
Abstract
Objective
This study aimed to determine whether total dietary intake assessed in the acute phase after hip fracture surgery is associated with walking ability.
Design
The retrospective observational study.
Setting
A single institution.
Participants
Patients with hip fractures aged ≥65 years.
Main measures
Dietary intake was recorded daily on an 11-point scale using visual plate waste. The primary outcome was walking ability, which was assessed using functional ambulation categories at discharge. We categorised the patients into those with improved walking ability (functional ambulation categories score ≥3) and those without (<3). Cox proportional hazard models were used to estimate hazard ratios and 95% confidence intervals for functional ambulation categories according to total dietary intake during acute hospitalisation.
Results
In total, 182 patients were included with a median age of 85 years; 73.6% were women. The median dietary intake during the first week after surgery, the second postoperative week, and throughout the postoperative period were 24.5, 28.4, and 27.1 kcal, respectively. After adjusting for potential confounders, high total dietary intake (hazard ratio, 1.05; 95% confidence intervals, 1.02–1.09; P = .006) and high dietary intake after the second week (hazard ratio, 1.04; 95% confidence intervals, 1.01–1.08; P = .017) were associated with walking ability.
Conclusions
Total dietary intake was associated with walking ability at discharge during the acute postoperative period after hip fracture. Dietary intake following the second postoperative week may play a significant role in the recovery of walking ability.
Introduction
Hip fracture is a serious condition with a poor prognosis in older individuals owing to high mortality rates and incomplete recovery of functional disability after fracture. Even with extensive rehabilitation, the activities of daily living and quality of life of hip fracture survivors do not recover completely to their pre-fracture levels,1,2 with 43.1–55.2% able to walk at their pre-fracture level one year later, and 18.7–28.5% becoming immobile.3,4 The persistence of disability highlights the urgent need for effective interventions to restore walking ability after hip fracture.
Common risk factors associated with functional disability after hip fracture include age, sex, place of residence, comorbidities, pre-fracture walking ability, fracture type, and cognitive function.5,6 Additionally, malnutrition is a poor prognostic factor, as malnourished patients with hip fracture have higher mortality rates, prolonged functional disability, and longer hospital stays.7,8 Conversely, comprehensive care including nutritional intervention, nutritional intervention combined with home environment rehabilitation, or high-intensity resistance training combined with nutritional intervention has been reported to shorten hospital stay and improve independence in activities of daily living compared with usual care.9,10
Patients with hip fractures often have low dietary intake postoperatively, which can reduce their ability to perform activities of daily living; the spontaneous dietary intake is often below the required level after surgery in these patients.11,12 A previous study reported that, in older patients with hip fractures, lower dietary intake within the first week after surgery was associated with lower activities of daily living at discharge from an acute care hospital.11,12 However, given the factors that contribute to low postoperative dietary intake, growing interest in active nutritional intervention during hospitalisation, and association between increased activity and dietary intake, it is crucial to evaluate dietary intake beyond the first week after surgery. The second postoperative week may be an especially critical period; however, further research is needed. Therefore, the aim of this study was to determine whether dietary intake assessed in the acute phase after hip fracture surgery was associated with walking ability. In addition, we investigated the relationship between walking ability and dietary intake during different periods of the acute phase.
Methods
This was a retrospective observational study of the medical records of patients with hip fractures admitted at the Kobe City Nishi-Kobe Medical Center between April 2018 and November 2021. The inclusion criteria were older adults aged ≥65 years who were able to walk before the fracture. The exclusion criteria included patients with conservative treatment, partial or no postoperative weight bearing, pathologic fractures, or terminal malignancy. Patients with missing data were also excluded. We analysed the relationship between postoperative dietary intake and walking ability at hospital discharge.
Postoperative patients with hip fractures were provided with medical care according to the clinical path developed by the hospital. In addition, patients with hip fractures were treated with comprehensive multidisciplinary care through systematic weekly conferences and rounds held in a multi-professional setting.
