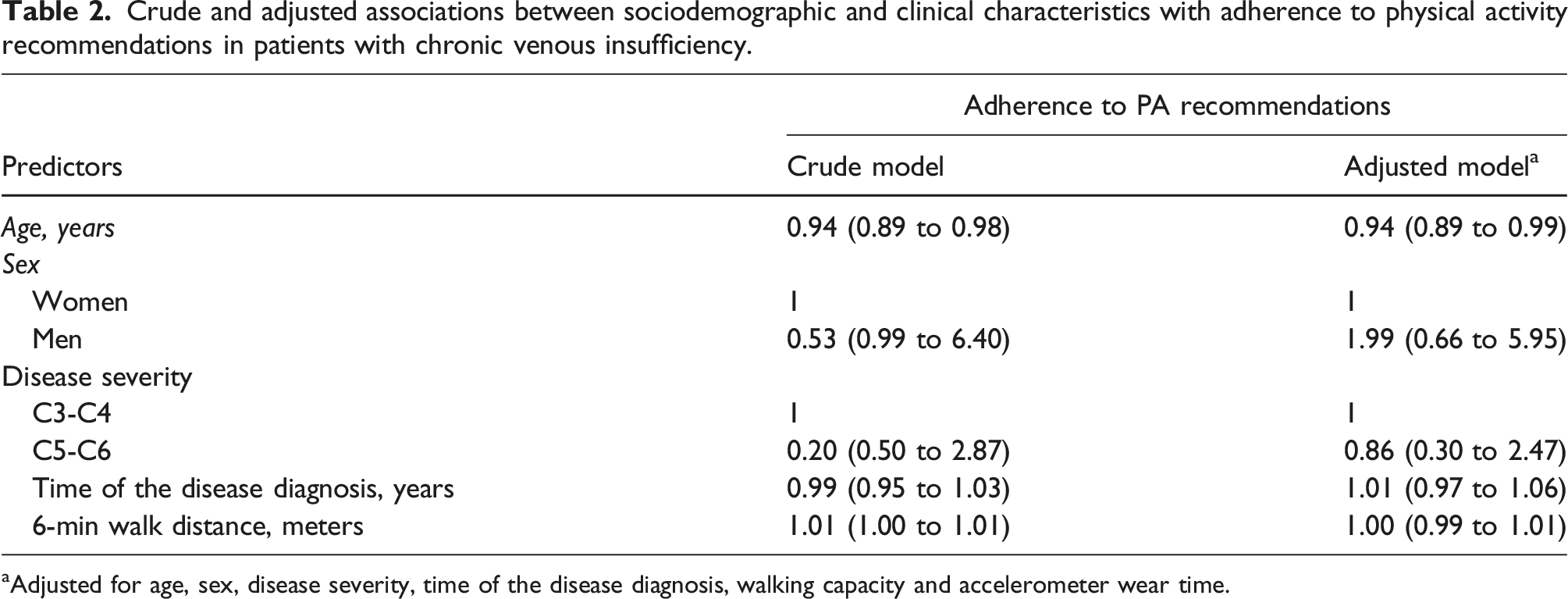
aAdjusted for age, sex, disease severity, time of the disease diagnosis, walking capacity and accelerometer wear time.
