
Abstract
Objective
This scoping review evaluates the current use of driving simulators in neurorehabilitation, focusing on diagnostic assessment and therapeutic training in neurological populations.
Data Sources
We searched nine major databases for studies published through September 2025, using broad terms related to simulated driving and neurorehabilitation.
Review Methods
Following PRISMA-ScR guidelines, we used ASReview software with active learning to identify relevant studies. Articles were grouped into diagnostic, therapeutic, review, and special interest categories, with data charted manually by two reviewers.
Results
Of 224 included articles, 124 addressed diagnostic use and 25 examined therapeutic interventions. Simulated driving was often evaluated for its predictive value in determining fitness-to-drive. Combined with neuropsychological tests, simulator outcomes reliably identified key cognitive predictors such as attention and executive function. Twenty-eight studies included on-road driving comparisons, supporting simulator validity. Simulator-based interventions showed benefits for patients with stroke, traumatic brain injury, or Parkinson's disease, particularly for improving tactical driving skills and awareness. Benefits were more pronounced in individuals with mild to moderate impairments. Simulators were generally well-accepted across patient populations.
Conclusion
Despite the heterogeneity of the literature, there is evidence to support the use of driving simulators as a promising tool for evaluating and improving fitness to drive in neurorehabilitation.
Introduction
Neurological disorders such as traumatic brain injury (TBI) or cerebrovascular accident (CVA) frequently result in impaired driving, characterised by cognitive, motor, perceptual, or behavioural deficits. ‘Fitness-to-drive’ (FTD) refers to the mental and physical capacities required for safe driving. Balancing individual autonomy with societal safety underscores the importance of accurate driving assessments in neurorehabilitation. Current assessment methods include cognitive testing, on-road evaluations, and, increasingly, driving simulators. Cognitive tests are widely used due to their accessibility and psychometric rigor. However, their predictive validity for real-world driving performance remains limited.1,2 On-road assessments, while often considered the gold standard, are logistically demanding and not without safety risks. As a result, driving simulators are gaining popularity as a safer and more flexible alternative.3–5
Simulators allow for the controlled presentation of critical driving scenarios and offer ecologically valid assessments. 6 They also facilitate cost-effective and repeatable testing and training. These benefits have led to growing interest in their use for both diagnostic and therapeutic purposes. At the same time, significant variability exists among simulators in terms of technology, scenario design, and outcome measures. This inconsistency poses challenges for comparing findings and establishing best practices.
Efforts to restore driving ability in patients have included cognitive rehabilitation, driving instruction, and simulator-based training. Early results suggest promise across different neurological populations,7–10 but key questions remain regarding optimal training protocols, frequency, and long-term outcomes.11,12 Currently, there is no consensus on which neuropsychological tests or simulator metrics are best suited for specific patient groups. Practitioners often rely on local protocols, in the absence of standardized, evidence-based recommendations.13,14 This review aims to address that gap 15 by providing a scoping overview over the literature thus far.
We conducted a systematic scoping review to evaluate how driving simulators are applied in neurorehabilitation. The review was guided by the following research questions. (1) How are driving simulators used in neurorehabilitation settings? (2) What are the technological and usability aspects relevant to their implementation? (3) To what extent are driving simulators effective in the rehabilitation of neurological patients? (4) Which factors support the effective use of simulators in clinical practice?
To address these questions, we employed an active learning algorithm to optimize article selection and provide a structured synthesis of the existing literature. Our review's distinctive feature is its examination of the use of driving simulators in neurorehabilitation for various neurological patient groups. From a neuropsychological point of view, we provide an updated and comprehensive overview of the current state of research, comparing driving simulators with on-road driving ‒ the current gold standard ‒ to evaluate their role in diagnosing and rehabilitating fitness-to-drive. The aim of this review is to clarify current applications and provide guidance for future research and clinical practice.
Methods
The methodology for this review article was based on a structured framework derived from Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 16 Clarity, transparency, and an iterative approach are essential to ensure the review provides a robust map of the literature and identifies gaps.17,18 In this scoping review on driving simulators in neurorehabilitation, we used ASReview (Lab), an active-learning, human-in-the-loop screening tool, to prioritize records for screening; all inclusion/exclusion decisions were made by human reviewers. 19
We did not preregister this review because, consistent with PRISMA-ScR guidance, preregistration is optional for scoping reviews and our questions, search strings, and eligibility rules were iteratively refined as evidence accrued. Preregistration would have constrained this planned iteration. To maintain transparency, we version-controlled the protocol, search strategies, decision logs, and ASReview projects and make the data, scripts, and outputs available on reasonable request (https://gitlab.com/IcexTrice/mindwheels_drivesim).
Eligibility criteria
In this scoping review we examined literature on driving simulators in neurorehabilitation, with an emphasis on cognitive alterations following neurological conditions. Eligibility criteria were aligned with the review objectives and practice guidelines relevant to neuropsychology. We included peer-reviewed journal articles and book chapters (original studies, reviews, and mixed-methods) published up to September 2025 in English or German that evaluated the application of driving simulators in neurorehabilitation (diagnostics or therapy), including studies on effectiveness, usability, technological aspects, or patient outcomes; evaluations led by occupational therapists were eligible. We excluded work primarily targeting motor impairments, studies confined to narrowly defined diagnostic constructs (e.g., mild cognitive impairment and/or dementia), driver training in the general population, simulations not specific to driving, and non-original contributions (e.g., editorials, conference abstracts).
Information sources
The current reflection of knowledge and ongoing advancements in using driving simulators for neurorehabilitation encompassed a detailed and thorough search strategy across multiple databases from the inception of each database through to September 2025. The comprehensive literature search strategy encompassed seven major databases: CINAHL, Cochrane Library, Embase, Eric, Ovid (MEDLINE), Pubmed, PsychINFO, Scopus, and Web of Science, as delineated in Figure 1. The selection of these databases was predicated on their comprehensive coverage of literature, thus ensuring a broad yet relevant pool of potential sources. The search strategy was iteratively developed between JK, WT, and ZHW and further refined through team discussion. The final search results were exported to Papers Readcube and merged. First duplicate removal was done automatically by papers read cube before exporting the merged databases to ASreview Lab where more duplicates were automatically tracked and removed.