As this was a retrospective study, we used an opt-out procedure instead of obtaining written informed consent to guarantee participants the right to withdraw from the study at any time. This study was conducted following the tenets of the Declaration of Helsinki, and the study protocol was approved by the Nishi-Kobe Medical Center Ethical Review Committee (number: 2022-03).
In this study, dietary intake was assessed by ward nurses and caregivers. They observed all meals and rated intake of each main and side dish at every meal. An 11-point scale was used, which was based on visual estimation of plate waste when the meals were withdrawn. 13 The data included multinutrient supplements provided by the hospital; however, it did not include snacks that were souvenirs or preferences. We calculated a guideline value for energy or protein requirements in older adults: 30 kcal or 1.2 g of protein per kg of body weight per day. 14 At the individual patient level, differences in food forms were considered to be based on individual preference and swallowing function. A dietitian monitored the intake of all meals during hospitalisation and provided individualised diets tailored to the preferences and swallowing function of each patient. We calculated the daily dietary intake (kcal/body weight/day) or protein intake (g/body weight/day) per standard body weight. 14 We defined the dietary intake for each week as the average of any three days of the week.
The primary outcome was walking ability at discharge as assessed using functional ambulation categories performed by trained physical therapists.15,16 The functional ambulation category is a six-point scale of walking ability ranging from 0 (unable to walk) to 5 (independent), based on the amount of physical assistance required to walk 15 m indoors without the use of a walker. The functional ambulation category score was defined as follows: 5 = independent walking and stair climbing; 4 = independent walking on flat surfaces but requiring supervision on stairs, inclines, and uneven surfaces; 3 = supervision required when walking; 2 = dependent on physical assistance, such as intermittent or continuous light touch, while walking; 1 = dependent on physical assistance, such as continuous manual contact, while walking; and 0 = unable to walk at all or requiring the assistance of two therapists. The reliability and validity of the functional ambulation categories have been demonstrated in patients with hip fractures previously.17,18 We defined a functional ambulation category score ≥3, i.e., not requiring assistance from a caregiver, as an improvement in walking ability because the patients were in the early postoperative recovery phase. 19
We evaluated clinical data, such as age, sex, body mass index, fracture type (neck or trochanteric), pre-fracture walking ability, cognitive function, and length of hospital stay, from electronic medical records. Pre-fracture walking ability was assessed using the functional ambulation category score. In cases in which the cognitive function of the patient was impaired and self-report was unreliable, the necessary information was obtained from family members or facility staff. Cognitive function was assessed by a physical therapist using the Hasegawa Dementia Scale–Revised early after admission. 20
Categorical variables are presented as numbers (percentage). Quantitative variables are presented as mean ± standard deviation or median (interquartile range 25–75 percentile) according to normality. Adjusted Cox proportional hazards models were used to estimate the hazard ratios and 95% confidence intervals for functional ambulation categories according to total dietary intake during acute hospitalisation to determine whether total dietary intake during acute hospitalisation was associated with walking ability at discharge. For additional analysis, the hazard ratios were calculated using a model with dietary intake in the first or second postoperative week as the independent variable to evaluate the effect of timing. We selected potential confounders, such as age, sex, fracture type, cognitive function, and pre-fracture walking ability, which have important clinical implications for postoperative dietary intake and recovery of functional disability in patients with hip fracture. A previous study identified pre-injury mobility as a significant predictor of discharge mobility. 5 Additionally, the majority of patients are unable to walk immediately after surgery, making it challenging to determine the optimal timing for baseline walking ability assessments after surgery. Based on these considerations, we adjusted for pre-fracture walking ability in this study. Similarly, we adjusted for the fracture type rather than the surgical procedure, as certain surgical procedures necessitate a period of non-weight-bearing after surgery, which can have a significant impact on the recovery of postoperative activities of daily living. However, patients requiring a period of non-weight-bearing after surgery were excluded from this study, ensuring that all included patients could walk with full weight-bearing after surgery. Therefore, fracture type was selected as a covariate. In the secondary analysis, we created Cox proportional hazards models for functional ambulation categories by total protein intake, protein intake during the first week after surgery, and protein intake after the second postoperative week to clarify the association between postoperative protein intake and walking ability at discharge. Statistical significance was set at P < .05. All statistical analyses were performed using SPSS version 19.0 (IBM Japan, Tokyo, Japan).
