
Abstract
Aim:
To identify factors reported with negative and positive outcomes for caregivers of the traumatic brain injury and spinal cord injury cohorts, to investigate what interventions have been studied to support carers and to report what effectiveness has been found.
Methods:
Scoping systematic review. Electronic databases and websites were searched from 1990 to December 2015. Studies were agreed for inclusion using pre-defined criteria. Relevant information from included studies was extracted and quality assessment was completed. Data were synthesised using qualitative methods.
Results:
A total of 62 studies reported caregiver outcomes for the traumatic brain injury cohort; 51 reported negative outcomes and 11 reported positive outcomes. For the spinal cord injury cohort, 18 studies reported caregiver outcomes; 15 reported negative outcomes and three reported positive outcomes. Burden of care was over-represented in the literature for both cohorts, with few studies looking at factors associated with positive outcomes. Good family functioning, coping skills and social support were reported to mediate caregiver burden and promote positive outcomes. A total of 21 studies further described interventions to support traumatic brain injury caregivers and four described interventions to support spinal cord injury caregivers, with emerging evidence for the effectiveness of problem-solving training. Further research is required to explore the effects of injury severity of the care recipient, as well as caregiver age, on the outcome of the interventions.
Conclusion:
Most studies reported negative outcomes, suggesting that barriers to caregiving have been established, but not facilitators. The interventions described to support carers are limited and require further testing to confirm their effectiveness.
Introduction
Informal or unpaid care refers to care that is provided by family and friends to support people of all ages who are restricted in their activities of daily living through disability. 1 Carers play an important role in the lives of the care recipient, often at the expense of their own health and wellbeing. It has been estimated that caregivers are significantly more likely to have a disability themselves, to loose gainful employment and to have household incomes in the lowest quintiles, when compared with their non-caring counterparts. 2
Despite the potentially negative impacts of caregiving, many people feel obliged to take on this role. One of the most common reasons cited for providing care is the sense of family responsibility. 2 This may develop slowly over time, as is reported in the case of chronic progressive diseases such as dementia. Alternatively, the caregiver role may be thrust upon a person as a result of a traumatic accident. Leading causes of traumatic accidents include falls, road transport accidents and assault. Traumatic brain injury and spinal cord injury are among the leading causes of injury sustained as a result of traumatic accidents in the Western world. 2 Although not studied together frequently, the two cohorts provide an interesting point of comparison, with regards to rehabilitation requirements and outcomes.
In terms of clinical rehabilitation, these two groups of patients represent two conditions of sudden onset, one affecting the brain and the other not, but both causing marked long term problems. People with a traumatic brain injury show initial improvement over the first year or two post-injury, but go on to provide considerable burden in terms of emotional and cognitive care required, often owing to difficulties with executive functioning. This is in contrast to people with a spinal cord injury, who pose a heavy burden in terms of hands-on physical care, but whose cognition remains largely intact. The rehabilitation trajectory for people who sustain a traumatic brain injury or a spinal cord injury does vary. However, both types of injuries frequently result in at least one or more restrictions in self-care, domestic and/or productive activities of daily living, thus requiring care to be sustained.
For informal care to be sustained, the outcome of the caregiving role needs to be positive. Systematic reviews about caregiving outcomes do exist for the stroke 3 and dementia 4 cohorts, but as neither of these conditions is associated with a traumatic accident, these reviews may not offer adequate information for the traumatic brain injury and the spinal cord injury cohorts. Therefore, the aims of this systematic review were as follows.
Aim
The primary question was to determine the following.
1. What factors have been reported with a negative or a positive outcome for caregivers of the traumatic brain injury and the spinal cord injury cohorts?
The secondary questions were to determine the following.
2. What interventions are described in the literature to support caregivers of the traumatic brain injury and the spinal cord injury cohorts?
3. Of the interventions described in the literature to support caregivers of the traumatic brain injury and the spinal cord injury cohorts, what effectiveness has been found?
In considering the results of this systematic review, data will be synthesised to draw some general conclusions across the two cohorts.
