
Abstract
Objective
This study investigates the influence of aerobic exercise training on inhibitory control of executive functions in children with hemiplegic cerebral palsy.
Design
Single-blind randomized controlled trial.
Setting
Outpatient Physical Therapy Clinic.
Participants
Children aged 7–11 with left-sided hemiplegic cerebral palsy with emotional and behavioral dysregulation evidenced by scores >28 on Paediatric Symptom Checklist and GMFCS I or II (n = 60).
Intervention
Participants were randomly allocated into two equal groups. The control group received standard-of-care physical therapy for 1 h, and the aerobic exercise group received standard-of-care physical therapy for 30 min and moderate-intensity continuous exercise on a bicycle ergometer for 30 min. All groups received treatment three times a week for 12 weeks.
Main Measures
The Eriksen Flanker test and Stroop Color–Word test were used to assess inhibitory control of executive function at the baseline and after 12 weeks.
Results
Differences between pre- and post-treatment values in the exercise group showed significant improvement in Flanker response accuracy and Stroop response accuracy (p = 0.001) and significant decreases in Flanker congruent reaction time and Stroop congruent reaction time (p < 0.05). However, there were no significant differences between both groups in Flanker incongruent reaction time and Stroop incongruent reaction time (p > 0.05).
Conclusions
Aerobic exercise has a promising effect on inhibitory control of executive function in children with left-sided hemiplegic cerebral palsy.
Introduction
Cerebral palsy is a permanent disorder of developing movement and posture leading to reduced activity and is considered the leading cause of physical disability induced by a non-progressive neurological condition that occurs in the infant brain. 1 In addition, motor impairment has frequently been associated with secondary disturbances affecting different aspects such as communication, sensation, perception, behavior, and cognition. 2 Hemiplegic cerebral palsy is a subtype in which one side of the body is affected. It affects about 1 in every 1300 live births 3 and is characterized by a clinical pattern of hemiplegic motor impairment. 4 The severity of hemiplegic cerebral palsy depends on the site and severity of the brain lesion. 5
Executive functions are cognitive processes critical for behavioral cognitive control. 6 In addition, these functions are necessary for goal-directed behavior. Although the structured nature of the neuropsychological assessment process may hide deficits that are obvious in daily life, several standardized psychological tests evaluate executive function deficiencies. Behavioral and emotional dysregulation are a part of the hemiplegic cerebral palsy phenotype, and these deficits can be identified using tools such as the pediatric symptom checklist. 7
Aerobic exercise training is a continuous and rhythmic process that improves oxygen consumption by the activity of large muscles, 8 increases cerebral blood flow, 9 and improves cardiorespiratory fitness. Aerobic exercise may also benefit cognition, with evidence to suggest that aerobic training increases cerebral perfusion; 10 metabolism 11 ; reduction in amyloid β load 12 ; upregulation of neurotrophins, including brain-derived neurotrophic factor11,13,14; and hippocampal neurogenesis. 15 Aerobic exercise is also an efficient strategy to enhance executive control during 16 and after exercise. 17 Executive function is considered a strong predictor of early school success, 18 and inhibition control positively impacts children's everyday functioning. Children with cerebral palsy have been shown to have worse inhibitory control than typically developing peers. 19 In healthy children, aerobic exercise significantly improves different executive functions. 18
Moreover, aerobic exercise in children with cerebral palsy improves aerobic capacity, gross motor function, and self-perception in adolescents with spastic cerebral palsy.20,21 As such, we aimed to identify a potential link between aerobic exercise training and inhibitory control in executive function. This study aimed to investigate whether aerobic exercise training can benefit executive function in children with hemiplegic cerebral palsy with emotional and behavioral dysregulation evidenced by scores >28 on Paediatric Symptom Checklist and Gross Motor Function Classification System (GMFCS) I or II. We hypothesized that aerobic exercise would demonstrate a favorable effect on inhibitory control of executive function in this patient population.
Methods
This study is a single-blinded, randomized controlled study conducted in the outpatient physical therapy clinics at Cairo University. Each child's parents signed informed consent forms before participation. The study was approved by the Institutional Ethical Committee at Cairo University (REC/012/002278) and registered on www.clinicaltrials.gov (NCT04154566).