Results
The present study included 278 patients with hip fracture aged ≥65 years who were able to walk before the fracture. Among them, 96 patients were excluded: 53 received conservative treatment after surgery with partial or no weight-bearing, three patients were diagnosed with pathological fractures, three patients had terminal malignant disease, and 37 had missing data. In total, 181 patients were included in the analysis (Figure 1).
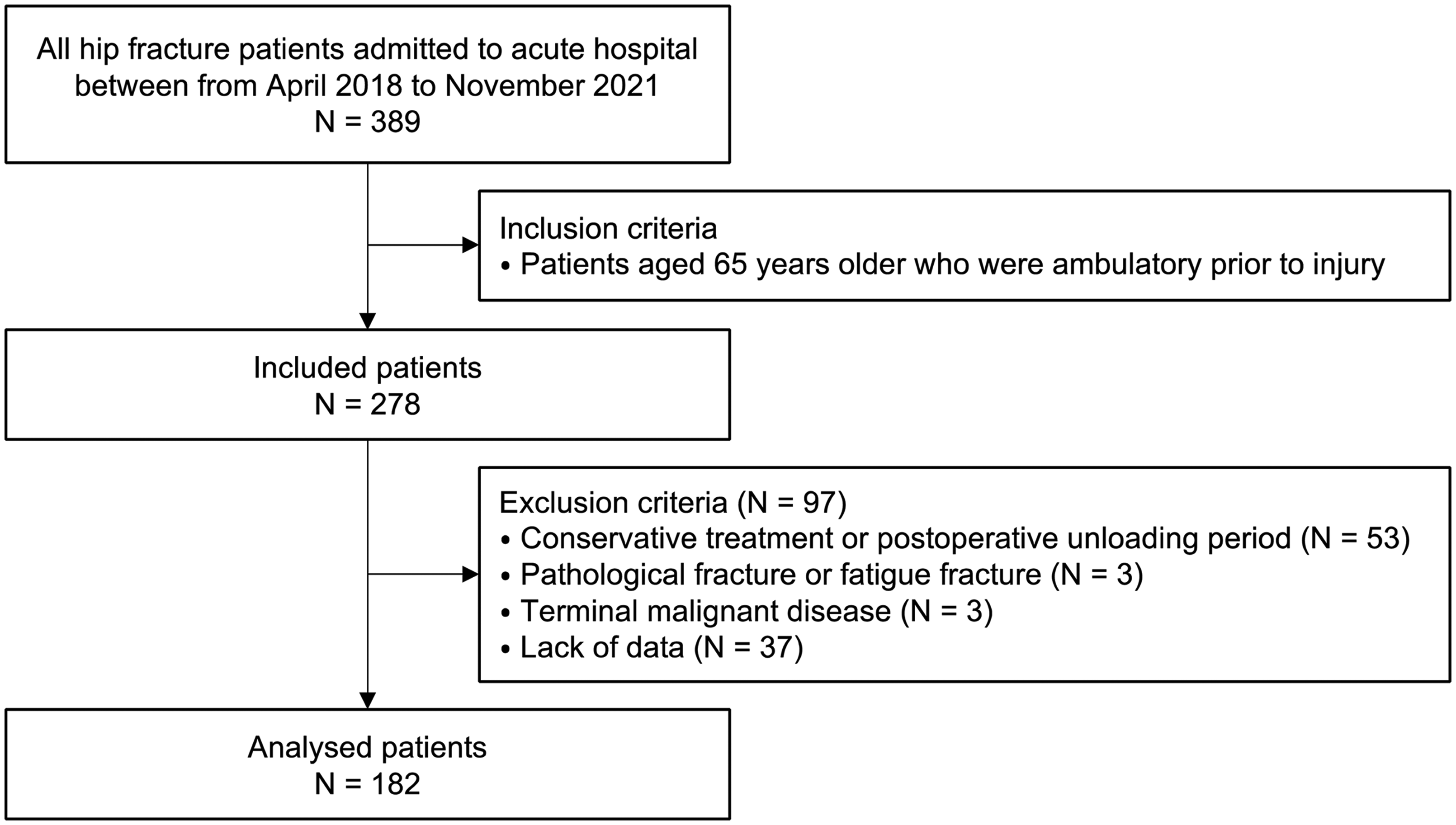
Flowchart of patient inclusion.