Methods
Search strategy
Four electronic databases (CINAHL, Cochrane Library, Medline and PsycINFO) were searched from 1990 to December 2015, with an English language restriction. Websites of organisations known to support carers of the traumatic brain injury and the spinal cord injury cohorts were also searched. Relevant combinations of the search terms and spelling derivatives were used, as shown in the Appendix, available online. The search strategy was first trialled and used in PsycINFO, and then adapted for use in each subsequent electronic database and website.
Results were downloaded into a bibliographic management software program (EndNote X7), and duplicate studies were deleted. Given the high number of studies identified, only one author screened each of the studies by title and abstract to determine eligibility to be included in the review, using predetermined criteria. Once the final pool of included studies had been identified, a second author confirmed the eligibility of each of the studies. If sufficient information was not described to make a decision based on title and abstract alone, the full text of the article was obtained. Finally, a review of the reference list from each of the included studies was completed in order to identify any articles that may have been missed by the literature search.
Inclusion/exclusion criteria
The following inclusion criteria were applied.
Population
Studies in which caregivers provided care to an adult (⩾18 years) with a traumatic brain injury or spinal cord injury were included.
Intervention
For the primary question, intervention criteria were not relevant. For the secondary questions, studies in which intervention was provided through carer services, carer support programmes, group support, online support, 1:1 support and peer support were included.
Outcome
The outcomes of ability to care, caregiver burden, caregiver emotional distress, caregiver preparedness, caregiver strain, cost, family functioning and resilience were included.
Research design
All research designs, including systematic reviews, primary studies and discussion/case study examples that had been peer-reviewed were included.
Quality assessment
For the primary question, quality assessment was deemed not to be relevant. For the secondary questions, quality assessment was completed using The Downs and Black Instrument. 5 Scores on The Downs and Black Instrument range from 0–31, with a score of zero used to indicate a low quality study and a score of 31 indicating a high quality study. 5 Level of evidence was determined using The Australian National Health and Medical Research Council Guidelines. 6