Participants
Participants were 70 children with hemiplegic cerebral palsy aged 7–11 selected according to a degree of behavioral and emotional dysregulation (pediatric symptom checklist > 28) and degree of motor impairment (GMFCS I or II). Inclusion criteria were (a) aged between 7 and 11 years (the age of significant development of executive function and notably inhibitory control), 22 (b) diagnosed with left-side hemiplegic cerebral palsy (damage to the right hemisphere increases susceptibility to deficits in evaluated cognitive activities), 23 (c) able to walk independently, (d) functional level I or II according to the GMFCS, 24 and (e) scored ≥ 28 or more on the pediatric symptom checklist (indicating emotional and behavioral impairment more likely to benefit from the possible cognitive effects of aerobic training).25,26 Exclusion criteria were (a) children with visual or auditory problems; (b) children with a history of drug intake that may affect cognitive functions such as aniracetam, L-theanine, or piracetam; or (c) medically unstable children, especially those with cardiovascular disorders or other diagnoses that would prevent participation in aerobic training or testing procedures.
Procedures and randomization
Seventy children with hemiplegic cerebral palsy were recruited and evaluated for eligibility. Seven children did not meet the inclusion criteria, and three declined to participate. A total of 60 children were enrolled in our study. Participants were randomly allocated into two groups of equal numbers (1:1) using random allocation software 27 (Figure 1). The random allocation was performed by an independent physiotherapist, and the therapists assessing the patient outcomes were blinded to the group allocation of the participants.
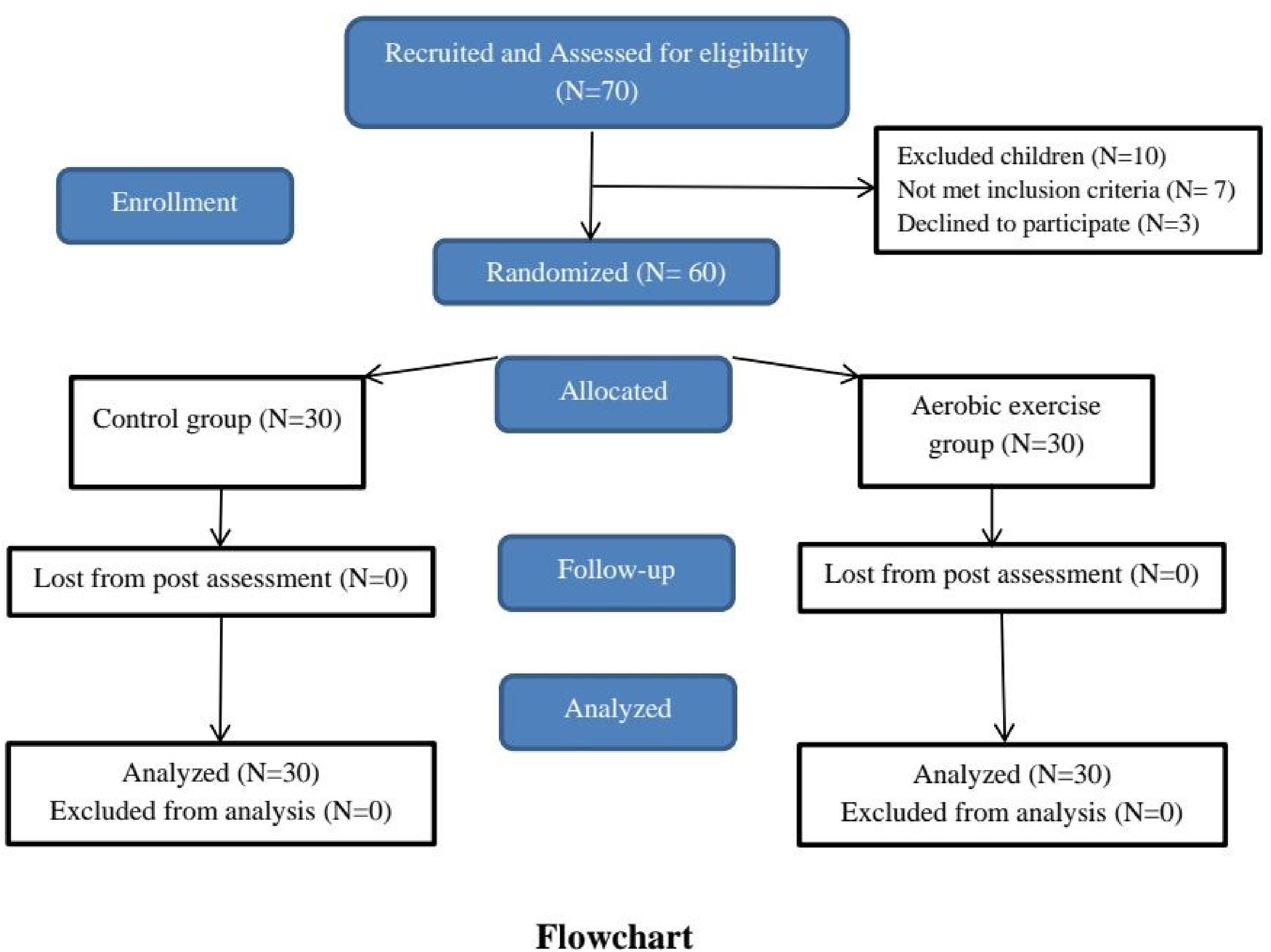
Flow chart of study design.
The control group received a 60-min standard-of-care physical therapy treatment which included strengthening exercises for both upper and lower extremity muscles, stretching exercises for elbow flexors, forearm pronators, wrist flexors, knee flexors, and ankle dorsiflexors.1,2 Participants also received balance exercises, coordination exercises, and gait training exercises. Treatment was provided three times per week for 12 consecutive weeks. The treatments and assessments were provided by physical therapists at the outpatient physical therapy clinics at Cairo University
The aerobic exercise group received a 30-min standard-of-care physical therapy treatment, similar to the control group. In addition, they also received a 30-min aerobic exercise training session on a bicycle ergometer (Monark Cardio Care 927E, Vansbro, Sweden).
