
Abstract
Introduction
Management of chronic venous disease (CVD) has shifted from high ligation and stripping (HL/S) to multiple endovenous options, yet no single technique is optimal for all anatomical patterns or patient profiles. This narrative review aimed to summarize current evidence and guideline recommendations and outline an anatomy-oriented framework for modality selection in daily practice.
Methods
A non-systematic search of MEDLINE and current guidelines from the European Society for Vascular Surgery and the Society for Vascular Surgery/American Venous Forum/American Vein and Lymphatic Society was performed, focusing on comparative trials, long-term series and key reviews of HL/S, endovenous thermal techniques (TT), cyanoacrylate closure (CAC), mechanochemical ablation (MOCA) and ultrasound-guided foam sclerotherapy (UGFS). Evidence was synthesized descriptively with attention to anatomical indications, efficacy and complications.
Results
HL/S remains valuable for markedly dilated, aneurysmal or tortuous trunks, epifascial segments and junctional disease with thrombus or unfavorable anatomy, and may provide durable occlusion in very large veins. TT is the best-studied modality, achieving high occlusion rates, rapid recovery and broad applicability across typical truncal diameters, but efficacy and skin-related events are problematic in superficial or extremely large veins. CAC and MOCA, as non-thermal non-tumescent options, offer excellent periprocedural comfort and avoid thermal nerve injury, making them attractive for below-the-knee segments; however, durability appears less robust in large-diameter or long trunks and both incur higher device-related costs. CAC is uniquely associated with phlebitis-like abnormal reaction or hypersensitivity. UGFS remains a versatile option for complex recurrent varices and neovascularization but is less suitable as a first-line treatment for truncal reflux.
Conclusions
No single “gold-standard” modality suffices for all CVD presentations. An anatomy- and patient-centered strategy that deliberately deploys all available modalities or hybrid combinations based on vein diameter, depth, length and patient factors is essential to optimize occlusion and minimize complications in daily practice.
Keywords
Introduction
Since the early 2000s, the treatment of chronic venous disease (CVD) has undergone remarkable changes and developments. There has been a striking transition from high ligation and stripping (HL/S) to minimally invasive endovenous techniques, accompanied by the rapid development of various related devices and treatment modalities. Consequently, endovenous thermal techniques (TT)—including endovenous laser ablation (EVLA) and radiofrequency ablation (RFA)—has become the standard care in literature, largely because multiple trials have demonstrated equivalent or better efficacy and quality-of-life outcomes compared with conventional surgery, together with faster recovery and less perioperative morbidity.1–3
Recently, a group of non-thermal non-tumescent (NTNT) modalities—including mechanochemical ablation (MOCA) and cyanoacrylate closure (CAC)—have emerged as an attractive alternative that avoids tumescent anesthesia and thermal nerve injury. Early and some long-term studies suggest that MOCA and CAC can achieve anatomical success rates approaching those of TT.4,5 Therefore, recent guidelines present TT and NTNT at an almost equivalent level in CVD treatment and state that these techniques may be selected based on the circumstances of the operator and patient.6,7
However, no single modality is ideal for all patients or for all patterns of CVD, because the condition of the veins and their anatomical configuration differ greatly from one patient to another. For instance, when choosing a treatment method, the physician must consider factors such as vein diameter and length, depth from the skin, tortuosity, aneurysmal changes, junctional anatomy, and whether the target segment is above or below the knee, as well as patient-specific factors such as comorbidities, tolerance for tumescent anesthesia, cosmetic priorities, and cost sensitivity, to move closer to truly optimal treatment for each patient.
In an era of multiple competing modalities, clinicians increasingly face a problem of “choice overload,” and evidence-based, anatomy-driven algorithms are needed to match the right modality to the right patient. This review aimed to summarize the key characteristics, strengths, and limitations of the major treatment options for varicose veins, such as HL/S, EVLA, RFA, MOCA, CAC, and ultrasound-guided foam sclerotherapy (UGFS), and integrate current evidence with practical considerations to propose a strategic, anatomy-oriented conceptual framework for modality selection in daily practice. The principal contribution of this review is to translate modality-specific evidence and guideline recommendations into practical anatomical and patient-related considerations for everyday treatment planning.
Methods
A non-systematic narrative search of MEDLINE/PubMed was performed to identify comparative trials, long-term series, meta-analyses, and key reviews addressing HL/S, endovenous TT, CAC, MOCA, and UGFS. The search covered publications from 2000 to 2025 using combinations of keywords such as “chronic venous disease,” “varicose veins,” “great saphenous vein,” “endovenous laser ablation,” “radiofrequency ablation,” “cyanoacrylate closure,” “mechanochemical ablation,” and “foam sclerotherapy.” Current guidelines from the European Society for Vascular Surgery and the Society for Vascular Surgery/American Venous Forum/American Vein and Lymphatic Society were also reviewed. Evidence was synthesized descriptively rather than quantitatively, with attention to anatomical indications, efficacy, complications, and practical considerations for modality selection. Because this was a narrative review, the author did not aim to capture all available studies exhaustively and did not perform a formal risk-of-bias assessment.