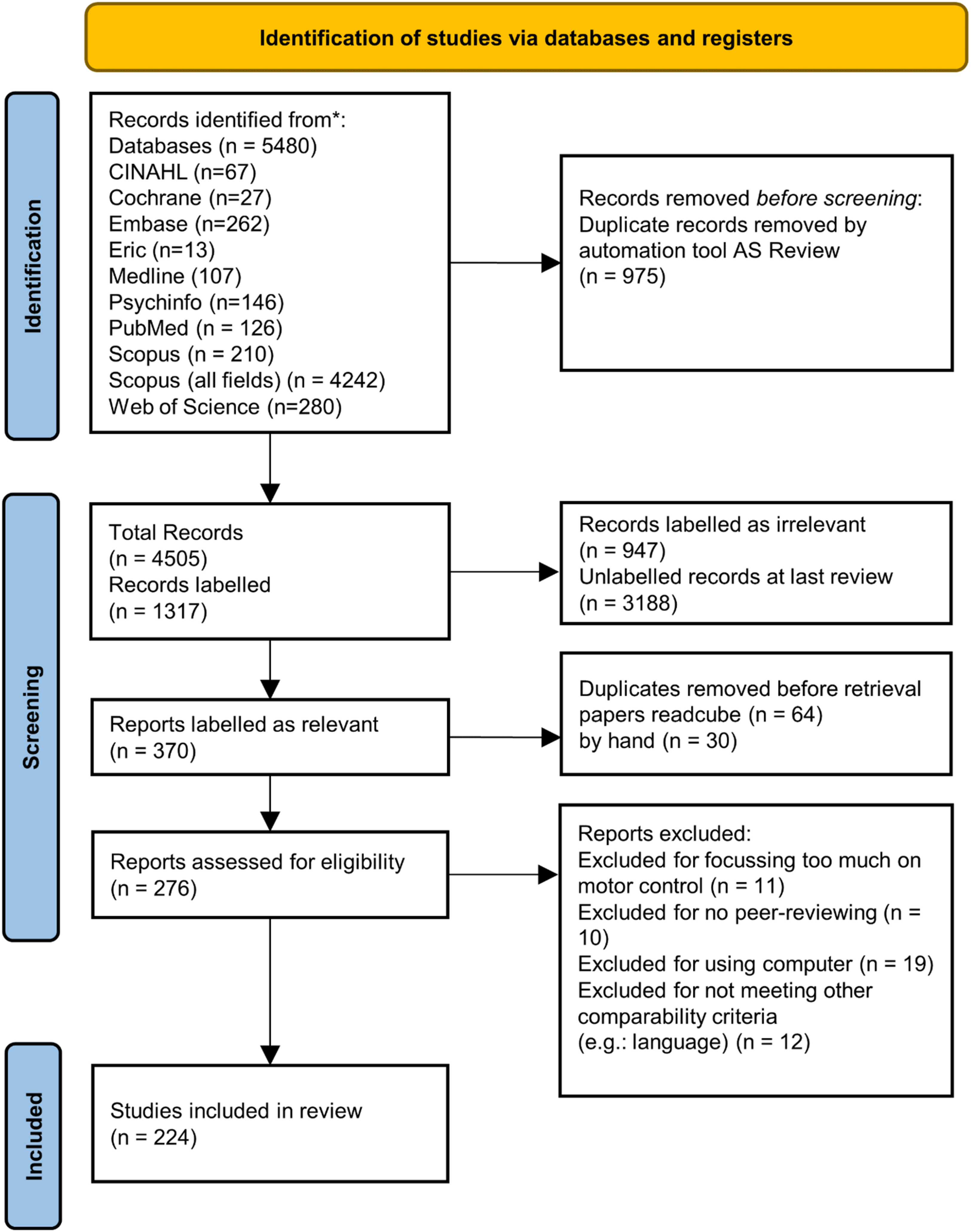
PRISMA flow-chart visualizing the number of articles in-/excluded at each timepoint.
Search
The search strategy employed a combination of keywords, as outlined below:
(“Driving Simulator” OR “Virtual Driving” OR “Simulated Driving”) AND (“Neurorehabilitation” OR “Driver Rehabilitation” OR “Stroke” OR “Cerebrovascular Disease” OR “Cerebrovascular Accident” OR “Traumatic Brain Injury” OR “Acquired Brain Injury” OR “Neurologic Cohort” OR “Brain Damage” OR “Brain Tumor” OR “Brain Lesion” OR “Neurodegenerative Disease” OR “Parkinson”). In developing the search strategy for the present review on driving simulators in neurorehabilitation, a broader approach was adopted to ensure comprehensive coverage of relevant studies. This decision aligns with the principles outlined by ASReview, which emphasises that the quality of a review depends heavily on the initial search process. The strategy employed an extensive array of keywords and a wide range of databases to maximise recall, defined as the probability of identifying all relevant studies, instead of prioritising precision, which focuses on retrieving only the most specific articles, reducing the risk of overlooking relevant studies that could offer valuable insights into the effectiveness, usability, and other patient-related outcomes associated with driving simulators. This broad, recall-oriented strategy was selected to supply a comprehensive pool of records for ASReview's active-learning loop while minimizing the risk of missed relevant studies.
Selection of sources of evidence
Screening workflow: We used ASReview (Lab) to prioritize records for screening while keeping all inclusion/exclusion decisions with human reviewers (human-in-the-loop). A standardized form, piloted on 30 citations, guided decisions. Two reviewers (WT, ZHW) independently screened an initial subset to calibrate decisions; disagreements were resolved by discussion. Screening then proceeded iteratively with one reviewer (ZHW) in ASReview and a second reviewer (WT) performing a full manual quality-control check of included and excluded records transferred back to ReadCube. Edge cases were flagged as ‘double check’, and any discrepancies were resolved by consensus.
ASReview was used in active-learning mode to prioritize the queue only (no automatic inclusion). Newly labeled records updated the model and re-ordered the remaining queue. The model was seeded with known-relevant studies identified during piloting plus a small random sample. Screening stopped at saturation (no new inclusions across successive prioritized batches), which we confirmed by checking the next prioritized tranche. Duplicates had been removed in ReadCube before export and were de-duplicated again within ASReview; only one instance of any record was screened.
Data extraction/data charting process
A proposal on which information to extract from the included articles was jointly developed. The data was abstracted by grouping articles into four distinct categories in a manual review procedure (diagnostics, therapy, reviews, and special interest). For each of these categories, the two reviewers (WT, ZHW) priorly discussed which metrics should be extracted and independently charted the data manually in tabular form.
Data charting
The data extraction process was guided by the research questions posed. The following key information was charted from the studies: The effectiveness of driving simulators in improving patient outcomes was a key area of interest. Furthermore, the types of neurorehabilitative conditions addressed were also documented. Finally, the overall impact of simulator-based interventions on patient therapy was considered.
Synthesis of results
The findings from the selected studies were consolidated and presented narratively. The sections were organised to provide a comprehensive overview of the usability and effectiveness of driving simulators, technological insights, and the therapeutic outcomes observed in patients. We chose a narrative synthesis because we could not conduct a meta-analysis due to heterogeneity in the interpretation of the descriptions. For example, besides using different types of driving simulators and cognitive tests, not all included studies gave a clear definition of performance parameters such as type of driving errors. We collected all information in tabular form (see Supplement Tables S1–7).