Before starting the training procedure, each parent was instructed to dress their children in comfortable exercise clothing and to sit vertically on the bicycle ergometer seat with an erect back. An extra strap was placed on the child's feet to provide complete fixation on the ergometer pedal.28–30
In the first week, children bicycled at 40–50% age-predicted max heart rate. Participants were instructed to gradually increase exercise intensity by the second week to achieve 70% max heart rate as tolerated. This intensity level was then maintained throughout the exercise program. 28 The first 5 min of each exercise bout was dedicated to warming up on the ergometer at a comfortable pace, followed by 20 min at the desired intensity level mentioned above. The last 5-min were dedicated to cooling down, with participants slowly decreasing their exercise intensity levels until resting heart rate is achieved.29,30 Both groups received a total of 60 min of direct care.
Cognitive performance tests
Eriksen Flanker and Stroop Color–Word tests were used to assessing inhibitory control of executive function pre-intervention at baseline and post-intervention after week 12. In addition, both cognitive performance tests were conducted by researchers not involved in the training intervention.
Eriksen Flanker test is a widely used test to examine inhibitory control of executive function.31,32 The Flanker task consisted of 20 total trials. In this version of the test, participants were presented with an array of arrows that were arranged horizontally and shown in the same direction (e.g. >>>>>) or arrows that had different orientations relative to the middle arrow (e.g. >><>>). Flanker congruent reaction time and Flanker incongruent reaction time were determined based on the reaction time to respond to arrows in congruent or incongruent arrangement, respectively. Children were asked to identify the middle arrow's direction by pressing the right or left arrow button on the keyboard quickly and accurately and ignoring the flanking arrows. Stroop Color–Word test is a neuropsychological test that uses word color to measure selective attention, cognitive flexibility, and the ability to inhibit cognitive interference.19,33,34 Participants were presented with words (red, orange, yellow, green, blue, or purple) but were asked to identify the ink color. The congruent condition refers to when the ink color agrees with the name of the word (e.g. the word “blue” presented in blue ink). On the other hand, the incongruent condition refers to when the ink color does not agree with the name of the word (e.g. the word “blue” presented in green ink). All children were asked to identify the ink color by the corresponding first letter of the specified color ([r]ed; [o]range; [y]ellow; [g]reen; [b]lue; or [p]urple) as quickly and accurately as possible.