High ligation and surgical stripping (HL/S)
Advantages
HL/S is the most traditional and longest-established operative method for CVD treatment. One of its advantages is the sense of certainty it provides, because the surgeon directly visualizes the target veins throughout the procedure.
HL/S can also be applied when puncture or endovenous access to the target vein is difficult. In some patients, the saphenous vein is difficult to puncture, has poor straightness with pronounced tortuosity, or thrombophlebitic event, such that endovenous catheters or fibers cannot be advanced smoothly or would require multiple puncture sites. In such situations, HL/S remains a reliable option independent of endovenous access.
Another advantage of HL/S is in cases where thrombus is present within the saphenous trunk, particularly near the junction of the deep venous system. Advancing wires, catheters, or fibers in this setting may theoretically dislodge and propagate thrombus locally or systemically. Therefore, when thrombus is located within the segment that needs to be treated, surgical interventions such as partial stripping or local resection may be the most appropriate and safest strategy.
In patients with dilated or aneurysmal change near the junction, unfavorable junctional anatomy was associated with an increased risk of endovenous heat-induced thrombosis (EHIT) after endovenous thermal ablation (ETA).8,9 In contrast, surgical high ligation is not affected by the presence of a junctional aneurysm in the same way, and is essentially free from TT-related EHIT concerns in this clinical scenario.
Since the widespread adoption of endovenous modalities, baseline vein diameter has been identified as one of the strongest predictive factors for recurrence, particularly recanalization, after treatment. This has been demonstrated in TT and NTNT alike.10,11 When the vein diameter is large, the volume and surface area of the venous wall increases, and the intraluminal blood volume also increases. To achieve effective thermal or chemical damage to the endothelium in such large-caliber veins, more intensive intervention is inevitably required. For TT, this means delivering higher total energy or higher linear endovenous energy density (LEED); for NTNT techniques, it may require injecting a larger amount of cyanoacrylate glue and/or increasing the degree of mechanical or chemical abrasion. However, intensifying these parameters naturally tends to increase procedure-related pain and may adversely affect postprocedural recovery.
Even if the author considers CAC alone, when the vein diameter doubles, the luminal volume increases by a factor of approximately four-fold and not double. Thus, simply adding one or two extra glue injections may be insufficient to achieve complete occlusion of this markedly increased volume. In contrast, with HL/S, an increase in vein diameter does not by itself lead to a higher revascularization rate, because the diseased trunk segment is physically removed. Although TT can achieve good occlusion rates even in relatively large-diameter veins, no long-term data exists on stable anatomic closure in extremely aneurysmal veins or in trunks approaching 15–20 mm in diameter. In the author’s opinion, one of the greatest advantages of HL/S is that it allows the operator to treat very large-diameter veins without the same degree of concern about revascularization or recurrence that exists with endovenous modalities.
Recently published SVS/AVF/AVLS guidelines explicitly note that, in patients with an epifascial or very superficial saphenous vein, mini-phlebectomy or limited stripping has advantages over TT or NTNT in preventing skin burns, hyperpigmentation, and induration.6,7 Similarly, CAC was associated with phlebitis-like abnormal reactions (PLAR) or irritation and hypersensitivity phenomena that are particularly likely to occur when the treated saphenous segment lies close to the skin or is epifascial.12,13 These observations further support the role of surgical removal (or limited stripping) in managing epifascial or superficial trunks.
Finally, although cost-effectiveness varies widely between healthcare systems and countries, HL/S can be performed at substantially lower cost in some countries. In this context, HL/S is often feasible at approximately one-half to one-third of the cost of other endovenous modalities, representing a significant economic advantage for patients in the author’s country.
Limitations and drawbacks
The limitations and drawbacks of HL/S are, straightforward. Since the procedure is performed through surgical incisions, it inevitably leaves scars, and the physical act of avulsing or stripping the vein tends to produce more extensive ecchymosis and postoperative pain than that with endovenous modalities, with a correspondingly longer recovery period and slower return to normal activities.2,14,15 However, some randomized trials have reported broadly comparable levels of postoperative pain between HL/S and endovenous laser ablation, suggesting that adequate perivenous tumescent infiltration can at least partially offset this traditional disadvantage.16,17
Nerve injury can also be more pronounced after HL/S, particularly when the below-the-knee (BTK) segment of the saphenous vein is stripped. Clinically relevant rates of saphenous nerve injury have been documented after saphenous vein stripping, and more extensive and distal stripping was associated with higher rates or greater severity of sensory disturbance along the saphenous nerve distribution.18,19 Thus, when BTK disease is treated with stripping rather than endovenous techniques, the risk of nerve-related morbidity becomes a major practical limitation.
