
Abstract
Objective:
To investigate the relationship between resilience and affective state, caregiver burden and caregiving strategies among family members of people with traumatic brain or spinal cord injury.
Design:
An observational prospective cross-sectional study.
Setting:
Inpatient and community rehabilitation services.
Subjects:
Convenience sample of 61 family respondents aged 18 years or older at the time of the study and supporting a relative with severe traumatic brain injury (n = 30) or spinal cord injury (n= 31).
Main measures:
Resilience Scale, Positive And Negative Affect Schedule, Caregiver Burden Scale, Functional Independence Measure, Carer’s Assessment of Managing Index.
Results:
Correlational analyses found a significant positive association between family resilience scores and positive affect (rs = 0.67), and a significant negative association with negative affect (rs = −0.47) and caregiver burden scores (rs = −0.47). No association was found between family resilience scores and their relative’s severity of functional impairment. Family members with high resilience scores rated four carer strategies as significantly more helpful than family members with low resilience scores. Between-groups analyses (families supporting relative with traumatic brain injury vs. spinal cord injury) found no significant differences in ratings of the perceived helpfulness of carer strategies once Bonferroni correction for multiple tests was applied.
Conclusions:
Self-rated resilience correlated positively with positive affect, and negatively with negative affect and caregiver burden. These results are consistent with resilience theories which propose that people with high resilience are more likely to display positive adaptation when faced by significant adversity.
Introduction
Extensive research over the past three decades has documented a range of negative impacts experienced by families when a relative sustains a traumatic brain injury or spinal cord injury. These have included psychological distress such as depression and anxiety,1–4 disorganisation of family functioning,5,6 instrumental difficulties (e.g. reduced income, loss of employment)7,8 and reduced life satisfaction.9,10 One cause of these impacts is the nature of the disabling conditions per se. Families report significant stress associated with the behavioural (e.g. anger dyscontrol, increased egocentricity) and cognitive (e.g. impaired attention, reduced memory, executive dysfunction) impairments characteristic of traumatic brain injury.11,12 In contrast, the care challenges after spinal cord injury principally relate to providing for physical support needs. 13
Factors such as kinship status, 14 the availability of attendant care 10 and perceived social support5,11 can modify the extent of distress experienced by family members. One factor that is yet to be systematically explored is the role of resilience.15,16 Although the theoretical application of resilience to family adaptation after traumatic brain injury has been canvassed,17,18 to the best of our knowledge there have been no empirical investigations into the importance of resilience among family members supporting relatives with either type of disability.
Resilience is a multidimensional construct constituting a range of thoughts (e.g. positive outlook), feelings (e.g. hopefulness, sense of humour), and behaviours (e.g. capacity to mobilise social and economic resources). 16 Resilience can be defined as a ‘dynamic process encompassing positive adaptation within the context of significant adversity’. 19 Such a definition reflects a growing consensus that resilience does not consist of fixed personality traits, but rather is a set of skills which can be learned.16,20,21 Research in clinical and non-clinical samples has suggested that people displaying higher resilience report relatively healthier levels of psychological adaptation and functioning in the face of either acute or chronic traumatic events.22,23
In this light, Wagnild and Young 24 have called for research into the relationship between burden, distress and resilience variables among caregivers, and the current study conducts such an inquiry among family members supporting relatives with traumatic brain injury or spinal cord injury. Consistent with the adaptive understanding of resilience, a range of generic skills (e.g. personal and social competence, personal structure) 16 associated with high resilience across a range of different life challenges and trauma have been identified.25,26 Relating this adaptive concept to the rehabilitation context, little is known about whether families with higher resilience display different approaches to caregiving in contrast to families with lower resilience. Finally, comparing families supporting relatives with two different types of disability can assist in delineating common elements of resilience in caregiving as well as highlighting elements that are specific to particular disability groups.
Therefore, the study objectives were to investigate: (i) the relationship between resilience and the presence of positive affect, negative affect and burden in caregiving; (ii) whether family members with higher resilience scores rated the helpfulness of caregiving management strategies differently from family members with lower resilience scores; and (iii) the similarities and differences in resilience among family caregivers supporting relatives with traumatic brain injury versus spinal cord injury.
Method
The study was approved by the relevant Human Research Ethics Committees for the three participating health services. A convenience sample of family members with a relative who had sustained a traumatic brain injury or spinal cord injury was recruited to the study between October 2006 and May 2009. Family members were identified using a combination of strategies, including review of medical records and staff caseloads. Letters were sent to potential participants, who were then contacted by phone. Those who agreed to participate in the project were provided with information and consent forms. Consent was obtained from both the family member and the relative with the injury. Family participants who provided informed consent were administered a number of self-report measures in person or over the phone. In addition, relatives completed a data protocol that contained demographic and psychosocial items. Injury and demographic items for the relative with the injury were extracted from the medical file. Functional Independence Measure 27 scores were either calculated by one of us (KJ) or, if routinely collected on the units, obtained from the medical file.