Sample size
A preliminary power analysis was used to avoid type II error [F test, MANOVA: special effects and interaction, power (1-α error) β = 0.80, α = 0.05, Pillai V = 0.17, and effect size f2 (V) = 0.204]. A total sample size of 48 was determined for this study (a minimum of 24 participants in each group) using G* power 3.1 software. The Pillai V and the effect size were calculated using data from a pilot study on ten participants. The trial was stopped once enrollment was complete.
Statistical analysis
Data are presented as mean ± SD unless noted otherwise. Independent t-tests were run to compare age between groups. A Mann–Whitney U test was run to determine differences in school grade. The chi-square test was used to compare differences in sex between groups. A mixed model MANOVA was used to compare within and between group effects of the Eriksen Flanker and Stroop Color–Word tests. The Bonferroni correction was used for post hoc multiple comparisons when indicated. All tests with a p < 0.05 were considered statistically significant. SPSS statistical software, version 26 (SPSS Inc., Chicago, IL), was used for all statistical analyses.
Results
A total of 60 children participated in this study. There were no statistically significant differences in baseline characteristics between groups (Table 1). There were no adverse effects reported from either group.
Participants’ characteristics.
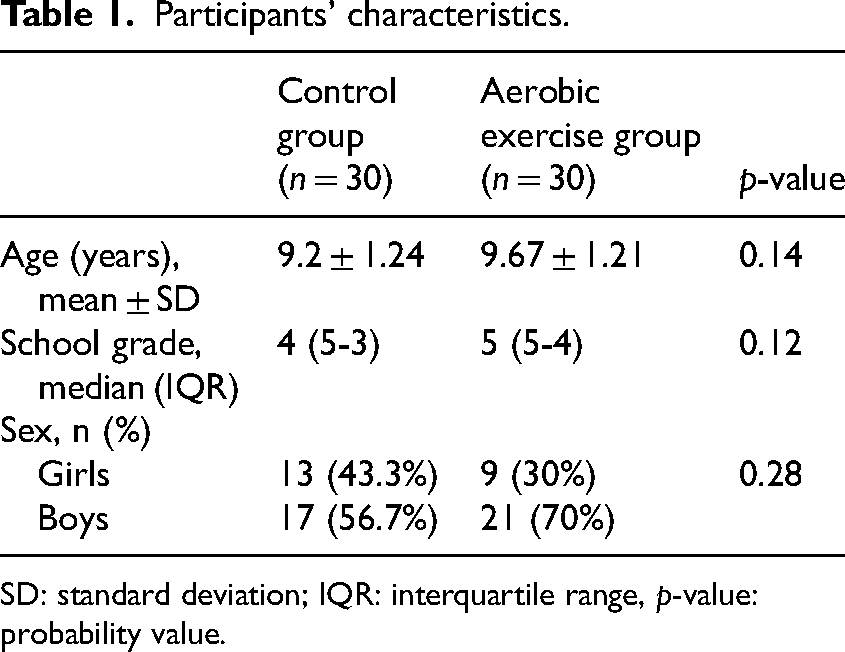
SD: standard deviation; IQR: interquartile range, p-value: probability value.
Effect of treatment on eriksen flanker and stroop color–word tests
There was a statistically significant interaction of treatment and time across groups [F (6,53) = 7.26, p = 0.001, η2 = 0.45].