Recurrence following HL/S is a challenge and the mechanisms of recurrence differ fundamentally between HL/S and endovenous modalities. Recurrence after endovenous treatment is related to recanalization of a previously treated truncal vein, leading to persistent/recurrent reflux. In contrast, recurrence after stripping is more often associated with neovascularization at the high ligation site and other changes that are captured within the framework of recurrent varices after surgery (REVAS).14,20,21 In theory, if high ligation is performed accurately and the saphenous trunk is completely stripped, REVAS should be minimal aside from a subset of cases driven by neovascularization. In everyday practice, however, recurrent varicose veins after HL/S are strongly influenced by anatomic variables that are difficult to predict pre-operatively, such as previously unrecognized or newly developed perforating veins, communicating veins, and other complex patterns of reflux.20,21
In addition, when the patient is markedly obese, HL/S becomes even less favorable. To expose and control the saphenofemoral junction (SFJ) or saphenopopliteal junction (SPJ), larger skin incisions and more extensive dissection may be required, which can increase tissue trauma, bleeding, wound-related problems, and the risk of nerve injury.2,22 In such patients, HL/S is clearly at a disadvantage compared with endovenous techniques, which allow junctional treatment through percutaneous access with minimal disruption of overlying soft tissues.
Endovenous thermal techniques (TT) – EVLA, RFA
Endovenous TT, represented primarily by EVLA and RFA, are the most popular treatments for CVD worldwide. In contemporary guidelines, TT is also the best-studied and most strongly recommended standard therapy, with high levels of evidence compared with other endovenous modalities and conventional surgery.1,2,6,7,14,15,23 Other thermal methods, such as endovenous steam ablation, show acceptable short-term efficacy, but the overall clinical evidence remains relatively limited, and the author have no personal experience with these techniques; therefore, they are not discussed further in this review.24,25
EVLA and RFA are delivered through a variety of generators and disposable devices that differ somewhat between countries and institutions. In the author’s country, commonly used RFA systems include the ClosureFast device (Medtronic; Minneapolis, Minnesota, USA), VeinCLEAR system (RF Medical; Seoul, South Korea), and VENISTAR system (STARmed; Goyang, South Korea). For EVLA, the author has treated patients using 980-nm, 1470-nm, and 1940-nm diode laser platforms. Regarding fibers, the author previously used bare-tip fibers but currently employs radial fibers. Peri-procedural symptoms after EVLA may also be influenced by fiber-related variables, including fiber design, jacket-type, emission profile, and bare-tip versus radial fiber configuration.
Although the technical principles and methods of use of RFA and EVLA differ, the intraoperative workflow, peri-procedural patient experience, and clinical end points (occlusion rate, pain scores, recovery time, and complication rates) have progressively converged. Historically, during the early generation EVLA era using 810- or 980-nm wavelengths and bare fibers, several randomized trials and meta-analyses reported that RFA was associated with less post-procedural pain and bruising than that observed with EVLA using lower wavelength.14,15,23 However, with the widespread adoption of higher wavelength (1470-nm and 1940-nm) EVLA and radial fibers, several studies have shown that differences between EVLA and RFA in terms of procedure-related pain, ecchymosis, and early outcomes have become minimal or clinically negligible, and in some series higher wavelength EVLA has even demonstrated slight advantages in selected subgroups with large diameter veins.26–28 On the basis of these observations, although the two techniques retain different handling characteristics from the operator’s perspective, their fundamental clinical profile and the outcomes perceived by patients are now very similar. Therefore, in this review the author did not attempt to separate EVLA and RFA into distinct categories but rather discussed them together under the common heading of endovenous TT.
Advantages
From a historical standpoint, TT has been compared directly with HL/S and has become firmly established as an alternative treatment modality with multiple advantages over conventional surgery. In randomized trials, Cochrane reviews, and meta-analyses, TT has consistently shown lower rates of procedure-related bleeding, hematoma, wound infection, and other incision-related problems than that observed with HL/S, along with reduced postoperative pain and faster recovery, including an earlier return to normal daily activities and work.2,3,14,15,23 These benefits are closely related to the minimally invasive, percutaneous nature of TT, which avoids groin incisions and long stripping tracks.
As mentioned earlier in regard to HL/S, the relative advantage of TT becomes even more pronounced in obese patients. In such patients, surgical exposure of SFJ or SPJ typically requires larger incisions and more extensive soft-tissue dissection, which can increase bleeding, wound complications, and postoperative discomfort. By contrast, TT enables treatment of SFJ or SPJ reflux through ultrasound-guided percutaneous access, with minimal disruption of the overlying adipose tissue and skin. This makes junctional treatment substantially easier and less morbid in obese individuals than that with HL/S.