Patient characteristics are shown in Table 1. The median age of all patients was 85 years (interquartile range: 78–88 years), and 134 (73.6%) were women; the median body mass index was 20.7 kg/m2 (interquartile range: 18.2–22.8), fracture types were 109 (59.9%) neck and 73 (40.1%) trochanteric, median Hasegawa Dementia Scale-Revised was 22 points (interquartile range: 14–27), and median hospital stay was 20 days (interquartile range: 16−27). Three patients were discharged within two weeks, but none were discharged within ten days. The median dietary intake during the first week after surgery, second postoperative week, and throughout the postoperative period was 24.5 kcal (interquartile range: 19.2–28.0), 28.4 kcal (interquartile range: 24.4–31.4), and 27.1 kcal (interquartile range: 22.6–29.9) per kg body weight, respectively. Additionally, the median protein intake during the first week after surgery, second postoperative week, and throughout the postoperative period was 1.01 g (interquartile range: 0.82–1.19), 1.20 g (interquartile range: 1.00–1.34), and 1.14 g (interquartile range: 0.96–1.27) per kg body weight, respectively. The median functional ambulation categories score at discharge was 3 (interquartile range: 1–4), and 108 patients (59.3%) were able to walk without assistance (functional ambulation categories score ≥ 3); however, 74 patients (40.7%) were not able to do this.
