
Abstract
Objectives
There is a deficiency in awareness and knowledge of lipedema disease among the general public and healthcare professionals. This situation may lead patients to waste time on getting the correct diagnosis and treatment. Currently, information regarding women’s awareness and knowledge level of lipedema in Turkey is limited. This study aims to examine women’s awareness, knowledge level, and desire for information concerning lipedema in Turkey.
Methods
A total of 502 volunteer women participated in this online cross-sectional survey study. The survey, constructed by the authors of the study with the assistance of guidelines, systematic reviews, and current literature, consisted of sections aimed at determining demographic data, lipedema awareness, knowledge level, lipedema symptoms and suspicion, as well as individuals’ health behavior and desire for information. The primary outcome of the study was lipedema awareness, which was defined by having previously heard the term lipedema.
Results
Despite 76.1% of participants reporting awareness of lipedema, the average knowledge score about the condition was a low-to-moderate level of knowledge. The vast majority of participants (71.3%) indicated that they were willing to learn more about lipedema, and their preferred source of information was healthcare professionals (80.3%). Yet, only 19 participants (3.8%) think that lipedema is sufficiently regarded within the healthcare system.
Conclusion
This study reveals that, despite relatively high awareness of lipedema among women in Turkey, the level of knowledge remains limited. The strong willingness to receive further knowledge and the preference for healthcare professionals as the principal source of information garner attention. However, the low confidence in the recognition of lipedema within the healthcare system may suggest that healthcare professionals have insufficient knowledge or do not prioritize this issue. Improving awareness and knowledge of lipedema among the public and healthcare professionals might facilitate early identification and minimize treatment delays.
Introduction
Lipedema is a chronic adipose tissue disorder first described by Allen and Hinnes in 1940 as leg enlargement caused by subcutaneous fat and fluid accumulation in the bilateral hips and lower extremities. 1 It is considered to arise from hormonal fluctuations associated with puberty, pregnancy, and menopause, or due to genetic factors. 2 The main appearance is the symmetrical involvement of the hips and lower extremities. 1 Some types of lipedema may involve the upper extremities, but they typically spare the trunk, hands, and feet. 3 Easy bruising occurs with less stress due to increased capillary fragility. 4 Skin pain, with or without light touch, is a typical attribute.5,6 The diagnosis is often determined through patient history, familial history, and physical examination. 7 Lipedema might appear in individuals with a normal body mass index (BMI) in its earliest stages, but obesity affects the entire body and is always associated with a higher BMI. Although weight loss can be achieved by appropriate dietary interventions in obesity, the adipose tissue in lipedema is resistant to diet. 8 In contrast to lipedema, pain and easy bruising in the legs are not typical characteristics of lymphedema and obesity. 4
A major issue with lipedema is the mistaken or delayed diagnosis. It is frequently confused with lymphedema or obesity.9,10 Frequently, an accurate diagnosis is only possible several years after the onset of symptoms, at a later stage.11–13 Lack of awareness or knowledge among healthcare professionals and the public is one of the main causes of these problems. The public’s inadequate awareness of lipedema can result in individuals with the condition being unconscious of the fact that their symptoms signify a medical problem. In addition, it is known that the lack of awareness and knowledge about lipedema among healthcare professionals is one of the factors leading to delayed diagnosis and treatment. Numerous studies indicate that individuals often attend multiple physician appointments before obtaining a diagnosis.12,13 For example, a survey conducted in the United Kingdom with 251 participants indicated that only 46.2% of lipedema cases were identified. 14 A 2022 study in Spain highlighted that patients required an average of 5.5 visits to obtain an appropriate diagnosis, with delays reaching up to 19.9 years. 15 A study conducted in the Netherlands showed that there was an average of 2.8 doctor visits before diagnosis and an 18-years diagnostic delay from the onset of symptoms. 11 This situation leads patients to waste time on unnecessary treatments and ultimately obtain a correct diagnosis at a later stage. 16 The probability of individuals experiencing significant weight gain, joint complications, diminished mobility, and psychological disorders increases due to delayed diagnosis and treatment. Evaluating the public’s awareness and knowledge may reveal potential deficiencies and guide problem resolution. Understanding women’s information-seeking behavior may shed light on the methods for effectively bringing awareness and knowledge to them. Previous studies show that awareness and knowledge of lipedema are lacking among both the general population and healthcare professionals.17–20 Nevertheless, data on lipedema awareness and knowledge levels among women in Turkey are inadequate.