Similarly, when BTK segments of the great saphenous vein require treatment, the risk of saphenous nerve injury is an important practical concern. Extensive BTK stripping has been associated with clinically relevant saphenous nerve injury and long-lasting sensory disturbance,18,19 whereas TT offers the possibility of treating BTK reflux with a more controlled thermal profile and limited dissection. Although nerve injury can still occur with TT, especially if tumescent anesthesia is inadequate, the overall risk of nerve-related morbidity is generally considered to be lower than that with long-segment BTK stripping.29–31
Finally, because TT has effectively become the standard endovenous approach in current practice and guidelines,1,6,7,23 it has the practical advantage of being applicable to the great majority of typical CVD cases encountered in daily clinical work. With appropriate selection of energy parameters and tumescent anesthesia, TT can be adapted to a wide range of truncal vein diameters and anatomic variations, providing a versatile and broadly applicable “workhorse” modality for the endovenous treatment of saphenous reflux.
Limitations and drawbacks
The limitations of TT are quite restricted, which is precisely why most contemporary guidelines recommend TT as a first-line option over other modalities in the treatment of CVD.1,6,7 Nevertheless, because TT relies on intraluminal heat to destroy endothelial cells, induce damage to the vein wall, and trigger inflammation and subsequent fibrosis, it inevitably carries its own specific drawbacks.
First, when the target saphenous vein runs in an epifascial or very superficial plane, there is a real risk of skin burns and hyperpigmentation. As noted earlier, the recent SVS/AVF/AVLS guidelines explicitly state that if the saphenous vein is close to the skin (e.g. <0.5 cm from the skin surface), thermal ablation may result in skin burns, hyperpigmentation, or induration. Therefore, in this clinical setting, the guidelines suggest that mini-phlebectomy or limited stripping may be more effective option than TT to reduce skin-related adverse events.6,7 Even with meticulous and generous tumescent infiltration to protect the skin and subcutaneous tissues—which can substantially reduce the risk of true skin burns—it remains difficult in practice to prevent hyperpigmentation completely in such cases.
Second, TT can be technically challenging when the course of the vein is not straight and endovenous access or device advancement is not easily achieved in a single pass. Examples include marked tortuosity, focal aneurysmal changes, segments with fibrotic transformation after previous phlebitis, or the presence of intraluminal thrombus. In these scenarios, advancing a catheter or laser fiber can be difficult or unsafe, and in some patients a limited stripping, segmental phlebectomy or UGFS may be easier and more straightforward than attempting TT.
Even in large diameter veins, TT could achieve good occlusion rates and favorable clinical outcomes.10,26 However, as the vein diameter increases, it often becomes necessary to use higher levels of thermal energy than would be needed for a smaller caliber trunk. In practice, increasing vein diameter often prompts operators to deliver higher total thermal energy—by applying higher LEED in EVLA or by modifying segmental treatment patterns in RFA—although specific strategies vary between systems and are not well-standardized.26,32,33
Once higher thermal doses are used for large vein, it is almost inevitable that peri-procedural pain and perivenous tissue injury will increase compared with TT protocols that employ lower energy. Several studies evaluating “higher-energy” EVLA of the great saphenous vein have indeed reported greater postoperative pain, bruising, and induration when elevated LEEDs are applied, illustrating the trade-off between energy delivery and local morbidity.34–38
In contrast, because HL/S physically removes the diseased trunk, its technical success is less directly dependent on vein diameter once the vein has been properly ligated and stripped. Thus, while many operators can expect TT to provide lower pain scores and at least comparable recurrence rates to HL/S in veins of more typical caliber—for instance, in great saphenous veins up to around 8–10 mm in diameter—this advantage becomes less certain in the setting of markedly enlarged trunk. In such extreme cases, it is difficult to conclude that TT is consistently less painful and less prone to recurrence than that with HL/S.
Finally, compared with HL/S, TT inevitably requires dedicated capital equipment (laser generator or RF console) and single-use consumables such as catheters or fibers. Multiple economic evaluations have shown that these device-related costs generally make TT more expensive than HL/S at the procedure level. 39 This cost differential remains an important limitation of TT in healthcare systems where reimbursement is constrained or where patients bear a substantial proportion of treatment expenses out of their pocket.