The injured relatives were patients of one specialist brain injury rehabilitation unit (located at Liverpool Hospital) and three specialist spinal injury services (located at the Royal Rehabilitation Centre Sydney and Royal North Shore Hospital) in Sydney Australia. Family members who (i) were aged 18 years or older; (ii) had a relative with a severe traumatic brain injury (duration of posttraumatic amnesia greater than 1 day 28 ) or spinal cord injury sustained at 18 years or older; and (iii) had sufficient English fluency to validly complete the study surveys were recruited from both inpatient and community settings. Family members were excluded if they had been diagnosed with a major psychiatric condition or illness.
Family members completed a set of reliable and valid self-report measures. The Resilience Scale 24 is a 25-item measure that evaluates five interrelated components of resilience, namely equanimity, perseverance, self-reliance, meaningfulness, and existential aloneness. Participants rate their response to items (e.g. ‘When I make plans I follow through with them’) on a seven-point likert scale, anchored at the two poles (‘disagree’ and ‘agree’). Scores range from 25 to 175, with higher scores representing higher resilience. The total score and two subscale scores (Personal Competence, Acceptance of Self/Life) were employed in the study. The Positive and Negative Affect Scale 29 is a widely used 20-item measure of emotional well-being. Participants rate a series of 20 adjectives (10 positive affect, 10 negative affect) on a five-point likert scale (‘very slightly or not at all’ to ‘extremely’), producing two scores that range from 10 to 50, with higher scores representing greater positive and greater negative affect respectively. The Caregiver Burden Scale 30 is a 22-item multidimensional scale that assesses the burden of caregiving for people with neurological impairment. Items are rated on a four-point scale (‘Not at all’ to ‘Often’; range 22–88) with higher scores representing greater burden.
The Carer’s Assessment of Managing Index 31 is a 38-item scale that measures carer ratings of the helpfulness of a list of management strategies in caring for their relative (e.g. ‘Establishing a regular routine and sticking to it’) and maintaining personal capacity to provide care (e.g. ‘Keeping a little free time for myself’). Items are rated on a four-point scale (I do not use this, not really helpful, quite helpful, very helpful, 0–3) with higher scores representing higher ratings of the helpfulness of the 38 strategies. The Index was developed among carers involved in chronic care situations (generally caregiving for two years or more).
The purpose of the Index is to provide information to clinicians to enable them to work with caregivers to better understand the management approaches utilised by caregivers in order to tailor interventions and service support to minimise caregiver stress and promote coping. 32 The manual for the Index did not provide a total score. For the purposes of this study, a total score was introduced, representing the cumulative ratings of helpfulness across all management strategies. Three of the 38 management strategies that were unlikely to be beneficial in the chronic care context (i.e. Trying to cheer myself up by eating, having a drink, smoking or the like; Ignoring the problem and hoping it will go away; Keeping my emotions and feelings tightly under control) were reverse scored, so that an increased score represented caregivers rating the strategy as less helpful. The total score ranged from 0 to 114.
Data were entered into Predictive Analytic Software (PASW) Statistics Version 18.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were generated for all variables. Given the ordinal nature of the scales, non-parametric statistical procedures were employed. Initial analyses were conducted to test for differences in demographic and psychosocial profiles between family participants (supporting relative with traumatic brain injury vs. supporting relative with spinal cord injury; High resilience scores group vs. Low resilience scores group) and the demographic and injury profile of the relatives with traumatic injury (traumatic brain injury vs. spinal cord injury). For aim 1, Spearman’s correlations were calculated to test the association among the variables of interest. To address aim 2, the sample was divided into two groups (high resilience scores vs. low resilience scores) employing a median split on Resilience Scale 24 scores. Between-groups analyses (Mann–Whitney U) were then conducted on the 38 items of the Carer’s Assessment of Managing Index. 31 Similarly, for aim 3, Mann–Whitney U tests were conducted on the 38 items of the Carer’s Assessment of Managing Index 31 (families supporting a relative with traumatic brain injury vs. families supporting a relative with spinal cord injury). When necessary, a Bonferroni correction was applied to the significance level to control for Type 1 error arising from multiple tests.
Results
Demographic, injury and psychosocial details of the family participants and their relatives with traumatic brain injury or spinal cord injury are summarised in Table 1. A total of 61 family members participated in the study. The great majority of participants had relatives who had sustained traumatic injuries, with the exception of six family participants who were supporting a relative with non-traumatic spinal cord injury. Statistical analyses found no differences between family members supporting a relative with traumatic brain injury (n = 30) and family members supporting a relative with spinal cord injury (n = 31) in relation to sex, age, and years of education (chi-square, Mann–Whitney U). However, there were significant kinship differences between the groups, with family members supporting relatives with spinal cord injury including significantly more spouses (χ 2 = 18.44, P < 0.001; Fisher’s exact test).
Demographic, injury and psychosocial characteristics of family members and relatives with traumatic brain injury or spinal cord injury.