This study aims to investigate the awareness, knowledge level, and willingness to receive information regarding lipedema among women in Turkey.
Methods
Study design
This study was designed as a cross-sectional nationwide online survey. The research received approval from the Hamidiye Scientific Research Ethics Committee at the University of Health Sciences (meeting date: 11.09.25, registration number: 25/676, decision number: 17/9).
Participants
The survey was disseminated electronically via social media platforms and messaging applications using a convenience sampling method. Literate women aged 18–65 years who provided informed consent were eligible to participate. Exclusion criteria included age below 18 or above 65 years, male sex, and incomplete survey responses. Participation was voluntary and anonymous, and no incentives were offered. The study was completed between November 2025 and December 2025.
Survey
The authors of the study structured the survey using Google Forms, following a review of guidelines, systematic reviews, and similar studies from the current literature.4,17,20–22 The first section of the five-part survey included questions regarding participants’ age, gender, region of residence, height, body weight, and previous diagnoses. The second section comprised five questions regarding lipedema awareness, whereas the third section utilized a true/false format designed to assess knowledge about lipedema. The fourth section comprised five questions addressing whether individuals exhibited symptoms associated with lipedema and their beliefs regarding the condition. The final section comprised three questions designed to assess individuals’ health behaviors and their willingness to participate in information (Supplemental data 1).
Data analysis
The primary outcome of the study was lipedema awareness (yes/no). The required sample size was calculated using a standard formula for estimating a single proportion with 95% confidence. In the absence of reliable prior data, a conservative expected prevalence of 50% was assumed to maximize the required sample size and ensure adequate precision. With an absolute margin of error of 5%, the minimum required sample size was calculated as 385 participants. The final sample exceeded this requirement, allowing for more precise estimation of awareness prevalence.