Cyanoacrylate closure (CAC)
CAC treatment is a representative NTNT modality that received CE marking in Europe in 2011 and US FDA approval in 2015. Unlike HL/S or TT, which rely on surgical removal or thermal destruction of the venous wall to eliminate reflux, CAC works by injecting a cyanoacrylate glue material into the refluxing saphenous vein segment and sealing the lumen to block reflux. Several CAC systems are currently available worldwide, all based on cyanoacrylate monomers but incorporating different proprietary additives. Consequently, there are meaningful differences between products in terms of glue viscosity, polymerization speed, and details of the instructions for use (IFU).40,41
Advantages
The greatest advantage of CAC is that intra- and early post-procedural pain are significantly lower than that with HL/S or TT.5,42 Because CAC does not require tumescent injections, patients are spared the discomfort associated with multiple tumescent needle passes. In clinical trials in which concomitant phlebectomy was either not performed or carefully standardized, CAC has shown closure rates and postoperative pain scores that are comparable or even superior to that of TT, despite not requiring compression stockings in the CAC arm, whereas stockings were routinely used after TT.1,6,7,42,43 These findings are most clearly illustrated in the VeClose randomized trial and its long-term extensions, in which CAC demonstrated non-inferior anatomic success, similar or better early pain scores, and faster return to normal activities when compared with that of RFA.5,42,44,45
As per the recent guidelines, when treating BTK disease—particularly reflux in the lower calf segment—NTNT modalities are attractive options because they avoid thermal energy and thereby eliminate the risk of thermal nerve injury in this vulnerable zone.6,7 In this specific anatomic context, CAC can be considered to be a safer alternative to TT from the standpoint of nerve preservation.
From the perspective of anatomic efficacy, CAC could achieve closure rates that are broadly equivalent to those of TT, at least in the short-to mid-term, and patient-reported satisfaction was also high.5,23,42–44 A recent systematic review and meta-analysis of CAC reported 12-months closure rates of approximately 95%–97%, with no significant differences in anatomic success compared with EVLA or RFA, and with fewer mild adverse events and better periprocedural pain and recovery profiles. 43
When CAC is compared with MOCA within the broader NTNT group, several analyses have suggested that CAC may offer somewhat higher anatomic closure rates, although both techniques typically achieve favorable occlusion in appropriately selected cases.45,46 Taken together, these data support the view that CAC occupies a strong position within the NTNT spectrum with high anatomic success. 1
Limitations and drawbacks
The most obvious drawback of CAC is its higher cost compared with more established modalities. Although CAC does not require capital equipment such as a laser generator or RF console, the single-use adhesive kit is substantially more expensive than the fibers or catheters used for TT in most healthcare systems. In cost analyses and health technology assessments, these device-related costs consistently make CAC more expensive at the procedure level than those of HL/S or TT, even when the absence of tumescent anesthesia and compression stockings is taken into account.39,43 The magnitude of this cost difference, however, varies considerably between countries and reimbursement environments. Anyway, no current evidence demonstrates that CAC is more cost-effective than established modalities such as TT or HL/S.
Several studies and guideline discussions have also raised concerns regarding CAC efficacy in very large-diameter veins. Some data indicate that larger baseline saphenous diameter is an important predictor of recanalization after CAC, with failure risk increasing as the trunk diameter approaches or exceeds 6.6 mm or 12 mm.11,47
Although some authors have proposed that “additional injections” of glue could compensate for the larger luminal volume in these veins, the basic geometric relationship between radius and volume (volume increasing with the cube of the radius) implies that there are inherent limitations to what can be achieved simply by adding a small number of extra glue deliveries.11,43,46,48,49
In practical terms, currently the most widely used VenaSealTM closure system (Medtronic, Minneapolis, Minn) contains 5 mL of glue in a single kit. In routine practice, this volume may be insufficient to cover multiple saphenous veins in one session—for instance, bilateral GSV reflux in tall patients, or combined treatment of GSV, SSV, and accessory saphenous veins—so that, unlike HL/S or TT, CAC cannot treat extensive length or multiple saphenous veins with a single disposable unit. In such situations, either multiple CAC kits or a staged strategy may be required, which further amplifies the cost disadvantage compared with those of HL/S or TT.
The most widely discussed complications of CAC are PLAR and related irritation or hypersensitivity phenomena. Although the underlying mechanisms have not yet been fully elucidated, clinical and histopathologic data suggest that these reactions span a spectrum from transient, “irritation-like” phlebitic changes that resolve spontaneously, to true type IV hypersensitivity with characteristic histologic patterns on excised vein segments.12,13,50,51 In the many published series, PLAR often presents with localized pain, erythema, and pruritus several days after the procedure.12,13,50 Most reactions improve with conservative, symptomatic management using nonsteroidal anti-inflammatory drugs, antihistamines, and short courses of corticosteroids. However, when a persistent, biopsy-proven type IV hypersensitivity pattern recurs despite medical therapy, several reports have described surgical excision of the affected vein segments as a definitive management strategy.50,51 In addition, although rare, there is a report of recurrent generalized urticaria following CAC. 52
PLAR is particularly prone to develop when the treated GSV segment is epifascial or very superficial, close to the skin.12,13,53,54 In such cases, the inflammatory reaction is not only more likely to occur but can also be more symptomatic, with substantial pain and pruritus in the early postoperative period. Clinically, this means that some patients may experience a less favorable recovery profile after CAC than they would after TT or HL/S, despite the inherent advantages of a NTNT.