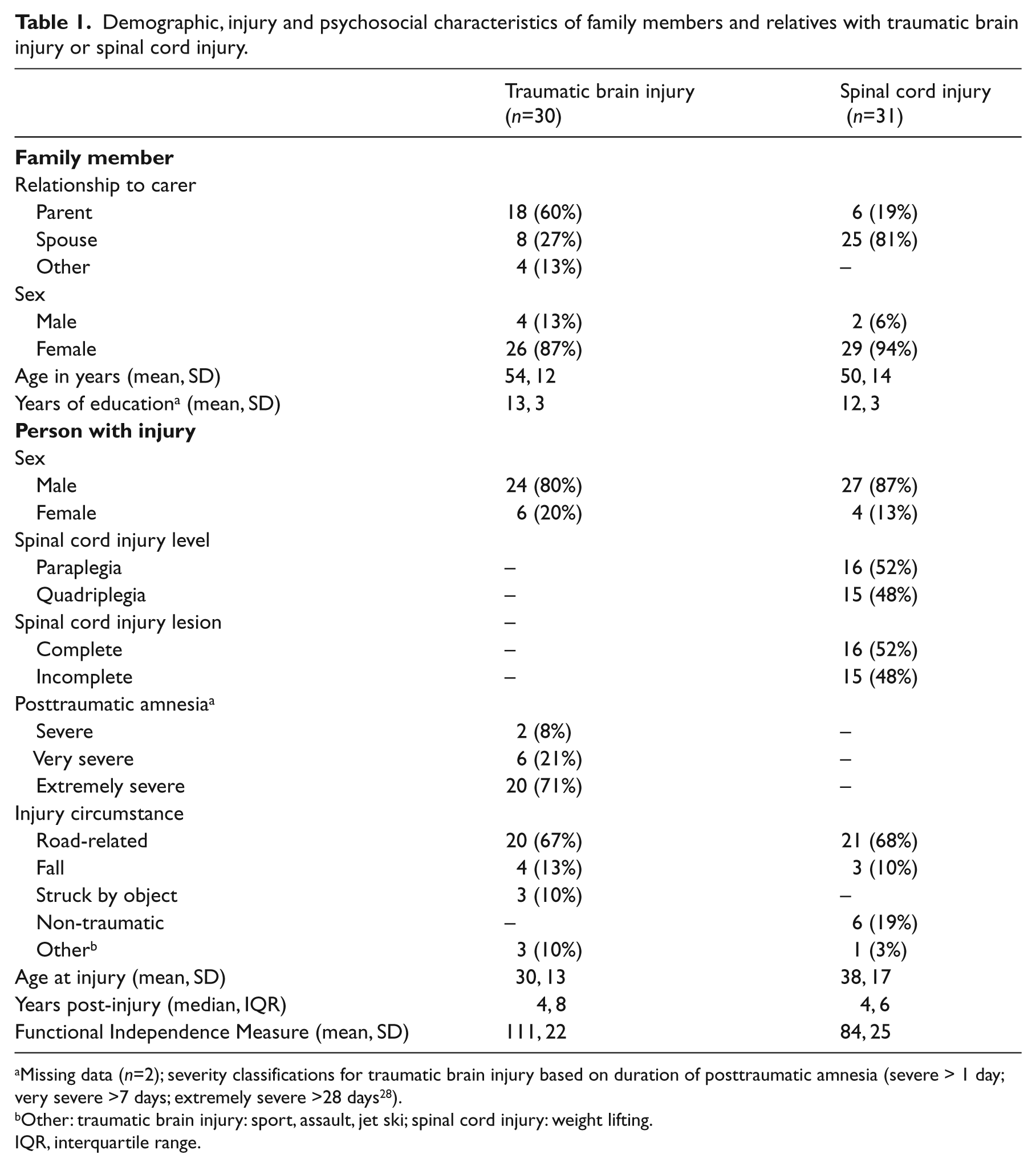
Missing data (n=2); severity classifications for traumatic brain injury based on duration of posttraumatic amnesia (severe > 1 day; very severe >7 days; extremely severe >28 days 28 ).
Other: traumatic brain injury: sport, assault, jet ski; spinal cord injury: weight lifting.
IQR, interquartile range.
Two-thirds of the relatives with traumatic brain injuries had extremely severe injuries. The relatives with spinal cord injury were evenly divided between paraplegia and quadriplegia, and also between the numbers of complete versus incomplete injuries. There were no differences between the relatives with traumatic brain injury versus spinal cord injury in relation to sex, years of education and time post-injury (chi-square, Mann–Whitney U). However, the relatives with spinal cord injury scored significantly lower Functional Independence Measure scores (z = −4.155, P< 0.05; Mann–Whitney U) and were significantly older (by approximately a decade) at the time of injury than the relatives with traumatic brain injury (z = −2.438, P < 0.015; Mann–Whitney U).