Data extraction
Data extraction was completed by one reviewer and cross-checked by a second reviewer. Separate tables were created for the traumatic brain injury and the spinal cord injury cohorts. For the primary aim, data were extracted and summarised pertaining to author (and year) of study, and factors reported with if the caregiver outcome is negative or positive. For the secondary aims, data were extracted and summarised pertaining to author (and year) of the study, country in which the study was conducted, details of the intervention and details of the intervention’s effectiveness.
Data analysis
Data were synthesised qualitatively, by using a narrative analysis. This method of analysis involved coding information from within individual studies and grouping them into like categories, where sufficient similarity existed between caregiver outcomes and caregiver interventions to allow this. Data were analysed separately for the traumatic brain injury and the spinal cord injury cohorts, and then compared to identify similarities and differences.
Results
A flowchart of the number of studies identified and screened is presented in Figure 1. Agreement was reached between two of the reviewers for all of the 105 included studies, as well as the scores awarded for quality assessment and level of evidence. From the process of website screening, no further information was obtained.
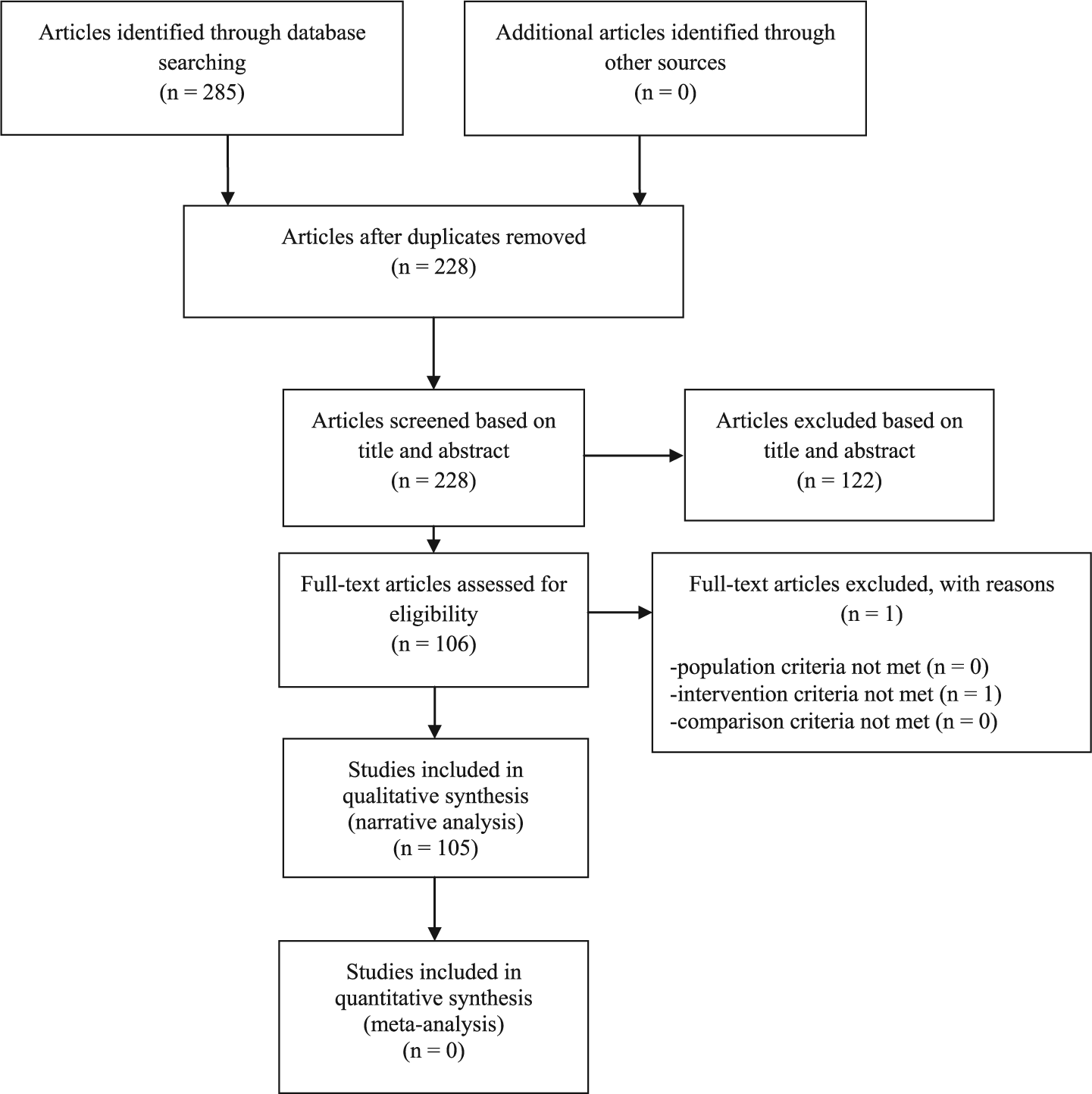
Number of studies identified and screened for inclusion or exclusion.
Primary aim
What factors have been reported with a negative or a positive outcome for caregivers of the traumatic brain injury and the spinal cord injury cohorts?
Factors reported with a negative or a positive outcome for caregivers of the traumatic brain injury and the spinal cord injury cohorts are summarised in Table 1. A total of 62 studies reported caregiver outcomes for the traumatic brain injury cohort; 51 reported negative outcomes, and 11 reported positive outcomes. A total of 18 studies reported caregiver outcomes for the spinal cord injury cohort; 15 reported negative outcomes, and three reported positive outcomes.
Factors reported with negative and positive outcomes for caregivers of the traumatic brain injury and the spinal cord injury cohorts.