Results
The synthesis included 224 articles (Figure 1). The articles were manually grouped into original studies and review articles. First, the original studies were classified according to their focus (1) diagnostics, (2) therapeutic interventions and (3) special issues (Figure 2). Articles were further grouped by their study population including stroke, traumatic brain injury (TBI), Parkinson's Disease (PD), Huntington Disease (HD), Multiple Sclerosis (MS), and other acquired brain injuries (including mixed etiologies). Second, the articles in the categories diagnostics and therapeutic interventions were screened and classified according to their use of on-road driving assessment as validation checks. This was done in order to identify studies that compared the use of the driving simulator against the current ‘gold standard’ of on-road assessments and to obtain the most robust results. With this procedure 20 out of 124 articles with a diagnostic focus (Figure 2 and Supplement Table 1), and eight out of 25 articles with a focus on therapy were identified (Figure 2 and Supplement Table 2). In addition, 21 articles with special foci were identified including technical aspects of simulated driving (Supplement Table 6). For reviews, only systematic reviews were included in the present review, resulting in 27 review articles (Supplement Table 3). Among the 27 reviews, 22 reviews focused on diagnostic purposes of fitness-to-drive using driving simulators, while five reviews dealt with a therapeutic use of driving simulators in neurorehabilitation. These numbers clearly point out that in the literature the main interest in using driving simulators in neurorehabilitation settings lies in the diagnostics of fitness-to-drive evaluations. In the following of our scoping review we are going to go through the different foci that were identified in our literature sample.
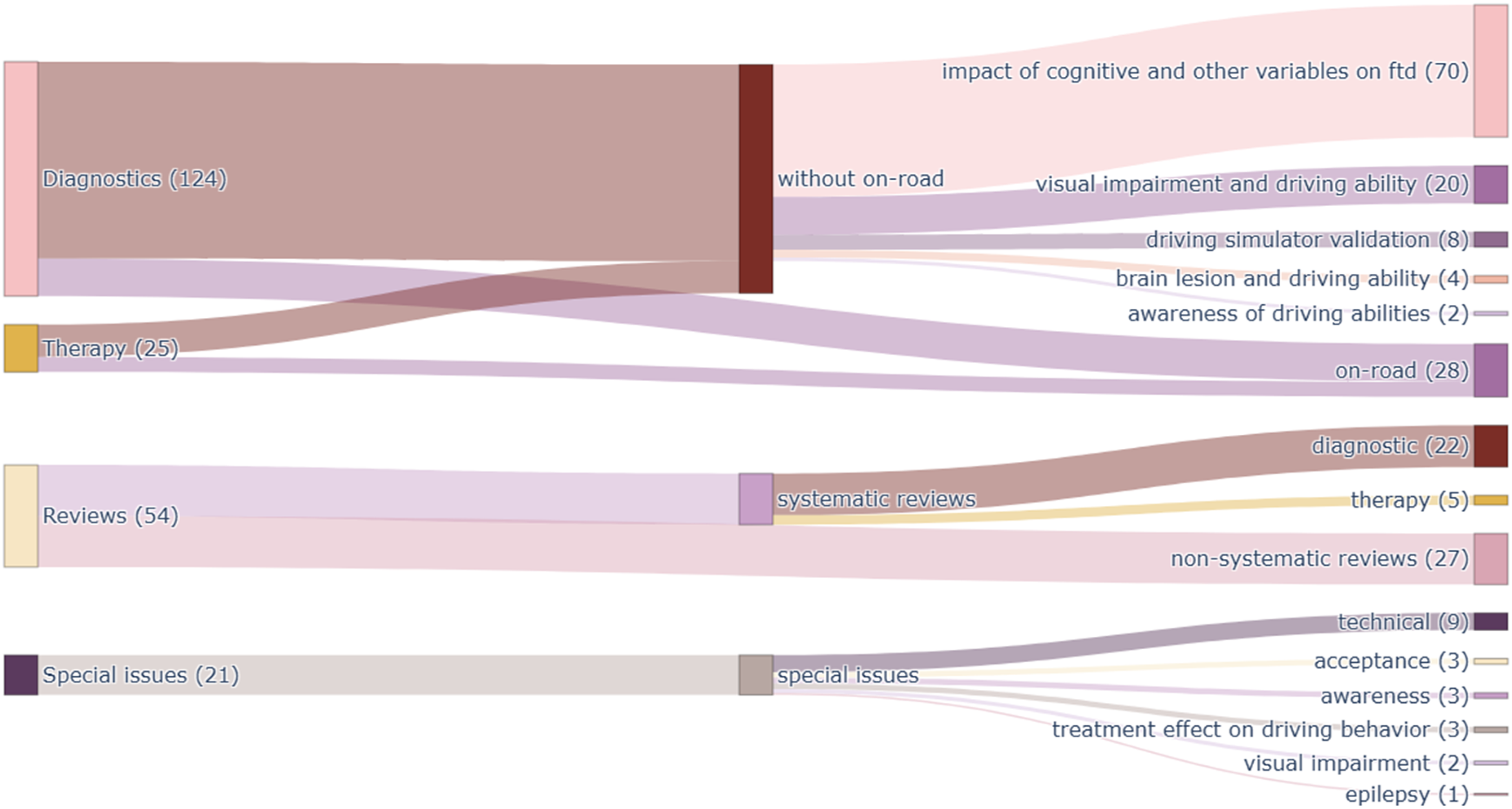
Sankey plot displaying the number of articles per category, reflecting the distribution of areas of interest in driving simulator applications in neurorehabilitation.
Simulated driving for assessing fitness-to-drive
In our literature sample, studies with a diagnostic focus were categorised according to the context in which driving simulators were examined. Firstly, a large proportion of the studies examined whether cognitive or other variables could predict outcomes of simulated driving. Predictors included not only neuropsychological test performance, but also other clinical factors such as disease severity, fatigue, activities of daily living, and socio-demographic factors. Secondly, validation studies investigated whether simulated driving performance could serve as a proxy for on-road driving performance. Thirdly, some studies used neuropsychological assessments and driving simulators together to test their predictive value for real-world driving abilities.
In the selected literature a large proportion of studies investigated which type of neuropsychological tests would predict the outcome of the driving simulator performance (Figure 3 and Supplement Tables 1 and 4). Figure 3 displays the results of this analysis and shows that stroke patients are the most frequently studied neurological population, whereas other neurological conditions, such as brain tumours, have received much less attention. 20 Several cognitive functions were identified as critical for driving behaviour including attention, executive functions and visuo-spatial processing (Supplement Table 8). In particular, for attentional processes, besides processing speed, selective and divided attention were identified as crucial functions for driving. 21 Executive functions relevant to driving have been identified as cognitive flexibility, cognitive control, inhibition and working memory. 22 However, some studies did also find only weak correlations between neuropsychological assessments and simulated driving outcomes,23–26 which suggests that simulators may reveal real-world adaptive behaviors that standardized neuropsychological tests could not predict (Figure 3).