Overall, between-groups analyses for the study variables found no significant differences in the measures between family members of relatives with traumatic brain injury and family members of relatives with spinal cord injury (Mann–Whitney U, Bonferroni correction α = 0.05/12, P = 0.004). The one exception was that traumatic brain injury family members recorded significantly higher scores on the Emotional Involvement Subscale of the Caregiver Burden Scale (z = 2.98, P = 0.003; Mann–Whitney U). The factor of Emotional Involvement includes the three items: ‘Are you sometimes ashamed of your relative’s behaviour?’; ‘Do you ever feel offended and angry with your relative?’; and ‘Do you feel embarrassed by your relative’s behaviour?’ (see Table 2).
Family caregiver ratings on resilience, carer burden, positive and negative affect.
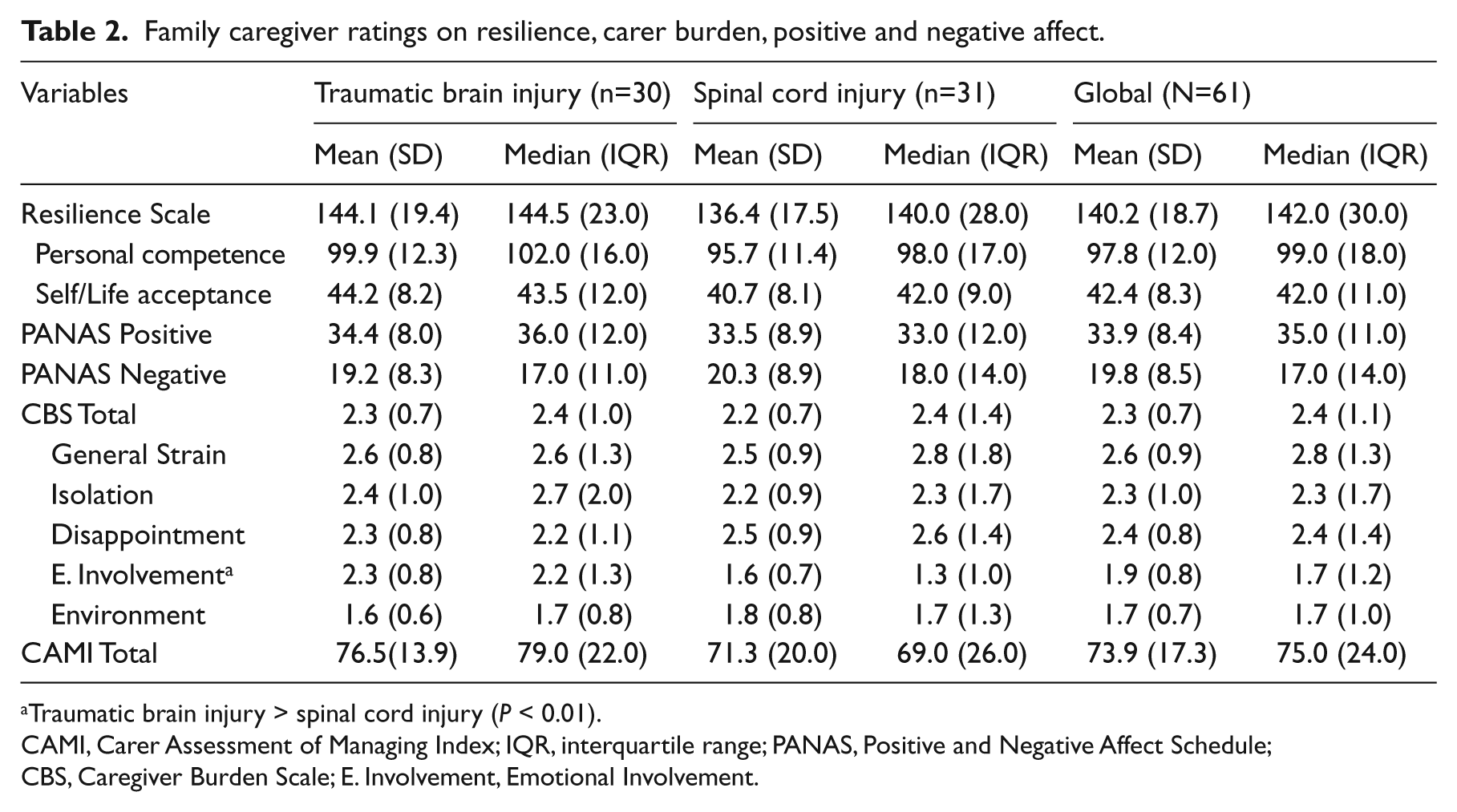
Traumatic brain injury > spinal cord injury (P < 0.01).
CAMI, Carer Assessment of Managing Index; IQR, interquartile range; PANAS, Positive and Negative Affect Schedule; CBS, Caregiver Burden Scale; E. Involvement, Emotional Involvement.