Between-group comparisons
There were no significant differences in pre-treatment values between groups across all conditions (Tables 2 and 3). Furthermore, no significant differences were found post-treatment between the aerobic exercise group and the control group for the Flanker incongruent reaction time (1413 ± 308 ms vs. 1625 ± 483 ms, p = 0.08) and Stroop incongruent reaction time (2679 ± 453 ms vs. 2850 ± 424 ms, p = 0.13) (Tables 2 and 3). However, the aerobic exercise group showed significant improvements compared to the control group post-treatment in Flanker response accuracy (90 ± 12% vs. 82 ± 13%, p = 0.02) and Stroop response accuracy (84 ± 13% vs. 76 ± 14%, p = 0.02). In addition, the aerobic exercise group also showed significant decreases compared to the control group in the Flanker congruent reaction time (1148 ± 308 ms vs. 1473 ± 375 ms, p = 0.001) and Stroop congruent reaction time (1934 ± 599 ms vs. 2702 ± 581 ms, p = 0.001) (Tables 2 and 3). Altogether, these results indicate some improvement in inhibitory control of executive function due to aerobic exercise training.
Mean values of Eriksen Flanker test pre- and post-treatment of control and aerobic exercise groups.
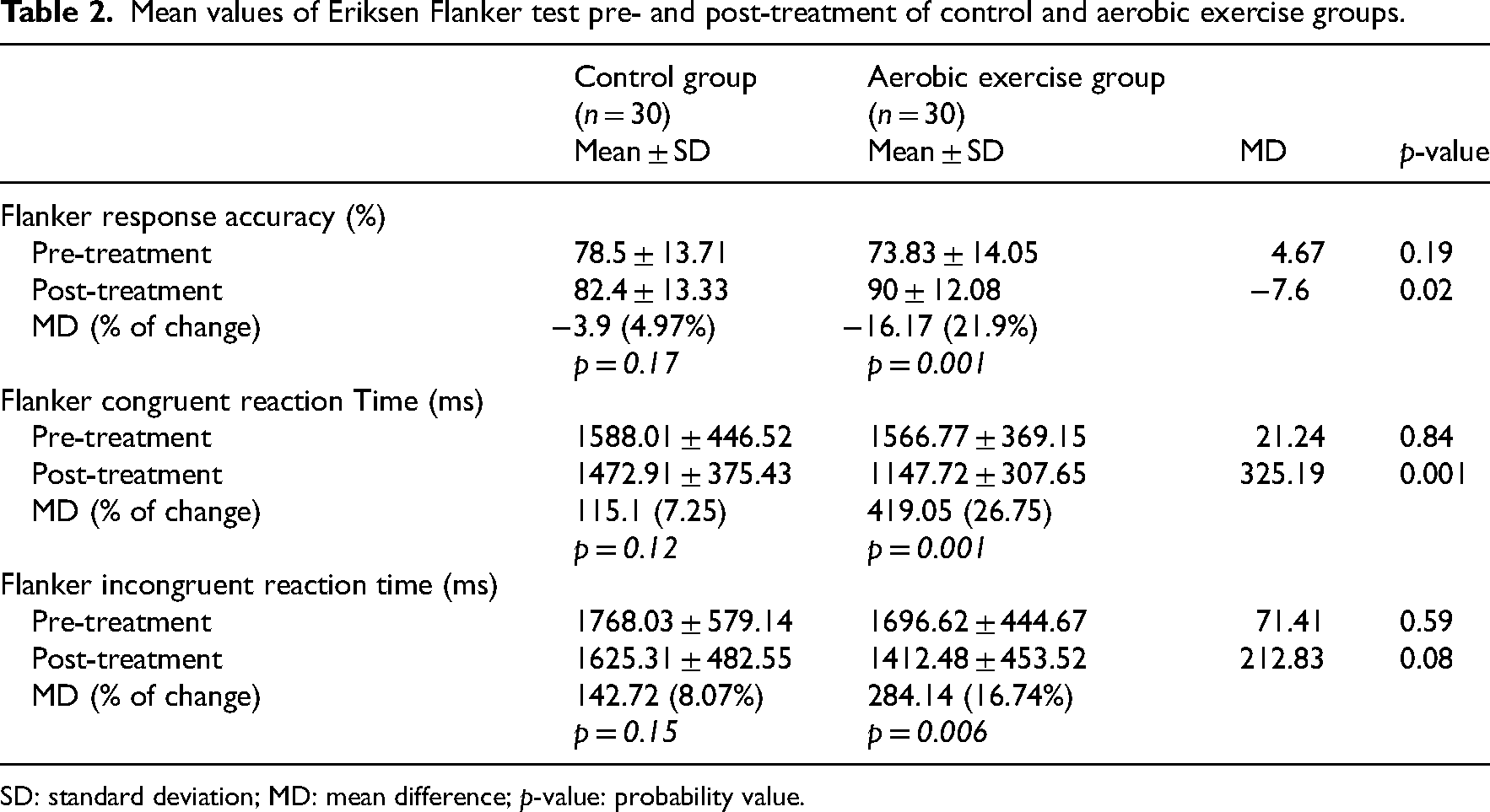
SD: standard deviation; MD: mean difference; p-value: probability value.