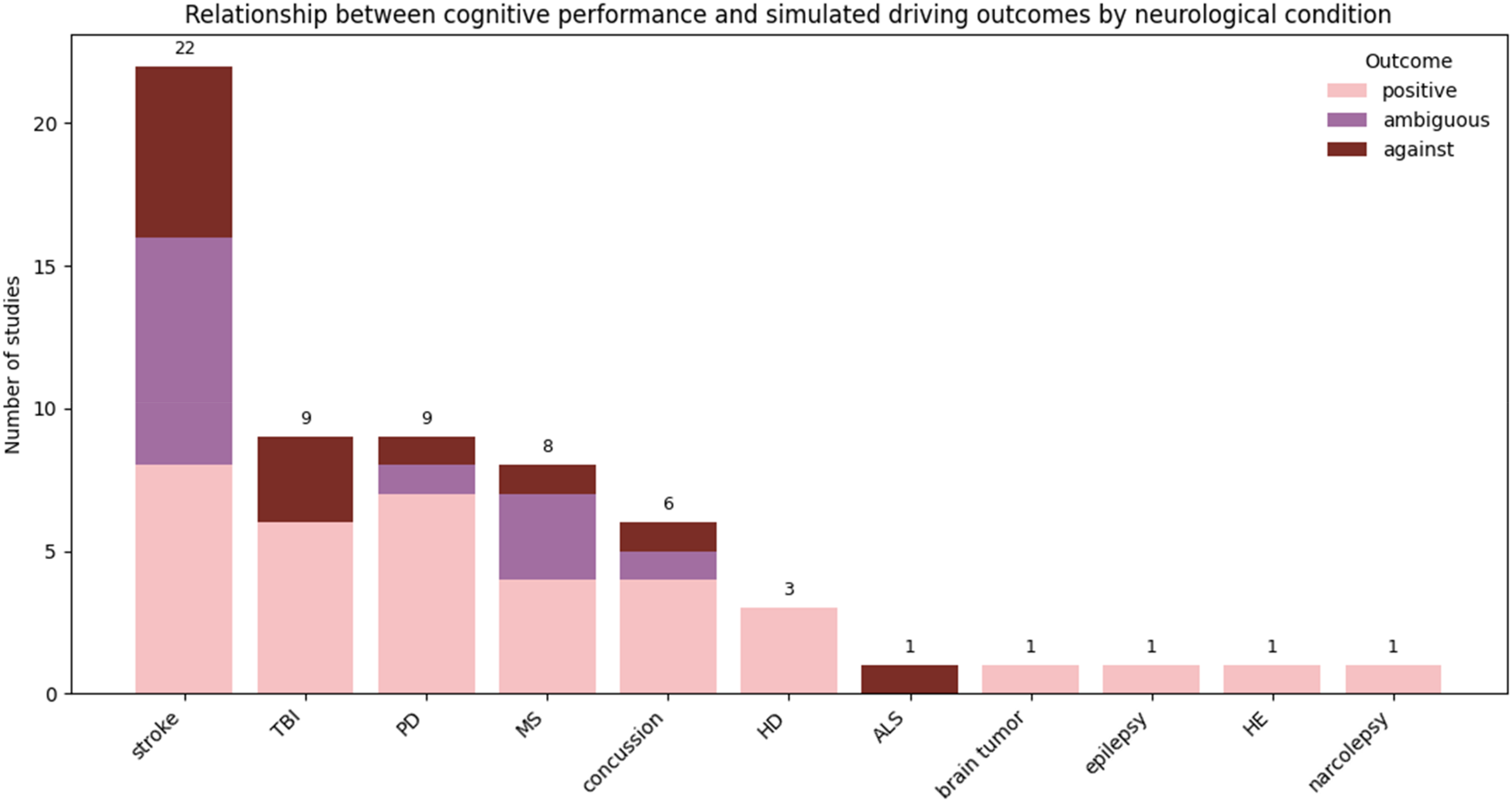
Number of studies investigating the relationship between neuropsychological assessments and simulated driving performance in different neurological populations. Studies were categorized as ‘positive relation’ when the majority of the tested variables showed a significant relationship. Studies were categorized as having ‘ambiguous results’ when at least one variable showed a significant relationship. Studies were categorized as having ‘no relation’ when none of the tested variables showed a significant relationship.
Several studies have investigated the validity of driving simulator settings by evaluating test parameters and the ability of simulated driving performance to make sound predictions of on-road driving performance (Figure 4 and Supplement Table 1). Although some older studies reported only fair agreement between driving simulator and on-road driving assessment outcomes,27,28 the majority of studies found that testing simulated driving may contribute to a valid decision about driving resumption.29–35 This might be due to the fact that in more modern high-fidelity driving simulators, the immersive effects of simulated driving are increased and therefore the outcomes in more recent studies agree better between driving simulator and on-road driving performance. For example, three studies compared the results obtained in a driving simulator and on-road assessments and reported agreement between the eventual decisions.33–35 While two of the studies showed that for patients with visual impairments the use of a driving simulator yielded comparable decision on the fitness-to-drive,33,34 the third study reported that the outcomes of a simulated driving assessment could predict on-road driving abilities ten months later. 35
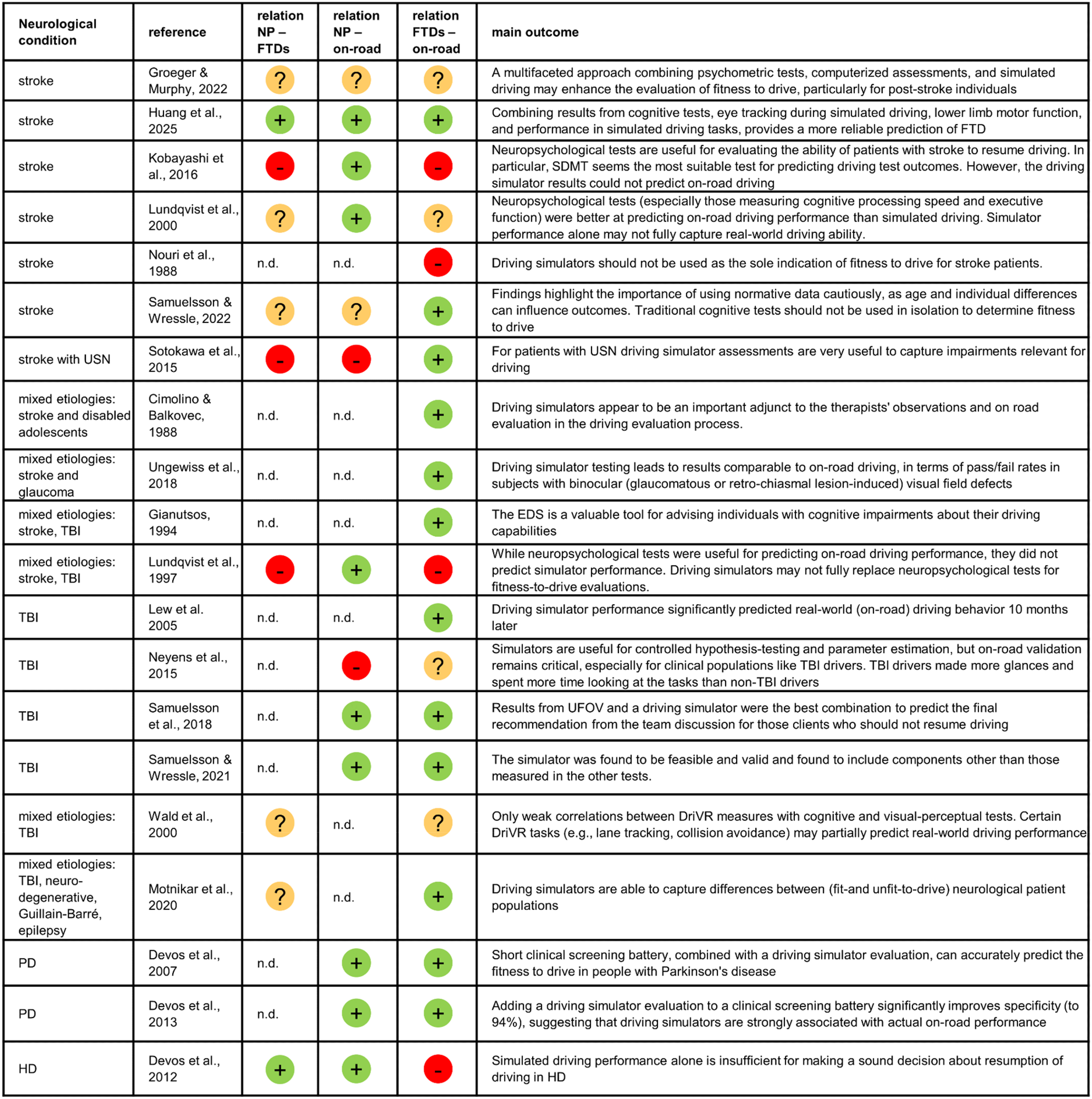
Schematic summary of all articles that included on-road driving as well as driving simulators in their diagnostic process. In the columns ‘relation NP - FTDs’, ‘relation NP-on-road’ and ‘relation FTDs-on-road’ the symbol ‘+’ stands for predominantly positive predictability, the symbol ‘-’ stands for predominantly no predictability, and the symbol ‘?’ stands for only weak predictability or ambiguous results. More detailed information can be found in Supplement Table 1. FTDs = fitness-to-drive evaluated based on simulated driving; EDS = elemental driving simulator.
The links between neuropsychological tests, simulated driving and on-road driving performance
In order to check, which type of measurements are most suitable for testing the fitness-to-drive of neurological patients, we identified studies that investigated the relationships between cognitive tests, driving simulation and on-road driving (Figure 4 and Supplement Table 1). While some studies found neuropsychological testing the best predictor of on-road driving performance,36–38 others reported the driving simulator being able to distinguish better patients to pass or fail an on-road test. 39 However, the majority of studies suggested that a multimodal assessment combining cognitive tests and simulated driving was the best way to assess fitness-to-drive.5,38,40–44 In addition, we categorized these studies according to which neurologic populations were studied, in order to identify potential differences and gaps of knowledge.
For stroke patients, evidence consistently shows that neuropsychological tests ‒ especially the Symbol Digit Modalities Test (SDMT), Trail Making Tests A and B (TMT-A/B), and divided attention measures ‒ predict on-road driving performance better than simulated driving performance alone5,27,36,37,44 . The SDMT stands out as having strong sensitivity and specificity for identifying those likely to fail on-road tests, with divided attention and executive function tasks also showing robust predictive value. Simulated driving assessments provide complementary data and can detect specific impairments, but studies show simulators and on-road outcomes often lack strong agreement and simulators should not be relied upon as standalone predictors for stroke ‒ even though certain behaviors in complex simulated scenarios, such as braking response, may show promise.5,27,28 Thus, for stroke patients a bundled assessment integrating neuropsychological tests, motor function, and targeted simulator metrics seems optimal, but among individual predictors, divided attention and executive function tests like SDMT and TMT-B remain the most reliable for forecasting real-world driving fitness after stroke.5,27,36,37,40,44