Results from the correlational analyses are displayed in Table 3. There was a strong significant positive association between resilience and the Positive and Negative Affective Schedule positive affect score. There was a moderate negative correlation between resilience and the Positive and Negative Affective Schedule negative affect score, so that, as resilience scores increased, there was an associated decrease in negative affect. There was a weak negative association between resilience and the carer burden score, so that, once again, increasing resilience scores were associated with a decrease in reports of carer burden. A similar pattern of weak negative correlations was found between increasing resilience and three subscales of the Caregiver Burden Scale (General Strain, Disappointment, Emotional Involvement). Importantly, there was no correlation between an objective measure of client disability (i.e. the Functional Independence Measure) and resilience scores, so that higher levels of resilience were not simply linked with lesser degrees of disability in the relative with traumatic brain injury or spinal cord injury.
Correlation matrix (N=61).
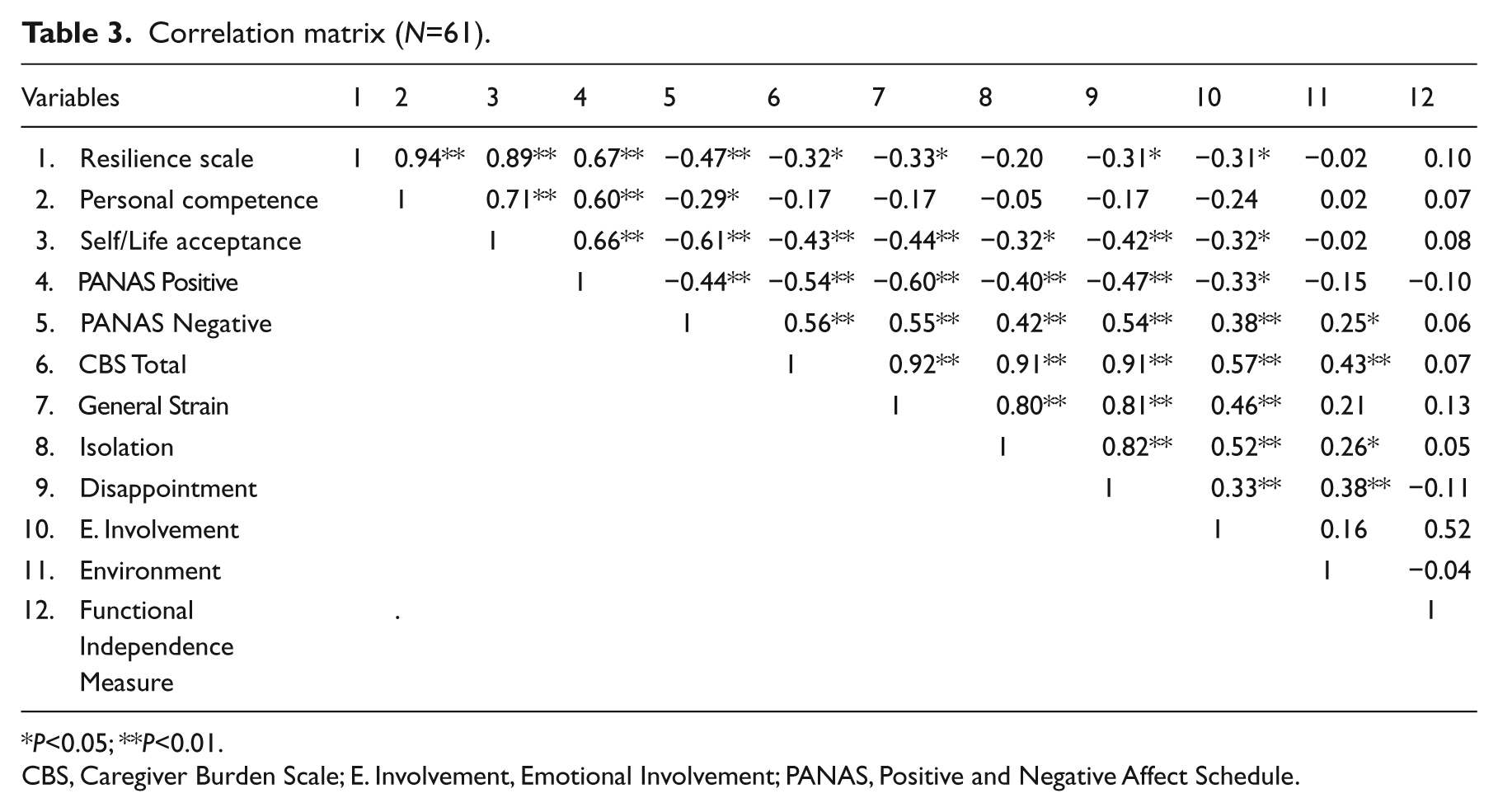
P<0.05; **P<0.01.
CBS, Caregiver Burden Scale; E. Involvement, Emotional Involvement; PANAS, Positive and Negative Affect Schedule.
Family members were then divided into two groups (high resilience scores, low resilience scores) using a median split of the Resilience Scale 24 scores. The difference in resilience scores between the two groups was statistically significant (Mann–Whitney U, P < 0.05). There were no significant differences in sex, age, or years of education between family participants in the high resilience scores versus the low resilience scores group (chi-square, Mann–Whitney U). Moreover, there was no difference in the numbers of families supporting a relative with traumatic brain injury versus spinal cord injury in the two groups (chi-square). Mann–Whitney U analyses found that the group of families reporting higher resilience scores displayed significantly greater levels of positive affect and a higher total score on the Carer Assessment of Managing Index than the low resilience scores group (Bonferroni correction, α = 0.05/10, P = 0.005) (see Table 4).