Mean values of Stroop Color–Word Test pre and post treatment of control and aerobic exercise groups.
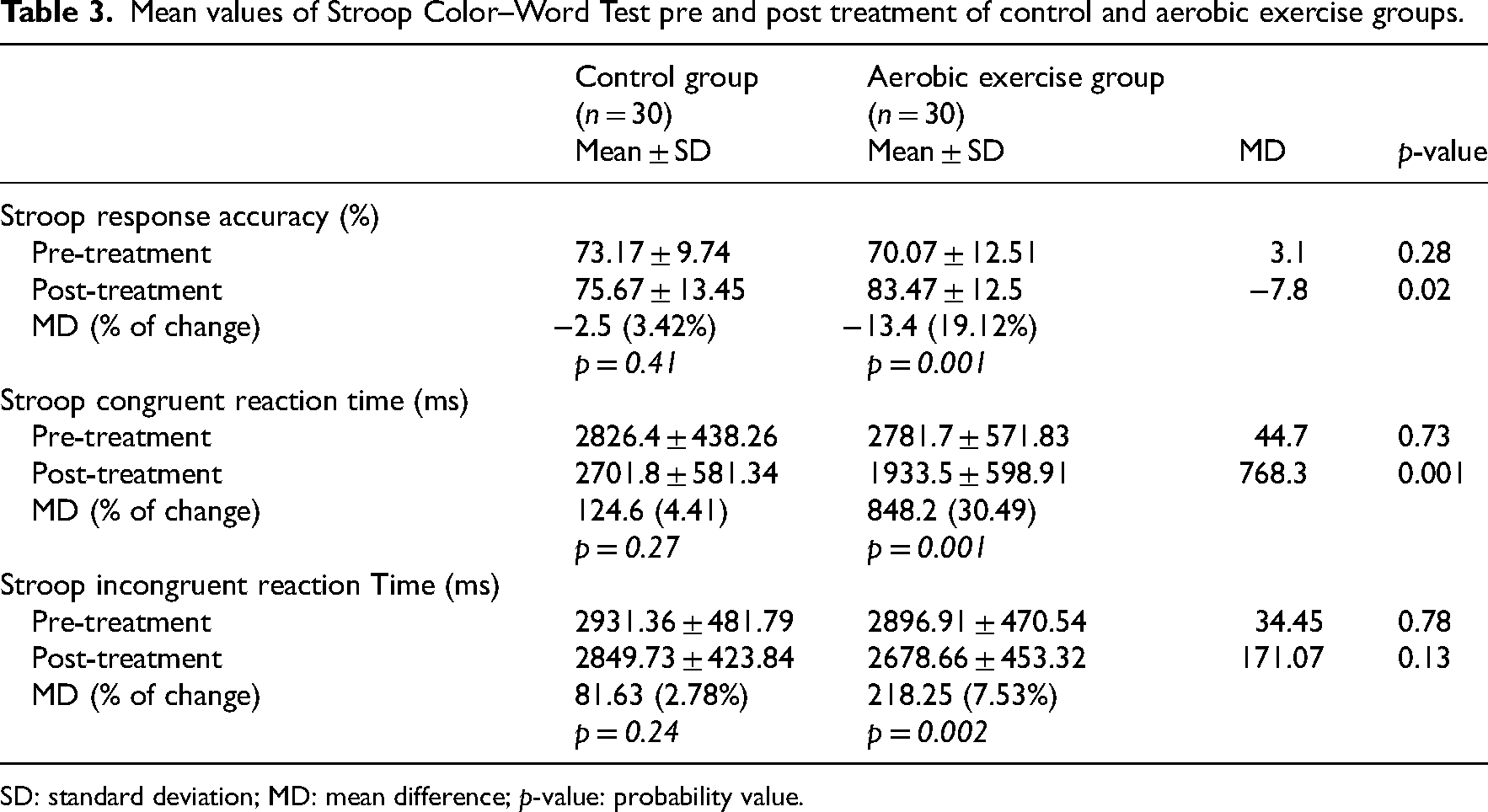
SD: standard deviation; MD: mean difference; p-value: probability value.