In patients with TBI one study found that neuropsychological tests could predict on-road performance, where neuropsychological tests classified risk awareness with 78% accuracy. 28 Among the tests, in particular tests evaluating simultaneous capacity contributed most to the on-road performance prediction. However, this study did not find any advantage of the driving simulator to predict on-road performance. A more recent study found that UFOV had the highest sensitivity (78%), while UFOV combined with driving simulator performance proved the best combination to predict the expert recommendations based on the on-road driving performance about who should not resume driving (sensitivity 87%). 41 This was confirmed by another study by the same group suggesting that the driving simulator could assess relevant motor aspects like wobbling and driving errors (e.g., misses and faults) that are not captured by purely neuropsychological tests. 45 Similarly, Motnikar and colleagues also suggested that simulators are able to capture real-time driving errors (e.g., lane deviation) better than paper-and-pencil tests, but point also to the importance of the virtual driving environment and scenarios to be able to assess driving errors sufficiently. 39 Moreover, certain driving simulator outcomes such as lane tracking and collision avoidance have been shown to partially predict on-road driving performance. 43
For patients with PD (PwP) one study by Devos and colleagues found that a screening battery consisting of four clinical variables (disease duration, contrast sensitivity, Clinical Dementia Rating, and the motor part of the Unified Parkinson's Disease Rating Scale) were able to predict best the fitness-to-drive and correctly classified in their sample 90% of the patients with PD as pass or fail (sensitivity 91%, specificity 90%) as assessed in on-road driving. 42 Adding an evaluation from a driving simulator to the prediction model the total explained variance increased and correctly classified 97.5% of patients as able and unable drivers (sensitivity 91%, specificity 100%). The validity of the screening battery was confirmed in a subsequent study. 46
For patients in an early stage of Huntington's disease another study by Devos and colleagues suggested that the driving simulator performance in HD patients aligned with their on-road driving risks, but the study did not suggest the simulator as a standalone predictor. 47 Instead, cognitive tests (SDMT, Stroop word reading, and TMT-B) outperformed simulator metrics in predicting on-road outcomes. Besides, studies have shown that driving simulators are able to classify drivers with specific neurologic disease such as patients with HD or patients with HIV-associated neurocognitive disorder (HAND) compared to healthy controls with a certain accuracy (see also Supplement Table 4).48,49
Visual impairment and simulated driving
Visual impairments are often a consequence of neurologic conditions. Yet, unimpaired vision is a crucial prerequisite for safe driving. In our literature selection 20 articles focused on the impact of visual impairments tested in simulated driving (Supplement Table 4). The driving simulator offers a safe way of testing the extent of visual impairment in a realistic setting.50,51 Studies using the driving simulator found that drivers with homonymous hemianopia show impaired fitness-to-drive and exhibit significant blind-side detection deficits with higher miss rates and longer reaction times for hazards (e.g., pedestrians) on the affected side.52,53 It was found that approaching pedestrians are detected more often than stationary ones, but responses are often too late to avoid collisions.50,54 Only approximately 25% of patients with homonymous hemianopia adapt gaze and head movements to effectively scan the impaired side. 55 Successful compensators show increased saccade amplitude/velocity and wider horizontal eye movements toward the blind side. 56 However, as an intervention using a specific setup in a driving simulator it has been shown that auditory cues significantly improve proactive scanning and hazard response times. 57 Overall, it has been suggested that visual field size alone only poorly predicts driving safety and that compensatory behaviours (e.g., head movements) are critical. 50