Family affect, burden and management strategies by resilience group.
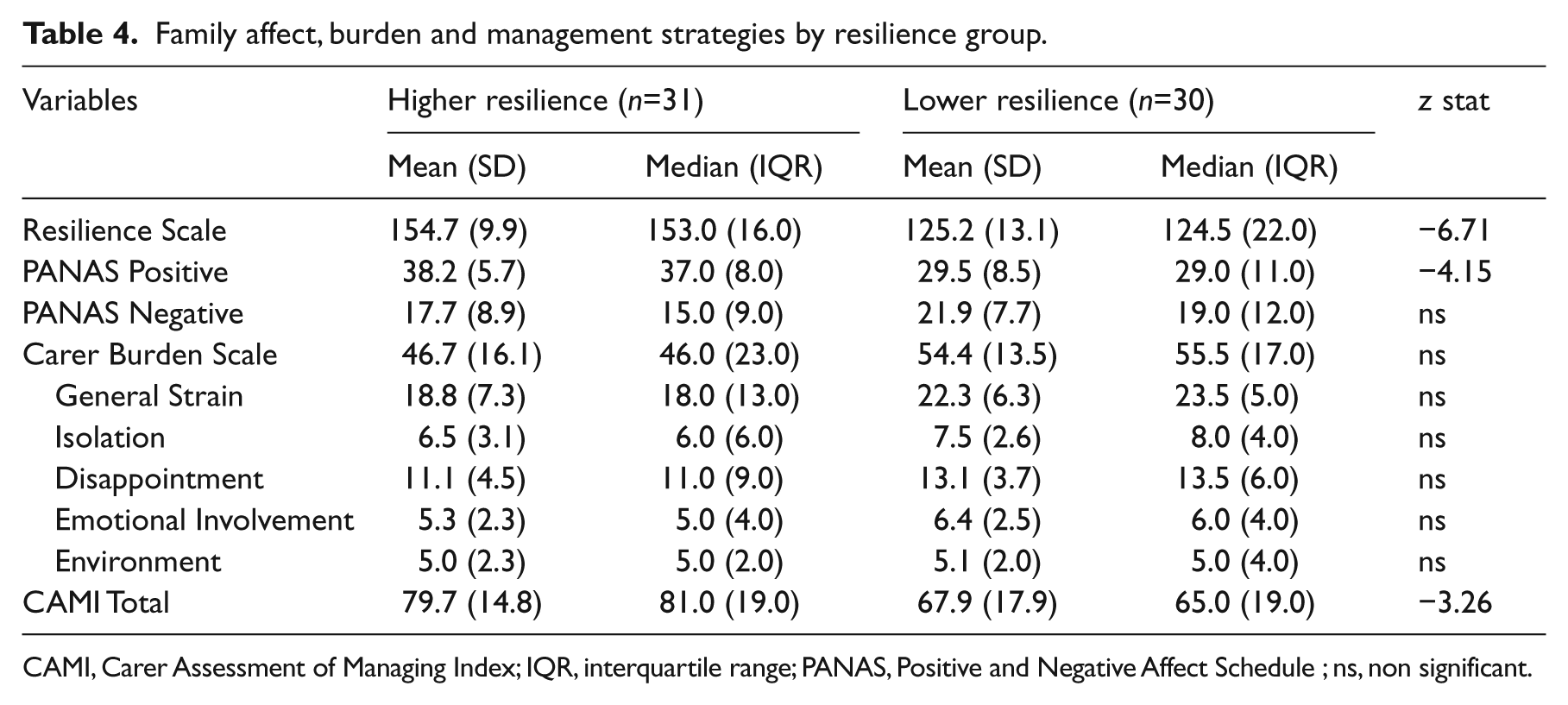
CAMI, Carer Assessment of Managing Index; IQR, interquartile range; PANAS, Positive and Negative Affect Schedule ; ns, non significant.
Between-groups analysis of the Carer Assessment of Managing Index items found that the group of families with high resilience scores rated the helpfulness of four management strategies significantly more highly than the low resilience scores group (Mann–Whitney U, Bonferroni correction α = 0.05/38, P = 0.001), with the median scores for three of the four items representing the highest level of ‘Very helpful’ (see Table 5). There was also a trend at P < 0.05 for family members in the high resilience scores group to rate the helpfulness of another nine strategies more highly than the low resilience scores group (Mann–Whitney U; see Table 5). Finally, there was one strategy that the high resilience scores group was less likely to rate as helpful (Item 28; Trying to cheer myself up by eating, having a drink, smoking or the like; Mann–Whitney U, P < 0.05).
Helpfulness of management strategies by resilience group.