For these reasons, before recommending CAC, the physician should carefully review the patient’s allergy history and provide detailed pre-procedural counseling about the possibility of PLAR and hypersensitivity reactions, including their usual benign course and the small but real risk of persistent symptoms requiring more intensive management. Adequate informed consent and realistic expectation-setting are essential components of safe CAC practice.
Mechanochemical ablation (MOCA)
MOCA, together with CAC, is one of the two major techniques within the NTNT category. It combines mechanical abrasion of the venous endothelium with the simultaneous infusion of a sclerosant to induce chemical ablation, thereby provoking inflammation and fibrosis of the vein wall. ClariVein® (Merit Medical, South Jordan, Utah) received FDA clearance in 2008 and the CE mark in 2010, whereas the Flebogrif® (Balton Company Ltd., Warsaw, Poland) system obtained CE approval in 2010. Both devices are classified as MOCA systems, but they differ in several fundamental aspects. 55 ClariVein system uses a liquid sclerosant delivered through a rotating infusion wire that is driven by a battery-powered motor, whereas Flebogrif system employs a manually operated catheter with five cutting element hooks and is designed to be used with foam sclerosant. In both systems, as with CAC, tumescent anesthesia is not required, and there is no thermal damage to surrounding tissues.4,32,46,56,57
Advantages
Like CAC, MOCA has repeatedly been shown to result in less peri-procedural pain and faster recovery than that observed with TT in many series, while providing comparable early occlusion rates and improvements in clinical severity and quality-of-life scores.4,32,46,56 In many respects, MOCA has been grouped together with CAC under the NTNT umbrella in recent guidelines and reviews, although its mechanism of action differs substantially from that of cyanoacrylate-based systems.1,6,7,32,46
As with CAC, current guidelines also emphasize the potential advantages of MOCA when treating reflux in lower calf segments of the saphenous vein, particularly in BTK disease, where avoiding thermal nerve injury is a key priority.1,6,7,29,30 In short-term and early mid-term studies, MOCA has shown anatomic success and clinical outcomes that are broadly comparable to that of TT with low peri-procedural pain scores and rapid return to normal activities.4,32,46
Unlike CAC, the sclerosant used in MOCA does not remain as a solid foreign material within the treated vein. From a biochemical perspective, the sclerosant is metabolized and cleared, leaving no persistent polymerized cast in situ. Consequently, MOCA does not carry the same potential for foreign-body–driven reactions that are uniquely associated with cyanoacrylate glue. For patients who desire NTNT treatment but have a history suggestive of hypersensitivity to cyanoacrylate or are reluctant to accept an intravascular glue implant, MOCA can therefore serve as a valuable alternative.12,13,46,50,51
Limitations and drawbacks
Recently, one of the limitations highlighted for MOCA has been its relatively lower long-term closure rate compared with that of TT and, in some analyses, with CAC. Several clinical studies and systematic reviews have suggested that, although early anatomical success is great, mid-to long-term occlusion tends to decline more rapidly with MOCA than those with TT or CAC, especially in large-diameter veins.4,32,46,56 In particular, follow-up data over 1–3 years indicate that when the treated truncal diameter is > 7 mm, the risk of recanalization or recurrent reflux increases, and closure rates become less robust than that in smaller-caliber veins.58,59
It is also important to recognize that most of the medium- and long-term MOCA data currently available are derived from ClariVein system-based series, whereas published Flebogrif system-based data remain relatively limited. The two systems, although grouped together as MOCA, differ substantially in device design and sclerosant formulation: ClariVein system uses a rotating wire with liquid sclerosant, whereas Flebogrif system uses multiple sharp ‘cutting element’ hooks with foam sclerosant. From a practical standpoint, the mechanical injury created by Flebogrif system appears stronger than that produced by the ClariVein system tip, and the foam formulation may interact differently with the vein wall. However, whether these differences translate into different closure rates or different long-term patterns of efficacy remains to be fully clarified and will require further dedicated studies.26,46,57
Reflecting these uncertainties, the latest ESVS guideline assign MOCA a slightly lower level of evidence or strength of recommendation compared with those of TT or CAC. 1 Therefore, when MOCA is being considered—especially in cases where the target vein diameter is relatively large—the operator should carefully reflect on these issues and the alternative options before deciding on the final treatment strategy.