Also, in patients with visuo-spatial neglect (VSN) the driving simulator represents a helpful tool to evaluate the extent of the impairment for driving. It has been shown that traditional paper-and-pencil tests miss mild or largely compensated VSN, while dynamic tests such as the driving simulator are better able to detect relevant deficits for safe driving behaviour. 58 For example, tested in a driving simulator it was found that VSN patients would deviate lane position toward the non-affected side. 33
For PwP it has been shown that these patients exhibit poorer vehicle control (e.g., more lane violations) and higher crash rates under simulated low-contrast conditions (e.g., fog). 59 Moreover, it was found that PwP show in their gaze behaviour reduced fixation on task-relevant areas which increases collision risk. 60 In general, visual processing speed, contrast sensitivity and motor dysfunction are suggested as key predictors of fitness to drive in people with Parkinson's disease. 59
Simulated driving interventions for driving rehabilitation
The second important field of application of the driving simulator is its use as a therapeutic tool. Twenty-five original articles were found to study the driving simulator for therapeutic interventions to rehabilitate driving abilities. Only eight of these studies used on-road driving as validation of effectiveness (see Figure 5 and Supplement Table 2).8,961–66 In addition, five of the systematic reviews were retained with a focus on simulator-based driving training (Supplement Table 3).67–71
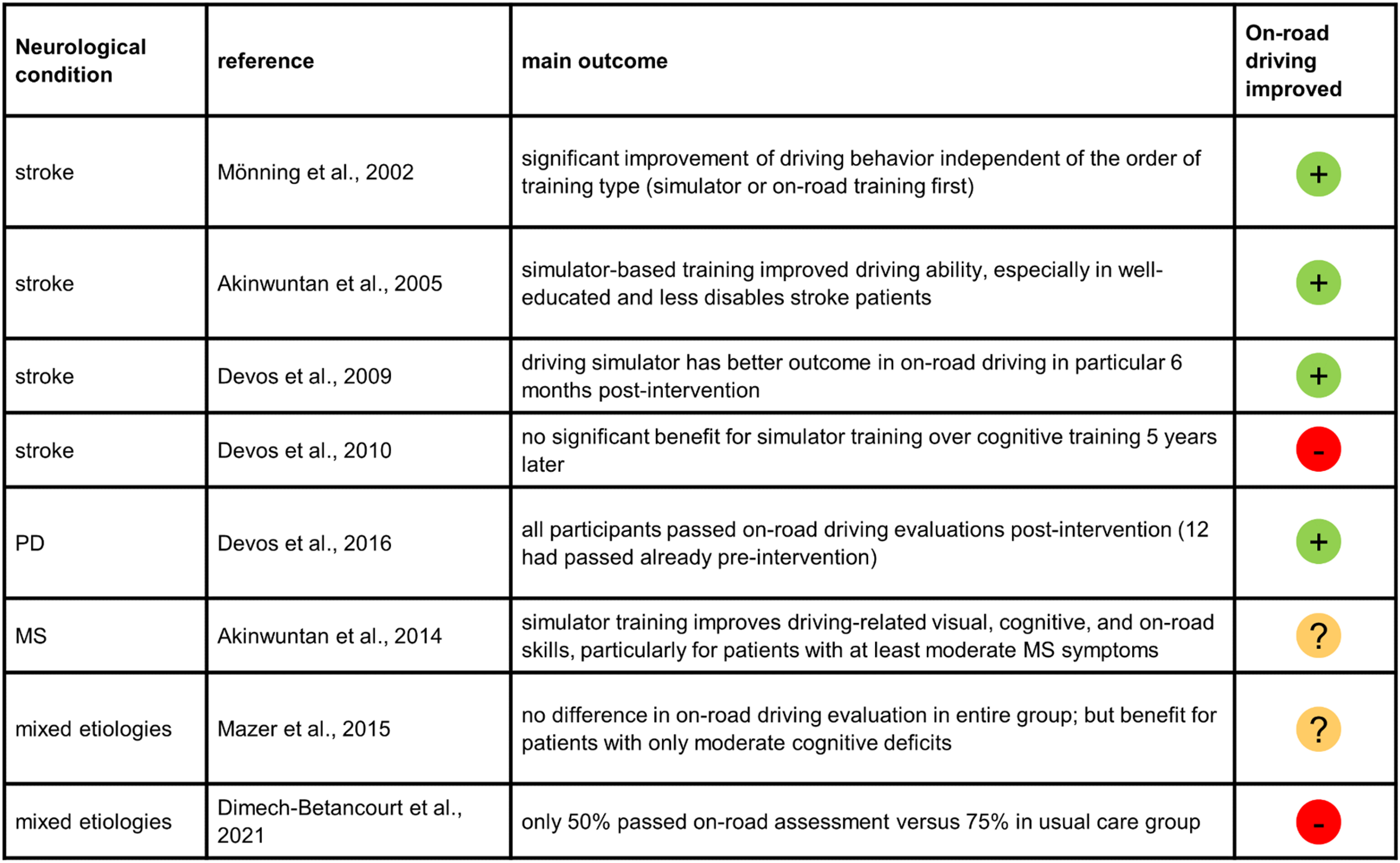
Schematic summary of articles including simulator training and on-road driving outcomes. In the column ‘on-road driving improved' the symbol ‘+’ indicates a benefit, the symbol ‘‒’ indicates no benefit and the symbol ‘?’ indicates ambiguous results for driving simulator training on on-road driving performance. More detailed information can be found in supplement table 2.
Regarding stroke patients, an original article about a randomized controlled trial reported about an intervention, in which post-stroke patients participated in 15 h of driving simulator training in comparison to cognitive training alone. 62 It was found that simulator-based driving training improved driving ability in stroke patients, especially those who were well-educated and had less overall disability. With a similar setup from the same research group it was found that simulator-based driving training led to greater improvements in tactical driving skills compared to cognitive training, both immediately after training and at 6-month follow-up. 63 However, a follow-up of this RCT after five years showed that the advantage of simulator-based driving training over cognitive rehabilitation therapy, evident at 6 months post-stroke, had faded 5 years later. 64 In the comparison of simulator-based driving training to on-road driving training it has been reported that stroke patients who failed an initial driving test were able to regain driving ability through a combination of driving lessons and simulator training (ten 30-min simulated driving trainings and five 45-min on-road driving trainings), with 90% passing a third driving test after the training. 61 A Cochrane review of interventions that examined the effects of training to improve driving after stroke identified four trials. 72 Overall, the Cochrane review found insufficient evidence to conclude that driving rehabilitation improves fitness-to-drive in stroke survivors, citing small sample sizes, heterogeneous protocols, and a lack of long-term outcome data.