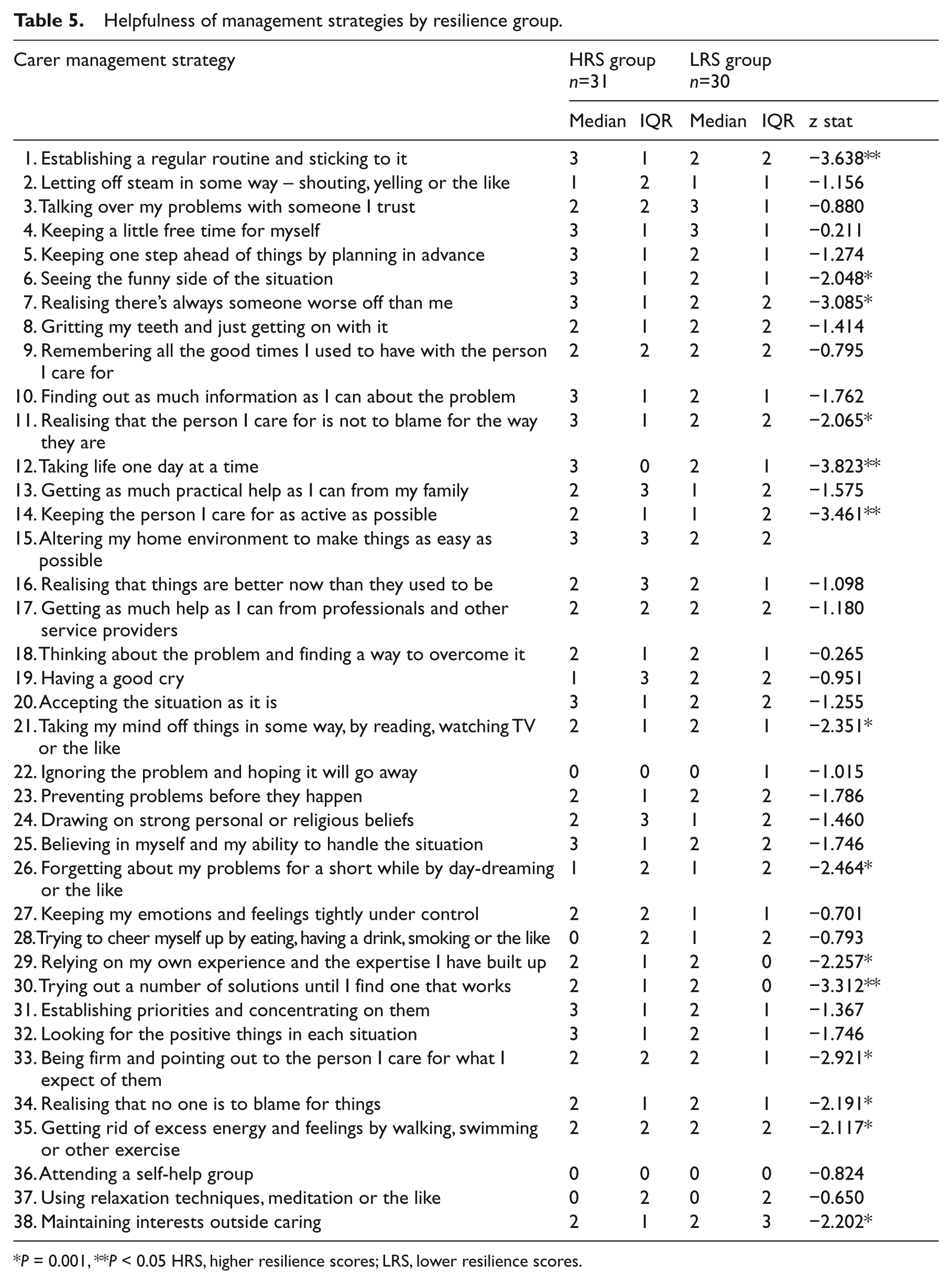
P = 0.001, **P < 0.05 HRS, higher resilience scores; LRS, lower resilience scores.
Between-groups analyses of the Carer’s Assessment of Managing Index items (with appropriate Bonferroni correction) found no significant differences in the helpfulness ratings of strategies (traumatic brain injury vs. spinal cord injury) among family participants. Two strategies approached the corrected significance level, with family members supporting a relative with traumatic brain injury rating the helpfulness of the strategy ‘Keeping the person I care for as active as possible’ significantly more highly (traumatic brain injury: Med 2 interquartile range (IQR) 1 vs. spinal cord injury: Med 1 IQR 1, z = −2.99, P = 0.003). Conversely, family members of relatives with spinal cord injury were significantly more likely to rate the helpfulness of the strategy ‘Altering my home environment to make things as easy as possible’ more highly (traumatic brain injury: Med 2 IQR 3 vs. spinal cord injury: Med 3 IQR 1; z = −2.89, P = 0.04). Another five strategies displayed a trend to significance (Items 2, 3, 7, 10 and 33; all traumatic brain injury>spinal cord injury; P < 0.05).