Because MOCA is fundamentally a sclerosant-based therapy, it shares many of the potential adverse effects associated with liquid or foam sclerosants. In most MOCA protocols, approximately 0.2 mL of sclerosant is injected per centimeter of target vein; in liquid-based systems, the recommended limitation total volume per session is typically around 10 mL, corresponding to roughly 50 cm of truncal vein. Although dilution can extend the length of vein treated, this necessarily increases the total sclerosant dose, which in turn raises the theoretical risk of dose-related adverse events. Therefore, caution is required when treating long segments or multiple truncal veins during the same session.60–62
For foam-based systems such as Flebogrif system, current European recommendations generally advise not exceeding a total foam volume of approximately 16 mL per session. 1 In practice, this recommendation may limit the number of veins that can be treated in a single sitting. Nevertheless, in one study using Flebogrif system, multiple great saphenous veins were treated safely with a mean foam volume of 17.7 mL and a maximum of 31 mL, suggesting that higher total doses can be used under careful monitoring and in experienced hands. 57
As with other sclerosant-based treatments, MOCA is associated with a relatively high likelihood of post-procedural thrombophlebitis in the treated trunk, and studies have reported that thrombophlebitis and hyperpigmentation can occur more frequently when the treated segment is suprafascial or very close to the skin. 63 In these circumstances, current SVS/AVF/AVLS guidelines echo prior recommendations for TT and NTNT, stating that “while nonthermal techniques may cause hyperpigmentation or induration, mini phlebectomy or limited stripping is safe and effective if the saphenous vein is close to the skin (<0.5 cm).”6,7 Thus, in suprafascial disease, the operator should consider whether MOCA or limited surgical removal would best balance efficacy with the risk of skin-related adverse events.
Finally, as with CAC, MOCA relies on dedicated single-use devices that are more expensive than the disposables used for TT or HL/S. Although MOCA does not require capital equipment, these higher device-related costs mean that MOCA is generally more expensive than conventional surgery and not clearly more cost-effective than TT; thus, robust evidence of superior cost-effectiveness is still lacking.
Ultrasound-guided foam sclerotherapy (UGFS)
UGFS has a very long history of use, and accordingly a large body of clinical data. Over time, it has become firmly established as an essential and durable tool in the treatment of CVD, and it continues to occupy an important role in modern practice, particularly for tributary veins and selected truncal or recurrent disease patterns.1,60,64
In more recent comparative studies, however, the occlusion rates achieved by UGFS for truncal vein ablation were significantly lower than those of other techniques, so UGFS is no longer recommended as a first-line option when the primary goal is durable closure of saphenous reflux.1,6,7 Several studies have reported that recurrence is relatively common after direct treatment of GSV reflux with UGFS, and that outcomes are significantly less favorable when the GSV diameter exceeds 6 mm.3,15,64,65 Notably, it must be recognized that UGFS outcomes are highly technique-dependent: injection strategy, foam production method, distribution of injections along the truncal segment, and ultrasound guidance throughout the procedure all have a major influence on efficacy, as emphasized in the European sclerotherapy guidelines. 60
Catheter-directed foam sclerotherapy (CDFS) has been proposed as a means of improving truncal outcomes, by allowing a more controlled, continuous delivery of foam along the saphenous trunk. Some studies and a recent review have reported higher occlusion rates with CDFS compared with conventional UGFS, but the available data are still limited, and further well-designed trials are needed before these findings can be fully incorporated into guideline recommendations.65,66
Despite these limitations in main saphenous trunk ablation, UGFS remains an extremely useful and often elegant option in specific anatomic situations. When the target segment is difficult to cannulate or when advancing an intraluminal device is technically challenging or hazardous, UGFS can provide a simple and highly practical alternative. Similarly, around the SFJ and SPJ, where neovascularization or complex patterns of recurrent varices may be present after previous HL/S, UGFS offers a versatile approach that can be tailored to tortuous or branching reflux pathways and has shown favorable results in dedicated series of recurrent disease.67,68 In these contexts, UGFS remains an important component of the therapeutic armamentarium, complementing surgery, TT, and NTNT techniques rather than competing with them as a universal first-line truncal treatment.
Strategic modality selection
Over years of performing and gaining experience with various treatment modalities, the author has continuously reflected on which option would be most appropriate in a given clinical scenario, and this question formed the basis for this narrative review. Each modality has its own advantages, disadvantages, and unique strengths, and because constraints differ across countries and healthcare settings, a single, absolute gold standard is unlikely to exist. In particular, given that anatomic circumstances vary from patient to patient and that numerous factors must be taken into account, the author believes it is impossible to define a true gold standard in the treatment of CVD.
Summary of indications for each treatment modality.