Data were analyzed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were reported as mean ± standard deviation (SD) for continuous variables, and as frequency (n) and percentage (%) for categorical variables. Normality of continuous variables was assessed using visual inspection of histograms and the Kolmogorov-Smirnov test.
Lipedema awareness was defined by having previously heard of the term lipedema (yes/no). Knowledge score was derived from six true/false statements: correct responses were coded as 1, and incorrect or “I don’t know” responses were coded as 0; the total knowledge score ranged from 0 to 6 (higher scores indicating greater knowledge). A symptom burden score was calculated by summing five lipedema-related symptoms (presence = 1, absence = 0), yielding a score from 0 to 5 (higher scores indicating greater symptom burden).
Group comparisons of continuous outcomes were performed using independent-samples t tests, and associations between categorical variables were examined using the Pearson chi-square test.
To identify independent factors associated with self-reported lipedema suspicion, binary logistic regression was conducted. Variables were selected a priori based on clinical relevance and supported by univariate screening. Lipedema suspicion was dichotomized as “Yes” versus “No/Unsure.” The primary multivariable model included symptom burden score, knowledge score, and lipedema awareness. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit test. Statistical significance was set at p < .05 (two-tailed).
Results
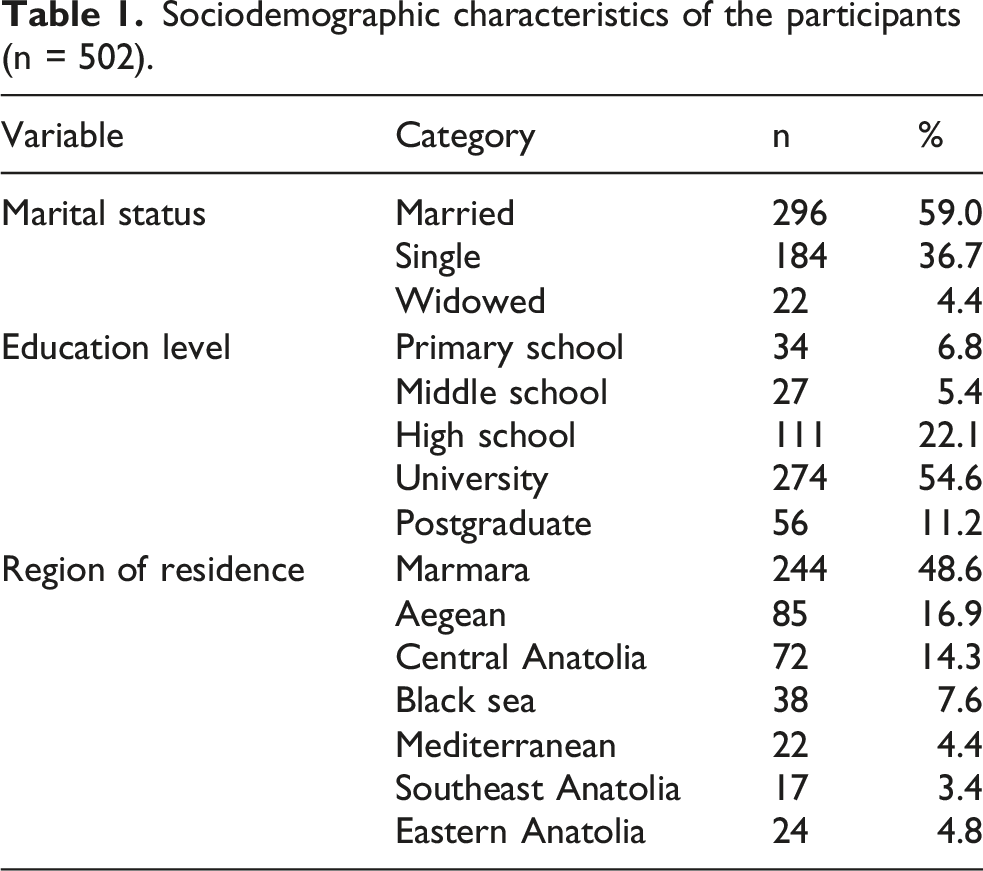
Sociodemographic characteristics of the participants (n = 502).
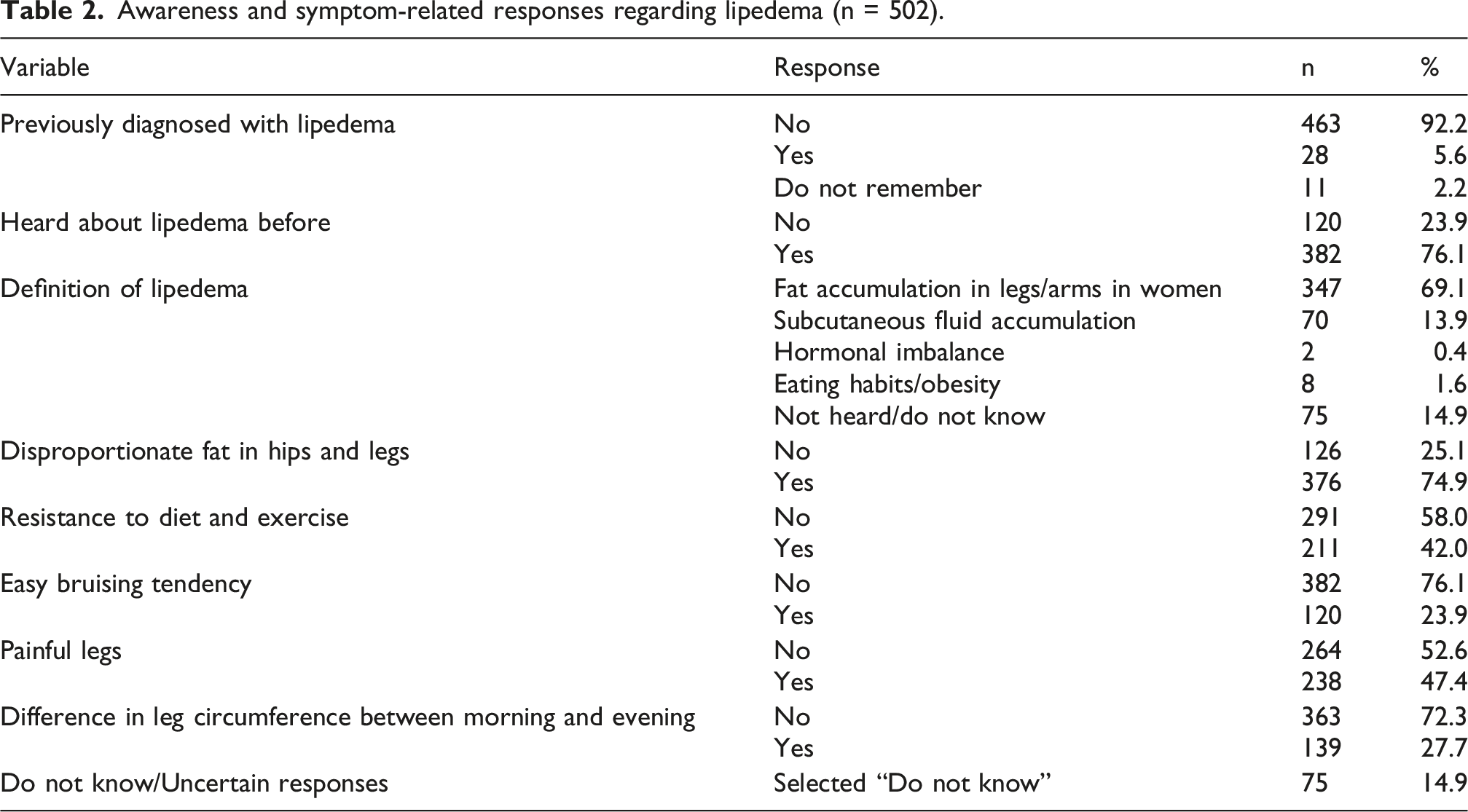
Awareness and knowledge of lipedema
Awareness and symptom-related responses regarding lipedema (n = 502).