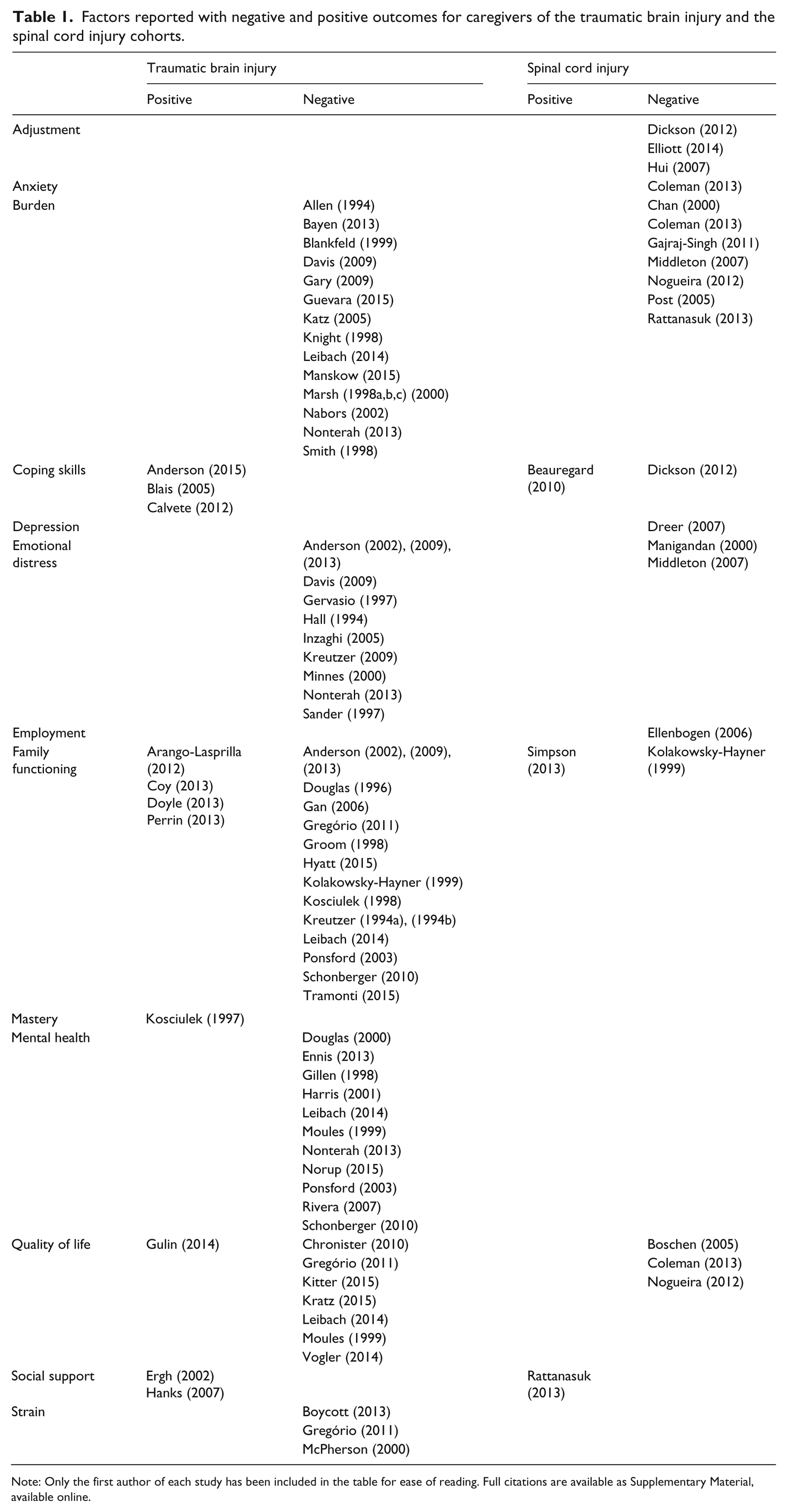
Note: Only the first author of each study has been included in the table for ease of reading. Full citations are available as Supplementary Material, available online.
Negative outcomes
In order of frequency (with number of studies in brackets), the top three factors reported with a negative caregiving outcome for the traumatic brain injury cohort were: high levels of caregiver burden (17); poor family functioning (16); and poor mental health and high levels of caregiver emotional distress (11). For the spinal cord injury cohort, the top three factors reported were: high levels of caregiver burden (7); poor caregiver adjustment (3); and poor caregiver quality of life (3). For both cohorts, burden of care (the factor most commonly reported with a negative caregiving outcome) was grossly referred to as the perceived impact that caregiving roles and responsibilities had on a carer’s life. High burden of care was associated with a poor level of functioning of the care recipient.
Positive outcomes
The top three factors reported with a positive caregiving outcome for the traumatic brain injury cohort were: good family functioning (4); good coping skills (3); and good social support (2). For the spinal cord injury cohort, the top three factors reported were: good family functioning (1); good coping skills (1); and good social support (1). Family functioning and coping skills were reported to improve outcomes by reducing caregiver burden. Social support was reported to give both cohorts of caregivers a broader focus, beyond caring for someone with an injury. Social support was also reported to improve problem-solving skills, when interacting with caregiving peers.