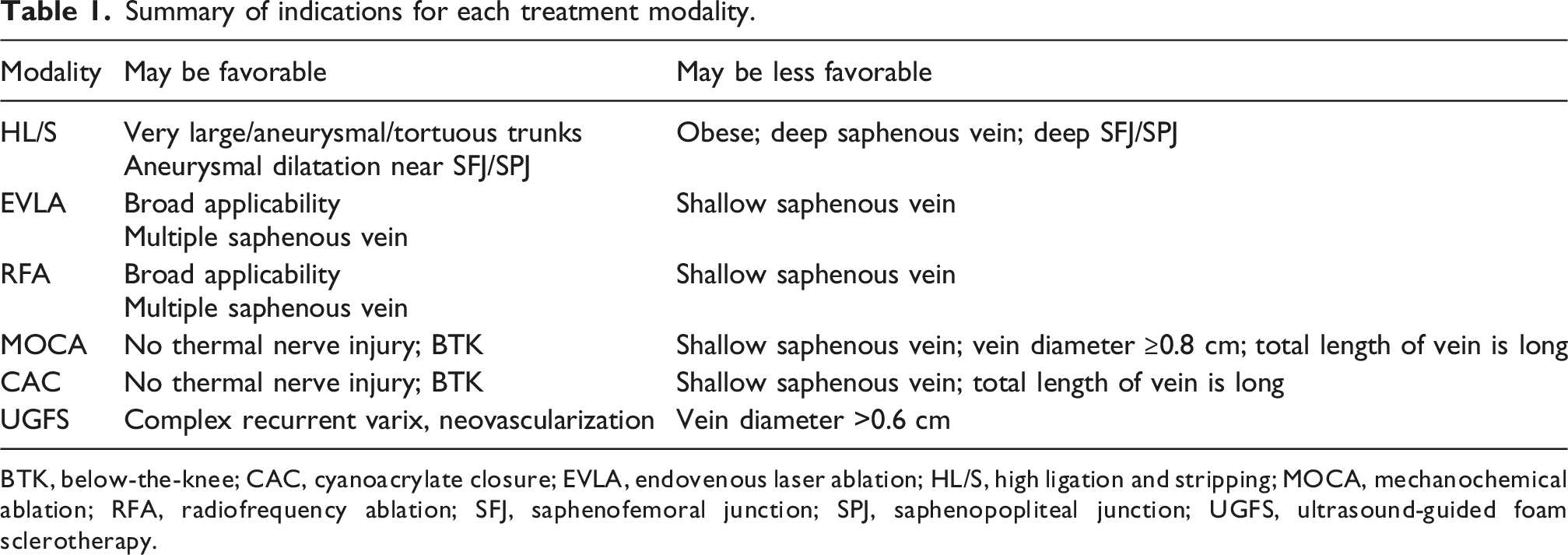
BTK, below-the-knee; CAC, cyanoacrylate closure; EVLA, endovenous laser ablation; HL/S, high ligation and stripping; MOCA, mechanochemical ablation; RFA, radiofrequency ablation; SFJ, saphenofemoral junction; SPJ, saphenopopliteal junction; UGFS, ultrasound-guided foam sclerotherapy.

Conceptual framework for strategic modality selection. BTK, below-the-knee; CAC, cyanoacrylate closure; CVD, chronic venous disease; EVLA, endovenous laser ablation; HL/S, high ligation and stripping; MOCA, mechanochemical ablation; PLAR, phlebitis-like abnormal reactions; RFA, radiofrequency ablation; SFJ, saphenofemoral junction; SPJ, saphenopopliteal junction; UGFS, ultrasound-guided foam sclerotherapy.
The author cautiously predicts that, in the near future, new hybrid approaches combining TT and NTNT will be introduced; perhaps concepts such as thermal ablation and chemical ablation (TACA), thermal ablation with mechanochemical ablation (TAMOCA), or non-tumescent thermal techniques (nTT).
Conclusion
The management of CVD has advanced significantly over the years, with the introduction of minimally invasive techniques that have improved outcomes for patients. Among these, endovenous TT, including EVLA and RFA, remain highly recommended owing to their proven efficacy and broad applicability. However, NTNT techniques such as MOCA and CAC provide promising alternatives, particularly in cases where thermal injury is a concern. Despite their advantages, all treatments present challenges, including cost considerations and limitations based on anatomical variations such as vein diameter, depth and length. Further studies are required to refine these techniques, assess long-term effectiveness, and provide more robust data on cost-effectiveness across different healthcare systems. As the field continues to evolve, a tailored, anatomy-driven approach that prioritizes what is truly best for each patient is essential for optimal outcomes.
Footnotes
Ethical considerations
Not applicable. This article is a narrative review and did not involve human participants, animal subjects, or identifiable patient data.
Author contributions
Insoo Park conceived the topic, performed the literature search, drafted the manuscript, and approved the final version.
Conception and design: IP.
Analysis and interpretation: IP.
Data collection: IP.
Writing the article: IP.
Overall responsibility: IP.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Insoo Park is the guarantor of this work.