Self-reported symptom burden
The mean lipedema knowledge score was 2.68 ± 1.51 (range: 0–6), indicating overall low to moderate knowledge levels in the study population. Based on predefined score ranges, 39.8% of participants were classified as having low knowledge (0–2), 51.2% as moderate knowledge (3–4), and only 9.0% as high knowledge (5–6). The mean symptom burden score was 2.16 ± 1.58 (range: 0–5), reflecting substantial variability in lipedema-related symptom reporting among participants.
Frequency of self-reported lipedema-related symptoms (n = 502).
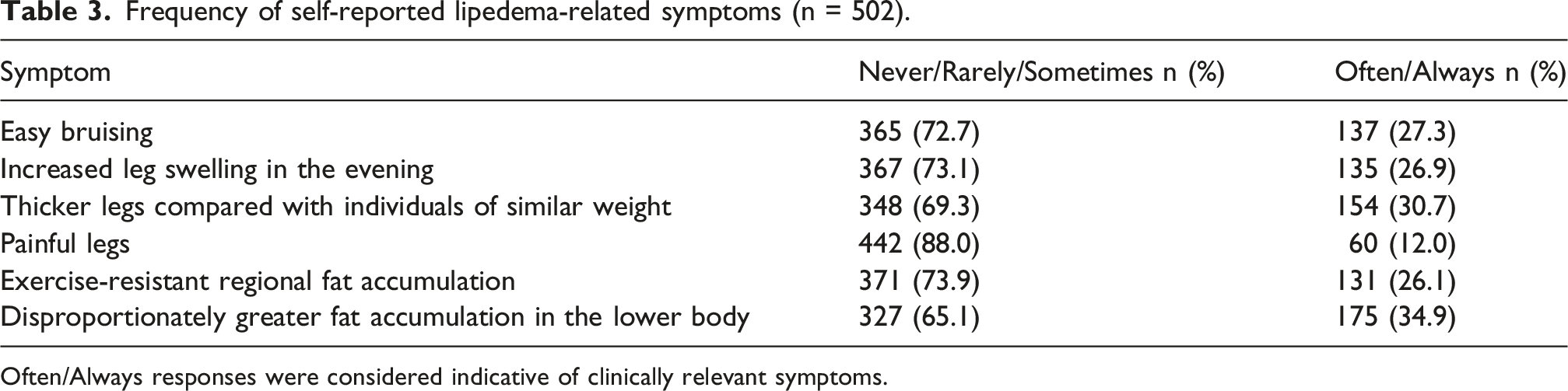
Often/Always responses were considered indicative of clinically relevant symptoms.
Self-perceived lipedema status and family history
Regarding self-perceived disease status, 106 participants (21.1%) believed that they might have lipedema, whereas 194 (38.6%) believed they did not, and 202 (40.2%) reported uncertainty. A family history of similar symptoms among female relatives was reported by 171 participants (34.1%), while 192 (38.2%) denied such a history and 139 (27.7%) were unsure.