Secondary aims
What interventions are described in the literature to support caregivers of the traumatic brain injury and the spinal cord injury cohorts?
A total of 21 interventions were described in the literature to support caregivers of the traumatic brain injury cohort (see Table 2) and four for the spinal cord injury cohort (see Table 3).
Interventions described to support carers of the traumatic brain injury cohort and their effectiveness.
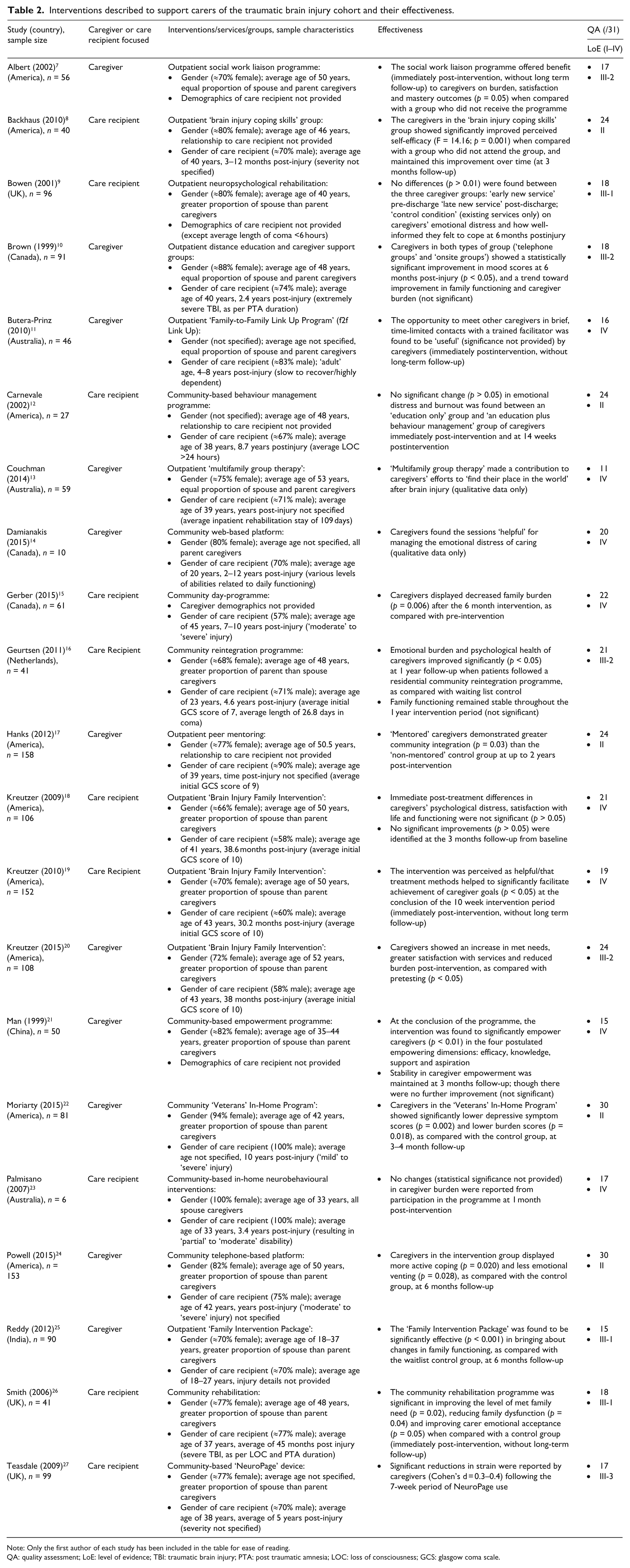
Note: Only the first author of each study has been included in the table for ease of reading.
QA: quality assessment; LoE: level of evidence; TBI: traumatic brain injury; PTA: post traumatic amnesia; LOC: loss of consciousness; GCS: glasgow coma scale.
Interventions described to support carers of the spinal cord injury cohort and their effectiveness.

Note: Only the first author of each study has been included in the table for ease of reading.
QA: quality assessment; LoE: level of evidence; ADLs: activities of daily living; QoL: quality of life.