For patients with Parkinson's disease one study showed that three simulator sessions reduced crashes and reaction times in PwP drivers. 73 Moreover, a pilot study showed that a 10-h stimulated driving training program over 12 weeks improved on-road pass rates in PwP, although simulator metrics did not change significantly. 8 An intervention study on the use of driving aids showed that an advanced driver assistance system (ADAS) that gives feedback during driving could improve speed control in PwP drivers, but the performance declined again when the ADAS was removed. 74 A systematic review reported beneficial effects of simulated driving training for PwP. 75 The authors suggested that driving rehabilitation strategies for individuals with PD should include training of operational and tactical driving skills or indirect comprehensive training programs of visual, cognitive, and motor skills. Besides, as a special issue in PD, driving simulators have also been used to show that subthalamic nucleus deep brain stimulation as PD treatment could improve driving accuracy and reduce driving errors in PwP compared to medication only (as assessed in simulated driving environments).76,77
For patients with relapsing-remitting MS a pilot study showed that a simulator-based training program led to improvements in passing the road test, with four out of seven participants who initially failed passing after the training. 65 The training group also showed improvements in visual, cognitive, and fatigue measures. The improvements were most pronounced in those with at least moderate disability (EDSS > 3).
In studies with mixed etiologies of acquired brain injuries (ABI) one RCT found that for patients with ABI (stroke and TBI) driving simulator retraining (16 sessions, 2 per week for 8 weeks, each lasting 60 min) did not improve the overall rate of passing the on-road driving evaluation compared to the control group. 9 However, participants with moderate impairment who received simulator training were more likely to pass the driving test compared to the control group. For patients with severe impairments no differences in pass rates were found. Another randomized controlled pilot study with patients with ABI (stroke, TBI, tumor) revealed that a driving simulator intervention (45 min, 2 days a week, for 4 weeks) did not clearly improve on-road driving performance compared to usual care. 66 However, the study indicated that a simulated driving intervention might help to improve the driver's confidence. In a systematic review on types and effectiveness of interventions used by occupational therapists to improve on-road fitness-to-drive three types of intervention approaches were identified to be commonly reported (computer-based driving simulator training, off-road skill-specific training, off-road education programs). However, only limited evidence for the effectiveness of these types of interventions were shown to improve fitness-to-drive. 78
Simulated driving for cognitive training
Some articles also investigated the use of driving simulators for cognitive training purposes regarding attention and memory,79–81 with the driving simulator being a realistic and motivating training option. However, besides limited evidence of generalized benefit for cognitive functions (one single case study reporting improvement of verbal working memory 82 ), in two studies it was reported that training in a driving simulator did not improve regarding UFOV, selective and divided attention any better than standard cognitive training.80,83
Impaired self-awareness and driving
Neurologic patients may also show impaired perception of their illness, and reduced awareness of driving impairment can lead to inappropriate self-assessment and decisions about resuming driving.84,85 Moreover, awareness of difficulties and evaluating one's own driving capacities is also required for compensatory behaviour on the strategic level. 28 It has been reported in one study that most stroke participants who failed a simulated driving evaluation showed limited awareness of their driving abilities. 84 Awareness and cognitive screening explained 74% of variance in driving ability, which highlights the need to consider awareness in evaluations of fitness-to-drive. However, another study reported that post-stroke drivers self-rated their performance more poorly, suggesting awareness of deficits and potential behavioral adjustments for compensation. 85 Moreover, McKay and colleagues showed that although stroke survivors overestimated their driving performance, feedback could improve accuracy, which supports driving simulators for awareness training. 86 These studies thus suggest that awareness represents an issue in fitness-to-drive in neurologic patients and that simulated driving and the confrontation with driving errors in simulated driving may improve awareness, which may lead to a more realistic self-evaluation about resumption to drive.85,86
Neural correlates of impaired driving
Some studies have used the driving simulator to investigate the neural correlates of impaired driving because the driving simulator offers a safe environment for testing driving behaviour in patients. Regarding hemispheric differences significant differences were found between stroke patients with left versus right hemispheric lesions regarding driving errors (e.g., center line crossing, brake reaction time). 87 Moreover, patients with right-hemisphere damage who were evaluated by official experts as not able to return to driving had lower reaction rates in simulator tasks. 88 One study by Papageorgiou and colleagues found that right-hemisphere lesions (parieto-occipital regions) impair spatial working memory, while left-hemisphere lesions (fusiform gyrus) affect object processing during collision avoidance. 89 Ventromedial prefrontal cortex (vmPFC) damage was reported to make patients more susceptible to adverse social pressure (e.g., aggressive honking), which led to riskier driving decisions (e.g., unsafe gap selection). 90 Regarding cerebellar damage one study reported impaired speed control in basic driving conditions, while interactive driving abilities were preserved. 91 These studies showed that hemispheric and cerebellar lesions differentially affect driving skills, which requires tailored interventions to regain fitness-to-drive.
Acceptance and applicability of simulated driving
The literature shows that driving simulators are generally well-accepted by patients and clinicians with positive feedback on usability and effectiveness.92–95 Driving simulators have been evaluated as feasible to be used in rehabilitation, assessment and training, in different neurological and brain injury populations.92,96 However, Crisler and colleagues reported that although seniors and physicians viewed driving simulators favorably for clinical assessments the adoption remains still limited 93 and the use of a driving simulator is not part of a clinical standard evaluation of fitness-to-drive. The barriers to implementing driving simulators in neurorehabilitation seem to include not only cost and accessibility, but also concerns are reported about providing false hope about returning to driving in some cases. 95 Another issue that might limit the use of driving simulators is simulator sickness that can be experienced in virtual environments. In the literature simulator sickness is reported as a notable issue, particularly among older adults and females, but does not disproportionately affect neurological patients.96,97
Automatic assessments of fitness-to-drive
In the development of driving simulators, efforts are also being made to carry out driving fitness checks using artificial intelligence methods. In two studies, the driving-pass system was tested, which is based on deep features and machine learning principles and uses the parameters from the driving simulator on the one hand and subjective assessments and information from the test subjects on the other hand to predict fitness-to-drive.98,99 The studies show that this approach is possible and enables a standardised assessment of fitness-to-drive. A systematic review on simulator-based automatic assessments of driving (SAAD) revised the metrics used in simulator-based driving assessments and provided guidelines and detailed recommendations for reporting and conducting SAAD research, including the design of driving scenarios, selection of assessment inputs, and use of simulator tools. 100 Moreover, automatic assessments of fitness-to-drive that could be provided by driving simulators as a perspective require beforehand the establishment of validated norms. 40 In the future, it seems quite conceivable that fitness-to-drive assessments could be carried out using fully automated, machine learning-based methods in driving simulators. As a future perspective, a new field of research involving the use of driving simulators in the context of self-driving vehicles is also emerging, which will also have a crucial impact on the assessment of fitness-to-drive in neurorehabilitation. Advanced driver-assistance systems have already been investigated in some neurologic populations, 74 however the improvement of this technology as well as the progressive development of automatic driving systems will represent new challenges in the evaluation and the rehabilitation of fitness-to-drive.