Healthcare-seeking behavior and diagnostic outcomes
Among the participants, 50 of 502 (10.0%) reported having consulted a healthcare professional regarding their symptoms, whereas 452 (90.0%) had not sought professional evaluation. Regarding diagnostic outcomes, 21 participants (4.2%) reported lipedema, 28 (5.6%) reported varicose veins, 8 (1.6%) reported obesity, and 2 (0.4%) reported lymphedema. Notably, the majority of participants (80.1%) indicated that no diagnosis had been established, and 41 (8.2%) reported that they could not recall whether a diagnosis had been made.
Misconceptions regarding lipedema
More than half of the participants (51.8%) reported confusing lipedema with cellulite, whereas approximately one quarter (24.3%) associated lipedema with obesity. Confusion with lymphedema was reported by 35.9% of respondents. In contrast, fewer participants confused lipedema with rheumatic diseases (10.2%). Notably, a substantial proportion of respondents (23.5%) indicated uncertainty by selecting the “I do not know” option.
Sources of information about lipedema
Among the participants, social media emerged as the most frequently reported source of information about lipedema (48.6%)
Perceptions of healthcare recognition and information needs
Most participants (71.3%) reported a willingness to receive further information about lipedema, whereas 12.0% were not interested and 16.7% were undecided.
Only 19 of 502 participants (3.8%) believed that lipedema is adequately recognized within the healthcare system. More than half of the participants (54.6%) reported that lipedema is not sufficiently taken into account, while 41.6% were uncertain.
Participants most frequently preferred healthcare professionals-provided information as a source for learning about lipedema, followed by e-government health portals and social media–based campaigns, whereas traditional media and printed materials were less commonly preferred (Figure 1). Preferred channels for receiving lipedema-related information among participants. Values above bars indicate percentages.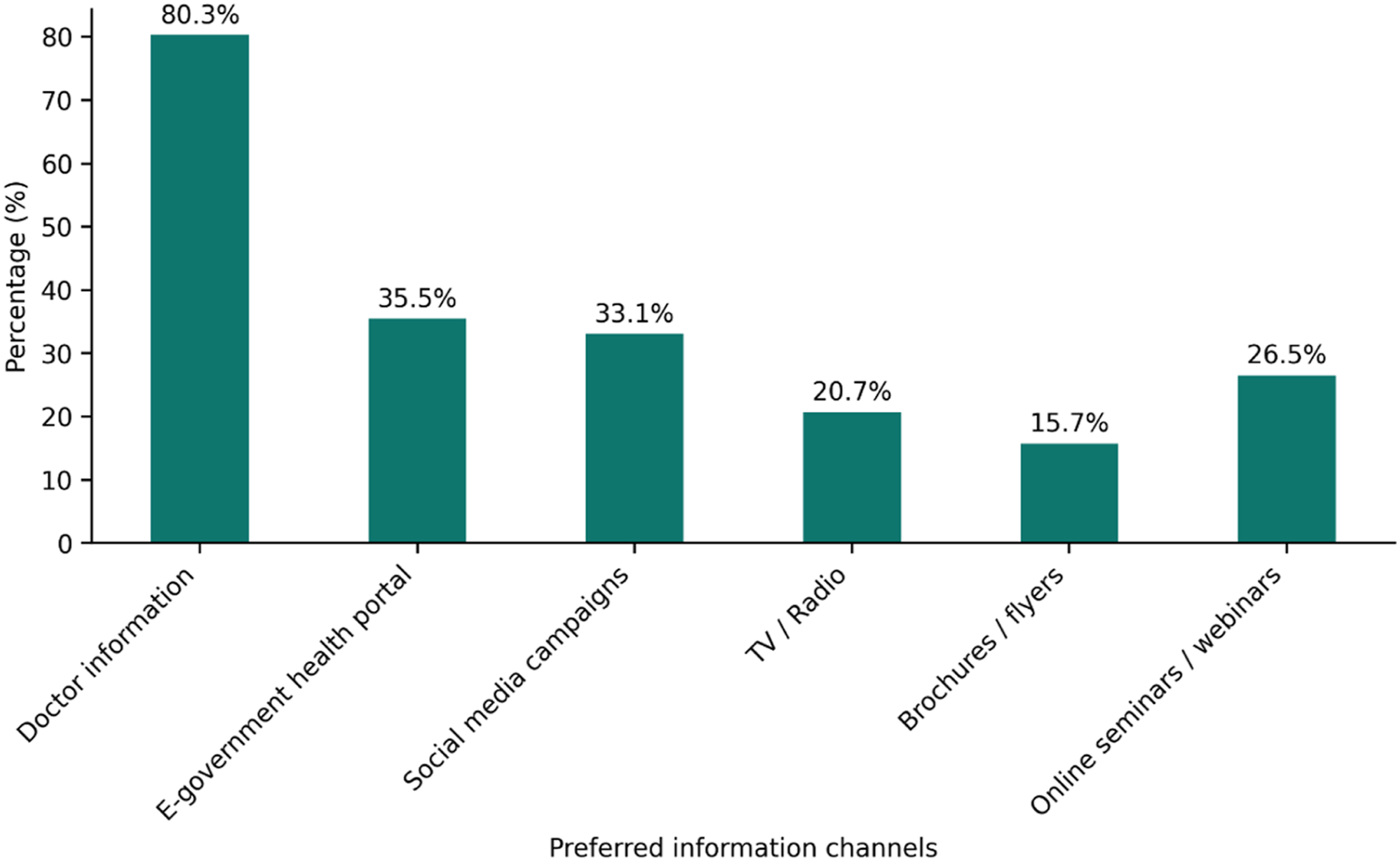
Knowledge score comparisons
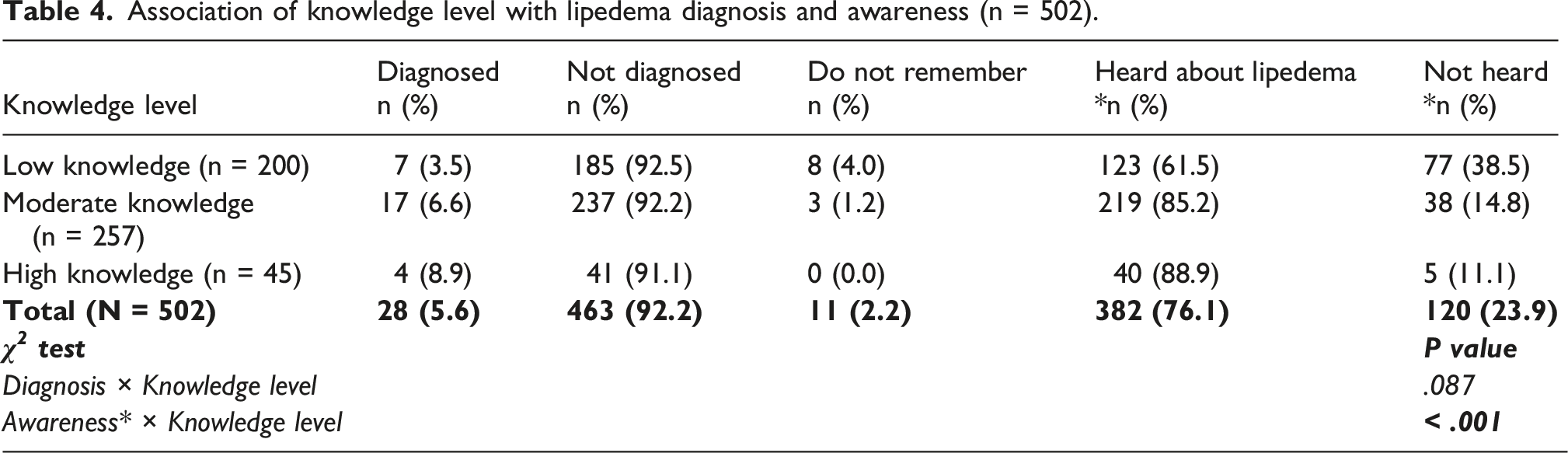
Participants who had heard about lipedema had higher knowledge scores than those who had not (3.03 ± 1.26 vs 1.58 ± 1.72; Welch t-test, p < .001). Knowledge scores did not differ significantly between participants with and without a prior lipedema diagnosis (3.21 ± 1.32 vs 2.68 ± 1.51, respectively; p = .067).
Participants who reported healthcare professionals as a source of lipedema-related information had significantly higher knowledge scores than those who did not (3.48 ± 1.23 vs 2.42 ± 1.51, p < .001). In contrast, participants who reported social media as a source of information showed only slightly higher knowledge scores compared with those who did not (2.82 ± 1.36 vs 2.55 ± 1.64), and this difference did not reach statistical significance (p = .052).
Association of knowledge level with lipedema diagnosis and awareness (n = 502).