Discussion
The key findings of the study were that higher ratings of resilience among family caregivers were significantly correlated with increased levels of positive affect and decreased levels of both negative affect and carer burden. The rates of family resilience were independent of the severity of functional impairment displayed by the relative they were supporting. Furthermore, family members with higher resilience scores did display differences in their approach to caregiving, rating some carer management strategies as significantly more helpful in comparison to families with lower resilience scores. Finally, there were no differences in the levels of resilience, positive and negative affect, and levels of burden reported by families supporting relatives with traumatic brain injury versus spinal cord injury.
In considering the findings of the study, the following limitations need to be kept in mind. The modest sample size and convenience sampling strategy means that participants may not be representative of the population of families supporting relatives with traumatic brain injury or spinal cord injury, possibly either understating or overstating the prevalence of resilience and the strength of association with the affect and burden variables. In addition, the response set of the Carer Assessment of Managing Index evaluates the helpfulness of strategy use, and so the frequency with which caregivers may have employed these strategies is unknown.
Given these caveats, the study findings of the correlation between resilience and affect/ carer burden are consistent with formulations from resilience theory33,34 and research among other populations,19,23 that people with higher resilience are more likely to adapt positively when exposed to a traumatic event. In addressing a metatheory of resilience and resiliency, Richardson 21 broadened the construct of resilience to include the possibility of growth in response to trauma rather than a simple return to homeostasis (i.e. the idea of bouncing back). The Positive and Negative Affect Schedule 29 is a useful instrument for testing these propositions, with the Positive Affect scale acting as one measure of caregiver well-being.
The personal qualities or skill set associated with resilient adaptation and growth provides a potential explanation for these outcomes.16,21 Perlesz et al. 15 and others35,36 have pointed to the benefits in studying families who display resilience, because such families could serve as a model for those caregivers struggling with the adaptation process. Employing the Carer Assessment of Managing Index 31 provided the opportunity to address this question at the very specific level of caregiver management strategies. The significantly greater global rating of strategy helpfulness observed in the higher resilience group suggests that this group had a wider range of strategies to draw on to address the challenges of caregiving in comparison to the group with lower resilience scores. Second, caregivers with higher resilience scores also rated specific management strategies as more helpful than the lower resilience scores group, and these strategies may play an important role in the resilient adaptation that the higher scores group displayed.
Resilience scores did not correlate with severity of functional impairment, suggesting that resilience was not simply a reflection of the degree of functional impairment. This lack of correlation is consistent with broader research which has found that carer perception of the support demands, rather than the objective functional status of the injured person, is most closely associated with distress levels and experience of burden. 34 The personal and social resources associated with higher resilience may mean that the multiple demands arising from a relative’s injury are more likely to be perceived as manageable rather than overwhelming.
The study found more commonalities than differences among families supporting relatives with traumatic brain injury versus spinal cord injury. The non-significant differences in affective state are in line with previous studies that compared the emotional distress levels of family members across the two disability types.1–3 In addition, scores on some measures were almost identical to caregiver reports from other neurodisability groups. For example, the resilience score in the study sample differed by less than two points (on a 150 point scale) from that of caregivers supporting relatives with Alzheimer’s disease. 24 Similarly, the mean Caregiver Burden Scale scores for the total sample were similar to those reported by the spouses of stroke patients. 30
The few differences detected were consistent with challenges faced by families in response to unique features of the two disability groups. The Emotional Involvement subscale items (Caregiver Burden Scale) captured family reactions to the dyscontrol in social behaviour commonly displayed after traumatic brain injury.11,12 The two Carer Assessment of Managing Index strategies in which a strong trend to significant between-groups differences was observed also reflected the unique features of each disability group. The item endorsed more frequently by family members supporting a relative with spinal cord injury was the helpfulness of home adaptations. In contrast, families supporting relatives with traumatic brain injury rated more highly the helpfulness of providing structure to their relative, an important compensatory strategy in managing cognitive and behavioural impairments.
Future research is needed to replicate the findings from this study. In addition, the association between resilience and clinical criterion measures (e.g. levels of psychological caseness) needs investigation to further support the construct validity and clinical significance of resilience. Additional evidence in support of the study findings will reinforce calls for proactive intervention to build resilience among family caregivers in rehabilitation settings.16, 19 The similarities between the two groups of family members in resilience levels, affective state and experience of caregiver burden suggest that some elements of such an intervention could be universal, complemented by disability-specific education and family support programs.
Clinical messages
Family members with higher resilience scores reported more positive affect than families with lower resilience scores
Family members with higher resilience scores reported less negative affect and carer burden than families with lower resilience scores
Family resilience was independent of the functional status of the patient
Footnotes
Acknowledgements
Thank you to all the families who participated. Thank you to Rob Gordon, Kathryn Younan, Lauren Gillett and the social workers from the Royal Rehabilitation Centre Sydney for their assistance.
Author contributors
GS and KJ both participated in study design, data collection, data analysis, and writing the manuscript.
Conflict of interest
None declared.
Funding
This work was supported by the NSW Life Time Care and Support Authority (08/210).