Discussion
Driving simulators are increasingly recognized as valuable tools for assessing and rehabilitating driving skills in individuals with neurological conditions. Their primary advantage lies in the ability to replicate complex driving scenarios in a controlled, safe, and ecologically valid environment.6,12 These environments enable clinicians to capture real-time driving behavior, such as reaction time, lane and speed control, and error patterns, which are often missed by traditional neuropsychological tests.45,101 Across the literature, simulators have been applied for diagnostic evaluation, therapeutic training, and, in some cases, to enhance patients’ self-awareness of driving limitations.66,86
When used for diagnostic purposes of fitness-to-drive, simulators often supplement neuropsychological testing and on-road assessments. Although findings vary, studies support the use of simulators as part of a multimodal approach.41,102,103 In particular, simulators appear to offer additional value in identifying performance-based deficits in attention, executive function, and visuospatial processing. Key cognitive domains are consistently linked with driving outcomes21,22,37 and some research suggests that cognitive tests alone can predict on-road performance.36,37 However, other studies report that simulators better capture functional impairments that emerge only in dynamic, context-rich settings.35,45 Moreover, the literature shows that simulators are sometimes more effective than cognitive screening in detecting specific impairments such as spatial neglect or hazard response deficits.33,50,52 The use of both modalities thus provides a more comprehensive picture of fitness-to-drive. Nevertheless, significant heterogeneity persists across studies in terms of simulator design, metrics, and outcome definitions. Although structured scenario-based protocols have been proposed,100,104,105 no consensus has yet been established. This lack of standardization hampers research synthesis and clinical implementation. Furthermore, the development of diagnosis- and age-specific normative data is necessary to improve the reliability of simulator-based evaluations. 40 It is also important to note that legal standards for determining fitness-to-drive vary internationally, which complicates uniform clinical guidance.
From a therapeutic point of view, driving simulators show promise, particularly in individuals with mild to moderate impairments following stroke, TBI, or Parkinson's disease.8,63,73 Multiple studies have demonstrated improvements in tactical driving skills such as lane maintenance, hazard anticipation, and braking performance.61,62,73 However, evidence for transfer to real-world driving remains mixed. While some studies report simulator training to be more effective than cognitive rehabilitation in improving on-road test outcomes,62,63 others found no significant difference between the two types of interventions, particularly regarding sustained improvements in visual attention or executive functioning.64,66,80 Moreover, as a gap of knowledge, no studies to date have systematically combined cognitive and simulator-based training, though such integration may be ideal. Driving is a complex behavior that relies on both underlying cognitive capacity and the ability to compensate through adaptive strategies. 98 As such, interventions that train both cognitive functions and real-time decision-making are likely to be more effective.
The literature highlights specific features that contribute to the success of simulator-based rehabilitation. Feedback mechanisms, such as auditory cues, can improve hazard detection and speed control in patients with TBI or hemianopia.57,106 Similarly, interventions that employ graded task difficulty, e.g., progressively increasing traffic complexity ‒ have proven beneficial in patients with Parkinson's disease. 73 Structured programs involving multiple sessions over time (e.g., 10–15 h over several weeks) are more likely to yield meaningful improvements. 7 These effects appear strongest in patients with residual cognitive or motor resources, while individuals with more severe deficits tend to benefit less.9,10,107 Simulator training has also shown utility in improving patient awareness of deficits, which is an important factor in safe return to driving.10,84,86 However, despite these findings, therapeutic guidelines for the clinical use of driving simulators remain scarce. 4 Clearer recommendations are needed regarding training duration, target outcomes, and patient selection criteria.
Technological variability further complicates both clinical and research applications. Simulators differ in motion feedback, scenario realism, data capture, and fidelity ‒ all of which influence outcomes and patient engagement.15,92,108 Some studies have addressed this by proposing unified scenario designs or scoring systems,100,103,104 while others are exploring machine learning solutions. For instance, automated driving performance assessments using deep features and classification models have demonstrated promising accuracy in pilot studies.100,105 These AI-based tools combine simulator data with subjective inputs to predict driving fitness and may eventually streamline clinical decision-making. However, such systems still require validation against clinical gold standards and must be supported by normative datasets. 40 Looking ahead, simulators may also play an important role in evaluating how individuals with neurological conditions interact with advanced driver-assistance systems (ADAS) or semi-autonomous vehicles.74,77 These developments will introduce new considerations for fitness-to-drive assessments, particularly in the context of shared control between human drivers and automated systems.
As limitations of our review it should be noted, that the selection of language might have induced a bias in the identified literature. However, as only a very small number of German articles were involved, this bias seems negligible. Furthermore, we recognize that publication bias is a potential limitation in any literature review, as studies with non-significant results are less likely to be published. The studies included in this review produced a variety of results, including positive, negative and inconclusive findings. This suggests that publication bias has not had an excessive influence on our findings.
In summary, this review highlights the evolving role of driving simulators in neurorehabilitation. Their ability to provide feedback, adapt to performance levels, and safely simulate complex traffic scenarios makes them a valuable addition to multimodal rehabilitation. Nonetheless, the absence of standardized protocols, normative reference values, and consistent clinical guidelines limits their broader application. Future research should prioritize the harmonization of simulator design, assessment protocols, and outcome measures. Combined training approaches that target both cognitive and behavioral components of driving may offer the greatest benefit. With further development, simulators can move from research contexts into routine clinical practice, offering a scalable, evidence-based method for evaluating and restoring driving capacity in neurological populations.
Clinical messages
Multimodal fitness-to-drive assessments, combining cognitive testing and driving simulation, offer the most accurate insight into driving readiness in neurological patients by capturing both underlying deficits and real-time behaviors. Driving simulators are effective for rehabilitation in patients with mild to moderate impairments, particularly for improving tactical driving skills like hazard perception, lane control, and response speed. Simulated driving enhances awareness by exposing patients to errors in real-time, helping them recognize limitations and adopt safer driving strategies before returning to on-road conditions. Standardized simulator protocols are urgently needed to ensure consistency, improve clinical decision-making, and enable comparisons across settings and patient groups in both diagnostics and training.
Supplemental Material
sj-docx-1-cre-10.1177_02692155251393560 - Supplemental material for State-of-the-art applications of driving simulators in neurorehabilitation: A scoping review
Supplemental material, sj-docx-1-cre-10.1177_02692155251393560 for State-of-the-art applications of driving simulators in neurorehabilitation: A scoping review by Wiebke Trost, Zino H Wellauer, Jutta Küst, Markus Hackenfort and Bartosz Bujan in Clinical Rehabilitation
Footnotes
Ethical approval and informed consent statements
There are no human participants in this article and informed consent is not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The references that this scoping review is based on are all listed in the article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.