Factors associated with self-reported lipedema suspicion
Multivariable logistic regression analysis of factors associated with self-reported lipedema suspicion.
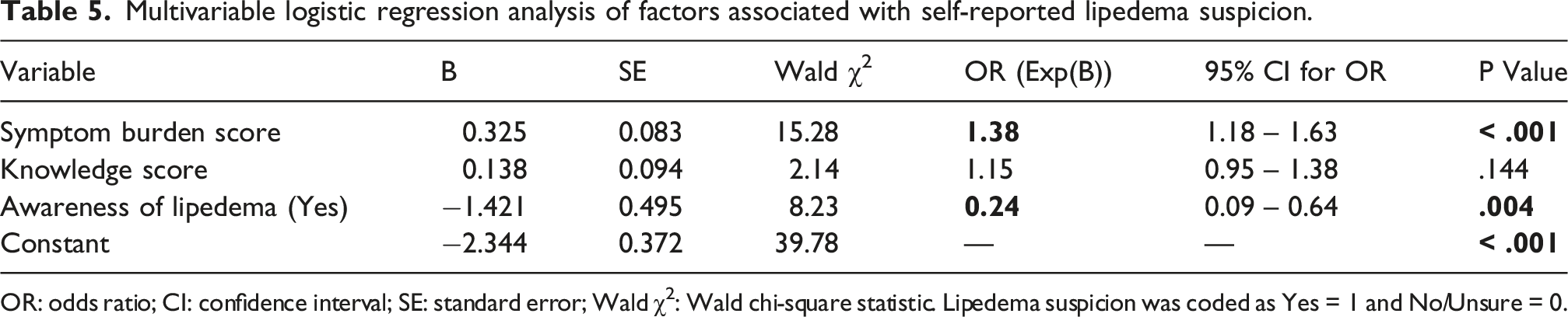
OR: odds ratio; CI: confidence interval; SE: standard error; Wald χ2: Wald chi-square statistic. Lipedema suspicion was coded as Yes = 1 and No/Unsure = 0.
Discussion
This study investigated the awareness, knowledge level, and willingness to receive information about lipedema among women in Turkey, finding that 76.1% of participants reported having previously heard of the condition. Participants of 69.1% correctly identified lipedema as “fat accumulation in the legs and arms in women,” confirming their awareness. The knowledge level of the study population was generally evaluated as low to moderate. Only 9% of participants exhibited a high level of knowledge, while 71.3% reported a willingness to receive further information.
The significant association between having heard of lipedema and the level of knowledge revealed in the study demonstrates the value of awareness for knowledge acquisition. Nonetheless, just awareness might be inadequate for obtaining accurate knowledge. In this study, low to medium levels of knowledge, despite elevated lipedema awareness and correct definitions, may suggest that awareness cannot always be transformed into accurate and sufficient knowledge. One of the various reasons for this situation could be the source of the information. In this study, which identifies social media as the most frequent source of information, it is noteworthy that participants who regarded social media as an information source did not demonstrate a significant difference in their level of knowledge compared to those who did not. Studies similar to ours, but conducted on Swedish and Czech women diagnosed with lipedema, showed that when asked where they first heard about lipedema, participants most frequently answered social media and online platforms, respectively.21,23 In addition, the article dealing with the issue of lipedema in Spain indicates that awareness is mostly generated by social media, but this results in an increase in non-scientific information and, consequently, confusion. 24 This situation highlights the importance of obtaining accurate information from a trustworthy source about lipedema, a health problem that is not yet sufficiently recognized by society. In the current study, participants who identified healthcare professionals as a source of information had significantly higher levels of knowledge compared to those who did not, which is another finding demonstrating the importance of the information source.