Characteristics of the participants.
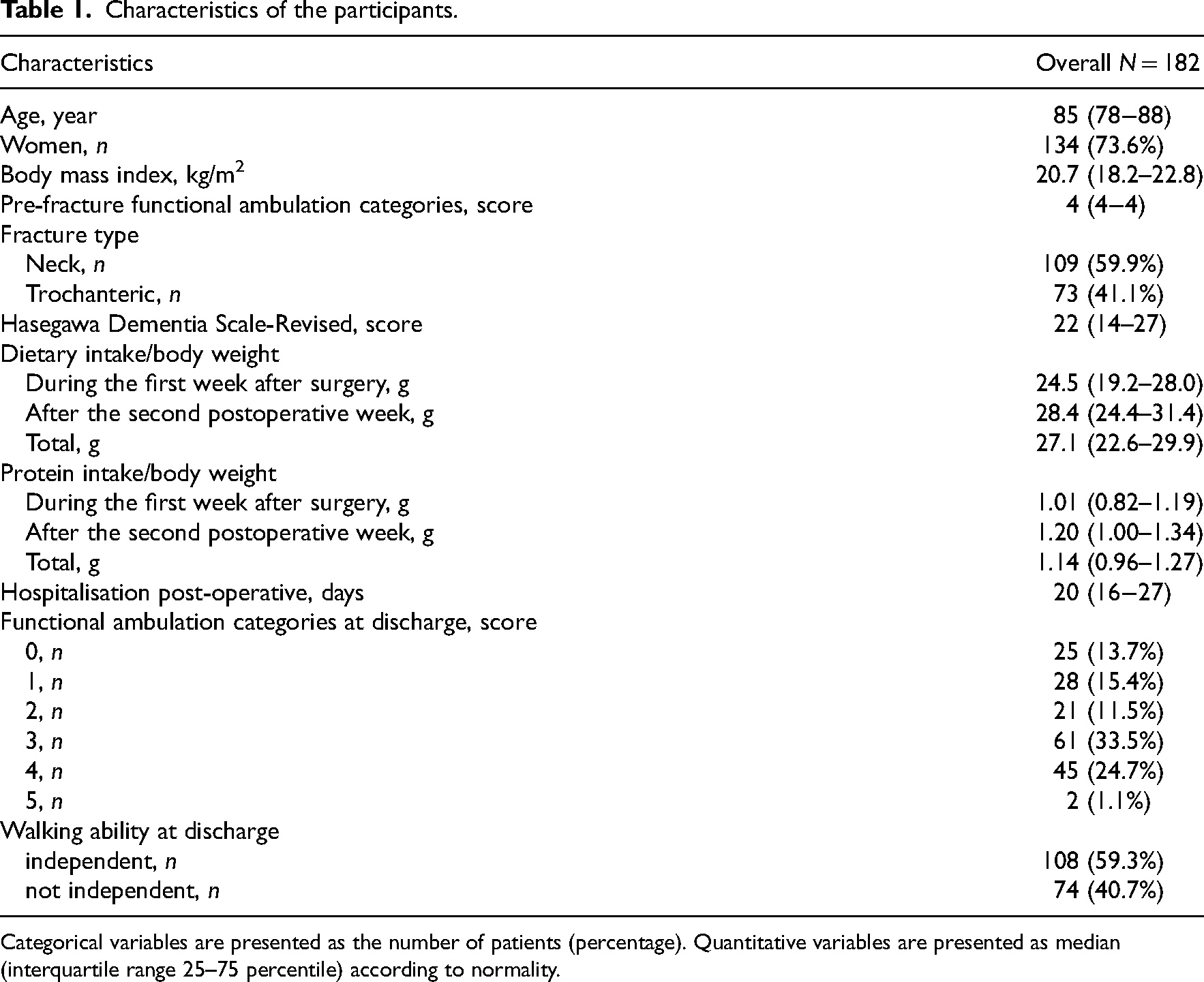
Categorical variables are presented as the number of patients (percentage). Quantitative variables are presented as median (interquartile range 25–75 percentile) according to normality.
The results of the Cox proportional hazards models for functional ambulation categories according to dietary intake per period during acute hospitalisation are shown in Table 2. High total dietary intake (hazard ratio, 1.06; 95% confidence intervals, 1.02–1.10; P = .001) and high dietary intake after the second postoperative week (hazard ratio, 1.05; 95% confidence intervals, 1.02–1.09; P = .002) were associated with walking ability. However, dietary intake during the first week after surgery was not associated with walking ability at discharge (hazard ratio 1.02; 95% confidence intervals: 0.98–1.05; P = .340). After adjusting for potential confounders, high total dietary intake (hazard ratio, 1.05; 95% confidence intervals,1.02–1.09; P = .006) and high dietary intake after the second week (hazard ratio, 1.04; 95% confidence intervals,1.01–1.08; P = .017) were associated with walking ability.
Cox proportional hazards models for functional ambulation categories by dietary intake per period during acute hospitalisation.