Figure 2 A presents the distribution of time spent in low-light, high-light, and moderate-to-vigorous PA, as well as the proportion of patients who achieved the PA recommendations according to age. In general, younger patients (age <60 years) presented less time spent in high-light PA (51.2 ± 30.0 min/day vs. 31.9 ± 21.8 min/day; p = .001) and moderate-to-vigorous PA (24.3 ± 15.8 min/day vs. 14.8 ± 18.8 min/day; p = .012), while no differences were found for low-light PA (328.5 ± 90.3 min/day vs. 292.6 ± 90.1 min/day; p = .066) (Figure 2(a)). Furthermore, the prevalence of physically active patients was 53.3% among those under 60 years of age, while only 19% reached the recommendations among those over 60 years of age (Figure 2(b)). Time distribution of physical activity level.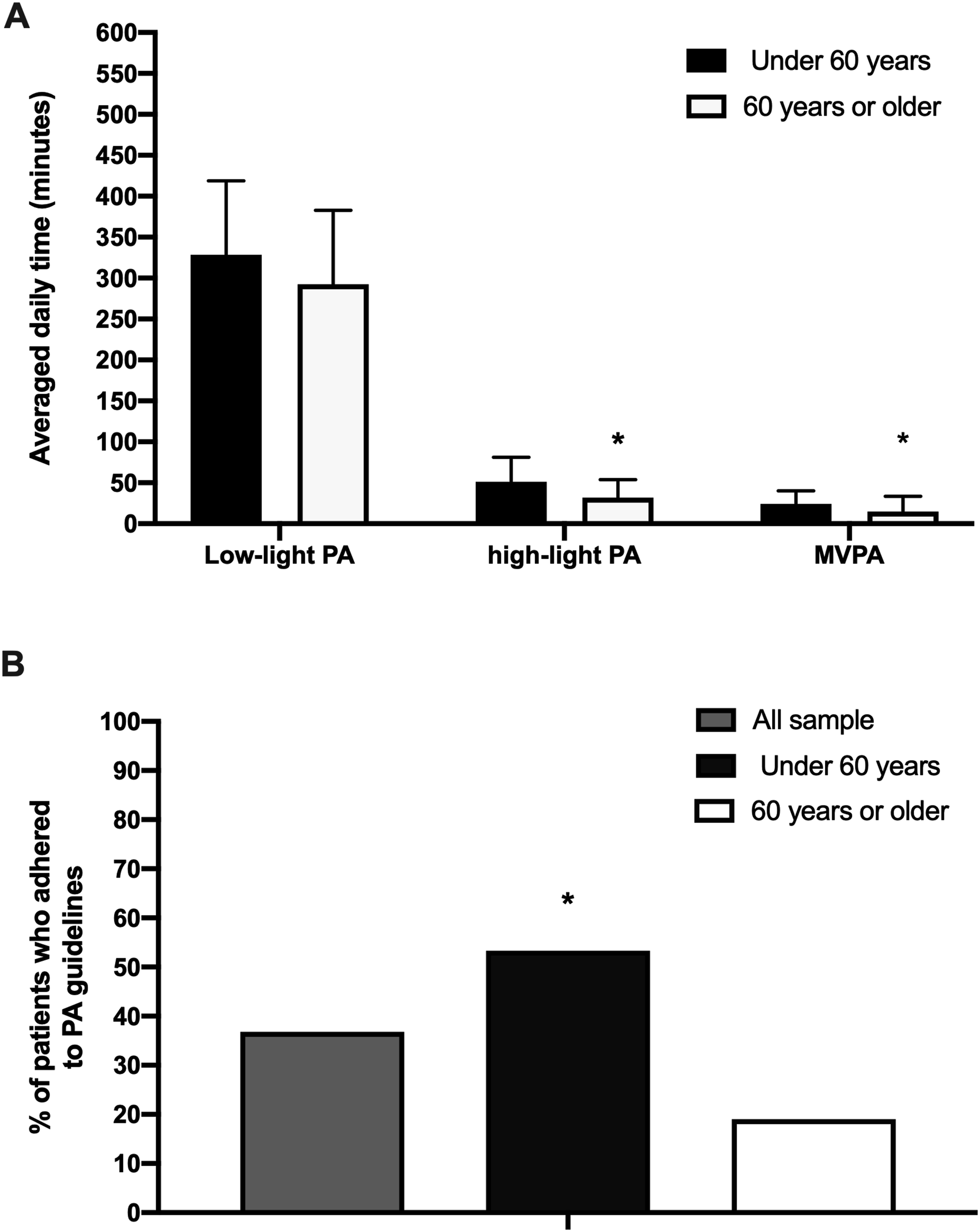
Values presented as mean and standard deviation. *Statistically significant difference.
Discussion
The main findings of the current study were twofold: a) 36,2% of the CVI patients adhered to the 150 min/week of moderate-to-vigorous PA; b) older age was associated with lower odds of meeting PA recommendations.
The proportion of individuals meeting PA recommendations in the current study (i.e., 36.25%) is higher than in a prior study conducted with patients with moderate to severe CVI (i.e., 6.0%). 5 This difference might be explained, at least in part, by the distinct methods used for PA measurement (ie., the current study measured objectively by accelerometer, while the prior study obtained PA level by self-report). Another factor refers to the PA recommendation itself as prior recommendations considered exclusively only activities with bouts of ≥10 min. Accordingly, a prior study with other vascular diseases (ie., peripheral artery disease and intermittent claudication) found that only 3.4% of patients met the prior guidelines using bouts of ≥10 min 12 Therefore, caution is needed when interpreting our results compared to previous findings, as current PA recommendations (i.e., those applied in this study) include all physical activities (i.e., non-bouted).