When examining the willingness to receive information, it was determined that the majority of participants reported a desire for more knowledge concerning lipedema, identifying official entities such as healthcare professionals and the e-government health portal as sources for this information. However, the majority of participants also reported that healthcare professionals do not adequately regard lipedema. The literature has frequently emphasized problems like healthcare professionals’ ignorance of lipedema and their mistaken and delayed diagnosis.11,23,25,26 A recent study in Turkey has shown a lack of awareness and knowledge about lipedema among physicians. 18 The lack of a significant association between diagnosis and knowledge level in this recent study may indicate that even patients who have received a diagnosis can not receive adequate information. This result may contribute to growing evidence of a lack of knowledge, awareness, or information-giving in the healthcare system.23,27,28
The additional subjects evaluated in this study were self-reported symptom burden, self-reported lipedema suspicion, self-perceived lipedema status, healthcare-seeking behavior, and misconceptions about lipedema. Multivariate analyses suggested that individuals largely based their clinical suspicion on the severity of their experienced symptoms, showing that symptom burden was the strongest predictor of self-reported lipedema suspicion. This could be because individuals tend to research this topic as their symptoms worsen, leading to the emergence of lipedema suspicions. In contrast, the reverse association between lipedema awareness and suspicion could suggest that as awareness increases, symptoms are interpreted more accurately and distinctively, preventing misconceptions.
In addition, in this study, out of 106 participants who believed they had lipedema and 202 participants who reported uncertainty, only 50 participants reported receiving a professional evaluation. This situation may arise from the perception that the healthcare system does not adequately recognize lipedema or from individuals’ lack of awareness regarding their symptoms or the associated clinical entities.
Our results support the findings in the literature in terms of the need to improve awareness and knowledge levels of lipedema among the public and healthcare professionals.18,25 Increasing individuals’ awareness and knowledge can contribute to a more accurate estimation of the potential causes of symptoms experienced by those who are experiencing them. Thereby, the process leading to the correct diagnosis can be supported. Additionally, increased awareness and knowledge can accelerate the diagnostic process, facilitating early intervention and minimizing morbidity. One of the future goals may be to increase the knowledge levels of healthcare professionals by including more information about lipedema in their training and to ensure that the public receives accurate information from healthcare professionals.
There are some limitations to this online survey study. The fact that the majority of participants have a high school education or higher may have led to the finding that awareness, knowledge, and willingness for information are higher than they actually are. Additionally, the fact that almost half of the participants are from the Marmara region affects the generalizability of the results to the entire country. Due to the voluntary nature of survey participation, those interested in lipedema may engage more frequently, leading to potential bias. However, in cases of voluntary participation, this circumstance is unavoidable. In this study, the authors used a questionnaire they designed based on existing guidelines. However, there are likely other factors that the survey did not examine. For example, the survey excluded inquiries regarding lipedema treatment. This situation highlights the need for validated and reliable assessment tools to evaluate lipedema awareness and knowledge levels among healthy or diagnosed individuals in society. This study was conducted among women in Turkey and is a local study; the findings may not reflect the global situation.
In conclusion, this survey study examined the awareness, knowledge level, and willingness to receive information about lipedema among women in Turkey, revealing that most participants were aware of the disease. However, a low-to-medium level of knowledge was identified. Although participants most frequently reported that they obtained information from social media, it was determined that those who received information from healthcare professionals had a higher level of knowledge compared to those who did not. The majority of participants expressed a desire for more information from healthcare professionals and government agencies, respectively. Nevertheless, another significant finding was the perception that the healthcare system does not take lipedema seriously enough. In the future, policies may be developed to increase awareness and knowledge levels of lipedema among both the public and healthcare professionals. Future studies ought to emphasize enhancing the accuracy and generalizability of results by engaging larger and more homogeneous populations via surveys with established validity and reliability.
Supplemental material
Supplemental material - Women’s awareness and knowledge of lipedema in Turkey: Findings from a nationwide online survey
Supplemental material for Women’s awareness and knowledge of lipedema in Turkey: Findings from a nationwide online survey by Zeynep Candan, Feyza Nur Yücel, Emre Ata in Phlebology.
Footnotes
Ethical considerations
The study was approved by the Hamidiye Scientific Research Ethics Committee of the University of Health Sciences (Meeting date: 11.09.25, registration no: 25/676, decision no: 17/9).
Consent to participate
Participants indicated their informed consent at the beginning of the survey.
Consent for publication
Participants consented to the study by voluntarily completing an anonymous survey online.
Author contributions
Concept and design of the manuscript, preparing and conducting the survey (Z.C, F.N.Y.), data analysis (F.N.Y), collection of literature (Z.C, F.N.Y, E.A), original draft preparation (Z.C, F.N.Y); project administration (F.N.Y, E.A); review and editing (Z.C, F.N.Y); editing and final approval (Z.C, F.N.Y, E.A.). All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Guarantor
Zeynep Candan, the corresponding author, is the guarantor of this manuscript and takes responsibility for the integrity of the work as a whole.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.