Traumatic brain injury
Of the 21 interventions, 11 targeted the caregiver directly for intervention. Interventions described in the caregiver-focused studies shared common principals such as education, empowerment, peer mentoring and peer support. Some of these interventions had specific names (e.g. the ‘Family-to-Family Link Up Program’ (f2f Link Up) provided by Butera-Prinz 11 and colleagues), whereas others were reported on in more general terms (e.g. the ‘outpatient social work liaison programme’ provided by Albert 7 and colleagues). All caregiver-focused interventions were delivered in an outpatient/community setting. There was significant variability reported in the frequency, duration and total number of intervention sessions, as well as the demographics of the caregivers who participated in these interventions.
The remaining 10 studies targeted the care recipient for intervention. These studies reported the underlying principal that if intervention improved the level of independence and functioning of the care recipient, then involvement from the caregiver would be lessened and the caregiving outcome thereby improved. All interventions reported in these studies included an element designed to improve the executive functioning of the care recipient. Strategies included behaviour management, community re-integration, coping skills training, neuropsychological rehabilitation and use of adaptive devices.
Spinal cord injury
Each of the four interventions targeted the caregiver. Three of the four studies involved problem-solving training, while the other study used peer support intervention. Problem-solving training was used to help caregivers to negotiate the practical demands of providing care to a person with a spinal cord injury. Caregivers were taught how to generate solutions to commonly encountered problems (e.g. transferring a person from a wheelchair into a vehicle), and were taught how to search through each of the possible solutions (e.g. hoist, slide-board, manual assist) in order to choose the right one to meet their needs.
Of the interventions described in the literature to support caregivers of the traumatic brain injury and the spinal cord injury cohorts, what effectiveness has been found?
Results could not be appropriately pooled owing to dissimilarity across the studies. Level of evidence and quality of each of the studies is summarised in Table 2 (traumatic brain injury) and Table 3 (spinal cord injury).
Traumatic brain injury
In each of the 11 studies reported to target the caregiver for intervention, caregivers demonstrated an improvement on one or more outcome measures immediately after the intervention period. Just over half of these studies also provided follow-up, where gains made by the caregivers were reported to be maintained between 3–24 months after the intervention period. Looking at the quality of the studies, Hanks (2012), 17 one of the highest quality studies (24/31), provided Level II evidence. In this study it was found that ‘mentored’ caregivers demonstrated greater community integration than the ‘non-mentored’ control group at 24 months post-intervention. One of the lowest quality study (11/31) provided Level IV evidence. 13 Couchman (2014) 13 concluded that ‘Multifamily Group Therapy’ helped caregivers to ‘find their place in the world’ after brain injury (qualitative data only).
Less effective results were reported in the studies that targeted the care recipient for intervention. Of the 10 studies, six reported an improvement on one or more outcome measures immediately after the intervention period. Only two studies provided long-term follow-up. Backhaus (2010), 8 a high quality study (24/31), provided Level II evidence. It was found that caregivers in the ‘Brain Injury Coping Skills’ group showed significantly improved perceived self-efficacy when compared with the carers who did not attend the group, and maintained this improvement at 3 months follow-up. Contradictory results were reported in another study at follow-up. 16 Geurtsen (2011) 16 showed that the initial gains made by the caregivers were not significantly maintained at 12 months post-intervention.
Spinal cord injury
All three studies using problem-solving training were found to be effective in promoting improvement on one or more outcome measures immediately after the intervention period. With regards to the quality of these studies, Schulz and colleagues (2009) 30 received the highest quality assessment score of 26/31, and provided Level II evidence. Schulz (2009) 30 found that caregivers in the ‘dual-target treatment group’ reported improved quality of life, significantly fewer health symptoms and were less depressed when compared with two other ‘treatment groups’ at 12 months post-intervention. The study completed by Elliott and colleagues (2008) 28 was the second highest quality for the spinal cord injury cohort (23/31), and provided Level II evidence. A significant decrease in depression was found among caregivers receiving ‘problem-solving training’, when compared with a ‘control group’ at 6 months post-intervention. Caregivers who received ‘problem-solving training’ also reported significant gains in social functioning over time. Although providing a lower level of evidence than Schulz (2009) 30 and Elliott (2008) 28 , Rivera and colleagues (2003) 29 found Level IV support for problem-solving interventions. Problem-solving interventions were found to effectively alleviate caregiver emotional distress and helped the caregiver to learn useful coping skills. Two of the three studies also provided follow-up, where the gains made by caregivers were maintained 6–12 months after the intervention period.