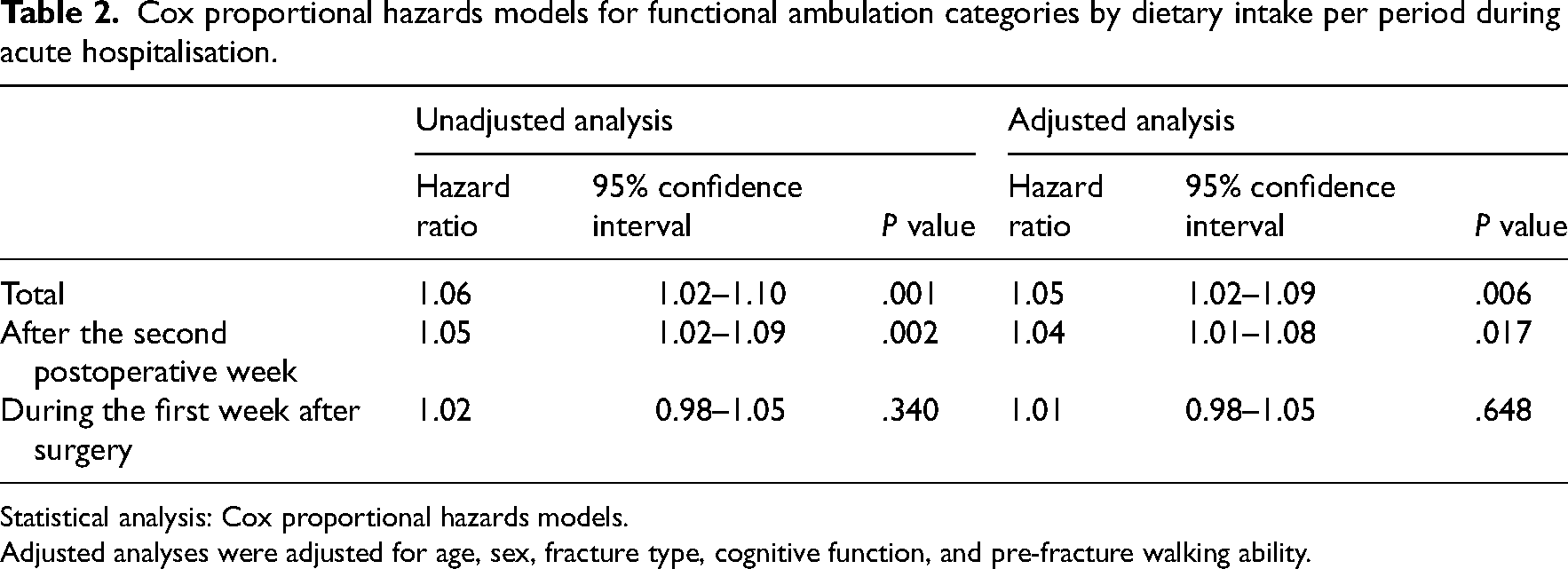
Statistical analysis: Cox proportional hazards models.
Adjusted analyses were adjusted for age, sex, fracture type, cognitive function, and pre-fracture walking ability.
The results of the Cox proportional hazards models for functional ambulation categories according to protein intake per period during acute hospitalisation are shown in Table 3. High total protein intake (hazard ratio, 3.11; 95% confidence intervals, 1.34–7.25; P = .008) and high protein intake after the second week (hazard ratio, 2.94; 95% confidence intervals: 1.35–6.41; P = .007) were associated with walking ability. However, protein intake during the first week after surgery was not associated with walking ability at discharge (hazard ratio, 1.37; 95% confidence intervals: 0.66–2.86; P = .404). After adjusting for potential confounders, high total protein intake (hazard ratio, 2.81; 95% confidence intervals, 1.15–6.90; P = .024) was associated with walking ability at discharge.
Cox proportional hazards models for functional ambulation categories by protein intake per period during acute hospitalisation.