Within-group comparisons in the control group
Comparing pre- and post-treatment results, the control group did not show any statistically significant increases in Flanker response accuracy (79 ± 14% vs. 82 ± 13%, p = 0.17) and Stroop response accuracy (73 ± 10% vs. 76 ± 14%, p = 0.41). Likewise, no significant decreases between pre- and post-treatment results were found for the Flanker congruent reaction time, Flanker incongruent reaction time, Stroop congruent reaction time, and Stroop incongruent reaction time (p > 0.05, Tables 2 and 3). These results indicate that standard-of-care physical therapy has no significant effect on inhibitory control of executive functions in our study sample.
Within-group comparisons in the aerobic exercise group
Comparing pre- and post-intervention results, the aerobic exercise group showed a statistically significant increase in Flanker response accuracy (74 ± 14% vs. 90 ± 12%, p = 0.001) and Stroop response accuracy (70 ± 13% vs. 84 ± 13%, p = 0.001). Likewise, significant decreases between pre- and post-treatment results, indicating improved inhibitory control of executive functions, were found for the Flanker congruent reaction time, Flanker incongruent reaction time, Stroop congruent reaction time, and Stroop incongruent reaction time (p < 0.05, Tables 2 and 3).
Discussion
Impairment in executive function is one of the primary impairments in children with cerebral palsy that significantly limit functional independence and reduce quality of life. Our study aimed to investigate the efficacy of aerobic exercise training on inhibitory control of executive function in children with hemiplegic cerebral palsy. Sixty children with left-side hemiplegic cerebral palsy were enrolled in this study. Our results suggest that aerobic exercise training improved our study population's inhibitory control of executive function. This improvement is indicated by the increases in response accuracy percentage and decreases in congruent reaction times in both cognitive tests. Although we found no changes in incongruent reaction times, these findings suggest that adding an aerobic exercise training component to standard-of-care physical therapy is advisable and may lead to some degree of improved cognitive function in children with hemiplegic cerebral palsy. These findings are consistent with many previous studies showing cognitive improvements post-exercise in multiple populations.35–41
The patient population we chose for this study was children with left-side hemiplegic cerebral palsy (indicating insult to the right hemisphere). As indicated by Bonato, 27 damage in the right hemisphere is one of the most frequent deficits that lead to impairment or loss of ability to react to the process of sensory stimuli. In addition to only including children with left-side deficits, we excluded any interference of motor deficits in hand function by using the unaffected hand during the assessment of inhibitory control of executive functions in both cognitive tests. Our inclusion criteria were also limited to children between 7 and 11 years of age since this is the age of marked development in executive function, especially inhibitory control.22,42
Additionally, we found no differences between groups in Flanker incongruent reaction time and Stroop incongruent reaction time. The lack of changes in incongruent times may be due to the difficulty of the incongruent tests, which are more challenging and require more attention than congruent times. The ability of the brain to read words is faster than the ability to recognize colors. According to the Selective Attention Theory, the brain requires greater attention to recognize colors than encode a word. This may explain why 30 min of continuous aerobic training was sufficient to show improvements in congruent times but not incongruent times. 35 Improvements in executive function following aerobic exercise training have been reported in healthy adults, 36 apparently healthy preadolescent children, 37 in children with attention deficit hyperactive disorder,38,39 and in children with spastic cerebral palsy. 43 Similar results were also reported in children with cerebral palsy after a single intensive bout of aerobic training. 19
Our study has a number of limitations. We only included children that scored 28 or more on the pediatric symptom checklist. It is unclear if the same results would have been found in children with cerebral palsy scoring lower. Furthermore, despite there being no significant differences between groups in baseline measures, there were minimal age differences between groups, with the aerobic exercise group being slightly older and with a higher median school grade (Table 1). Minimal age and school grade differences in this age group, given the relatively small sample size, could amplify practice effects unrelated to the exercise intervention. This effect could also be exaggerated by the inter-test interval of 12 weeks, especially since there were no other assessment points in between. We did not perform a standardized cardiopulmonary exercise test to determine true maximum heart rate values. As such, the exercise intensity prescription may not have provided a sufficient exercise load for all participants. Furthermore, since we did not perform a cardiopulmonary exercise test pre- and post-exercise, we cannot determine the actual improvement in cardiorespiratory fitness resulting from the aerobic exercise training. However, the benefits observed in inhibitory control indicate that aerobic exercise training was effective. Furthermore, the assessors collecting data were not blinded to group assignments as the assessors also provided the treatment sessions. However, since testing was entirely computerized, we do not think this significantly impacted our results. Additionally, another potential limitation is that we did not control for physical activity outside of scheduled treatment sessions; however, this was the case across both groups. This has been removed as suggested.