Discussion
The results of this systematic review show that there is strong, reproducible evidence concluding what factors are associated with a negative outcome for caregivers. Burden of care, in particular, is over-represented in the traumatic brain injury and spinal cord injury literature. Social support meanwhile has been reported essential to mediate this caregiver burden and to enhance the outcomes of caregiving, in part through the improvement of caregivers’ problem-solving skills. It was surprising therefore that problem-solving training only appeared once in the literature, 24 describing interventions to support carers of the traumatic brain injury cohort. Good evidence, however, was found for this intervention with the spinal cord injury cohort of caregivers. Finally, results from this systematic review suggest that in clinical practice carers themselves, not the care recipient, should be targeted for intervention. Further research is required to explore the effects of injury severity of the care recipient, as well as caregiver age, on the outcome of the interventions described.
The responsibility to provide care after a traumatic accident is usually assumed by informal caregivers. For informal care to continue into the future, the outcome of the caregiver role must be positive. However, this review suggests that while literature on the negative outcomes of caregiving is close to reaching data saturation, positive caregiving outcomes remain scarcely studied. This idea of needing to invest more into positive outcomes for caregivers after traumatic accidents is not a new idea, and is consistent with other systematic reviews in the caregiving arena more broadly.3,4 In the stroke 3 and dementia 4 cohorts for example, the suggestion has already been made for rehabilitation researchers to turn their attention towards interventions that create a positive outcome for caregivers. Problem-solving interventions were the most promising avenue identified from the results of this systematic review.
Given the success in the spinal cord injury cohort, problem-solving training may be an avenue also worth considering with the traumatic brain injury cohort of carers, as well as in the caregiving arena more broadly. It would be reasonable to assume that caregivers of the traumatic brain injury cohort may benefit from problem-solving training, given that this approach to intervention would tie in with the rehabilitation trajectory following traumatic brain injury. Typically after traumatic brain injury, considerable burden exists for the caregiver in terms of emotional and cognitive care. This is often owing to deficits in the care recipient’s executive functioning, which manifest in behaviours of concern. Powell and colleagues (2015) 24 have described a problem-solving training protocol, which was found to promote more active coping and less emotional venting for caregivers of the traumatic brain injury cohort. With further testing, this protocol may be used with caregivers to identify appropriate strategies in which to manage these behaviours.
There are limitations associated with this systematic review, including the English language restriction and the start-date for the search that was imposed. It is possible that studies published in languages other than English and that studies that were published prior to the cut-off date of 1990 have not been represented in this systematic review. Also, in this review, a conscious decision was made to group together the entire spectrum of injury severity. Caregivers of those with mild, moderate and severe injuries were analysed as a whole. This approach was adopted to reflect real-world practice, where interventions are not currently provided to distinguish injury severity. Although not investigated in this systematic review, it may be that caregiver outcomes are different for different injury severity types, which may limit the results of the review.
Alongside investigating whether injury severity of the care recipient impacts on caregiver outcome, a number of areas exist for further research. Exploring caregiver outcomes for different age groups of caregivers is one of these areas, as it may be that the effectiveness of interventions on carer and recipient outcomes are dependent on the age of the caregiver. Also, the field of technological advances is an area that needs to be further explored. Websites and online resources are frequently accessed by caregivers and are increasingly becoming an important service-delivery tool. 2 Yet from the websites reviewed within, evidence to suggest the sources of the online resources was not described. Maintaining websites with up-to-date resources, including links to the original study, is important so that the quality and the strength of the resource can be critiqued.
Clinical messages
Burden of care is over-represented in the literature for the traumatic brain injury and spinal cord injury cohort of caregivers, with few studies looking at factors associated with positive outcomes.
Of the interventions described in the literature to support caregivers, problem-solving training offers a promising direction for intervention.
Footnotes
Contributors
All authors were involved in drafting the manuscript, and all four authors revised the article critically for intellectual content. The authors have given approval for the final version of this article to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ISCRR is a joint initiative of WorkSafe Victoria, the Transport Accident Commission and Monash University. The opinions, findings and conclusions expressed in this publication are those of the authors and not necessarily those of ISCRR or its partners.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.