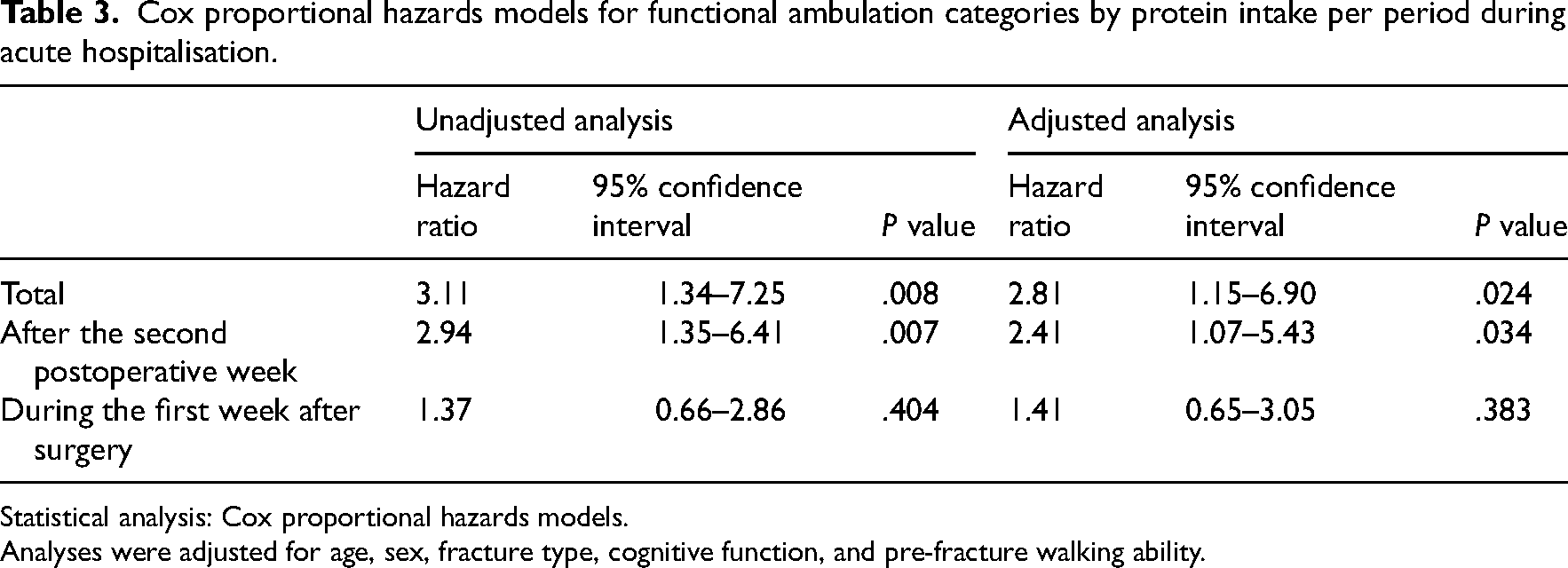
Statistical analysis: Cox proportional hazards models.
Analyses were adjusted for age, sex, fracture type, cognitive function, and pre-fracture walking ability.
Discussion
This study demonstrated that high total dietary intake was associated with walking ability at discharge in patients with hip fractures, even after adjusting for potential confounders. Furthermore, when evaluating the impact of timing, a high dietary intake after the second week was associated with improved walking ability at discharge. However, this association was not observed in the first week after surgery. In the secondary analysis, a high total protein intake was associated with walking ability at discharge after adjustment. To the best of our knowledge, this is the first study to examine the relationship between total dietary intake and walking ability throughout the acute postoperative phase by considering confounding factors. We believe that maintaining dietary intake after the second postoperative week is crucial for the recovery of walking ability.
The primary finding of this study was that the total dietary intake was associated with the walking ability at discharge. In the time-specific analysis, dietary intake during the second-week post-surgery was associated with improved walking ability at discharge; however, dietary intake during the first week was not associated with this. Existing literature has established a correlation between postoperative dietary intake and activities of daily living. For instance, Goisser et al. 11 found that patients consuming <25% of the provided diet in the first four days post-surgery demonstrate decreased mobility at discharge or after six months compared with those consuming >25%. Similarly, Inoue et al. 12 reported that patients who consume <70% of the recommended dietary intake within the first week after surgery experience diminished functional gain. Some studies have reported an association between dietary intake and the Functional Independence Measure within the first postoperative week.11,12 In contrast, this study identified an association between dietary intake and walking ability using the functional ambulation category score. The differences in the outcome measure characteristics may partly explain why our results differ from those of previous studies. In general, multidisciplinary geriatric interventions, including nutritional interventions, are effective in recovering activities of daily living in patients with hip fractures, and such care is typically provided in standard hospital settings. Maintaining an individualised dietary intake that meets patient requirements is crucial for functional recovery after surgery. This study monitored all dietary intakes during the acute hospital stay and found that maintaining a high dietary intake throughout the acute period, including the second week and beyond, may be critical for the recovery of walking ability.