Finally, the battery of cognitive tests used in this study is also a source of limitation. Despite the extensive use of both tests in research and clinical settings, the nature of neuropsychological tests, in general, is limited by common deficiencies such as a lack of adequate normative data, presence of practice effects, and limited reliability and validity. Additionally, these tests require specific baseline cognitive and motor skills and may present difficulties for children of this age group with cerebral palsy, such as requiring reading ability that may potentially be advanced for the sample population. This may therefore pose a limit to dependability and reliability. However, due to the wide use and adoption of these tests and the motor level of this population, they were utilized in this study. Nonetheless, these results need to be further replicated using other assessment tools such as Children's Stroop or evaluation of reading age prior to test administration.
The findings of our study suggest that aerobic exercise training may positively impact executive function by improving inhibitory control in children with hemiplegic cerebral palsy. We also conclude that adding aerobic exercise to standard-of-care physical therapy may provide additional cognitive benefits to this patient population. Given the wide range of documented benefits of aerobic exercise training and the results of this study, we believe that aerobic exercise training should be added to the physical therapy plan of care for children with hemiplegic cerebral palsy whenever feasible. However, further research is required to establish these results and determine other effects of aerobic exercise on cognitive abilities in children with hemiplegic cerebral palsy and the exact physiological mechanisms behind these effects. In addition, future research should focus on the optimal exercise prescription required to optimize the beneficial effects of exercise in this patient population.
Clinical message
Aerobic exercise training in conjunction with standard-of-care physical therapy has a positive impact on inhibitory control of executive function in children with hemiplegic cerebral palsy.
Aerobic exercise training improves some but not all aspects of inhibitory control of executive function in children with hemiplegic cerebral palsy.
Supplemental Material
sj-docx-1-cre-10.1177_02692155231208578 - Supplemental material for Influence of aerobic exercise on inhibitory control of executive functions in children with hemiplegic cerebral palsy: A randomized controlled trial
Supplemental material, sj-docx-1-cre-10.1177_02692155231208578 for Influence of aerobic exercise on inhibitory control of executive functions in children with hemiplegic cerebral palsy: A randomized controlled trial by Nehad A Abo-zaid, Amira M El-Gendy, Islam Hewidy, Mohammed Essam Ali and Ahmad Sabbahi in Clinical Rehabilitation
Supplemental Material
sj-docx-2-cre-10.1177_02692155231208578 - Supplemental material for Influence of aerobic exercise on inhibitory control of executive functions in children with hemiplegic cerebral palsy: A randomized controlled trial
Supplemental material, sj-docx-2-cre-10.1177_02692155231208578 for Influence of aerobic exercise on inhibitory control of executive functions in children with hemiplegic cerebral palsy: A randomized controlled trial by Nehad A Abo-zaid, Amira M El-Gendy, Islam Hewidy, Mohammed Essam Ali and Ahmad Sabbahi in Clinical Rehabilitation
Footnotes
Acknowledgments
The authors thank all children and parents who kindly participated in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.