In our study, 64% of CVI patients do not meet the minimum PA recommendations, classifying them as physical inactivity. Physical inactivity increases complications health. A total of 7.2% and 7.6% of all-cause and cardiovascular disease deaths, respectively, are attributable to physical inactivity. 13 Further, the proportions of non-communicable diseases attributable to phys- ical inactivity range from 1.6% for hypertension to 8.1% for dementia. 13 These data are relevant to understanding the physical inactivity on the health of CVI patients. Recent data demonstrate that physically inactive elderly people (>65 years old) have a 75% and 60% higher risk of death from cardiovascular diseases compared to elderly people who practice low-light and moderate-vigorous PA, respectively. 14 These data highlight the importance of adhering to the World Health Organization’s PA recommendations. Additionally, the impacts of physical inactivity are not restricted to the elderly; it is also a problem among adults (18 to 59 years). In our study, patients with CVI have a higher prevalence of physical inactivity compared to adults (30%). 14 One of the biggest causes of physical inactivity in the world has been attributed to the increase in screen time among the population (ie., TV, computer, smartphone). 13 Therefore, reducing physical inactivity is recommended in CVI patients, mainly by controlling factors associated with the disease and consequently reducing the healthcare costs of these patients. 15
The present study also examined some potential factors associated with adherence to PA recommendations. The results indicated that only age was independently associated with adherence, suggesting that each year of life corresponds to a 6% decrease in adherence to PA recommendations. This is consistent with previous studies,16,17 showing that aging leads to a reduction in PA levels (i.e., particularly at higher intensities). 12 Non-compliance with PA recommendations has negative health impacts. Spending less than 150 min per week in moderate-intensity physical activity is associated with a 7.9 times higher chance of deat.18,19 Additionally, physical activity and advancing age are associated with greater severity of CVI. 20 Therefore, strategies to increase PA participation among CVI patients should prioritize those with older ages.
Limitations
The current study has some limitations that should be considered. Firstly, we used a cut-off point to classify PA intensity previously validated for older adults 11 and even though a prior study with vascular disease patients (ie., peripheral artery disease), 20 which might have similar characteristics to our sample, the lack of a specific cut-off might be considered a limitation. Second, the accelerometer model we used does not allow the capture of water-based activities, so it might underestimate patients’ PA levels. Third, as no specific PA guidelines for CVI patients are currently available, we used the PA recommendations for the overall adult population. Finally, we did not use venous ultrasound to objectively assess the CVI degree. However, the CEAP classification is highly utilized and recommended in clinical practice, as it allows healthcare professionals to standardize the severity of the disease.20,21
Conclusion
Our findings showed that 36,2% of CVI patients met PA recommendations, with lower odds found among older patients. Public health interventions to enhance PA engagement among CVI patients should prioritize those who are older.
Footnotes
Acknowledgements
Thank you for the support from Faculdade Estácio do Amazonas for providing laboratories for patient assessment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES) – “Finance Code 001″, and the Fundação de Amparo a Pesquisa do Estado do Amazonas (FAPEAM) – Edital N. 010/2021 – CT&I ÁREAS PRIORITÁRIAS.
Ethical statement
Guarantor
Fundação de Amparo a Pesquisa do Estado do Amazonas - FAPEAM.
Contributorship
Conception, research design and writing of the manuscript: Domingues, WJR; Simões CF. Obtaining financing, writing and data analysis: Domingues, WJR. Writing and analysis and interpretation of data: Domingues, WJR; Soares, AHG; Silva, GO; Simões, FC. Manuscript writing: Domingues, WJR; Soares, AHG; Simões, FC; Brandão, EKSS; Souza, L. C.; Souza, ELC; Silva, TRS; Costa, C; Campelo, PRS; Santos, NJN; Data collection: Brandão, EKSS; Souza, L. C.; Souza, ELC; Silva, T.R.S. Statistical analysis and writing of the manuscript: Domingues, WJR; Soares, AHG; Silva, GO. Critical review of the manuscript for important intellectual content: Cucato, GG; Areas, GPT; Silva, GO. Accountability Agreement: Domingues, WJR. Approval of the published version: Domingues, WJR; Soares, AHG; Silva, GO; Simões, FC; Brandão, EKSS; Souza, L. C.; Souza, ELC; Silva, TRS; Costa, C; Campelo, PRS; Santos, NJN; Data collection: Brandão, EKSS; Souza, L. C.; Souza, ELC; Silva, T.R.S; Cucato, GG; Areas, GPT; Silva, GO.