Another significant finding of this study was the independent association between total protein intake throughout the acute phase and walking ability at discharge. Although it is evident that protein-rich oral nutritional supplements can improve nutritional indices, whether the provision of oral nutritional supplements leads to improvements in activities of daily living remains uncertain. 21 Protein intake also plays a critical role in muscle repair. As hypermetabolism persists for at least three months after surgery, 22 reducing protein intake during this time may result in increased catabolism. Insufficient protein intake may trigger muscle dysfunction owing to protein breakdown, thereby delaying functional recovery. 23 Consequently, both diminished dietary and protein intakes could be crucial factors contributing to a decline in motor function in patients with postoperative hip fractures. To elucidate this relationship, high-quality clinical trials that include blood data and muscle strength assessments should be designed.
The postoperative dietary intake observed in our patients with hip fractures was comparable to that observed in other patients in the acute phase. Inoue et al. 12 found that patients with hip fractures have a dietary intake, as assessed by visual plate waste, equivalent to 80% of the recommended intake during the first seven days after surgery. In this study, the dietary intake during the first week after surgery was 24.5 (19.2–28.0) kcal/day/body weight, which was 82% of the recommended amount. Umezawa et al. 24 also reported that the dietary intake during the first seven days after admission to a recovery hospital is 29.9 kcal/day/body weight. In our study, the dietary intake after the second week was 28.4 kcal/day/kg body weight. Therefore, the dietary intake of our patients with hip fractures was consistent with that reported in previous studies, suggesting comparable levels of care.
This study had some limitations. Firstly, this was an observational study conducted at a single institution; hence, caution is necessary when generalising our findings. Second, the assessment of dietary intake did not include snacks and drinks that were brought as a gift or were personally preferred. Despite this limitation, however, there were no clear differences in dietary intake between participants in this study and those in previous studies. In addition, when using a visual assessment method such as plate waste, there is a possibility that food intake may be overestimated. Therefore, the interpretation of the results should be approached with caution. Thirdly, this study did not investigate the cause of inadequate dietary intake when it fell below the recommended levels. However, patients with hip fractures were systematically treated with comprehensive multidisciplinary care through multidisciplinary conferences, which we believe will benefit these patients. Finally, muscle strength and postoperative pain, which are crucial factors in the recovery of walking ability, 25 were not assessed in this study. Therefore, the possibility of other confounding factors, such as pain, that may have affected the recovery of walking ability, should be considered.
In conclusion, total dietary intake was associated with walking ability at discharge during the acute postoperative period after hip fracture. Dietary intake following the second postoperative week may play a significant role in the recovery of walking ability.
Clinical messages
In patients with hip fractures, during the acute postoperative period, total dietary intake is associated with walking ability at discharge.
Dietary intake after the second postoperative week may play a significant role in the recovery of walking ability.
Footnotes
Acknowledgements
We would like to express our gratitude to the members of the Rehabilitation Nutrition Laboratory for their cooperation in this study.
Author contributions
Hikaru Kobayashi: conceptualisation; data curation; formal analysis; investigation; methodology; roles/writing – original draft; writing – review and editing. Koutatsu Nagai: conceptualization; methodology; supervision; writing – review and editing. Yasuhiro Shimamura: conceptualization; data curation; methodology. Masami Hidaka: conceptualization; methodology; writing – review and editing. Akiko Mori: conceptualization; methodology; writing – review and editing. Kaoru Sakuma: conceptualization; methodology; writing – review and editing. Tomoyuki Ogino: conceptualization; methodology; writing – review and editing.
Consent to participate
As this was a retrospective study, we used an opt-out procedure instead of obtaining written informed consent to guarantee participants the right to withdraw from the study at any time.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted following the tenets of the Declaration of Helsinki, and the study protocol was approved by the Nishi-Kobe Medical Center Ethical Review Committee (number: 2022-03).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.